
Abstract
Purpose
To determine whether additional stem extension for stability is necessary, we performed mid-term follow-up of patients who had been managed with 5-mm metal block augmentation for a tibial defect, where tibial prosthesis was fixed using bone cement without stem extension. Also, we evaluated clinical and radiologic results including survival rate of patients without stem extension.
Methods
We retrospectively analyzed patients with tibial bone defect, had undergone primary total knee arthroplasty, and had been treated with 5-mm metal block augmentation without stem extension between March 2003 and September 2013. Among 74 patients (80 cases), 47 patients (52 cases) were followed up for at least 5 years.
Results
Mean flexion contracture improved from 8.8° (0–40°) preoperatively to 0.4° (−5° to 15°) at final follow-up (P < 0.01), but there was no significant change in the mean angle of great flexion: 124.6° (75–150°) preoperatively and 126.2° (90–145°) at final follow-up (P = 0.488). Mean range of motion improved from 115.8° (35–150°) preoperatively to 125.5° (90–145°) at final follow-up (P < 0.01). Mean knee score improved from 38.7 points (0–66 points) preoperatively to 93.2 points (79–100 points) at final follow-up (P < 0.01), and mean functional score also improved from 50.4 points (10–70 points) preoperatively to 81.8 points (15–100 points) at final follow-up (P < 0.01). The mean postoperative Western Ontario and McMaster University osteoarthritis score was 19.5 points (0–66.0 points). The mean femorotibial angle was corrected from 9.0° varus (23.0° varus–6.3° valgus) preoperatively to 5.5° valgus (2.2° varus–11.1° valgus) at final follow-up (P < 0.01). There was no change in the mean β-angle, which was 90.7° (87.2–94.9°) immediately postoperative and 90.8° (87.2–94.9°) at final follow-up (P = 0.748) and in the mean δ-angle, which was 86.2° (81.3–90.0°) immediately postoperative and 87.2° (83.1–96.5°) at final follow-up (P = 0.272). Radiolucent lines (RLL) were observed in ten cases (26.3%), and the mean RLL scores at final follow-up were 0.34 points (0–3 points) in the anteroposterior view and 0.42 points (0–6 points) in the lateral view. Scores for the RLL were ≤ 4 points in 36 cases, 5–9 points in two cases. Revision surgery due to aseptic loosening (three cases) is rarely required, and the Kaplan–Meier survival rate at 10 postoperative years was 96.4%
Conclusion
When performing 5-mm metal block augmentation for a proximal tibial defect, no additional tibial stem extension can be a good surgical option for the stability of tibial prosthetic construct and mid-term clinical and radiologic results.
Level of evidence
IV.
Similar content being viewed by others

Introduction
Total knee arthroplasty (TKA) is a treatment method for advanced knee osteoarthritis (OA) that produces good clinical outcomes and high satisfaction [1,2,3]. As knee OA progresses, it leads to a varus deformity and a bone defect develops at the proximal tibial osteotomy site. Depending on its size, depth, and location, the bone defect can be managed by the methods of bone cement filling, bone cement and metal screw fixation, bone graft, or metal wedge or metal block augmentation[4,5,6,7,8,9,10,11]. Of these, metal block augmentation has the advantage of being a relatively easy method to treat the bone defect, but is unable to restore bony structures [12]. In using metal block augmentation to treat bone defects in the proximal tibia, stem extension is often recommended to enhance the stability of the tibial prosthesis[13, 14].
However, there are several problems in using additional stem extension. In the course of operation, tibial prosthesis could not be placed on the tibial cutting surface by extended stem sometimes. Moreover, the prosthesis costs related to stem extension cause financial burden. In addition, it can cause stem tip pain, which affects patient dissatisfaction [38]. Finally, when revision surgery is needed, large bone resection might be necessary, which may be followed by low bone density and technical problems such as fixation of revision implant [39, 40].
There are no clear guidelines on additional stem extension for the tibial component stability in primary total knee arthroplasty [15] The purpose of the study is to evaluate mid-term clinical and radiologic results of patients who had been managed with 5-mm metal block augmentation for a tibial defect, where tibial prosthesis was fixed using bone cement without stem extension. The authors hypothesize that they can show good clinical and radiologic results including survival rate without using stem extension.
Materials and methods
Patient treatment and evaluation
Among patients who had undergone primary TKA by a single surgeon at our hospital between March 2003 and September 2013, we retrospectively analyzed patients whose tibial bone defect had been treated with 5-mm metal block augmentation without stem extension. The study was approved by the consent of the System Review Committee of the Human Subject Research Ethics Committee.
Before the surgery, clinical data were assessed using Knee Society Scoring system (KSS) [16]. Preoperative alignment, deformity evaluation and surgical planning [17] were performed with both knees standing anteroposterior (AP), posteroanterior (PA), lateral, merchant view and whole lower extremity standing view.
During surgery, proximal tibial osteotomy was performed to generate a 4–7° posterior tibial slope in the sagittal plane, perpendicular to the anatomical axis of the tibia in the coronal plane. Thereafter, the medial tibial defect was measured, and for patients who could be treated with 5-mm metal block augmentation, a block cutting instrument was used to perform additional osteotomy of the medial tibia. A 5-mm metal block was fixed at the medial part of the tibial prosthesis using screws. The knee prostheses used for all the cases were posterior cruciate ligament-substituting prostheses (Scorpio, 42 cases or NexGen LPS, ten cases: Table 1). Metal-backed prostheses were used in all cases, and the length of the basic stem connected to the tibial plate was 30–40 mm. Additional stem extension was not performed. The whole prosthesis, including under-surface of tibial plate, basic stem, and under-surface of 5-mm metal block, was fixed to the tibia with fully covered cementation.
After surgery we took immediate postoperative knee AP and lateral view [18] for evaluating femorotibial alignment and tibial prosthesis position. In addition, these data were used as a reference point for comparison with the image at the time of last follow-up.
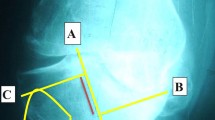
Radiologic and clinical evaluation was performed on regular outpatient visits (3 months, 6 months, 1 year, and annually) after surgery, and additional tests were performed if patients had symptoms. The clinical outcomes were assessed using the Knee Society Scoring system (KSS) and the Western Ontario and McMaster Universities (WOMAC) osteoarthritis index [19]. The American Knee Society radiological assessment method [20] was used for radiologic evaluation. The femorotibial alignment and tibial prosthesis position (β and δ angle) were checked with both knees standing AP, lateral, and whole lower extremity standing view and radiolucent line scores were evaluated with tibial prosthesis focused anteroposterior (AP) and lateral view knee fluoroscopy images.
Study population
Among 74 patients (80 cases) who underwent primary TKA using a 5-mm metal block without stem extension for their tibial defect, 9 patients (9 cases) died, 18 patients (19 cases) were lost to follow-up, and the remaining 47 patients (52 cases) were followed up for at least 5 years. For 13 of these patients (14 cases), the KSS function score and revision surgery status were confirmed by telephone contacts, while the other 34 patients (38 cases) underwent clinical and radiological assessment at final follow-up (Fig. 1). The mean age at the time of surgery was 65.0 years (40–79 years). There were 43 female patients (47 cases) and 4 male patients (5 cases), and 39 patients (44 cases) were diagnosed with OA and 8 patients (8 cases) with rheumatoid arthritis (Table 1).

Flowchart summarizing the follow-up process
Statistical analysis
Paired t-test was used for statistical comparisons of pre- and postoperative clinical and radiological outcomes. Kaplan–Meier survival analysis was used for the progress of TKA using a 5-mm metal block without stem extension, and the end point of event was defined as the time of performing the revisional surgery due to the problem of the tibial component. Statistical significance was set at P-value < 0.05. All statistical analyses were performed using IBM-SPSS v.26 software (SPSS Inc., Chicago, USA).
Results
The mean follow-up duration was 8 years, 11 months (60.6–185.3 months). All clinical and radiological results showed significant improvement between preoperative and final follow-up evaluation. The comparisons between postoperative radiological parameter and final follow-up evaluation for implant stability showed no significant difference.
Mean flexion contracture improved from 8.8° (0–40°) preoperatively to 0.4° (−5° to 15°) at final follow-up (P < 0.01), but there was no significant change in the mean angle of greatest flexion (AGF): 124.6° (75–150°) preoperatively and 126.2° (90–145°) at final follow-up (P = 0.488). Mean joint range of motion (ROM) improved from 115.8° (35–150°) preoperatively to 125.5° (90–145°) at final follow-up (P < 0.01; Table 2). Among patients with at least 5 years of postoperative follow-up, mean knee score improved from 38.7 points (0–66 points) preoperatively to 93.2 points (79–100 points) at final follow-up (P < 0.01), and mean functional score also improved from 50.4 points (10–70 points) preoperatively to 81.8 points (15–100 points) at final follow-up (P < 0.01). The mean postoperative WOMAC OA score was 19.5 points (0–66.0 points; Table 3).
For radiological outcomes of the tibial prostheses augmented with a 5-mm block, the mean femorotibial angle was corrected from 9.0° varus (23.0° varus–6.3° valgus) preoperatively to 5.5° valgus (2.2° varus–11.1° valgus) at final follow-up. There was no change in the mean β-angle, which was 90.7° (87.2–94.9°) immediately postoperative and 90.8° (87.2–94.9°) at final follow-up (P = 0.748) and in the mean δ-angle, which was 86.2° (81.3–90.0°) immediately postoperative and 87.2° (83.1–96.5°) at final follow-up (P = 0.272; Table 4).
For the patients who had been evaluated with knee fluoroscopy (38 cases), radiolucent lines around the tibial prosthesis were observed in 10 cases (26.3%), and the mean radiolucent line scores at final follow-up were 0.34 points (0–3 points) in the AP view and 0.42 points (0–6 points) in the lateral view. None of the patients showed findings that suggest instability. Scores for the radiolucent line were ≤ 4 points in 36 cases, 5–9 points in 2 cases, and ≥ 10 points in none of the cases. The areas where radiolucent lines were observed were the medial part of AP views in six cases, the lateral part of AP views in two cases, the anterior part of lateral views in five cases, and the posterior part of lateral views in one case. No radiolucent lines were observed around the stem of the tibial prosthesis (Table 5). Radiolucent lines were observed after 1 postoperative year in eight cases and after 4 postoperative years in two cases; apart from one case with rotational displacement of the tibial component where the radiolucent line score increased by 4 points after 8 postoperative years, the radiolucent lines did not progress in these cases. One case showed a high radiolucent line score of 9 points immediately after surgery and was followed up regularly, but the patient continually showed excellent clinical outcomes. Apart from this case, no case showed findings of aseptic loosening or osteolysis; therefore, no case required revision arthroplasty.
Finally, revision surgery due to aseptic loosening (three cases) is rarely required, and the Kaplan–Meier survival rate at 10 postoperative years was 96.4% (Fig. 2).

Kaplan–Meier curve analysis of primary total knee arthroplasty with a 5-mm metal block augmentation without stem extension
Discussion
The most important finding of this study is that 5-mm metal block augmentation with no additional tibial stem extension brought about good clinical and radiological results with no stability problems for the proximal tibial defect management during primary total knee arthroplasty in at least 5 years mid-term follow-up period.
In advanced OA requiring TKA, varus deformity is often observed, and in such cases, bone defects of the medial tibia are very common[21]. Depending on the location, size, and depth of the bone defect, primary TKA methods such as lateralization of the tibial prosthesis, cement filling [10], bone grafting [4, 8], or metal block augmentation are used to treat the medial tibial bone defect, and metal augmentation is one of the easiest of these methods [12]. Because metal block augmentation involves removal of the defective site, the bone mass cannot be restored; on the other hand, potential problems with bone graft such as incorporation failure or collapse, are not expected [22]. Lee and Choi [12] reported favorable outcomes at a 5-year follow-up, and Tsukada et al. [23] reported that clinical results of total knee arthroplasty with metal augmentation showed no differences compared with those without bone defects.
There are some doubts whether the basic tibial prostheses designed for the primary TKA might have stability problems caused by partial modification with metal block attachment. Therefore, additional tibial stem extension has been suggested for the increasing stability when metal block augmentation is attached to the tibial component. Stem extension is expected to enhance the stability [12, 24, 25] because it can provide shear force resistance [26], reduce tibial lift-off [27], and mitigate micromotion [28]. The length of stem extension has been reported to influence stability [29,30,31,32]; hence, when performing metal block augmentation of a tibial prosthesis, stem extension is recommended [13, 14].
However, there have also been reports that, when an eccentric load is applied in stem extension, micromotion increases; therefore, stem extension does not increase initial stability in TKA [31, 33]. As loading on the proximal tibia is reduced, the bone density also decreases [26] due to the stress shielding effect occurs along the stem. This in turn increases the risk of subsidence, loosening, and periprosthetic fracture [34]. Meanwhile, when stress is focused on the stem tip, it can lead to stem tip pain [34, 35]. Additional problems that need to be considered are the heightened risk of fat embolism during intramedullary manipulation and implant placement for an intramedullary stem extension, increased prosthesis costs due to the metal block and stem, and clinically, potential loss of bone quality and difficulties of stem removal in a future revision surgery.
In a biomechanical study that assessed metal block augmentation and stem extension for proximal tibial defects, performing a stem extension was reported to produce favorable outcomes compared with using only the metal block [15]. However, that study had certain limitations: it included only relatively large bone defects, it used a 10-mm metal block augmentation, and the stability results were assessed at time zero state and applied on the synthetic bone rather than real bony structure. When using a cement fixation method for tibial prosthesis, cementation of the tibial cutting surface only and cementation that also includes the tibial stem are known to show differences in stability. Cawley et al. [36] pointed out that, even though full cementation of the surface and stem provided excellent initial stability, there was a risk of proximal tibial bone resorption with time because there was a lot of stress shielding. Therefore, the stability at time zero is not the ultimate measurement in typical patients, and with time, it is also important to monitor for aseptic loosening indicated by bony absorption in the proximal tibia.
From the results of this study, there were positive outcomes in clinical parameter including flexion contracture, ROM and KSS at final follow-up among primary TKA patients who underwent 5-mm block augmentation without stem extension and were available for at least 5 years of follow-up. And there was no change in β-angle or δ-angle after a mean of 9 years of follow-up compared to angles measured immediately after surgery. Radiolucent line scores around the tibial implant, investigated by fluoroscopy, were mostly ≤ 4 points at final follow-up, indicating sustained stability.
Among the 47 patients (52 cases) who were followed up for at least 5 years, there were 3 cases related to revision surgery; 1 case in which revision surgery was performed, 1 case in which revision surgery was advised, and 1 case in which continuous observation was advised. In the case where revision surgery was performed, there were no clinical and radiological signs of loosening during 4 postoperative years. However, at 13 postoperative years, the patient underwent revision surgery for aseptic loosening at the other hospital. Also, in the case where revision surgery was advised, there were no signs of loosening for up to 7 postoperative years. But at 8 postoperative years, revision surgery was advised due to rotational displacement of the tibial component.
In this study, revision surgery was recommended in 3 cases and the Kaplan–Meier survival rate for 10 years after surgery was 96.4%, which is not much different from 97%, the 10-year survival rate of primary TKA reported by Nugent et al. [37], and 95.3% reported by Khaw et al. [41]. However, since comparative analysis of survival rates has not been conducted, studies using statistical techniques such as log-rank test should be conducted to see if there is a difference in survival rates according to the implementation of stem extension.
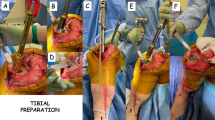
Among the cases, one patient is under the continuous monitoring for 9 points of the radiolucent line score, noticed immediate postoperative state, but there was still no interval changes in the radiolucent line scores till 90 postoperative months and the clinical outcomes were excellent (knee score 100, function score 90). So this patient is still followed up very closely. The other patient who underwent 5-mm metal block augmentation without stem extension in her primary TKA revised only the femoral component at 11.5 postoperative years. However, the tibial component showed good stability (Fig. 3) in the revision procedure. After the femoral component revision surgery, the patient continued to show excellent knee/function scores and no radiolucent line around the tibial prosthesis. Therefore, we concluded that, in primary TKA patients, a 5-mm metal block augmentation of tibial bone defects without stem extension can provide stability in 5-year postoperative outcomes.

A, B Preoperative fluoroscopy on right knee (post-operative day (POD) POD#11.5 years); C, D postoperative fluoroscopy on right knee (POD#12.8 years); E intraoperative clinical photo on revision TKA on right knee (POD#11.5 years)
This study was conducted to answer the question of the necessity of stem extension for metal block augmentation of medial defects on the basis of clinical outcomes after at least 5 years of follow-up. We were able to demonstrate that, in mid-term follow-up of at least 5 years and an average of 9 years, no additional stem extension is required to the 30–40 mm basic length tibial stem plate for the stability with fully cemented tibial component when performing 5-mm metal block augmentation in primary TKA.
However, this study also had several limitations. First, since this study is a case series for patients who underwent 5-mm metal block augmentation without stem extension, it was possible to confirm improvement in clinical and radiological results compared with before surgery. However, it reveals the limitations of not performing non-inferiority test because there is no comparison group with stem extension.
Second, we only evaluate no additional tibial stem extension cases for the focal proximal tibial defect, which is managed with 5-mm metal block augmentation. So, our results may not be applied to the situation of generalized poor bone quality on the proximal tibia.
Third, there were relatively many patients who could not receive clinical and radiation follow-up measures due to the long data collection period, especially elderly patients who died or had other accompanying diseases. This also has a limitation in that selection bias may appear because there are patients who have been eliminated during long period.
Conclusion
When performing TKA, 5-mm metal block augmentation can be used to deal with uncontained bone defects less than 5-mm depth. If the tibial component with 30–40 mm basic stem was fixed through full cementation, the additional tibial stem extension was not mandatory for the stability of tibial prosthesis and mid-term clinical and radiologic results. Therefore, when performing 5-mm metal block augmentation for a proximal tibial defect, no additional tibial stem extension can be a good surgical option.
Abbreviations
- TKA:
-
Total knee arthroplasty
- OA:
-
Osteoarthritis
- KSS:
-
Knee Society Scoring system
- WOMAC:
-
Western Ontario and McMaster Universities
- AP:
-
Anteroposterior
- AGF:
-
Angle of greatest flexion
- ROM:
-
Range of motion
- RLL:
-
Radiolucent line
References
Polascik BW, Bin Abd Razak HR, Chong H-C, Lo N-N, Yeo S-J (2018) Acceptable functional outcomes and patient satisfaction following total knee arthroplasty in Asians with severe knee stiffness: a matched analysis. Clin Orthop Surg 10:337–343
Lee SH, Kim DH, Lee YS (2021) Is there an optimal age for total knee arthroplasty? A systematic review. Knee Surg Rel Res 32:60
Choi YJ, Seo DK, Lee KW, Ra HJ, Kang HW, Kim JK (2021) Result of total knee arthroplasty for painless stiff knees. Knee Surg Rel Res 32:61
Altchek D, Sculco TP, Rawlins B (1989) Autogenous bone grafting for severe angular deformity in total knee arthroplasty. J Arthroplasty 4:151–155
Brand MG, Daley RJ, Ewald FC, Scott RD (1989) Tibial tray augmentation with modular metal wedges for tibial bone stock deficiency. Clin Orthop 248:71–79
Elia EA, Lotke PA (1991) Results of revision total knee arthroplasty associated with significant bone loss. Clin Orthop 114–121
Engh GA, Ammeen D (1999) Results of total knee arthroplasty with medial epicondylar osteotomy to correct varus deformity. Clin Orthop 141–148
Fipp GJ (1989) A bone grafting technique in reconstructive joint arthroplasty. J Arthroplasty 4:285–287
Harris AI, Poddar S, Gitelis S, Sheinkop MB, Rosenberg AG (1995) Arthroplasty with a composite of an allograft and a prosthesis for knees with severe deficiency of bone. J Bone Joint Surg Am 77:373–386
Ritter MA, Keating EM, Faris PM (1993) Screw and cement fixation of large defects in total knee arthroplasty: a sequel. J Arthroplasty 8:63–65
Song I-S, Sun D-H, Chon J-G, Jang S-W, Sun D-H (2014) Results of revision surgery and causes of unstable total knee arthroplasty. Clin Orthop Surg 6:165–172
Lee JK, Choi CH (2011) Management of tibial bone defects with metal augmentation in primary total knee replacement: a minimum five-year review. J Bone Joint Surg Br 93:1493–1496
Cuckler JM (2004) Bone loss in total knee arthroplasty: graft augment and options. J Arthroplasty 19:56–58
Murray PB, Rand JA, Hanssen AD (1994) Cemented long-stem revision total knee arthroplasty. Clin Orthop 309:116–123
Hashemi A, Ziada S, Adili A, de Beer J (2014) Stem requirements of tibial augmentations in total knee arthroplasty. Exp Tech 38:8–17
Insall JN, Dorr LD, Scott RD, Scott WN (1989) Rationale of the Knee Society clinical rating system. Clin Orthop 248:13–14
Song SJ, Park CH, Bae DK (2019) What to know for selecting cruciate-retaining or posterior-stabilized total knee arthroplasty. Clin Orthop Surg 11:142–150
Park J-K, Seon J-K, Cho K-J, Lee N-H, Song E-K (2018) Is immediate postoperative mechanical axis associated with the revision rate of primary total knee arthroplasty? A 10-year follow-up study. Clin Orthop Surg 10:167–173
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW (1988) Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol
Ewald FC (1989) The Knee Society total knee arthroplasty roentgenographic evaluation and scoring system. Clin Orthop 248:9–12
Rand JA (1991) Bone deficiency in total knee arthroplasty. Use of metal wedge augmentation. Clin Orthop 271:63–71
Hamai S, Miyahara H, Esaki Y, Hirata G, Terada K, Kobara N et al (2015) Mid-term clinical results of primary total knee arthroplasty using metal block augmentation and stem extension in patients with rheumatoid arthritis. BMC Musculoskel Dis 16:225
Tsukada S, Wakui M, Matsueda M (2013) Metal block augmentation for bone defects of the medial tibia during primary total knee arthroplasty. J Orthop Surg Res 8:36
Radnay CS, Scuderi GR (2006) Management of bone loss: augments, cones, offset stems. Clin Orthop 446:83–92
Rawlinson JJ, Closkey RF, Davis N, Wright TM, Windsor R (2008) Stemmed implants improve stability in augmented constrained condylar knees. Clin Orthop 466:2639–2643
Scott C, Biant L (2012) The role of the design of tibial components and stems in knee replacement. J Bone Joint Surg Br 94:1009–1015
Lonner JH, Klotz M, Levitz C, Lotke PA (2001) Changes in bone density after cemented total knee arthroplasty: influence of stem design. J Arthroplasty 16:107–111
Rawlinson JJ, Peters LE, Campbell DA, Windsor R, Wright TM, Bartel DL (2005) Cancellous bone strains indicate efficacy of stem augmentation in constrained condylar knees. Clin Orthop 440:107–116
Murase K, Crowninshield RD, Pedersen DR, Chang T-S (1983) An analysis of tibial component design in total knee arthroplasty. J Biomech 16:13–22
Reilly D, Walker P, Ben-Dov M, Ewald F (1982) Effects of tibial components on load transfer in the upper tibia. Clin Orthop 165:273–282
Stern SH, Wills RD, Gilbert JL (1997) The effect of tibial stem design on component micromotion in knee arthroplasty. Clin Orthop 345:44–52
Wright J, Ewald F, Walker P, Thomas W, Poss R, Sledge C (1990) Total knee arthroplasty with the kinematic prosthesis. Results after five to nine years: a follow-up note. J Bone Joint Surg Am 72:1003–1009
Barrack RL, Rorabeck C, Burt M, Sawhney J (1999) Pain at the end of the stem after revision total knee arthroplasty. Clin Orthop 367:216–225
Pérez-Blanca A, Prado M, Ezquerro F, Montañéz E, Espejo A (2008) Addition of a short central extension to surface cemented tibial trays in primary TKA: an in vitro study of the effect on initial fixation stability and its relationship to supporting bone density. Clin Biomech 23:483–492
McLean AJ (2007) The effect of modular stems and cement fixation techniques on the initial stability of the tibial prosthesis and the strain distribution within the proximal tibia in primary and revision total knee arthroplasty. Dissertation, University of Edinburgh
Cawley DT, Kelly N, Simpkin A, Shannon FJ, McGarry JP (2012) Full and surface tibial cementation in total knee arthroplasty: a biomechanical investigation of stress distribution and remodeling in the tibia. Clin Biomech 27:390–397
Nugent M, Wyatt MC, Frampton CM, Hooper GJ (2019) Despite improved survivorship of uncemented fixation in total knee arthroplasty for osteoarthritis, cemented fixation remains the gold standard: an analysis of a national joint registry. J Arthroplasty 34(8):1626–1633
Kim MS, Koh IJ, Sohn S, Park HC, In Y (2020) Modified hybrid cementing technique reduces stem tip pain and improve patient’s satisfaction after revision total knee arthroplasty. J Orthop Surg Res 15:393
Pasquier GJM, Huten D, Common H, Migaud H, Putman S (2020) Extraction of total knee arthroplasty intramedullary stem extensions. Orthop Traumatol Surg Res 106:S135–S147
Filip AC, Cuculic SA (2022) Tibial stem extension versus standard configuration in total knee arthroplasty: a biomechanical assessment according to bone properties. Medicina 58(5):634
Khaw FM, Kirk LM, Morris RW, Gregg PJ (2002) A randomised, controlled trial of cemented versus cementless press-fit condylar total knee replacement. Ten-year survival analysis. J Bone Joint Surg Br 84(5):658–666
Acknowledgements
None.
Funding
This study had no funding.
Author information
Authors and Affiliations
Contributions
J.J.R. carried out the acquisition of data and drafting the manuscript. Y.H.K. participated in the partial drafting manuscript and statistical analysis. C.H.C. made substantial contribution to conception and study design, helped to draft the manuscript, and gave the final approval for the version to be published. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the Institutional Review Board on Human Subjects Research and Ethics Committee of Hanyang University Hospital, Seoul, Korea (ID number 2020-04-026-003).
Consent for publication
Informed consent was obtained from all individual participants included in the study.
Competing interests
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Ryu, J.J., Kim, Y.H. & Choi, C.H. The additional tibial stem extension is not mandatory for the stability of 5 mm metal block augmented tibial prosthesis construct in primary total knee arthroplasty: 5-year minimum follow-up results. Knee Surg & Relat Res 35, 5 (2023). https://doi.org/10.1186/s43019-023-00174-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43019-023-00174-6