
Abstract
Background
Minimal residual disease (MRD), which is characterized as leukemic cells at a level below morphologic detection, has been connected to the risk of relapse in acute myeloid leukemia. In 80–90% of acute myeloid leukemia (AML) patients, the Wilms tumor (WT1) gene is overexpressed at the mRNA level. In our prospective study, a total of 55 patients were enrolled in the study. Group I involved 40 AML patients and group II involved 15 patients healthy controls. WT1 gene expression was quantified using quantitative real-time PCR on bone marrow samples from AML patients at initial diagnosis and at day 28 after induction chemotherapy, and compared to 15 healthy controls in group II. Follow up of patients for prognosis evaluation was assessed. IBM SPSS software was used to capture and analyses the data.
Results
At diagnosis, the mean WT1 transcript value in AML patients was substantially higher than the expression observed in control patient’s Bone marrow. There was no statistically relevant relationship between the onset of relapse and WT1 expression. Patients with WT1 overexpression at diagnosis had a shorter overall survival than patients with negative WT1 expression.
Conclusions
Wilms tumor 1 gene expression was found to be significantly higher in AML patients than control cases, overall, our results confirmed the prognostic significance of WT1 overexpression in AML patients. Our findings support the application of MRD in AML patients based on WT1 overexpression.
Similar content being viewed by others

Background
Acute myeloid leukaemia (AML) is a disease with a wide range of genetic anomalies, as well as immunophenotypes, and clinical outcomes. AML is currently the most common type of acute leukaemia in adults [1]. After achieving morphologically specified complete remission (CR) with induction chemotherapy, more than half of adult patients with AML relapse [2]. Traditionally, cytomorphology has been used to determine post-treatment remission, with relapse being identified as 5% blasts in the BM that are not due to other causes. Microscopic evaluation of BM or PB morphology is based on the analysis of a limited number of cells (200–500 cells), and its accuracy is influenced by sample quality and pathologist expertise [3].
Post-chemotherapy perseverance of minimal residual disease (MRD), which is characterized as leukemic cells at a level underneath morphologic detection, has been linked to the risk of relapse [4].
In the treatment of patients with acute lymphoblastic leukemia, acute promyelocytic leukemia (APL), and chronic myeloid leukemia, MRD monitoring has become standard practice. The existence of MRD is a solid, autonomous prognostic marker of amplified risk of relapse and shorter survival in patients with AML compared to patients with a negative MRD, according to mounting evidence [5].
Flow cytometry and molecular techniques for detecting remaining disease are more sensitive than morphologic assessment, and there is growing agreement that MRD should be renamed “measurable residual disease,” since the existence of any disease identified by these methodologies after treatment is linked to an inferior prognosis, and identification of residual disease even in morphologic remission is associated with a poorer prognosis [6]. MRD monitoring is rapidly becoming the most successful method and technique for determining prognosis and therapeutic strategy for AML patients, and it is now widely tracked using qRT-PCR, as evidenced by numerous studies from various laboratories. Over the last few years, real-time PCR has been implemented, allowing for a remarkable degree of sensitivity in diagnosis and the ability of leukemia to be detected [7].
Detecting fusion genes derived from chromosomal translocations, such as PML-RARA, AML-ETO1, and CBFb-MYH11, and more recently gene mutations, such as NPM1, is currently the most sensitive tool for this strategy [8, 9]. Unfortunately, more than half of all AML patients do not have the genetic lesions that can be monitored for MRD. As a result, alternative MRD markers are in high demand, and Wilm's tumor is one of them [10].
In BM samples from 80 to 90% of AML patients at diagnosis, the WT1 gene is overexpressed at the mRNA level, and it is detectable in a stable low range in normal donors [11]. It can be thought of as a universal molecular marker of malignant hematopoiesis, and several studies have suggested that quantifying WT1 expression level as a molecular marker for MRD monitoring is useful. Moreover, it’s been proposed that its level of expression can have prognostic consequences for AML patients' remission rate and overall survival [12]. While treatment outcomes of AML have improved steadily over the last decades in younger and adults, limited changes have been observed in survival. We investigated the function of WT1 gene expression in AML patients' prognosis and its utility as an MRD marker after induction chemotherapy.
Materials and Methods
A total of 55 patients were recruited from the hematology unit of Alexandria main university hospital for the research. Group I: WT1 expression was tested in bone marrow samples of 40 adult patients with newly diagnosed de novo AML at diagnosis and at day 28 after induction chemotherapy. Group II: included 15 (age and sex-matched) healthy controls with no prior history of hematological malignancy. The revised French-American-British classification was used to diagnose and classify AML established on morphologic, immunophenotypic, and cytochemical parameters [3]. From all participants an informed consent was taken in this study.
Laboratory investigations
-
Complete blood image and morphological analysis in the laboratory.
-
Aspiration of bone marrow
-
Cytogenetic study
-
Assays for fluorescence in situ hybridization (FISH).
-
Immunophenotyping by flowcytometry. The Mo Abs mentioned below were used Table 1.
-
RT-PCR quantification of a bone marrow sample for WT1 gene expression assay
A Blood QI Aamp RNA blood mini kit was used to isolate RNA (Qiagen, Germany). Thermocycler (Applied Biosystems, USA) was used for reverse transcription, and the samples were held at -800 until PCR amplification. Finally, using Ipsogen WT1 ProfileQuant, real-time quantitative detection was performed on Stratagene (PCR MX 3000P, USA) (QIAGEN, Germany). The WT1 gene level was determined and expressed as a ratio to the ABL gene (endogenous control) found in the human body.
Treatment protocol
Induction chemotherapy for AML patients consisted of 3 days of anthracycline within 7 days of cytarabine (“3 + 7” protocol) [13]. From day one to day three, patients were given 45 mg/m2 Anthracyline (Daunorubicin) intravenously. From days 1 to 7, they were given Cytarabine (cytosine arabinoside) 100 mg/m2 via continuous infusion [14].
Assessment and consolidation after remission with four additional cycles of (HiDAC); high-dose Cytosine Arabinoside or (HAM regimen); high-dose Cytosine Arabinoside with Mitoxantrone.
Response criteria for AML patients after induction chemotherapy: [13]
Complete remission (CR) was defined as morphologically normal bone marrow with less than 5% lasts, neutrophil count more than 1.5 × 109/l, and platelet count more than 100 × 109/l.
Complete remission with incomplete hematologic recovery (CRi) Partial remission.
Primary induction failure (PIF), Relapse is characterized as disease recurrence after complete remission (CR) with more than 5% leukemic blasts in BMA or new extra medullary leukemia. Early relapse occurs within 6 months of CR1, while late relapse occurs after a period of more than 6 months [15]. The overall survival (OS) of a trial's patients is determined. It is calculated from the time of enrollment in a clinical trial or diagnosis to the time of death [16].
Statistical analysis of data
IBM SPSS software was used to capture and analyses the data. Quantitative data were defined using range (minimum and maximum), mean, standard deviation, median, and interquartile range, while qualitative data were described using numbers and percentages (IQR). The significance of the gained results was determined at a 5% level of significance.
Chi-square test, Fisher's exact correlation, Mann Whitney test, Student t-test, Spearman coefficient, Receiver operating characteristic curve (ROC), were some of the tests used.
Results
Demographic data
AML patients were divided into 23 females (57.5%) and 17 males (42.5%). The participants' ages ranged from 30 to 50 years old, with a mean of 38.40 6.62 years. The FAB classification of AML patients is shown in Fig. 1. The majority of them were FAB-M5 (42.5%). AML patients' cytogenetic risk stratification. The majority of the people were at a medium risk (55%) Table 2.

Distribution of the AML patients according to FAB classification (n = 40)
WT1 Expression in AML patients and controls
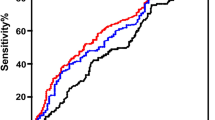
The mean value of WT1 transcript in AML patients at presentation was 11,109.3 ± 133,387.3 × 104/ABL, which was significantly greater than expression found in control patients BM. (median value of 69 × 104/ABL) Table 3. To determine a cut-off value for WT1 positivity, a receiver operating characteristic (ROC) curve analysis was created, based on the NCN of WT1 gene expression of both AML patients and controls Fig. 2. According to the Youden index, a cut-off value of 1059 was used, which was 87.5% adaptive, had an AUC of 0.95, 100% accuracy, a negative predictive value (NPV) of 75%, a positive predictive value (PPV) of 100%, and was significant statistically (p value 0.001) Table 4.

ROC curve generated for level of WT1 expression among AML patients and controls
WT1 Expression at diagnosis
WT1 expression levels in the BM of 40 adults with newly diagnosed AML were tested using real-time quantitative polymerase chain reaction (RQ-PCR). According to the cut-off value for WT1 positivity, 35 AML patients (87.5%) showed WT1 overexpression at diagnosis and 5 patients (12.5%) were WT1-negative. WT1 expression at diagnosis did not correlate with age, sex, hemoglobin level, leukocyte count, or peripheral blood & bone marrow last percentage at diagnosis. Also, no correlation was found between WT1 expression at diagnosis and AML FAB subtype & cytogenetic findings.
WT1 Expression after induction treatment
WT1-positive AML patients were followed up on post-induction chemotherapy by real-time PCR for their level of WT1 expression and morphological assessment by BM analysis in a trial to see whether WT1 expression could be utilized as a marker for follow-up and MRD assessment. A statistical significance was found between WT1 expression post-induction & hematological response on BM examination, thus, indicating a higher sensitivity of WT1 assessment over the morphological examination of the BM in the follow-up of AML patients to estimate the response to chemotherapy Table 5.
WT1 expression and long term outcome of AML
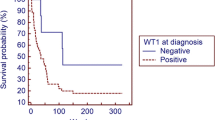
AML patients were followed up on for 15 months after diagnosis to see whether WT1 expression levels had any impact on their overall survival. The OS was calculated using the Kaplan–Meier survival study Fig. 3. The potential difference between WT1 positive and WT1 negative was analyzed by the log-rank test. Although the WT1-positive patients had a shorter OS than those with negative WT1, the disparity was not statistically significant. (Average of 10.14 vs. 13 months) Tables 6 and 7.

Kaplan–Meier survival curve for overall survival with WT1 expression (n = 40)
We then used Cox regression analysis between OS and WT1 expression at diagnosis among the WT1-positive AML patients. WT1 expression seems to affect statistically significant OS (P value < 0.038). As a result, it appears that patients with WT1 overexpression at diagnosis have a shorter OS than those who do not have WT1 positivity.
WT1 expression and relapse prediction of AML
Among AML patients 44.8% experienced early relapse and 55.2% late relapse. There was no significant difference among the time of occurrence of relapse and WT1 expression Table 8.
Discussion
In AML, relapse is still the leading cause of treatment failure and death. Despite the fact that more than 80% of patients receive a CR after traditional chemotherapy, a large proportion of them develop recurrent disease [17]. Indeed, more stringent response requirements than CR are needed. The gold standard approach for stratifying patients based on the likelihood of relapse is to detect leukemia-specific gene mutations using PCR. Unfortunately, more than half of all AML cases lack one of these unique genes, so new MRD-detecting genes are required. WT1 is a transcriptional factor that has been identified as an MRD marker in acute leukemia [11].
The aim of this study was to look into the prognostic value of WT1 gene overexpression in AML patients, as well as its utility as an MRD marker after treatment. At a statistically significant amount, the WT1 level in AML patients was significantly higher than in control cases in our cohort. At the time of diagnosis, 87.5% of AML patients had an overexpression of the WT1 transcript. This finding was similar to that revealed by other studies where WT1 overexpression was reported to be approximately between 70 and 90% of AML patients [18,19,20,21].
Regarding our AML patients in this study, WT1 expression was not affected by the patient’s hematological profile such as platelet count, hemoglobin level, or WBC count. This was also in agreement with Østergaard et al. who conducted a study on BM samples from 133 newly diagnosed AML patients and compared them with those in healthy volunteers and found no statistical significance between WT1 expression and hemoglobin level, WBC, or platelet count [18, 23]. No significant association was found between a higher PB and BM blasts percentage and WT1 overexpression which came in congruence with Assem et al. and Ibrahim et al. who also had similar findings in their studies [23, 24]. However, Lane et al. conducted a study on 58 de novo AML patients and found, by using multivariate Cox regression analysis, that elevated WT1 levels were significantly associated with higher PB and BM blast percentage [25]. The high WT1 expression is hypothesized to originate from CD34-positive cells, thus it seems that the discrepancies might be due to differences in sample size.
In the current research, we discovered that AML patients who were WT1-positive at diagnosis had a shorter OS than those who were WT1-negative. Similarly, Bergmann et al., who conducted a study on 139 de novo AML patients reported that Patients with low WT1 levels had a 59% chance of 3-year overall survival (OS), while patients with high levels had a 21% chance [27]. Galimberti et al. also discovered that AML patients with elevated WT1 levels have a higher risk of disease progression [26]. In a larger sample population, Nomdedéu et al. reported the prognostic function of high WT1 levels at diagnosis [27]. In contrast, Noronha et al. conducted a study on 155 AML patients and found no correlation between OS and WT1 expression [28]. Similarly, Ibrahim et al. followed up 50 AML patients over 20 months and found no significant impact of WT1 on OS [22]. The difference in sample size and the ability to follow up AML patients over a longer period might confer an explanation to these discrepancies.
In our cohort, all WT1-positive patients that turned negative post-induction have achieved CR on BM examination, a finding that reflects concordance between the WT1 status and morphological response to chemotherapy. However, some patients who were considered to have achieved CR on BM examination remained WT1-positive post-induction. Given that WT1 is reported to be expressed on CD34 positive blast cells may reflect a higher sensitivity of WT1 monitoring over the morphological examination of the BM in the evaluation of treatment response and detection of residual disease after induction chemotherapy. Candoni et al. found that 24% of his AML patients who were in CR were still WT1-positive [29]. In a study of 197 AML patients, Liu et al. discovered that low and high WT1 expression is correlated with clinical remission and relapse, respectively [30]. A strong correlation between WT1 expression and BM morphological remission was also found in other studies [31,32,33].
Conclusions
WILMS tumor 1 gene expression was found to be significantly higher in AML patients than control cases, overall, our results confirmed the prognostic significance of WT1 overexpression in AML patients. Our findings support the application of MRD in AML patients based on WT1 overexpression.
Availability of data and materials
Data and materials are available upon request.
Abbreviations
- ABL:
-
Abelson
- AML:
-
Acute myeloid leukemia
- APL:
-
Acute promyelocytic leukemia
- BM:
-
Bone marrow
- BMA:
-
Bone marrow aspiration
- CD34:
-
Cluster of differentiation 34
- CR:
-
Complete remission
- CRi:
-
Complete remission with incomplete hematologic recovery
- FAB:
-
French American British
- FISH:
-
Assays for fluorescence in situ hybridization
- HiDAC:
-
High-dose cytosine arabinoside
- HAM:
-
High-dose cytosine arabinoside with mitoxantrone
- MRD:
-
Minimal residual disease
- NPM1:
-
Nucleophosmin 1
- NPV:
-
Negative predictive value
- OS:
-
Overall survival
- PB:
-
Peripheral blood
- PIF:
-
Primary induction failure
- PPV:
-
Positive predictive value
- QRT-PCR:
-
Quantitative real-time polymerase chain reaction
- ROC:
-
Receiver operating characteristic
- WT1:
-
Wilms tumor 1
References
Hourigan CS, Gale RP, Gormley NJ, Ossenkoppele GJ, Walter RB (2017) Measurable residual disease testing in acute myeloid leukaemia. Leukemia 31(7):1482–1490
Chen X, Xie H, Wood BL, Walter RB, Pagel JM, Becker PS et al (2015) Relation of clinical response and minimal residual disease and their prognostic impact on outcome in acute myeloid leukemia. J Clin Oncol 33(11):1258–1264
Tallman MS, Wang ES, Altman JK, Appelbaum FR, Bhatt VR, Bixby D et al (2019) Acute myeloid Leukemia, version 3. 2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 17(6):721–49
Cloos J, Harris JR, Janssen J, Kelder A, Huang F, Sijm G et al (2018) Comprehensive protocol to sample and process bone marrow for measuring measurable residual disease and leukemic stem cells in acute myeloid leukemia. J Vis Exp 133:e56386
Tomlinson B, Lazarus HM (2017) Enhancing acute myeloid leukemia therapy - monitoring response using residual disease testing as a guide to therapeutic decision-making. Expert Rev Hematol 10(6):563–574
Percival ME, Lai C, Estey E, Hourigan CS (2017) Bone marrow evaluation for diagnosis and monitoring of acute myeloid leukemia. Blood Rev 31(4):185–192
Thörn I, Forestier E, Botling J, Thuresson B, Wasslavik C, Björklund E et al (2011) Minimal residual disease assessment in childhood acute lymphoblastic leukaemia: a Swedish multi-centre study comparing real-time polymerase chain reaction and multicolour flow cytometry. Br J Haematol 152(6):743–753
Schnittger S, Weisser M, Schoch C, Hiddemann W, Haferlach T, Kern W (2003) New score predicting for prognosis in PML-RARA+, AML1-ETO+, or CBFBMYH11+ acute myeloid leukemia based on quantification of fusion transcripts. Blood 102(8):2746–2755
Ommen HB, Schnittger S, Jovanovic JV, Ommen IB, Hasle H, Østergaard M et al (2010) Strikingly different molecular relapse kinetics in NPM1c, PML-RARA, RUNX1-RUNX1T1, and CBFB-MYH11 acute myeloid leukemias. Blood 115(2):198–205
Krönke J, Schlenk RF, Jensen KO, Tschürtz F, Corbacioglu A, Gaidzik VI et al (2011) Monitoring of minimal residual disease in NPM1-mutated acute myeloid leukemia: a study from the German–Austrian acute myeloid leukemia study group. J Clin Oncol 29(19):2709–2716
Li H, Xing C, Zhou B, Ye H, Feng J, Wu J et al (2018) A regulatory circuitry between miR-193a/miR-600 and WT1 enhances leukemogenesis in acute myeloid leukemia. Exp Hematol 61:59–68
Schuurhuis GJ, Heuser M, Freeman S, Béné M-C, Buccisano F, Cloos J et al (2018) Minimal/measurable residual disease in AML: a consensus document from the European LeukemiaNet MRD Working Party. Blood 131(12):1275–1291
Döhner H, Estey E, Grimwade D, Amadori S, Appelbaum FR, Büchner T et al (2017) Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood 129(4):424–447
Du D, Zhu L, Wang Y, Ye X (2019) Expression of WT1 gene and its prognostic value in patients with acute myeloid leukemia. Zhejiang Da Xue Xue Bao Yi Xue Ban 48(1):50–57
Estey EH (2000) Treatment of relapsed and refractory acute myelogenous leukemia. Leukemia 14(3):476–479
Medeiros BC (2018) Interpretation of clinical endpoints in trials of acute myeloid leukemia. Leuk Res 68:32–39
Mrózek K, Harper DP, Aplan PD (2009) Cytogenetics and molecular genetics of acute lymphoblastic leukemia. Hematol Oncol Clin North Am 23(5):991–1010
Østergaard M, Olesen LH, Hasle H, Kjeldsen E, Hokland P (2004) WT1 gene expression: an excellent tool for monitoring minimal residual disease in 70% of acute myeloid leukaemia patients: results from a single-centre study. Br J Haematol 125(5):590–600
Abd-Elkodous RMA, Abo-Elenein AM, Hamam SMA (2018) Study of Wilms tumor 1 gene expression in patients with acute leukemia. Tanta Med J 46(4):255
Mossallam GI, Abdel Hamid TM, Mahmoud HK (2013) Prognostic significance of WT1 expression at diagnosis and end of induction in Egyptian adult acute myeloid leukemia patients. Hematology 18(2):69–73
Cilloni D, Gottardi E, De Micheli D, Serra A, Volpe G, Messa F et al (2002) Quantitative assessment of WT1 expression by real time quantitative PCR may be a useful tool for monitoring minimal residual disease in acute leukemia patients. Leukemia 16(10):2115–2121
Marjanovic I, Karan-Djurasevic T, Ugrin M, Virijevic M, Vidovic A, Tomin D et al (2017) Use of Wilms tumor 1 gene expression as a reliable marker for prognosis and minimal residual disease monitoring in acute myeloid leukemia with normal karyotype patients. Clin Lymphoma Myeloma Leuk 17(5):312–319
Assem M, Osman A, Kandeel E, Elshimy R, Nassar H, Ali R (2016) Clinical impact of overexpression of FOXP3 and WT1 on disease outcome in Egyptian acute myeloid Leukemia patients. Asian Pac J Cancer Prev 17(10):4699–4711
Mikhael NL, Ibrahim AM, Helmy MA, El Sheikh H (2020) Wilms’ tumor gene (WT1) expression levels as prognostic marker in pediatric acute lymphoblastic leukemia. Egypt J Haematol 45(1):35
Lane SW, Saal R, Negus S, Mollee P, Mather M, Gill D et al (2006) Characterisation and prognostic significance of WT-1 gene expression in acute myeloid leukemia (AML). Blood 108(11):2313
Galimberti S, Ghio F, Guerrini F, Ciabatti E, Grassi S, Ferreri MI et al (2010) WT1 expression levels at diagnosis could predict long-term time-to-progression in adult patients affected by acute myeloid leukaemia and myelodysplastic syndromes. Br J Haematol 149(3):451–454
Nomdedéu JF, Hoyos M, Carricondo M, Bussaglia E, Estivill C, Esteve J et al (2013) Bone marrow WT1 levels at diagnosis, post-induction and post-intensification in adult de novo AML. Leukemia 27(11):2157–2164
Noronha SA, Farrar JE, Alonzo TA, Gerbing RB, Lacayo NJ, Dahl GV et al (2009) WT1 expression at diagnosis does not predict survival in pediatric AML: a report from the Children’s Oncology Group. Pediatr Blood Cancer 53(6):1136–1139
Candoni A, De Marchi F, Zanini F, Zannier ME, Simeone E, Toffoletti E et al (2017) Predictive value of pretransplantation molecular minimal residual disease assessment by WT1 gene expression in FLT3-positive acute myeloid leukemia. Exp Hematol 49:25–33
Liu H, Wang X, Zhang H, Wang J, Chen Y, Ma T et al (2019) Dynamic changes in the level of WT1 as an MRD marker to predict the therapeutic outcome of patients with AML with and without allogeneic stem cell transplantation. Mol Med Rep 20(3):2426–2432
Válková V, Polák J, Marková M, Vítek A, Hájková H, Šálek C et al (2013) Minimal residual disease detectable by quantitative assessment of WT 1 gene before allogeneic stem cell transplantation in patients in first remission of acute myeloid leukemia has an impact on their future prognosis. Clin Transplant 27(1):E21–E29
Saito Y, Kitamura H, Hijikata A, Tomizawa-Murasawa M, Tanaka S, Takagi S et al (2010) Identification of therapeutic targets for quiescent, chemotherapy-resistant human Leukemia stem cells. Sci Transl Med 2(17):17ra9
Gray JX, McMillen L, Mollee P, Paul S, Lane S, Bird R et al (2012) WT1 expression as a marker of minimal residual disease predicts outcome in acute myeloid leukemia when measured post-consolidation. Leuk Res 36(4):453–458
Acknowledgements
Authors would like to thank all the patients and their families for participating in this project.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
NF designed the research, HD carried out the molecular genetics studies, EN recruited the patients with management and follow up and NE processed the samples and performed the statistical analysis. All authors shared in writing the manuscript, read and approved the final version of this manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The authors give thanks to all the study participants. Written consent to inclusion was obtained from all participants and they were informed of the study. The study was conducted after being authorized by the Medical Ethics Committee of Alexandria Faculty of Medicine. Reference Number Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors confirm that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Donia, H.M., Elsweify, N.M., Farahat, N.M. et al. Wilms tumor 1 gene expression in acute myeloid leukemia: prognostic significance and usefulness in minimal residual disease monitoring—a case–control study. Egypt J Med Hum Genet 23, 109 (2022). https://doi.org/10.1186/s43042-022-00291-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43042-022-00291-z