
Abstract
Background
Although the mean arterial pressure (MAP) target of 65 mmHg was achieved, diastolic blood pressure (DBP) was still low in some septic shock patients. The effects of DBP on the prognosis and optimal target for patients with septic shock are unclear. We sought to investigate the relationship between DBP and 28-day mortality in septic shock patients.
Methods
In this retrospective observational study, we obtained data from the Chinese Database in Intensive Care (CDIC). We included patients with an admission diagnosis of septic shock and shock was controlled. DBP was measured every 1 h, and the mean DBP during the first 24 h (mDBP24h) was recorded. The primary outcome was 28-day mortality. Multivariable logistic regression determined the relationship between mDBP24h and 28-day mortality.
Results
In total, 1251 patients were finally included. The 28-day mortality of included septic shock patients was 28.3%. The mDBP24h, not mSBP24h, was higher among 28-day survivors compared with non-survivors. 28-day mortality was inversely associated with mDBP24h (unadjusted OR 0.814 per 10 mmHg higher mDBP24h, P = 0.003), with a stepwise increase in 28-day mortality at lower mDBP24h. The 28-day mortality of patients with mDBP24h < 59 mmHg had an absolute risk reduction of 9.4% (P = 0.001). And mDBP24h < 59 mmHg was the remaining high risk factor inversely associated with 28-day mortality after multivariable adjustment (adjusted OR 1.915, 95% CI 1.037–3.536, P = 0.038), while mMAP24h and mSBP24h were not.
Conclusion
In patients with septic shock after initial resuscitation, we observed an inverse association between mDBP24h and 28-day mortality. The poor outcomes in patients with mDBP24h < 59 mmHg provide indirect evidence supporting a further DBP goal of 59 mmHg for patients with septic shock after MAP of 65 mmHg was achieved.
Similar content being viewed by others


Background
Septic shock is the most common form of circulatory shock in intensive care units [1]. And septic shock is considered a leading causes of death for critical patients worldwide [2]. A cross-section survey study of forty-four ICUs in mainland China showed that septic shock accounted for 53.3% of all sepsis patients, while 90-day mortality was up to 51.94% [3]. Thus, the surviving sepsis campaign bundle including fluid resuscitation are the most important therapeutic measures to ensure adequate tissue perfusion and prevent poor outcomes in patients with septic shock [4,5,6]. Initially, maintaining a mean arterial pressure (MAP) greater than 65 mmHg as part of the early fluid resuscitations has been always recommended by the surviving sepsis campaign guidelines [4, 6]. However, even then the target of MAP was achieved, the mortality of septic patients was high [7, 8], indicating that simply reaching the MAP target value is inadequate.
Although a MAP of 65 mmHg was achieved, some patients with septic shock had low diastolic blood pressure (DBP) [9, 10]. DBP is a good marker of vascular tone and upstream pressure for the coronary perfusion. It has been confirmed that low level of DBP, not systolic blood pressure and MAP, was the independent predictor of early progression to septic shock [11], associated with the development of acute kidney injury (AKI) [12, 13], and significantly associated with in-hospital mortality [14, 15]. DBP has been recommended as a trigger to start norepinephrine (NE) treatment while cooperated with MAP in the early resuscitation of septic shock [16, 17]. Considering the clinical relationships between the DBP level and sepsis progression, maintaining a suitable DBP level could be crucial and have immediate effect on prognosis in patients with septic shock.
Given the lack of clinical evidence of specific DBP target levels in septic shock patients, we sought to describe the relationship between DBP and 28-day mortality among patients with septic shock. We hypothesized that 28-day mortality among patients with septic shock would increase as a function of lower DBP and that a threshold DBP may be identified as an optimal DBP range.
Methods
Study population
We conducted a retrospective observational study in which the data were extracted from the Chinese Database in Intensive Care (CDIC). The latest CDIC contains about 7,000 admitted to the Department of Crit Care Medicine, Zhongda Hospital, Southeast University, China, from January 2016 to July 2022. Patients in CDIC with septic shock diagnosis within 24 h after ICU admission and shock control were eligible for inclusion. The diagnosis of septic shock was consistent with the third international consensus definitions for sepsis and septic shock (Sepsis-3) [18]. Shock control was defined as achievement of sustained mean arterial blood pressure of at least 65 mmHg, together with urine flow at least 0.5 ml/kg/h for two consecutive hours, or decreased serum lactate great than or equal to 10% from baseline by 6 h after septic shock diagnosis [19]. We only included the first intensive Care Unit (ICU) admission of each patients and excluded patients younger than 18 years, died in the first 24 h after ICU admission, accompanied by moderate or severe aortic valve insufficiency.
The present study was approved by the Research Ethics Commission of Zhongda Hospital Southeast University which certified that the present study was performed in accordance with all required guidelines and regulations (2023ZDSYLL004-P01).
Data collection and outcome
All demographic data including age, gender, source of infection, chronic comorbidities, vital sign, laboratory, clinical and outcome data were collected. We included the worst values of laboratory test data in the first 24 h after septic shock admission diagnosis. Vital signs containing DBP, systolic blood pressure (SBP), MAP, heart rate (HR), and central venous pressure (CVP) were all recorded every 1 h. Blood pressure of septic shock patients was preferentially recorded from invasive arterial blood pressure monitoring methods, and otherwise from noninvasive methods. The mean DBP during the first 24 h (mDBP24h) was calculated as the mean recorded values of the first 24 h after septic shock admission diagnosis. The other vital signs (mMAP24h, mSBP24h, mHR24h, mCVP24h) calculation methods are the same as mDBP24h.
The vasoactive-Inotropic Score (VIS) was calculated by peak vasopressor and inotrope doses during the first 24 h of septic shock diagnosis (in mcg/kg/min): VIS = dobutamine + dopamine + (10 * phenylephrine + milrinone) + (100 * [epinephrine + norepinephrine]) + (10,000 * units/kg/min vasopressin). And one VIS is considered equal to 1 mcg/kg/min of dobutamine or dopamine or 0.01 mcg/kg/min of epinephrine or norepinephrine [20].
The primary outcome in the CDIC derivation was 28-day mortality. We also recorded other outcome data, such as new mechanical ventilation (MV) and continuous renal replacement therapy (CRRT) during ICU stay, length of ICU and hospital stay, ICU and hospital mortality.
Statistical analysis
Continuous variables are presented as medians [interquartile ranges (IQRs)] and the Mann–Whitney U test was used for comparison in groups. Categorical variables are expressed as number (percentage), and Pearson χ2 test is used to compare between groups. The number of missing or censoring values are presented in Additional file 1: Table S1. Variables with more than 25% missing ratio were excluded [21]. Outliers were censored, and missing data of less than 25% were replaced with the sequence mean value.
Logistic regression was used to find the association between mDBP24h and 28-day mortality before and after adjusting for age, gender, Acute Physiology and Chronic Health Evaluation II (APACHE II), peak VIS of the first 24 h after ICU admission. We use the area under the receiver-operator characteristic (AUC, c-statistic) value, and use the Youden’s J index to define the optimal cutoff value. The 28-day survival was evaluated using the Kaplan–Meier survival analysis and Cox proportional-hazards analysis. Two-tailed P-value < 0.05 was considered as statistical significance. Analyses were performed by IBM SPSS statistic 25.
Results
Study population
The CDIC included 6997 unique ICU patient admissions, and 1548 patients both met septic shock diagnosis and shock control definition, then 297 was excluded due to the exclusion criteria (Fig. 1). The mean age of 1251 patients with septic shock was 68.0 years (55.0–78.0), including 67.5% males. The median Acute Physiology and Chronic Health Evaluation II score (APACHE II) was 19.0 (14.0–25.0). Lung was the leading cause of infection (50.7%).

Flow of screening the shock controlled patients after ICU admission of septic shock
The 28-day mortality of the septic shock patients enrolled was 28.3%. Compared with septic shock patients in 28-day survival group, the APACHE II and SOFA score were significantly increased in the 28-day non-survival group (P < 0.001). The proportion of patients using vasoactive drugs and VIS was similar between the two groups. However mDBP24h and mMAP24h was significantly lower in 28-day non-survival group, while mSBP24h was similar (Table 1).
A total of 67 (5.4%) patients had a mDBP24h < 50 mmHg, 386 (30.9%) patients had a mDBP24h 50–60 mmHg, 512 (40.9%) patients mDBP24h 60–70 mmHg, 238 (19.0%) patients mDBP24h 70–80 mmHg, and 48 (3.8%) patients a mDBP24h ≥ 80 mmHg. Compared with low mDBP24h group patients, the high mDBP24h group had less illness severity, decreased norepinephrine used proportion and VIS, and also had decreased levels of creatinine, fewer CRRT and mechanical ventilation (Table 2).
Association between mDBP24h and 28-day mortality
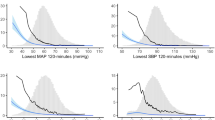
The 28-day mortality of the included septic shock patients was 28.3%. Crude 28-day mortality of septic shock patients was gradually decreased with the increased of mDBP24h (41.8% vs. 31.9% vs. 25.0% vs. 28.2% vs. 16.7%, P = 0.006) (Fig. 2 and Additional file 2: Table S2). The mDBP24h was inversely associated with 28-day mortality (unadjusted OR 0.814 per 10 mmHg higher mDBP24h, 95%CI 0.711–0.933, P = 0.003; optimal cutoff 58.9 mmHg) (Fig. 3). Similar findings were observed in the relationship of mDBP24h with ICU mortality and hospital mortality (Additional file 2: Table S2, Additional file 6: Figure S1). The mDBP24h was also inversely associated with ICU mortality (unadjusted OR 0.845 per 10 mmHg higher mDBP24h, 95%CI 0.735–0.971, P = 0.018; optimal cutoff 58.5 mmHg).

28-day mortality as a function of the mDBP24h of septic shock controlled patients

The mDBP24h was inversely associated with 28 days mortality (unadjusted OR 0.814 per 10 mmHg higher mDBP24h, 95% CI 0.711–0.933, P = 0.003)
The patients were further divided into two groups according to whether the mDBP24h was less than 59 mmHg. Compared with patients with mDBP24h ≥ 59 mmHg, patients with mDBP24h < 59 mmHg had older age, higher APACHE score, higher serum creatinine, lower levels of central venous oxygen saturation, more patients received mechanical ventilation and renal replacement therapy, and had higher ICU and hospital mortality (Additional file 3: Table S3). We analyzed the relationship between mDBP24h and 28-day mortality in patients with mDBP24h < 59 mmHg group. There is no correlation between DBP and mortality in the DBP impaired (mDBP24h < 59 mmHg) group, OR 0.964 (95%CI 0.925–1.003, P = 0.073), which may be related to the small sample size.
The 28-day mortality of patients with mDBP24h < 59 mmHg had an absolute risk reduction of 9.4% (P = 0.001) (Fig. 4). After multivariable adjustment, mDBP24h < 59 mmHg remained inversely associated with 28-day mortality (adjusted OR 1.915, 95% CI 1.037–3.536, P = 0.038), while mMAP24h and mSBP24h was not associated with 28-day mortality (Table 3). The worst DBP in the first 24 h was also an independent factor of 28-day mortality (Additional file 4: Table S4).

Probability of survival in septic shock patients through Day 28. The graph shows the Kaplan–Meier estimates for the probability of survival among septic shock patients with low DBP (mDBP24h < 59 mmHg) and high DBP (mDBP24h ≥ 59 mmHg) level. The P-value was calculated with the use of the log-rank test
Compared with patients with mDBP24h < 60 mmHg, the likelihood of 28-day survival rate of patients with mDBP24h in 60–70 mmHg (OR 1.500 [1.134–1.984], P = 0.004) and great than or equal to 80 mmHg had all significantly increased (OR 2.500 [1.142–5.475], P = 0.022) (Table 4).
The duration of mDBP24h < 60 mmHg in the first 24 h was divided according to the interquartile range. Patients with septic shock in the first quartile had the lowest 28-day mortality, indicating that the longer duration of mDBP24h < 60 mmHg, the higher the 28-day mortality was (P = 0.020) (Fig. 5). In contrast, the longer maintained mDBP24h in 60–70 mmHg during the first 24 h, the lower the 28-day mortality was (P = 0.009) (Additional file 7: Figure S2). While in other mDBP24h ranges, there was no significant difference in mortality among different mDBP24h duration (Additional file 5: Table S5).

28-day mortality of different interquartile intervals with mDBP24h less than 60 mmHg duration (Time-IQR1: ≤ 2 h, Time-IQR2: 2–8 h, Time-IQR3: 8–15 h, Time-IQR4: ≥ 15 h) IQR: interquartile range
The subgroup analysis of relationship between mDBP24h ≥ 59 mmHg and 28-day mortality showed that among the septic shocks patients who were younger than 65 years, underlying hypertension, APACHE II above 20, and P/F ratio less than or equal to 187 mmHg, mDBP24h ≥ 59 mmHg was more relevant to 28-day survival (Fig. 6). Similar subgroup results were found in the relationship between mDBP24h, mMAP24h and 28-day survival, but not in mSBP24h subgroup analysis (Additional file 8: Figure S3).

Subgroup analysis of the association between 28-day mortality and mDBP24h ≥ 59 mmHg in septic shock patients
Discussion
In this retrospective study of a large tertiary ICU septic shock controlled patients, we demonstrate that mDBP24h is inversely associated with 28-day mortality. The septic shock controlled patients who were able to maintain a mDBP24h great than or equal to 59 mmHg had lower 28-day mortality. Among those patients with a mDBP24h blow 59 mmHg, they had more severely illness condition and higher 28-day mortality. These data also suggest that mDBP24h, not mMAP24h and mSBP24h, was an independent predictor of 28-day mortality.
Surviving Sepsis Campaign guidelines recommended targeting a MAP of 65 mmHg in the initial resuscitation of septic shock patients [4]. However, even if septic shock patients get the MAP target above 65 mmHg, the 90-day mortality was still around 40% [8, 22]. Numerous studies have confirmed that there are still microcirculation disorders after shock resuscitation [23, 24]. DBP was the only independent microcirculatory determinant of tissue oxygen saturation resaturation (resStO2) [25], which was measured by Near infrared spectrometry as one of the main studied microcirculation parameters and strongly associated with outcome in sepsis patients [26, 27]. The findings of our study, which showed a higher DBP target (≥ 59 mmHg) in septic shock controlled patients was associated with lower lactate levels and better prognosis, may indirectly support the view of a correlation between DBP and microcirculation perfusion.
Vasodilation is an important pathophysiological feature and plays a key role in the progression of hypotension and tissue hypoperfusion in septic shock [28]. Considering DBP is a good marker of arterial tone, a low DBP in patients with septic shock detected at peripheral vessels should reflect the systemic vasodilation [10]. A retrospective cohort study indicated that DBP lower than 52 mmHg of nonsevere sepsis patients at emergence department(ED) triage (OR 4.59; 95% CI 1.57–13.39) was independently predict early progression to severe sepsis or septic shock within 96 h of ED presentation [11]. Other trials showed that low DBP was associated with the development of severe AKI [13]. And DBP within 24 h admission, not MAP, was a potential important hemodynamic target for preventing AKI in ICU patients [12]. Further studies proved that DBP, but not SBP, was one of the independent positive predictive factors of ICU patients’ outcome [14, 15, 29]. We also found that the serum creatinine was significantly higher in the low mDBP24h group and a strong independent association between mDBP24h and mortality.
Another physiological feature of DBP is a determinant of coronary perfusion. More than 50% of patients with septic shock have evidence of a reduced coronary flow blood reserve, which is a predictor of ICU mortality in septic shock [30]. A low DBP may impair the myocardial perfusion, especially in the case of tachycardia [31]. Our study showed that myoglobin was significantly higher in the low mDBP24h group, suggesting that low DBP may be associated with myocardial ischemia. SPRINT data confirmed that a DBP lower than 50 mmHg was significantly associated with increased cardiovascular events in patients with 50 years older and a screening SBP of 130 to 180 mmHg [32]. And a DBP lower than 70 mmHg was significantly associated with mortality of patients with coronary artery disease [33]. A national cross-sectional survey showed that 39.6% and 17.0% of sepsis patients, respectively, had underlying hypertension and coronary artery disease in Chinese ICUs [3]. Therefore, a low DBP level during treatment for septic shock may significantly increase the risk of cardiovascular events.
The possible pathophysiological mechanisms of low DBP and high mortality are as follows: first, low DBP indicates more obvious vasodilation, which will lead to tissue hypoperfusion [10, 13]; second, low DBP will lead to reduced coronary blood flow and increase cardiovascular adverse events [30, 33]; the last one, low DBP is associated with impaired microcirculation [25]. Therefore, we need to further correct low DBP even after MAP target is achieved.
European Society of Intensive Care Medicine recommended that the combination of MAP (60–65 mmHg) and DBP (> 40 mmHg) targets should be considered as trigger to start vasopressor treatment in septic shock [17]. The flow diagram of initial resuscitation of sepsis induced hypotension or serum lactate ≥ 4 mmol/L suggested that we should initiated noradrenaline infusion along with the 30 ml/kg fluid bolus when DBP is lower than 50 mmHg [34]. However, these DBP cutoff values were either based of experts practice or the estimated value corresponded with a MAP of 65 mmHg and a SBP of 90 mmHg, and were not supported by clinical studies. Our findings supported that the mDBP24h should be raised to a higher pressure level (≥ 59 mmHg) in the first 24 h of patients with septic shock controlled after initial resuscitation, showing it was associated with the illness severity and mortality benefit.
Limitations
This retrospective study has a number of inherent limitations we should acknowledge. First, the missing data could bias the results and also other possible residual confounders due to single-center retrospective design, Second, patients were retrospectively enrolled from a single center which may impede the generalization of the results. The results of this single-center retrospective study need further studies to confirm. Third, this observational study could not lead to causal inferences for any associations. Finally, the mDBP24h may include both noninvasive and invasive arterial pressure, and we could not distinguish the source of DBP measurements.
Conclusions
There was an inverse correlation between DBP in the first 24 h and 28-day mortality among septic shock controlled patients admitted to the ICU. Patients with a mDBP24h less than 59 mmHg during the first 24 h after septic shock controlled had an increased risk of 28-day mortality. These findings provide indirect support for a DBP target of 59 mmHg for septic shock controlled patient in ICU. More high quality prospective or randomized controlled studies are needed to further validate the DBP target in septic shock patients.
Availability of data and materials
The data in CDIC used and analyzed in the current study are available from the corresponding author on reasonable request.
Abbreviations
- AKI:
-
Acute kidney injure
- CDIC:
-
Chinese Database in Intensive Care
- DBP:
-
Diastolic Blood Pressure
- mDBP24h :
-
Mean diastolic blood pressure during the first 24 h of septic shock diagnosis
- MAP:
-
Mean arterial pressure
- VIS:
-
Vasoactive-Inotropic Score
References
Vincent JL, De Backer D. Circulatory shock. N Engl J Med. 2013;369(18):1726–34. https://doi.org/10.1056/NEJMra1208943.
Rudd KE, Johnson SC, Agesa KM, Shackelford KA, Tsoi D, Kievlan DR, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395(10219):200–11. https://doi.org/10.1016/S0140-6736(19)32989-7.
Xie J, Wang H, Kang Y, Zhou L, Liu Z, Qin B, et al. The epidemiology of sepsis in Chinese ICUs: a national cross-sectional survey. Crit Care Med. 2020;48(3):e209–18. https://doi.org/10.1097/CCM.0000000000004155.
Evans L, Rhodes A, Alhazzani W, Antonelli M, Coopersmith CM, French C, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Crit Care Med. 2021;49(11):e1063–143. https://doi.org/10.1097/CCM.0000000000005337.
Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017;43(3):304–77. https://doi.org/10.1007/s00134-017-4683-6.
Levy MM, Evans LE, Rhodes A. The surviving sepsis campaign bundle: 2018 update. Crit Care Med. 2018;46(6):997–1000. https://doi.org/10.1097/CCM.0000000000003119.
Lamontagne F, Meade MO, Hebert PC, Asfar P, Lauzier F, Seely AJE, et al. Higher versus lower blood pressure targets for vasopressor therapy in shock: a multicentre pilot randomized controlled trial. Intensive Care Med. 2016;42(4):542–50. https://doi.org/10.1007/s00134-016-4237-3.
Asfar P, Meziani F, Hamel JF, Grelon F, Megarbane B, Anguel N, et al. High versus low blood-pressure target in patients with septic shock. N Engl J Med. 2014;370(17):1583–93. https://doi.org/10.1056/NEJMoa1312173.
Hamzaoui O, Teboul JL. Importance of diastolic arterial pressure in septic shock: PRO. J Crit Care. 2019;51:238–40. https://doi.org/10.1016/j.jcrc.2018.10.032.
Ospina-Tascon GA, Teboul JL, Hernandez G, Alvarez I, Sanchez-Ortiz AI, Calderon-Tapia LE, et al. Diastolic shock index and clinical outcomes in patients with septic shock. Ann Intensive Care. 2020;10(1):41. https://doi.org/10.1186/s13613-020-00658-8.
Holder AL, Gupta N, Lulaj E, Furgiuele M, Hidalgo I, Jones MP, et al. Predictors of early progression to severe sepsis or shock among emergency department patients with nonsevere sepsis. Int J Emerg Med. 2016;9(1):10. https://doi.org/10.1186/s12245-016-0106-7.
Legrand M, Dupuis C, Simon C, Gayat E, Mateo J, Lukaszewicz AC, et al. Association between systemic hemodynamics and septic acute kidney injury in critically ill patients: a retrospective observational study. Crit Care. 2013;17(6):R278. https://doi.org/10.1186/cc13133.
Deep A, Sagar H, Goonasekera C, Karthikeyan P, Brierley J, Douiri A. Evolution of acute kidney injury and its association with systemic hemodynamics in children with fluid-refractory septic shock. Crit Care Med. 2018;46(7):e677–83. https://doi.org/10.1097/CCM.0000000000003156.
Benchekroune S, Karpati PC, Berton C, Nathan C, Mateo J, Chaara M, et al. Diastolic arterial blood pressure: a reliable early predictor of survival in human septic shock. J Trauma. 2008;64(5):1188–95. https://doi.org/10.1097/TA.0b013e31811f3a45.
Bamoulid J, Philippot H, Kazory A, Yannaraki M, Crepin T, Vivet B, et al. Acute kidney injury in non-critical care setting: elaboration and validation of an in-hospital death prognosis score. BMC Nephrol. 2019;20(1):419. https://doi.org/10.1186/s12882-019-1610-9.
Shi R, Hamzaoui O, De-Vita N, Monnet X, Teboul JL. Vasopressors in septic shock: which, when, and how much? Ann Transl Med. 2020;8(12):794. https://doi.org/10.21037/atm.2020.04.24.
Scheeren TWL, Bakker J, De Backer D, Annane D, Asfar P, Boerma EC, et al. Current use of vasopressors in septic shock. Ann Intensive Care. 2019;9(1):20. https://doi.org/10.1186/s13613-019-0498-7.
Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–10. https://doi.org/10.1001/jama.2016.0287.
Permpikul C, Tongyoo S, Viarasilpa T, Trainarongsakul T, Chakorn T, Udompanturak S. Early use of norepinephrine in septic shock resuscitation (CENSER). A randomized trial. Am J Respir Crit Care Med. 2019;199(9):1097–105. https://doi.org/10.1164/rccm.201806-1034OC.
Jentzer JC, Wiley B, Bennett C, Murphree DH, Keegan MT, Kashani KB, et al. Temporal trends and clinical outcomes associated with vasopressor and inotrope use in the cardiac intensive care unit. Shock. 2020;53(4):452–9. https://doi.org/10.1097/SHK.0000000000001390.
Zhang R, Chen H, Teng R, Li Z, Yang Y, Qiu H, et al. Association between the time-varying arterial carbon dioxide pressure and 28-day mortality in mechanically ventilated patients with acute respiratory distress syndrome. BMC Pulm Med. 2023;23(1):129. https://doi.org/10.1186/s12890-023-02431-6.
Thompson BT. In septic shock, MAP targets of 80 to 85 mm Hg vs 65 to 70 mm Hg did not differ for 28-day mortality. Ann Intern Med. 2014;161(2):JC7. https://doi.org/10.7326/0003-4819-161-2-201407150-02007.
Dilken O, Ergin B, Ince C. Assessment of sublingual microcirculation in critically ill patients: consensus and debate. Ann Transl Med. 2020;8(12):793. https://doi.org/10.21037/atm.2020.03.222.
Cooper ES, Silverstein DC. Fluid therapy and the microcirculation in health and critical illness. Front Vet Sci. 2021;8:625708. https://doi.org/10.3389/fvets.2021.625708.
Collet M, Huot B, Barthelemy R, Damoisel C, Payen D, Mebazaa A, et al. Influence of systemic hemodynamics on microcirculation during sepsis. J Crit Care. 2019;52:213–8. https://doi.org/10.1016/j.jcrc.2019.05.002.
Doerschug KC, Delsing AS, Schmidt GA, Haynes WG. Impairments in microvascular reactivity are related to organ failure in human sepsis. Am J Physiol Heart Circ Physiol. 2007;293(2):H1065-1071. https://doi.org/10.1152/ajpheart.01237.2006.
Payen D, Luengo C, Heyer L, Resche-Rigon M, Kerever S, Damoisel C, et al. Is thenar tissue hemoglobin oxygen saturation in septic shock related to macrohemodynamic variables and outcome? Crit Care. 2009;13(Suppl 5):S6. https://doi.org/10.1186/cc8004.
Siegel JH, Greenspan M, Del Guercio LR. Abnormal vascular tone, defective oxygen transport and myocardial failure in human septic shock. Ann Surg. 1967;165(4):504–17. https://doi.org/10.1097/00000658-196704000-00002.
Xiao W, Liu W, Zhang J, Liu Y, Hua T, Yang M. The association of diastolic arterial pressure and heart rate with mortality in septic shock: a retrospective cohort study. Eur J Med Res. 2022;27(1):285. https://doi.org/10.1186/s40001-022-00930-6.
Ikonomidis I, Makavos G, Nikitas N, Paraskevaidis I, Diamantakis A, Kopterides P, et al. Coronary flow reserve is associated with tissue ischemia and is an additive predictor of intensive care unit mortality to traditional risk scores in septic shock. Int J Cardiol. 2014;172(1):103–8. https://doi.org/10.1016/j.ijcard.2013.12.155.
Cecconi M, Hernandez G, Dunser M, Antonelli M, Baker T, Bakker J, et al. Fluid administration for acute circulatory dysfunction using basic monitoring: narrative review and expert panel recommendations from an ESICM task force. Intensive Care Med. 2019;45(1):21–32. https://doi.org/10.1007/s00134-018-5415-2.
Khan NA, Rabkin SW, Zhao Y, McAlister FA, Park JE, Guan M, et al. Effect of lowering diastolic pressure in patients with and without cardiovascular disease: analysis of the SPRINT (systolic blood pressure intervention trial). Hypertension. 2018;71(5):840–7. https://doi.org/10.1161/HYPERTENSIONAHA.117.10177.
Vidal-Petiot E, Ford I, Greenlaw N, Ferrari R, Fox KM, Tardif JC, et al. Cardiovascular event rates and mortality according to achieved systolic and diastolic blood pressure in patients with stable coronary artery disease: an international cohort study. Lancet. 2016;388(10056):2142–52. https://doi.org/10.1016/S0140-6736(16)31326-5.
Cinel I, Kasapoglu US, Gul F, Dellinger RP. The initial resuscitation of septic shock. J Crit Care. 2020;57:108–17. https://doi.org/10.1016/j.jcrc.2020.02.004.
Acknowledgements
None.
Funding
This work was supported by National Natural Science Foundation of China (81971888) and Jiangsu Provincial Special Program of Medical Science (BE2018743).
Author information
Authors and Affiliations
Contributions
GZW, YY designed the data analysis plan, acquired the data. GZW, LC, CH, CDY and MSL contributed to the acquisition of data and performed the statistical analysis. XJF, WCD and LL take responsibility for the integrity of the data and the accuracy of the data analysis. YY helped conceive of the study. GZW wrote the first draft of the paper and other authors provided comments and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The present study was approved by the Research Ethics Commission of Zhongda Hospital Southeast University (2023ZDSYLL004-P01).
Consent for publication
Not applicable.
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
Percentages of missing data in the variables of interest in the cohort.
Additional file 2.
Mortality of septic shock patients at different diastolic blood pressure levels.
Additional file 3.
Baseline characteristics of the study population according to mDBP24h cutoff value.
Additional file 4.
The association between the worst DBP and 28-day mortality.
Additional file 5.
The relationship between the duration different mDBP24h levels and 28-day mortality of septicshock patients.
Additional file 6.
Mortality of septic shock patients.
Additional file 7.
The 28-day mortality of different interquartile intervals with mDBP24h in 60-70mmHg duration.
Additional file 8.
Subgroup analysis of the association between 28 day survival and mDBP24h mSBP24h and mMAP24h in septic shock patients.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Gao, Z., Li, C., Chen, H. et al. Association between diastolic blood pressure during the first 24 h and 28-day mortality in patients with septic shock: a retrospective observational study. Eur J Med Res 28, 329 (2023). https://doi.org/10.1186/s40001-023-01315-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40001-023-01315-z