
Abstract
Background
This study was aimed to examine the relationship between muscular fitness indicators in childhood and areal bone mineral density (aBMD) in adulthood and to verify whether the relationship is mediated by performance on muscular fitness indicators in adulthood.
Methods
A sample of 138 healthy adults (69 males; 22.3 years) were followed after a previous assessment at the age of 7–10 years. Stature, body mass and muscular fitness indicators (handgrip strength, standing long jump and sit-ups tests) were assessed in childhood and adulthood. Additionally, total body, upper limbs, lower limbs, right femoral neck and lumbar spine aBMD was assessed in adulthood using dual X-ray absorptiometry. Analysis included descriptive statistics; t-test or Mann-Whitney U-test for comparison between males and females, multiple linear regression for the prediction aBMD from muscular fitness indicators in childhood, mediation analysis of the respective muscular fitness indicators in adulthood and the relationship between muscular fitness indicators in childhood and aBMD.
Results
Males were stronger compared to females regarding muscular fitness indicators in childhood and adulthood, and presented higher mean values for aBMD in adulthood, except for lumbar spine (p < 0.05). Regression analysis revealed that some muscular fitness indicators in childhood showed significant positive relationship with bone health indicators in adulthood, such as: handgrip strength and total body aBMD (β = 0.005; R2 = 0.35; p = 0.040) and upper limbs aBMD (β = 0.005; R2 = 0.55; p = 0.019); and sit-ups test was a significant predictors of lumbar spine BMD (β = 0.003; R2 = 0.06; p = 0.039). Mediation analysis pointed out the following: adulthood handgrip strength mediated relationships between childhood handgrip strength and total aBMD (indirect effect (IE) = 0.0025; 95%CI = 0.0005–0.0048), and upper limbs aBMD (IE = 0.0040; 95%CI = 0.0017–0.0069).
Conclusions
Muscular fitness indicators in childhood showed significant relationship with bone health indicators in adulthood and the sit-ups test in childhood had direct effect on lumbar spine aBMD in adulthood. Adulthood handgrip strength mediated the relationship between childhood handgrip strength and total body and upper limb aBMD, pointing out that muscular fitness in childhood may be a aBMD determinant in adulthood, especially when higher muscle fitness performance is maintained in adulthood.
Similar content being viewed by others


Introduction
Peak bone mass (PBM) is reached in early adulthood and is interpreted as the achievement of the highest expression of bone tissue [1]. It is considered a relevant indicator in prediction of osteoporosis and fractures in the course of aging [2, 3]. The literature suggests that an increment of 10% in PBM tends to delay the onset of osteoporosis by 13 years [4]. In addition, epidemiological evidences [5] concluded that this increase of 10% in PBM during the first decades of life is associated to a decrement of 50% in the risk of fracture among elderly women. By inference, optimization of the bone mass gain during growth seems central to mitigate the consequences of the physiological loss with aging.
Several factors contribute to PBM such as genetics, bone status during childhood, endocrine regulators, interaction of bone tissue with other tissues, lifestyle factors, chronic diseases during childhood, and others [6,7,8]. Meantime, the trajectory of bone mass gains is similar to that of linear growth and believed to be sensitive to modifiable or non-modifiable determinants during this period [9]. There is evidence of the effect of physical activity [7] and improved muscular fitness on bone mass [10]. Bones are exposed to muscular action, stronger muscles exert more tension on bones and consequent mechanical adaptations. The mechanical adaptations of bones according to what type of exercise they are submitted to are explained by mechanostatic [11], mechanosensation and transduction theories [12].
Positive relationship between muscle fitness and bone health indicators between children and adolescents aged 8–18 years, has been previously demonstrated in cross-sectional studies [13, 14], but evidence that muscular fitness in childhood and adolescence is a determinant of bone health in adulthood is still limited [15]. Recently, García-Hermoso et al. [16] performed a meta-analysis to conclude for a moderate effect of muscle fitness during childhood and adolescence on follow-up studies assessing areal bone mineral density (aBMD). Although evidence about the impact of mechanical stress through muscle action on bone modulation [17], it is not clear whether the advantages obtained are maintained when the physical stimulus ceases [18, 19]. A few studies observed the maintenance of benefits from exposure to mechanical loads even years after physical activity has ceased [20, 21]. In contrast, other studies showed that gains were not maintained after activity cessation or reduction [22, 23].
Adult males and females who had been physically active during adolescence demonstrated bone mineral content 8 to 10% higher compared to inactive or moderately active peers during adolescence, and also had higher physical activity scores in adulthood [24]. Meantime, the association between muscle fitness indicators (MFI) in circumpubertal years and bone strength variables in adulthood could be attenuated after the model was adjusted for the performance of muscle fitness indicators in adulthood [25]. Thus, it is of interest to identify the direct, indirect or mediated effects by performance in MFI in adulthood on the relationship between muscle fitness in childhood and aBMD in adulthood. The current study is aimed to examine the relation-ship between MFI in childhood and different aBMD regions of interest in adulthood and to verify whether this relationship is mediated by performance of MFI in adulthood.
Methods
Procedures and ethics committee
This prospective study was initially designed to examine growth, maturation and physical fitness in schoolchildren aged 7 to 10 years recruited from a private school in Londrina (Paraná, Brazil), with a mixed longitudinal design with four birth cohorts (1992, 1993, 1994, 1995) followed annually from 2002 to 2006 (initial moment research approved by ethics committee of Campinas State process CEP N 249/2002, July 16, 2002, and longitudinal data by ethics committee of Londrina State University process CEP N 024/03, April 01, 2003). Criteria of sampling were an α of 95%, a statistical power of 80%, and an error of 5% as previously described [26]. Parents or legal guardians of 1052 children signed an informed consent, and participants were informed that their participation was voluntary. Data were collected during Physical Education requiring three visits of the research team to elementary school within two weeks in all follow-up years. Participants of the preceding sample were contacted 15 years later to be reassessed as part of the “Physical fitness and practice of sports in childhood and adolescence and behavioral risk factors in adulthood” (ethics committee of Londrina State University approved the research: process N 1.340.735, November 27, 2015). The baseline and follow-up have been previously described [27].
Sample
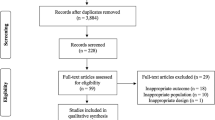
Inclusion criteria for the current study were: (i) not being injured or physically limited (as, for example, asthma); (ii) have at least one baseline measure for fitness tests to determined MFI were assessed; (iii) completed the same muscular fitness indcators battery as adults in addition to dual energy x-ray absorptiometry. Exclusion criteria were: participants under frequent use of medication to treat any disease that could interfere with the study variables (Fig. 1).

Sample selection
A total of 138 healthy young adults aged 18–25 years were eligible to participate in the study (50% males). Examination of dropouts compared to children who were assessed at baseline and follow-up is summarized in Table 1. Differences between children who participated as adults and those who were evaluated only at baseline did not indicate significant differences in variables, except for the sit-up test in males (p = 0.02).
Anthropometry
Anthropometry was assessed according to procedures described by Gordon et al. [28]. Body mass was measured on a digital platform scale with precision of 0.05 kg. Harpenden portable stadiometer with 0.1 cm precision was used to measure height. Subsequently, body mass index (BMI) was calculated and expressed in kg per m2. Childhood BMI z-score was calculated using reference values from the CDC Growth Charts [29] and was used as an adjustment variable in the statistical analyses.
Muscular fitness indicators (MFI)
Muscle fitness is understood as the capacity to perform work against resistance and involves maximum isometric or dynamic strength, isokinetics, muscular endurance and power [10]. The hand grip strength test (HS), strength measure, was completed according to procedures described by Soares and Sessa [30], using Jamar Hydraulic Dynamometer (Sammons and Preston Scientific Industries Inc.) with precision of 1 kilogram force (kgf). Three measurements were performed and the best score was retained for analysis. Standing long jump test (SLJ), explosive strength indicator, corresponded to the maximal horizontal jumping performance performed from a starting position with participant with parallel feet. Three attempts were performed with the best scores in cm retained for analysis [30]. Sit-ups test, endurance strength indicator, required a mat and a stopwatch. With participants in dorsal decubitus, hips and knees flexed, feet soles facing the ground, arms crossing the thorax, hands supported on shoulders, the evaluator was holding the feet of participants who were instructed to perform the maximum number of trunk elevation including a contact of the forearms with the thighs and return to the initial position, the test was performed only once for a period of 60 seconds and the total number of repetitions was used in the analyses [31]. For the analysis, the total number of repetitions performed on a single trial was recorded.
In addition to the performance in each indicator of muscular fitness during the childhood period, an index called childhood muscular fitness z-Score (CMF z-Score) was calculated by adding the standardized z-score value (individual value - mean / standard deviation) of the performance in each indicator of muscular fitness (HS + SLJ + Sit-ups).
Regarding the quality control of observed data, the muscular fitness indicators of 20 adults randomly selected, after an interval of 7 days, were analyzed. Intraclass correlation coefficients for intra-observer reliability were: HS (ICC = 0.98), SLJ (ICC = 0.98) and sit-ups (ICC = 0.90).
Dual energy X-ray absorptiometry (DXA)
Participants were positioned on the table in supine position with the body aligned along with the central axis. A single certified technician completed the scans using DXA (Lunar DPX-MD+, GE Lunar Corporation, 726 Heartland Trail, Madison, WI 53717 − 1915 USA). Data were obtained using the software recommended by the manufacturer. Scans allowed calculations for aBMD of total body, lumbar spine (L1-L4), upper limbs, lower limbs, right femoral neck. The equipment was previously calibrated according to manufacturer. Full body scan was performed with participants in supine position and aligned, holding still for approximately 15 to 20 minutes. For the lumbar region, individuals were also positioned in dorsal decubitus, with legs placed on a block forming a 90-degree angle in relation to the table, with the intention of straightening the lumbar spine. For the proximal femur examination, keeping the patient positioned in dorsal decubitus, a triangular support was used to immobilize the lower limbs after internal rotation and adequate positioning of the femur, in order to capture the femoral neck region of interest.
Data analysis
Descriptive statistics of the sample were summarized in Table 2, separately for baseline and follow-up and sex. Comparisons between males and females were determined using independent t-test at baseline and follow-up. Linear regression using the enter method was used to analyze the relationship between MFI measured in childhood (baseline) and aBMD of different regions of interest measured in adulthood (follow-up). Regression analyses were adjusted for sex, chronological age, and childhood BMI z-score. Mediation analysis was performed on the MFI in childhood that showed statistically significant relationship with bone health indicators (BHI), considering the respective MFI in adulthood as the mediator variable. Mediation analysis followed the principles of Baron and Kenny [32] using the PROCESS 3.0 macro by Andrew F. Hayes, where “a” reflected the relationship between independent variable and the proposed mediator variable, “b” was the effect of the mediator variable on the dependent variable, partializing the effect of the independent variable, “c’” represented the direct impact of the independent variable on the dependent variable, and, “c’” represented the total effect of the independent variable on the dependent variable. The indirect effect is the product of “a” and “b” and quantifies the effect of the independent variable on the dependent variable through the mediator variable. Mediation assumptions were confirmed, the confidence interval of the indirect effect was estimated by the bootstrapping technique (5000, resampling), and unstandardized parameters were used to describe Betas. The mediation proportion was estimated by calculating 1 - (direct effect/total effect). Data were analyzed using SPSS version 25.0. The significance level adopted was 5%.
Results
Table 2 summarize the mean and standard deviation of males and females separately at the baseline and follow-up. At baseline, although boys and girls did not differ in terms of body size given by stature, body mass and BMI, significant differences were noted for the MFI (HS, p < 0.01; SLJ, p < 0.01; sit-ups, p < 0.01). Meantime, among the adult sample, males were heavier (p < 0.001), taller (p < 0.001), stronger (HS, p < 0.001; SLJ, p < 0.001; sit-ups, p < 0.001). Regarding aBMD that was uniquely assessed among adults, sex differences were significant for total body (p < 0.001), upper limbs (p < 0.001), lower limbs (p < 0.001), right femoral neck (p < 0.001).
The association between MFI in childhood and aBMD of the different regions of interest in adulthood and significant values were obtained (Table 3). In the multiple linear regression procedure, adjustments for sex, age, and childhood BMI z-score were considered. Muscular fitness in childhood HS was significant predictors of total body aBMD (p = 0.040), trunk aBMD (p = 0.017) and upper limbs aBMD (p = 0.019). The sit-ups test was significant predictors of lumbar spine aBMD (p = 0.039) and trunk aBMD (p = 0.036), and the CMF z-Score was significant predictors of trunk aBMD (p = 0.040). The other relationships were not statistically significant.
Subsequently to this identification, the respective MFI measured at follow-up, i.e., in early adulthood, was evaluated as mediators in the relationship between MFI in childhood and BHI in adulthood. The mediation analyses can be seen in Fig. 2 only in the models that attended the statistical assumptions.

Mediation models for muscular fitness indicators in adulthood on the relationship between muscular fitness indicators in childhood and BMD of different regions of interest in adulthood, non-standard parameters
Note: HS = Handgrip strength; aBMD = Areal bone mineral density; a = Effect of the independent variable on the pro-posed mediating variable; b = Effect of the variable proposed as mediator on the dependent variable with partial effect of the independent variable; c’ = Direct effect of the independent variable on the dependent variable; c = Total effect of the independent variable on the dependent variable. Adjusted model by sex, childhood chronological age, and childhood BMI z-score; * = p < 0.05; ** = p < 0.01
Considering the coefficients of regression equations in the mediation analysis identified as a, b, c and c’, as well as the significance level from the confidence interval of the indirect effect (a and b), it was observed that the mediator effect (indirect effect) between childhood HS and total body aBMD (β = 0.0025; 95% CI = 0.0005–0.0048), upper limbs aBMD (β = 0.0040; 95% CI = 0.0017–0.0069) was significant. Adulthood HS mediated approximately 52% of the relationship between childhood HS and total aBMD and 83% of the relationship between childhood HS and aBMD of the upper limbs (Fig. 2). No mediator effect (indirect effect) was observed between childhood sit-ups with lumbar spine aBMD.
Discussion
The aim of the present study was to verify the relationship between MFI in childhood and aBMD of the different regions of interest in adulthood and to verify whether this relationship is mediated by performance in MFI in adulthood. The main finding of this study is that adulthood HS plays a mediating role in the relationship between childhood HS and total and upper limbs aBMD, pointing out that muscle fitness in childhood may be important aBMD determinants in adulthood, especially when muscle fitness performance is maintained in the transition to adulthood. Direct effect was observed between childhood sit-ups with lumbar spine aBMD.
The magnitude of the relationship between MFI in childhood with aBMD in adulthood found in the present study is low to moderate, according to results observed in literature [33, 34]. When considering sex, chronological age, childhood BMI z-score, and MFI in determining BHI, models explained from 6% (sit-ups test and lumbar spine aBMD) to 55% (HS and upper limbs aBMD). Although the magnitude of the relationship and the explanation of some models are discrete, it is important to point out some considerations. There is a wide variety of determinants that influence PBM [7], even if low, making these results worthy of attention. Lower correlation coefficients are generally found in longitudinal studies as the time interval between measurements increases, and in this study, this interval is on average 13 years, so discrete coefficients are assumed [33, 35]. Finally, small changes impact bone strength and postpone weakening that comes with osteoporosis [4, 7].
Few studies have attempted to observe these relationships longitudinally, mainly in childhood. Foley et al. [25] evaluated the relationship between physical fitness in childhood with adulthood BHI by calcaneal quantitative ultrasonography measurements, and found positive and significant association between standing long jump and BHI in females; however, when performance in the standing long jump in adulthood was controlled, this association was not significant. A few other longitudinal studies evaluated the relationship between BHI obtained by DXA in adulthood and MFI in adolescence [33, 34, 36, 37]. These studies are heterogeneous regarding the regions of interest measured by DXA and methods used such as MFI, but in general, they point to significant, positive, and low to moderate magnitude relationships.
Additionally, as conducted by Kemper et al. [34], this study controlled regression analyses with sex and also obtained significant relationships between childhood MFI and adulthood BHI. There is a need to control the variable sex in analyses involving muscle fitness and aBMD, due to hormonal aspects, body size [38] and preference for specific physical activities that are inherent to sex and may not reach thresholds that stimulate osteogenesis.
With regard to SLJ, muscle fitness indicator, showed no statistically significant relationship with aBMD for any of the regions of interest, although some studies have reported positive association [27, 41], others have reported negative association [40] and some found no association [41]. The aspect that may explain this result in motor tests involving body displacement to estimate muscle strength, is the body weight, which can play a key role in performance during the execution of tests, and those with weight values below average may perform better [40]. In addition, SLJ requires greater motor efficiency, so force generation with lower limb speed may be affected by poor motor coordination [40, 10].
On the other hand, relationships found between HS and upper limbs aBMD and sit-ups with lumbar spine aBMD can be understood through the mechanostatic theory, via interaction of bones with muscles [11]. The role of HS in childhood and adults with aBMD is worth highlighting. This relationship between HS and total body aBMD may be explained, in part, by the ability of the handgrip test to represent the individual’s overall strength level [42]. Furthermore, mechanical and biological stimuli can trigger generalized systemic endocrine effects, such as myokines in bone metabolism, which could explain the interaction of bone and muscle tissue even at anatomically distant sites [43].
With regard to mediation analysis, mediation of adulthood HS in relationships between childhood HS and total body and upper limbs aBMD and direct effect of childhood sit-ups on lumbar spine aBMD were found. This result allows concluding that muscle fitness performance in childhood provides higher adulthood aBMD, especially when higher muscle fitness performance is maintained in adulthood. Thus, the stimuli need to be constant in order to maintain the osteogenic effects. Furthermore, these relationships were longitudinally examined, while other studies have investigated mediator variables in similar relationships with cross-sectional design, such as the work by Torres-Costoso et al. [40] and Vicente-Rodríguez et al. [44]. A recent study found a mediator effect of muscle mass on the relationship between physical activity in child-hood and adolescence and bone parameters at the age of 17 years, highlighting the important effect of muscle fitness on BHI [45]. Studies have sought to analyze the mediator effect of muscular fitness on the association between other factors such as eating disorders [46], sports involvement [47], vitamin D [48], physical activity [49] and BHI.
Finally, direct relationship of sit-ups in childhood with aBMD of the lumbar spine in adulthood was observed, sit-ups test performance did not play a mediating role in the relationship of equivalents in childhood. The direct effect of childhood MFI on adulthood aBMD highlight the importance of improving muscle fitness from childhood.
The strength of this study is its longitudinal design, capable of partially inferring the causal relationship among variables analyzed. Follow-up studies can have a dropout effect, and in this analysis, they were negligible and not significant. Another potential was the assessment of bone variables and application of motor tests that analyze different body regions, allowing close and distant associations of anatomical specificities. Limitations include sample size, which made stratification by sex unfeasible, but allowed controlling sex in the analyses; the application of motor tests in the identification of muscle fitness, which suffers interference from other variables that could not be controlled; obtaining aBMD only at the adult moment and lack of control of other confounding variables, such as calcium, vitamin D intake, and practice of physical activity between childhood and adulthood. Future studies should invest in assessing and training muscular fitness to promote bone health at all stages of the life cycle, seeking to adequate the dose response needed to obtain advantages and to seek to maintain health benefits already obtained.
Conclusion
It was possible to conclude that some MFI in childhood showed significative relationship with BHI in adulthood, such as between HS and total body and upper limbs aBMD, sit-ups test and lumbar spine aBMD. In addition, the sit-ups test in childhood had a direct effect on lumbar spine aBMD in adulthood, highlight the importance of improving muscle fitness from childhood. Adulthood HS mediated the relationship between childhood HS and total body and upper limbers aBMD, pointing out that muscle fitness in childhood may be an aBMD determinant in adulthood, especially when higher muscle fitness performance in adulthood is maintained.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- MFI:
-
Muscular fitness indicators
- aBMD:
-
Areal bone mineral density
- BHI:
-
Bone health indicators
- HS:
-
Handgrip strength
- IE:
-
Indirect effect
- PBM:
-
Peak bone mass
- SLJ:
-
Standing long jump test
- DXA:
-
Dual Energy X-Ray Absorptiometry
- CMF z-Score:
-
Childhood Muscular Fitness z-Score.
References
Heaney RP, Abrams S, Dawson-Hughes B, et al. Peak bone mass. Osteoporos Int. 2000;11(12):985–1009. https://doi.org/10.1007/s001980070020.
Bonjour JP, Chevalley T, Ferrari S, Rizzoli R. The importance and relevance of peak bone mass in the prevalence of osteoporosis. Salud Publica Mex. 2009;51(Suppl 1):5–S17. https://doi.org/10.1590/s0036-36342009000700004.
Min SK, Oh T, Kim SH, et al. Position Statement: Exercise Guidelines to increase peak bone Mass in Adolescents. J Bone Metab. 2019;26(4):225–39. https://doi.org/10.11005/jbm.2019.26.4.225.
Hernandez CJ, Beaupré GS, Carter DR. A theoretical analysis of the relative influences of peak BMD, age-related bone loss and menopause on the development of osteoporosis. Osteoporos Int. 2003;14(10):843–7. https://doi.org/10.1007/s00198-003-1454-8.
Bonjour J, Chevalley T, Ferrari S, Rizzoli R. Peak bone mass and its regulation. In: Gloriex F, Pettifor J, Juppner H, editors. Pediatric bone: biology and disease. San Diego: Academic Press; 2012. p. 120.
Gordon CM, Zemel BS, Wren TA, et al. The determinants of peak bone Mass. J Pediatr. 2017;180:261–9. https://doi.org/10.1016/j.jpeds.2016.09.056.
Weaver CM, Gordon CM, Janz KF, et al. The national osteoporosis Foundation’s position statement on peak bone mass development and lifestyle factors: a systematic review and implementation recommendations. Osteoporos Int. 2016;27(4):1281–386. https://doi.org/10.1007/s00198-015-3440-3.
Zhu X, Zheng H. Factors influencing peak bone mass gain. Front Med. 2021;15(1):53–69. https://doi.org/10.1007/s11684-020-0748-y.
Bonjour JP, Chevalley T. Pubertal timing, bone acquisition, and risk of fracture throughout life. Endocr Rev. 2014;35(5):820–47. https://doi.org/10.1210/er.2014-1007.
Ortega FB, Ruiz JR, Castillo MJ, Sjöström M. Physical fitness in childhood and adolescence: a powerful marker of health. Int J Obes. 2008;32(1):1–11. https://doi.org/10.1038/sj.ijo.0803774.
Frost HM. Bone’s mechanostat: a 2003 update. Anat rec a Discov Mol. Cell Evol Biol. 2003;275(2):1081–101. https://doi.org/10.1002/ar.a.10119.
Klein-nulend J, Bakker AD, Bacabac RG, Vatsa A, Weinbaum S. Mechanosensation and transduction in osteocytes. Bone. 2013;54(2):182–90. https://doi.org/10.1016/j.bone.2012.10.013.
Alghadir AH, Gabr SA, Rizk AA. Physical fitness, adiposity, and diets as surrogate measures of Bone Health in Schoolchildren: a biochemical and cross-sectional survey analysis. J Clin Densitom. 2018;21(3):406–19. https://doi.org/10.1016/j.jocd.2017.12.006.
Gracia-Marco L, Vicente-Rodríguez G, Casajús JA, et al. Effect of fitness and physi-cal activity on bone mass in adolescents: the HELENA Study. Eur J Appl Physiol. 2011;111(11):2671–80. https://doi.org/10.1007/s00421-011-1897-0.
Barbosa CCL, Romanzini CLP, Batista MB, et al. Neuromuscular fitness in early life and its impact on bone health in adulthood: a systematic review. Rev Paul Pediatr. 2020;9(38):e2019119. https://doi.org/10.1590/1984-0462/2020/38/2019119.
García-Hermoso A, Ramírez-Campillo R, Izquierdo M. Is muscular Fitness Associated with Future Health benefits in children and adolescents? A systematic review and Meta-analysis of Longitudinal Studies. Sports Med. 2019;49(7):1079–94. https://doi.org/10.1007/s40279-019-01098-6.
Naughton G, Greene D, Courteix D, Baxter-Jones A, Resilient. Responsive, and healthy developing Bones: the Good News about Exercise and Bone in Children and Youth. Pediatr Exerc Sci. 2017;29(4):437–9. https://doi.org/10.1123/pes.2017-0205.
Bielemann RM, Domingues MR, Horta BL, et al. Physical activity throughout adolescence and bone mineral density in early adulthood: the 1993 Pelotas (Brazil) Birth Cohort Study. Osteoporos Int. 2014;25(8):2007–15. https://doi.org/10.1007/s00198-014-2715-4.
Karl Karlsson M, Erik Rosengren B. Physical activity as a strategy to reduce the risk of osteoporosis and fragility fractures. Int J Endocrinol Metab. 2012;10(3):527–36. https://doi.org/10.5812/ijem.3309.
Erlandson MC, Runalls SB, Jackowski SA, Faulkner RA, Baxter-Jones ADG. Structural strength benefits observed at the hip of Premenarcheal Gymnasts are maintained into Young Adulthood 10 years after Retirement from the Sport. Pediatr Exerc Sci. 2017;29(4):476–85. https://doi.org/10.1123/pes.2017-0039.
Scerpella TA, Dowthwaite JN, Rosenbaum PF. Sustained skeletal benefit from childhood mechanical loading. Osteoporos Int. 2011;22(7):2205–10. https://doi.org/10.1007/s00198-010-1373-4.
Karlsson MK, Linden C, Karlsson C, et al. Exercise during growth and bone mineral density and fractures in old age. Lancet. 2000;355(9202):469–70. https://doi.org/10.1016/s0140-6736(00)82020-6.
Tervo T, Nordström P, Neovius M, Nordström A. Constant adaptation of bone to current physical activity level in men: a 12-year longitudinal study. J Clin Endocrinol Metab. 2008;93(12):4873–9. https://doi.org/10.1210/jc.2008-1313.
Baxter-Jones AD, Kontulainen SA, Faulkner RA, Bailey DA. A longitudinal study of the relationship of physical activity to bone mineral accrual from adolescence to young adulthood. Bone. 2008;43(6):1101–7. https://doi.org/10.1016/j.bone.2008.07.245.
Foley S, Quinn S, Dwyer T, Venn A, Jones G. Measures of childhood fitness and body mass index are associated with bone mass in adulthood: a 20-year prospective study. J Bone Miner Res. 2008;23(7):994–1001. https://doi.org/10.1359/jbmr.080223.
Werneck AO, Silva DR, Oyeyemi AL, et al. Tracking of physical fitness in elementary school children: the role of changes in body fat. Am J Hum Biol. 2019;31(3):e23221. https://doi.org/10.1002/ajhb.23221.
Blasquez Shigaki G, Barbosa CCL, Batista MB, et al. Tracking of health-related physical fitness between childhood and adulthood. Am J Hum Biol. 2020;32(4):e23381. https://doi.org/10.1002/ajhb.23381.
Gordon CC, Chumlea WC, Roche AF. Stature, recumbent length, and weight. In: Lohman TG, Roche AF, Martorell R, editors. Anthropometric standardization reference ManuaI. Champaign, IL, USA: Human Kinetics; 1998.
Kuczmarski RJ, Ogden CL, Guo SS et al. CDC Growth Charts for the United States: methods and development. Vital Health Stat 11. 2002;(246):1-190. PMID: 12043359.
Soares J, Sessa M. Medidas de força muscular. In: Matsudo VKR (org.), editor. Testes em ciências do esporte. São Caetano do sul: Celafisc. CD-ROM; 2001.
American Alliance for Health, and Dance. Physical Best: A Physical Fitness Education & Assessment Program. The Alliance, 1988.
Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–82. https://doi.org/10.1037//0022-3514.51.6.1173.
Delvaux K, Lefevre J, Philippaerts R, et al. Bone mass and lifetime physical activity in flemish males: a 27-year follow-up study. Med Sci Sports Exerc. 2001;33:1868–75. https://doi.org/10.1097/00005768-200111000-00011.
Kemper HC, Twisk JW, Van Mechelen W, et al. A fifteen-year longitudinal study in young adults on the relation of physical activity and fitness with the development of the bone mass: the Amsterdam Growth and Health Longitudinal Study. Bone. 2000;27:847–53. https://doi.org/10.1016/s8756-3282(00)00397-5.
Maia JAR, Lefevre J, Beunen G, Claessens A. A estabilidade da aptidão física: o problema, essência analítica, insuficiências e apresentação de uma proposta metodológica baseada em estudos de painel com variáveis latentes. Movimento. 1998;5(9):58–79. https://doi.org/10.22456/1982-8918.2387.
Barnekow-Bergkvist M, Hedberg G, Pettersson U, Lorentzon R. Relationships between physical activity and physical capacity in adolescent females and bone mass in adulthood. Scand J Med Sci Sports. 2006;16(6):447–55. https://doi.org/10.1111/j.1600-0838.2005.00500.x.
Faulkner RA, Mirwald RL, Baxter-Jones A, Bailey DA. The relationship of physical fitness at adolescence to adult bone mineral density. Abstracts from the 23rd Annual Meeting of the American Society for Bone and Mineral Research. Phoenix, Arizona, USA, 2001.
Manolagas SC, Almeida M, Jilka RL. Gonadal steroids. In Primer on the metabolic bone diseases and disorders of mineral metabolism; Rosen, C.J., Ed.; John Wiley & Sons:195–207. 2013.
Janz KF, Letuchy EM, Burns TL, Francis SL, Levy SM. Muscle power predicts adolescent bone strength: Iowa Bone Development Study. Med Sci Sports Exerc. 2015;47(10):2201–6. https://doi.org/10.1249/MSS.0000000000000648.
Torres-Costoso A, Gracia-Marco L, Sánchez-López M, et al. Lean mass as a total mediator of the influence of muscular fitness on bone health in schoolchildren: a mediation analysis. J Sports Sci. 2015;33(8):817–30. https://doi.org/10.1080/02640414.2014.964750.
Jürimäe T, Hurbo T, Jürimäe J. Relationships between legs bone mineral density, anthropometry and jumping height in prepubertal children. Coll Antropol. 2008;32(1):61–6. PMID: 18494189.
Wind AE, Takken T, Helders PJ, Engelbert RH. Is grip strength a predictor for total muscle strength in healthy children, adolescents, and young adults? Eur J Pediatr. 2010;169(3):281–7. https://doi.org/10.1007/s00431-009-1010-4.
Hart NH, Nimphius S, Rantalainen T, et al. Mechanical basis of bone strength: influence of bone material, bone structure and muscle action. J Musculoskelet Neuronal Interact. 2017;17(3):114–39. PMID: 28860414.
Vicente-Rodríguez G, Urzanqui A, Mesana MI, et al. Physical fitness effect on bone mass is mediated by the independent association between lean mass and bone mass through adolescence: a cross-sectional study. J Bone Miner Metab. 2008;26(3):288–94. https://doi.org/10.1007/s00774-007-0818-0.
Zymbal V, Baptista F, Letuchy EM, Janz KF, Levy SM. Mediating effect of muscle on the relationship of physical activity and bone. Med Sci Sports Exerc. 2019;51(1):202–10. https://doi.org/10.1249/MSS.0000000000001759.
Garrido-Miguel M, Torres-Costoso A, Martínez-Andrés M, et al. The risk of eating disorders and bone health in young adults: the mediating role of body composition and fitness. Eat Weight Disord. 2019;24(6):1145–54. https://doi.org/10.1007/s40519-017-0458-x.
Ward RC, Janz KF, Letuchy EM, Peterson C, Levy SM. Contribution of High School Sport participation to Young Adult Bone Strength. Med Sci Sports Exerc. 2019;51(5):1064–72. https://doi.org/10.1249/MSS.0000000000001870.
Gil-Cosano JJ, Gracia-Marco L, Ubago-Guisado E, et al. Muscular fitness mediates the Association between 25-Hydroxyvitamin D and areal bone Mineral density in children with Overweight/Obesity. Nutrients. 2019;11(11):2760. https://doi.org/10.3390/nu11112760.
Henriques-Neto D, Magalhães JP, Júdice P, et al. Mediating role of physical fitness and fat mass on the associations between physical activity and bone health in youth. J Sports Sci. 2020;38(24):2811–8. https://doi.org/10.1080/02640414.2020.1801326.
Acknowledgements
The authors would like to thank the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq). E.R.V.R. and R.A.F. are supported by CNPq for the research productivity grant; and the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for the master’s grants awarded to JCC.
Funding
There is no funding source.
Author information
Authors and Affiliations
Contributions
CB: Conception and design, analysis and interpretation of data, drafting the article, final approval; JC: Conception and design, analysis and interpretation of data, drafting the article, final approval; CR: Acquisition of data, conception, revising it critically, final approval; MB: Acquisition of data, conception, revising it critically, final approval; GBS: Acquisition of data, conception, revising it critically, final approval; RF: Revising it critically, final approval; DM: Revising it critically, final approval; TO: Revising it critically, final approval; DR: Revising it critically, final approval; MCS: Analysis and interpretation of data, revising it critically, final approval; ER: Conception and Design, analysis and interpretation of data, drafting the article, final approval.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was approved by the Ethics Committee in Research with Human Beings of the State University of Londrina (document 1.340.735) and complies with the Declaration of Helsinki on human research. All participants signed the Free and Informed Consent Term and the Infant Assent Term.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Barbosa, C.C.L., da Costa, J.C., Romanzini, C.L.P. et al. Interrelationship between muscle fitness in childhood and bone mineral density in adulthood: mediation analysis of muscle fitness in adulthood. BMC Public Health 23, 648 (2023). https://doi.org/10.1186/s12889-023-15545-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12889-023-15545-7