
Abstract
Background
Low back pain has been associated with obesity or with being overweight. However, there are no high-quality systematic reviews that have been conducted on the effect of all types of weight loss programs focused on individuals with low back pain. Therefore, the present systematic review aims to evaluate the effectiveness of weight loss programs in reducing back pain and disability or increasing quality of life for individuals experiencing low back pain.
Materials and methods
Searches for relevant studies were conducted on CINAHL, Web of Science, Ovid Medline, Ovid Embase and AMED. Studies were included if they were randomized controlled trials, non-randomized studies of intervention or quasi-experimental designs evaluating a weight loss program for persons with low back pain aimed at decreasing back pain and disability. The Effective Public Health Practice Project (EPHPP) Quality Assessment Tool was used to evaluate individual studies and GRADE was used to summarize the quality of the evidence. The review was prospectively registered; PROSPERO#: CRD42020196099.
Results
Eleven studies (n = 689 participants) including one randomized controlled trial, two non-randomized studies of intervention and eight single-arm studies were included (seven of which evaluated bariatric surgery). There was low-quality evidence that a lifestyle intervention was no better than waitlist for improving back pain and very low-quality evidence from single-arm studies that back pain improved from baseline after bariatric surgery. Most studies included were of poor quality, primarily due to selection bias, uncontrolled confounders, and lack of blinding, limiting the quality of evidence.
Conclusion
There is very low-quality evidence that weight loss programs may improve back pain, disability, and quality of life in patients with LBP, although adherence and maintenance are potential barriers to implementation.
Similar content being viewed by others


Introduction
According to the World Health Organization, low back pain (LBP) has reached epidemic proportions, with 80% of people reporting LBP at some time in their life [1]. About one in four persons with LPB are expected to seek care within six months, resulting in considerable social and economic burden [2]. Persons who suffer from either acute or chronic LBP usually have high levels of disability, decreased function and participation, and poor quality of life [3,4,5,6]. Consistent guidelines for acute LBP feature early and gradual advice to stay active and avoid prescribing bed rest, while common guidelines for the management of chronic LBP includes supervised exercises, cognitive behavioural therapy, and self-management strategies [6]. In addition to the emphasis on exercise, recent studies suggest that lifestyle modifications should be integrated into LBP management programs [7,8,9].
There is a growing number of studies suggesting an association between being overweight/obese and having LBP [7, 8, 10,11,12]. Multiple studies have found that after controlling for potential confounders (e.g., age, sex), the prevalence of LBP is significantly increased in the presence of a high body mass index (BMI) [10, 12, 13]. In addition, a systematic review reported that 32% of 65 epidemiological studies identified a statistically significant positive association between body weight and LBP [14]. One proposed mechanism of association between LBP and weight is that high BMI leads to additional mechanical load on the spine, predisposing individuals to spinal overload [8, 10, 12, 15]. Similarly, there is evidence of a relationship between obesity, systemic inflammation, and LBP, with pro-inflammatory pathways amplified in obesity due to the presence of increased cytokines in adipose tissue [13]. Regardless of the potential pathway through which obesity could be associated with LBP, the findings implicate the vital role that a weight loss program could play in the management of LBP. Ultimately, participating in a weight loss program could translate into a lifestyle change that could not only decrease LBP but also create lifelong benefits in one’s overall health.
Previously, a review of the effects of bariatric surgery on spine pain and upper and lower extremity pain concluded that most of the existing evidence has shown favorable improvements in back pain symptoms after bariatric procedures [16]. However, no systematic literature review is currently available on the effect of all types of weight-loss programs for individuals with LBP. Thus, the present systematic review aims to determine whether a weight loss program is effective in decreasing back pain and disability and/or increasing quality of life in patients with LBP. Given that there are no high-quality systematic reviews that have been conducted on the effect of all types of weight loss programs, we conducted a systematic review of randomized controlled trials (RCTs), non-randomized studies of intervention (NRSI) and quasi-experimental designs such as single-arm studies.
Materials and methods
This systematic review was reported following the PRISMA guidelines [17] and conducted following the Cochrane Handbook review methods [18].
Search methods for identification of studies
An electronic search was conducted on CINAHL (1981 to June 2020), Web of Science (1900 to June 2020), Ovid Medline (1946 to June 2020), Ovid Embase (1974 to June 2020), and AMED (1985 to June 2020) to identify relevant articles. The search was not restricted to any specific language or year of publication. Key terms for weight loss and LBP were used and a search strategy was constructed in consultation with an experienced university librarian (Appendix 1). Citation tracking of the included studies was performed using Web of Science (Thomson Reuters). A manual search of the reference lists of previous reviews and eligible trials was also conducted.
Inclusion Criteria
Types of participants: Studies with adults (18 years or older), who are overweight or obese (BMI > 25 kg/m2), with LBP, with or without leg pain, of any duration (acute: 0–6 weeks, subacute: 6 -12 weeks and chronic: > 12 weeks) were included. Trials evaluating non-specific LBP, as well as specific conditions, such as radiculopathy or spinal stenosis were included. Trials involving a mixed population where some participants did not have back pain at baseline were included if we could identify data for the subgroup of patients that did have back pain at baseline.
Types of interventions/comparators: Studies were included if they evaluated a weight loss program (e.g., physical activity, dietetic treatment) or weight loss treatment (e.g., surgical intervention). If a comparator group existed, the study was included if the comparator group received no treatment, a placebo, or another active treatment (e.g., healthy lifestyle education vs no education).
Types of outcome measures: Trials were included if one of the following outcome measures had been reported: presence of LBP, LBP intensity, disability, or quality of life. For studies with a mixed population of participants with and without back pain, when average pain was presented for the whole population rather than the subgroup of back pain patients, the paper was excluded.
Types of studies
Articles were eligible for inclusion if they were RCTs, NRSIs or quasi-experimental designs such as single-arm studies. Case studies, retrospective chart analysis, gray literature studies (e.g., abstracts, conferences, commentaries, editorials), systematic reviews, and psychometric studies were not eligible for inclusion.
Data extraction and risk of bias assessment
All authors were involved in screening. Screening for all levels was conducted in duplicate by two review authors who screened all search results (titles and abstracts) for potentially eligible studies and screened full texts for eligibility. Data extraction and assessment of risk of bias was checked by a second author. A third independent reviewer resolved disagreements when necessary. Given the inclusion of multiple study designs, the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool for Quantitative Studies was used to evaluate risk of bias of all studies [19]. Although the Cochrane Handbook suggest the use of different scales to assess the risk of bias of different study designs, given that there was only one RCT in this review, we chose to use the EPHPP tool for all included studies. This quality assessment tool scores six components individually (selection bias, study design, confounders, blinding, data collection method, and withdrawals and dropouts) as either strong, moderate, or weak. A global rating is provided as strong if no individual component is rated as weak, moderate if one of the six components is rated as weak and finally, weak if two or more components are rated as weak. The rating was done based on the EPHPP Quality Assessment Tool Dictionary [19].
Data was extracted from each included study using a standardized extraction form. Mean scores, standard deviations and sample sizes were extracted from the studies when continuous outcomes were reported. Number of events and sample sizes were extracted when dichotomous outcomes were reported. When these results were not presented in the studies, a fixed effects model was used to calculate within or between group differences when possible, using the PEDro Excel sheet calculator [20]. Information about characteristics of participants, treatments provided, co-interventions, duration of the treatment and outcome measures were also extracted from the studies. Given the heterogeneity of the included studies, results were summarized qualitatively using tables.
Quality of evidence assessment
We assessed the overall quality of evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach, as recommended in the Cochrane Handbook [18]. For rating, we considered a study of weak or moderate quality on the EPHPP to have high risk of bias.
Results
Study selection
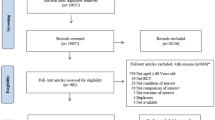
The initial electronic database search resulted in a total of 5624 articles after removing duplicates. Following the removal of duplicates and screening of titles and abstracts, 56 full text articles were assessed. Of these articles, 11 fulfilled the inclusion criteria and were included in this review [21,22,23,24,25,26,27,28,29,30,31]. Through additional manual searches of reference lists, hand searches and Web of Science searches, we did not identify any additional eligible studies. Figure 1 shows the flowchart of the inclusion process of this review. A list of all excluded full text studies with reasons for exclusion can be found in Appendix 2. A few potentially eligible studies were excluded because LBP was not an inclusion criterion and it was unclear whether all patients included had LBP at baseline, even when back pain was a primary outcome.

Flow diagram of study selection
Study characteristics
All studies included in this systematic review investigated the impact of a weight loss intervention on individuals suffering from LBP. However, most studies did not specify the type of LBP included, with some authors mentioning back pain without further consideration of the specific diagnosis. There was one RCT [30], two NRSIs [28, 29], and eight single-arm studies [21,22,23,24,25,26,27, 31]. The outcomes evaluated in these studies were LBP (e.g., Numeric Pain Rating Scale, the presence or absence of pain), disability (e.g., Oswestry Low Back Disability Index) and quality of life (e.g., 36-Item Short Form Health Survey).
Participants
Across all studies there were 689 participants included, 381 in the nonsurgical intervention studies [27, 28, 30] and 308 in the bariatric surgery studies [21,22,23,24,25,26, 29, 31]. Study sample sizes ranged from 18 to 175. The mean age ranged from 33 to 57 years old. At baseline, the participants’ average weight ranged from 80.2 kg to 144.5 kg and their baseline BMI ranged from 24.8 kg/m2 to 54.2 kg/m2. Detailed information on the characteristics of the participants is provided in Table 1.
Interventions
The one RCT by Williams et al. (2018) evaluated a healthy lifestyle intervention (consisting of telephone-based advice, clinical consultation, and healthy lifestyle coaching) compared to waitlist [30]. Eight of the 11 studies investigated the effect of bariatric weight loss surgery on back pain in individuals with LBP [21,22,23,24,25,26, 29, 31] (7 single-arm studies, 1 NRSI). One study investigated nutritional and behavioral modification in combination with analgesic drug treatment, physiotherapy, and massage compared to only analgesic drug treatment, physiotherapy, and massage (NRSI) [28]. The last study investigated a multidisciplinary nonsurgical weight loss program (single-arm study) [27].
Risk of Bias Assessment
The EPHPP Quality Assessment Tool was used to assess the risk of bias in all studies [19]. Ten out of 11 studies received an EPHPP global rating of weak and the only one RCT received a global rating of moderate. Table 2 shows the EPHPP grading process, with primary weaknesses being selection bias, uncontrolled confounders, and lack of blinding.
Effect of nonsurgical weight loss interventions
Randomized controlled trial
Williams et al. randomly assigned 160 participants to a telephone advice session consultation with a 6-month telephone-based healthy lifestyle coaching service versus waitlist and followed them for 26 weeks [30]. The results of the study show that the healthy lifestyle intervention did not improve back pain intensity (MD = 0.3, 95% CI -0.4 to 1.0), decrease disability (MD = -0.1, 95% CI -1.7 to 1.5) or improve quality of life (Physical function: MD = -0.6, 95% CI -3.5 to 2.4; Mental function: MD = -1.7, 95% CI -5.4 to 2.0) for patients with LBP who were overweight/obese. Therefore, there is low-quality evidence given there is one moderate quality study (GRADE reduced due to risk of bias) that a lifestyle intervention is no better than waitlist at improving pain, disability, and quality of life in patients with LBP. See Table 3 for detailed results.
Non-randomized study of intervention
Silisteanu et al. conducted a NRSI that allocated 175 patients diagnosed with chronic LBP to the control (analgesic drug treatment, physiotherapy, and massage) and treatment groups (same as control plus nutritional counselling and physical activity) [28]. The study demonstrated that when nutritional counselling was applied, the VAS pain index (p < 0.01) and QOLS (p < 0.05) (except for men in urban areas) were further improved in the treatment group compared to the control group. Mean differences and confidence intervals could not be calculated as sample size was not available for each group. Although the authors state that correlation analysis demonstrated strong associations between BMI, VAS and QOLS following nutritional intervention, they did not provide results to allow a better interpretation of the findings. See Appendix 3 for weight loss results. Therefore, there is very low-quality evidence from one weak quality study that a nutritional and behavioural modification treatment program may be superior to controls at improving pain and quality of life in obese patients with LBP. See Tables 4 and 5 for detailed results.
Single-arm studies
Roffey et al. conducted a pilot study evaluating a 52-week multidisciplinary weight loss program in 46 obese adults [27]. At week 14, of the 98% of participants that lost more than 5% of their body weight, 50% of participants reported clinically significant improvements in back pain (Minimal Clinically Important Difference (MCID) NPRS = 2/10) (MD = -1.6, 95% CI -2.6 to -0.6) and 73% of participants reported clinically significant improvements in disability (MCID ODI = 10/50) (MD = -8.4, 95% CI -16.2 to -0.06). The results of this study also demonstrated that participants who continued to lose weight beyond 14 weeks and had achieved a greater percentage reduction in BMI after one year, had a positive correlation with improvement in LBP and ODI scores at one year. Thus, given that there is one weak quality study, there is very low-quality evidence that back pain and disability can be reduced after a multidisciplinary weight loss program. See Tables 4 and 6 for detailed results.
Effect of surgical weight loss interventions
Non-randomized study of intervention
Vincent et al. compared a bariatric surgery group to nonsurgical counterparts and identified that at 3 months follow up, 61.1% (n = 25) of participants in the bariatric group had no moderate to severe LBP compared to 25% at baseline (OR = 4.8, 95% CI 1.4 to 16.1), while the control group did not demonstrate any significant changes from baseline [29]. This study also demonstrated between group differences in the SF-36 physical component score of MD = 17.9, 95% CI 12.7 to 23.1 but no difference between groups for the mental component score of MD = 1.6, 95% CI -5.0 to 8.2. Therefore, there is very low-quality evidence from a single weak quality study that bariatric surgery compared to no surgery may improve pain and quality of life (physical component only) at 3 months follow up. See Tables 4 and 5 for detailed results.
Single-arm studies
Seven single-arm studies of weak quality assessed the effectiveness of bariatric surgery on LBP, disability, and quality of life at a median of 12 months after surgery (range 12 – 24 months) [21,22,23,24,25,26, 31]. Six studies evaluated back pain reduction (Numeric pain rating scale (NPRS) and Visual analogue scale (VAS)) at long-term (12 to 24 months) with changes from baseline ranging from -5.0 to -0.7 (on a scale from 0 to 10). Bhandari et al. reported a moderate association between BMI change and NPRS of back pain 1 year post operation (r = 0.40; P = 0.002), while Lidar et al. reported no significant correlation between decreased BMI and improvement in back pain (r = 0.231; P = 0.218). See Appendix 3 for weight loss results. Melissas et al. (2003) reported that at 24 months, 66% (n = 19/29) of patients had complete resolution of LBP and 34% (n = 10/29) of patients reported improvement in LBP symptoms [31]. McGoey et al. demonstrated a 51% (n = 53/104) reduction in the number of participants experiencing LBP at 22.5 months follow-up [25]. The authors state that back pain relief was not statistically different between patients who lost a low to moderate amount of weight (< 27 kg) compared with those who lost a large amount of weight (> 45 kg). However, they did not provide results to allow a better interpretation of the findings. These results from single-arm studies of weak quality, demonstrate very low-quality evidence that bariatric surgery may lead to a reduction in LBP in the long-term.
There were two single-arm studies that demonstrated statistically significant effects of weight loss surgery on disability (ODI) at long-term (12 to 24 months) [23, 26] with change from baseline ranging from -15.6 to -6.3 (on a scale from 0 to 100). These studies demonstrate very low-quality evidence from single-arm studies of weak quality that bariatric surgery may improve disability at long-term.
Lastly, there was one single-arm study that reported a statistically significant improvement and possible clinically significant change in quality of life (SF-36 Physical Function) at long-term (12 months) (MD = 25.7, 95% CI 15.1 to 36.4) [23]. However, another study [24] reported no significant changes in both the mental and physical components of SF-36 at 12 months. Therefore, there is conflicting evidence from two weak quality studies on the effect of bariatric surgery on quality of life at long-term. See Tables 4, 5 and 6 for detailed results.
Overall quality of evidence rating
Due to the fact that all papers, except one, were non-RCTs and had high risk of bias and small sample sizes, the overall quality of the body of evidence for all intervention types and outcomes are rated as very low-quality, as described above.
Discussion
This systematic review included 11 studies evaluating weight loss programs to improve self-reported outcomes of LBP. Most of the studies included were single-arm studies of surgical interventions on obese participants. Of the included studies, there was one moderate quality RCT, two weak quality NRSIs and eight weak quality single-arm studies. There was low-quality evidence that a lifestyle intervention is not better than wait list in improving back pain, disability, and quality of life in patients with LBP. There was very low-quality evidence that nutritional and behavioural modification may be superior to controls at improving back pain and quality of life in obese participants with LBP. Further, there was very low-quality evidence that bariatric surgery may improve back pain and disability in obese participants. Our study demonstrates a lack of high-quality studies in the literature investigating the effectiveness of weight loss programs for LBP.
A multitude of weight loss interventions are available and the most appropriate conservative method for patients with back pain or chronic back pain is yet to be established. Importantly, compliance with weight loss interventions is usually poor and even when an individual losses weight with a program, maintenance is usually a problem [32]. In fact, one study noted that the positive effects of weight loss were reversed at follow-up likely due to a subsequent weight gain of participants [27]. Thus, weight loss interventions may be susceptible to adherence issues and outcomes may be dependent on the maintenance of weight loss. Future studies evaluating the amount of weight loss necessary to observe improvements in back pain and disability and mediators of change are needed. Additionally, future studies should also evaluate the effect of amount of weight loss on other types of joint pain, such as knee osteoarthritis, to determine how weight loss can affect an individual in various aspects.
Potential clinically significant effects of weight loss surgery on LBP were found across eight studies of weak quality [21,22,23,24,26,27, 31]. McGoey found that back pain relief was not superior in patients who lost a large amount of weight (> 45 kg) compared to those who lost a low to moderate amount of weight (< 27 kg) [25]. Thus, patients may even benefit with clinically significant improvements in pain from a modest reduction in weight loss [33]. However, more evidence is needed to evaluate the relationship between weight loss and symptom reduction as this relationship may not be linear with the possibilities of plateauing. Furthermore, these results suggest that other indirect benefits of weight loss could be the primary mediator in the reduction of LBP such as increased mobility, increased physical activity level and changes in psychosocial factors such as self-esteem and self-efficacy. In fact, many of the included full text studies were secondary analysis of weight loss interventions, for which reduction of LBP was not the primary objective. Conversely, weight loss can also be a consequence of LBP treatments such as physical activity and medications [34, 35]. More studies with a primary focus on weight loss interventions for the management of LBP are needed. Studies should focus on the effectiveness of the intervention but also on the amount of weight lost required for symptom improvement, subgroups of BMI that require a weight loss intervention as well as long term adherence to these programs.
There is a lack of literature examining the effects of weight loss programs on LBP despite the large number of studies identifying obesity or high BMI as important risk factors for the development of LBP. This review shows that studies investigating the effect of a weight loss intervention on LBP have been of extremely weak methodological quality with high risk of bias. Although the results of the studies included in this review are promising, no definitive conclusions can be drawn at this time due to the paucity of high-quality RCTs.
Some limitations of this review include the low-quality of studies evaluating within group effects, inconsistent use of outcome measures, and the differences in implementation of the interventions. Most of the included studies are single-arm studies with poor quality of reporting—particularly the inclusion criteria, patient characteristics, and results. Additionally, the inclusion of multiple types of interventions in this review make it difficult to form any solid conclusions and do not allow for pooling of data. However, we presented the results separately by intervention (i.e., bariatric surgery vs nonsurgical weight loss interventions). Lastly, the exclusion of grey literature is a limitation of our review and a deviation from the Cochrane Handbook.
The results of this review highlight the scarcity of research examining the effect of weight loss on LBP. It demonstrates that although associations have been drawn between weight and LBP, there is only very low-quality evidence that some weight loss interventions lead to improvements in LBP and disability. Further, there is evidence to suggest that adherence to these interventions is problematic, particularly in the long term. Future research should focus on conducting higher quality trials that evaluate the effect of weight loss on improving outcomes such as LBP, disability, and quality of life in individuals with LBP with considerations on mediators and moderators of outcomes.
Availability of data and materials
All data generated or analysed during this study are included in this published article and its supplementary information files.
Abbreviations
- BMI:
-
Body mass index
- EPHPP:
-
Effective Public Health Practice Project
- GRADE:
-
Grading of Recommendations Assessment, Development and Evaluation
- LBP:
-
Low back pain
- MD:
-
Mean difference
- NPRS:
-
Numeric pain rating scale
- NRSI:
-
Non-randomized studies of intervention
- RCT:
-
Randomized controlled trials
- VAS:
-
Visual analogue scale
References
WHO Scientific Group on the Burden of Musculoskeletal Conditions at the Start of the New Millennium, World Health Organization. The burden of musculoskeletal conditions at the start of the new millennium: report of a WHO Scientific Group. World Health Organization; 2003.
Hoy D, March L, Brooks P, Woolf A, Blyth F, Vos T, Buchbinder R. Measuring the global burden of low back pain. Best Pract Res Clin Rheumatol. 2010;24(2):155-65.
von Korff M, Deyo R, Cherkin D, Barlow W. Back Pain in Primary Care. Spine. 1993;18(7):855–62.
Hayden J, Van Tulder MW, Malmivaara A, Koes BW. Exercise therapy for treatment of non‐specific low back pain. Cochrane Database Syst Rev. 2005;(3).
Deyo R, Battie M, Beurskens A, Bombardier C, Croft P, Koes B, et al. Outcome measures for low back pain research: a proposal for standardized use. Spine. 1998;23(18):2003–13.
Koes BW, van Tulder M, Lin CWC, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur Spine J. 2010;19:2075–94.
Shiri R, Lallukka T, Karppinen J, Viikari-Juntura E. Obesity as a risk factor for sciatica: A meta-analysis. Am J Epidemiol. 2014;179:929–37.
Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Varonen H, Kalso E, et al. Cardiovascular and lifestyle risk factors in lumbar radicular pain or clinically defined sciatica: A systematic review. Eur Spine J. 2007;16(12):2043–54.
Schumann B, Bolm-Audorff U, Bergmann A, Ellegast R, Elsner G, Grifka J, et al. Lifestyle factors and lumbar disc disease: Results of a German multi-center case-control study (EPILIFT). Arthritis Res Ther. 2010;12(5):R193.
Heuch I, Heuch I, Hagen K, Zwart JA. Body mass index as a risk factor for developing chronic low back pain: A follow-up in the nord-trøndelag health study. Spine. 2013;38(2):133–9.
Wasser JG, Vasilopoulos T, Zdziarski LA, Vincent HK. Exercise Benefits for Chronic Low Back Pain in Overweight and Obese Individuals. PM R. 2017;9:181–92.
Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E. The association between obesity and low back pain: A meta-analysis. Am J Epidemiol. 2010;171(2):135–54.
Briggs MS, Givens DL, Schmitt LC, Taylor CA. Relations of C-reactive protein and obesity to the prevalence and the odds of reporting low back pain. Arch Phys Med Rehabil. 2013;94(4):745–52.
Leboeuf-Yde C. Body weight and low back pain: a systematic literature review of 56 journal articles reporting on 65 epidemiologic studies. Spine. 2000;25(2):226.
Smuck M, Kao MCJ, Brar N, Martinez-Ith A, Choi J, Tomkins-Lane CC. Does physical activity influence the relationship between low back pain and obesity? Spine Journal. 2014;14(2):209–16.
Vincent HK, Ben-David K, Cendan J, Vincent KR, Lamb KM, Stevenson A. Effects of bariatric surgery on joint pain: A review of emerging evidence. Surg Obes Relat Dis. 2010;6:451–60.
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339:b2700.
Higgins J, Thomas J, Chandler J, Cumpston M, Li T, Page M, et al. Cochrane Handbook for Systematic Reviews of Interventions version 6.2 (updated February 2021) [Internet]. Cochrane. 2021 [cited 2021 Aug 25]. Available from: www.training.cochrane.org/handbook
Quality Assessment Tool for Quantitative Studies [Internet]. Effective Public Healthcare Panacea Project. 2019 [cited 2022Feb11]. Available from: https://www.ephpp.ca/quality-assessment-tool-for-quantitative-studies/
Confidence interval calculator [Internet]. PEDro. 2020 [cited 2022Feb11]. Available from: https://pedro.org.au/english/resources/confidence-interval-calculator/
Bhandari M, Mathur W, Kosta S, Salvi P, Fobi M. Assessment of functional ability of nonambulatory patients with obesity: after and before bariatric surgery. Surgery for Obesity and Related Diseases. 2019;15(12):2087–93.
Hooper MM, Stellato TA, Hallowell PT, Seitz BA, Moskowitz RW. Musculoskeletal findings in obese subjects before and after weight loss following bariatric surgery. Int J Obes. 2007;31(1):114–20.
Khoueir P, Black MH, Crookes PF, Kaufman HS, Katkhouda N, Wang MY. Prospective assessment of axial back pain symptoms before and after bariatric weight reduction surgery. Spine Journal. 2009;9(6):454–63.
Lidar Z, Behrbalk E, Regev GJ, Salame K, Keynan O, Schweiger C, et al. Intervertebral disc height changes after weight reduction in morbidly obese patients and its effect on quality of life and radicular and low back pain. Spine. 2012;37(23):1947–52.
McGoey B, Deitel M, Saplys R, Kliman M. Effect of weight loss on musculoskeletal pain in the morbidly obese. J Bone Joint Surg. 1990;72(2):322–3.
Melissas J, Kontakis G, Volakakis E, Tsepetis T, Alegakis A, Hadjipavlou AA. The Effect of Surgical Weight Reduction on Functional Status in Morbidly Obese Patients with Low Back Pain. Obes Surg. 2005;15(3):378–81.
Roffey DM, Ashdown LC, Dornan HD, Creech MJ, Dagenais S, Dent RM, et al. Pilot evaluation of a multidisciplinary, medically supervised, nonsurgical weight loss program on the severity of low back pain in obese adults. Spine Journal. 2011;11(3):197–204.
Silişteanu S, Covaşă M. Reduction of body weight through nutrition intervention reduces chronic low back pain. 2015 E-Health and Bioengineering Conference (EHB). 2015;14(2):1–3.
Vincent HK, Ben-David K, Conrad BP, Lamb KM, Seay AN, Vincent KR. Rapid changes in gait, musculoskeletal pain, and quality of life after bariatric surgery. Surg Obes Relat Dis. 2012;8(3):346–54.
Williams A, Wiggers J, O’Brien KM, Wolfenden L, Yoong SL, Hodder RK, et al. Effectiveness of a healthy lifestyle intervention for chronic low back pain: A randomised controlled trial. Pain. 2018;159(6):1137–46.
Melissas J, Volakakis E, Hadjipavlou A. Low-Back Pain in Morbidly Obese Patients and the Effect of Weight Loss Following Surgery. Obes Surg. 2003;13(3):389–93.
Ostelo RW, Deyo RA, Stratford P, Waddell G, Croft P, von Korff M, et al. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine. 2008;33(1):90–4.
Johnston BC, Kanters S, Bandayrel K, Wu P, Naji F, Siemieniuk RA, et al. Comparison of weight loss among named diet programs in overweight and obese adults: A meta-analysis. JAMA - Journal of the American Medical Association. 2014;312(9):923–33.
Muehlbacher M, Nickel MK, Kettler C, Tritt K, Lahmann C, Leiberich PK, et al. Topiramate in Treatment of Patients With Chronic Low Back Pain A Randomized, Double-blind, Placebo-controlled Study. The Clinical journal of pain [Internet]. 2006 Jul 1;22(6):526–31. Available from: https://journals.lww.com/clinicalpain
Szczurko O, Cooley K, Busse JW, Seely D, Bernhardt B, Guyatt GH, et al. Naturopathic care for chronic low back pain: A randomized trial. PLoS ONE. 2007;2(9):e919.
Acknowledgements
Not applicable.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors contributed equally to the work in this paper. The author(s) read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare to have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Chen, L.H., Weber, K., Mehrabkhani, S. et al. The effectiveness of weight loss programs for low back pain: a systematic review. BMC Musculoskelet Disord 23, 488 (2022). https://doi.org/10.1186/s12891-022-05391-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12891-022-05391-w