
Abstract
Background
Schwannomas are benign usually encapsulated nerve sheath tumors derived from the Schwann cells, and affecting single or multiple nerves. The tumors commonly arise from the cranial nerves as acoustic neurinomas but they are extremely rare in the pelvis and the retroperitoneal area. Retroperitoneal pelvic schwannomas often present with non-specific symptoms leading to misdiagnosis and prolonged morbidity.
Case presentation
We report the case of a 59-year-old woman presenting with a feeling of heaviness in the lower abdomen who was found to have a retroperitoneal pelvic schwannoma originating from the right femoral nerve. She had a history of two resections of peripheral schwannomas at four different sites of limbs. After conducting magnetic resonance imaging, this pelvic schwannoma was misdiagnosed as a gynecological malignancy. The tumor was successfully removed by laparoscopic surgery. Pathological analysis of the mass revealed a benign schwannoma of the femoral nerve sheath with demonstrating strong, diffuse positivity for S-100 protein.
Conclusions
Although retroperitoneal pelvic schwannoma is rare, it should be considered in the differential diagnosis of pelvic masses, especially in patients with a history of neurogenic mass or the presence of neurogenic mass elsewhere.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Schwannomas (neurilemmomas), are encapsulated nerve sheath tumors derived from the Schwann cells, and affecting single or multiple nerves [1]. Most schwannomas are benign and grow slowly. Schwannomas can arise in peripheral, cranial, or visceral nerves at any anatomic site of the human body [2].These tumors commonly arise from the cranial nerves as acoustic neurinomas, but are extremely rare in the pelvis and the retroperitoneal area [3]. Retroperitoneal schwannomas often present with non-specific symptoms leading to misdiagnosis and prolonged morbidity. Retroperitoneal pelvic schwannomas are easily confused with gynecological tumors. Herein, we report a case of multiple schwannomas, most likely schwannomatosis, in which the retroperitoneal pelvic schwannoma was located in the right femoral nerve, misdiagnosed as gynecological malignancy by preoperative imaging.
Due to numbness in the left middle finger and ring finger, the patient underwent resection of a solid tumor in the left axilla 27 years ago. The postoperative pathology showed that it was a schwannoma originating from the median nerve. 16 years ago, the patient developed right palm pain, right calf and sole pain, and multiple soft tissue masses in the right upper and lower extremities could be palpated on physical examination. Surgery confirmed that these tumors were all schwannomas, originating from the right ulnar, sciatic, and peroneal nerves, respectively. In the past 5 years, the patient complained of occasional paroxysmal radiating pain in the right inguinal area and the right leg, accompanied by a feeling of bulging in the lower abdomen, and no obvious abnormality in the motor and sensory function of the lower limbs.
Case presentation
A 59-year-old postmenopausal woman, gravida 2 para 1, obtained a pelvic ultrasound examination at a local hospital 1 year ago. Ultrasound showed multiple uterine fibroids and a cystic-solid mass in the right adnexal area with a size of 3.5 × 3.4 × 3.0 cm. The patient underwent laparoscopic resection of the entire uterus and both adnexa at the same hospital, and no tumor was found in the bilateral adnexal areas during the operation. Histopathology of both ovaries was normal. Half a year after the operation, the patient came to the gynecology out-patient department of our hospital complaining a sense of heaviness in the lower abdomen. During the physical examination, a solid mass was touched in the right pelvis with obvious tenderness. The transvaginal ultrasound scan showed a 3.5 × 3.2 × 3.5 cm solid-based mass in the right adnexa, adjacent to the bladder. The mass was well-defined, hypoechoic with multiple small anechoic cystic areas, vascularized on Doppler (Fig. 1). During the examination, the patient described a palpable nodule on the inner of her right thigh. Ultrasound showed a 3.9 × 2.6 cm solid mass in the deep muscle of right thigh, which was considered as a neurogenic tumor (Fig. 2). The level of CA125, AFP and CEA were normal. The pelvic magnetic resonance imaging (MRI) revealed a round mass on the right side of the pelvis, hypointense on T1, hyperintense but heterogenous on T2, hyperintense on diffusion-weighted imaging, and the solid part of the mass with obvious contrast-enhancement (Fig. 3). The appearance of the lesion on MRI was suggestive of a malignant tumor of the right ovary. After that, the patient underwent a trunk 18 F-fluorodeoxyglucose positron emission tomography and computed tomography (FDG-PET/CT) examination, which confirmed the presence of the pelvic mass with increased tracer uptake, and a metabolic enhancement of lesion was also seen in the right thigh muscles, with 2.7 cm, both considered malignant lesions (Fig. 4).

The transvaginal ultrasound at diagnosis. a and b A well-defined, hypoechoic mass is in the right adnexa, adjacent to the bladder. c Color Doppler image shows the mass contains internal flow. BL bladder

Ultrasound shows a solid mass in the deep muscle of right thigh suspiciously originating from the nerve. a The mass is located 1.9 cm away from the thigh surface. b Doppler flow can be detected in the mass

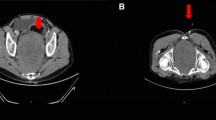
The MRI reveals a round mass in the pelvis (arrow). a Hypointense on T1. b Hyperintense but heterogenous on T2. c Hyperintense on diffusion-weighted imaging. d The solid part of the mass with obvious contrast-enhancement. MRI magnetic resonance imaging

The trunk PET/CT examination confirm the presence of the pelvic mass and the lesion in the right thigh muscles. a and b Both the pelvic mass (thick arrow) and the mass in the right thigh (thin arrow) show high tracer uptake. PET/CT positron emission tomography and computed tomography
After consultation, the surgeon considered that this pelvic mass was likely to be a schwannoma of retroperitoneal origin combining the patient's medical history and clinical symptoms. On August 2021, the patient was hospitalized and opted for surgical removal of the pelvic mass. Laparoscopic exploration showed smooth pelvic floor and lateral pelvic wall peritoneum, and no obvious protrusions and space-occupying lesions were found. The right retroperitoneum was opened along the stump of the infundibulopelvic ligament, clearly showing the lateral ureter and iliac vessels. The obturator fossa was explored, and no significant lesions were found.
The gynecologist checked the MRI and PET/CT images again, and finally determined that the mass was located in the retroperitoneum of the pelvic floor on the right side of the bladder. Cutting the peritoneum on the surface of the mass, a smooth and encapsulated solid mass was visible (Fig. 5), attached to the right femoral nerve surface. The right quadriceps muscle was contracted and the right hip and knee joints were straightened when the mass was touched. The tumor well dissected from the surface of the femoral nerve and totally removed with no neural damage. Macroscopically, the mass was cystic and solid with yellow bean dregs-like contents. Finally, the tumor was diagnosed as a benign retroperitoneal schwannoma, and histopathological morphology showed on standard coloration a spindle-shaped proliferation of cells without cyto-nuclear atypia, with numerous hyalinized vessels. On immunohistochemistry, the whole schwannoma cellular population demonstrated strong, diffuse positivity for S-100 protein (Fig. 6). After surgery, the patient recovered smoothly and left the hospital 7 days later. The patient had no numbness, pain or abnormal movement of the lower limbs during follow-up.

Laparoscopic procedure. a Encapsulated solid mass in the retroperitoneal pelvis. b The mass was removed intact

Histopathologic examination of the benign schwannoma. a × 200. b Strong immunohistochemical positivity for S-100 protein
Discussion and conclusions
To our knowledge, this is the first case of a retroperitoneal pelvic schwannoma following a history of resection of multiple peripheral schwannomas of the extremities, and the present mass in the right thigh is also considered as a schwannoma. The presence of multiple schwannomas is associated with neurofibromatosis (NF). There are three types of NF: type 1 (NF1) accounting for 96% of all cases, type 2 (NF2) in 3%, and schwannomatosis in < 1% [4, 5]. Schwannomatosis is characterized by multiple schwannomas of the peripheral nervous system in the absence of vestibular schwannomas [6]. This patient has no family history of neurofibromas, no NF1- or NF2-related stigmata on physical examination, and no clinical manifestations of hearing impairment. Although she did not have a cranial MRI examination, schwannomatosis is the most likely diagnosis.
Schwannomas are rarely found in the retroperitoneal region (less than 0.5% of cases) [2]. When located in pelvis, they can be misdiagnosed as uterine myoma [7] or adnexal masses [8, 9]. Retroperitoneal schwannomas are slow-growing tumours and do not cause many symptoms until they have attained a large size. They may cause some symptoms secondary to pressure on adjacent nerves, vessels and organs, such as vague pain in the lower back, abdomen and pelvis. Most patients have no specific clinical symptoms, and the preoperative diagnosis rate is low, which often leads to insufficient preoperative preparation and a passive state during surgery.
Preoperative diagnosis of pelvic and retroperitoneal schwannomas is difficult as there are no specific imaging findings. A review of 82 retroperitoneal schwannomas revealed that only 15.9% were identified preoperatively by ultrasound, CT, or MRI [10]. MRI is the optimal imaging tool for these kinds of tumors [11], since it is able also to show its possible origin, vascularization, and invasiveness, and can even definitively diagnose pelvic schwannomas [3]. MRI also helps to clarify the relationship with neighboring pelvic organs (sacrum, rectum, and bladder), which is an important consideration for the surgical procedure [12], but misdiagnosis is not uncommon. In addition, MRI is often used to check the abdominal and pelvic cavity, but multiple schwannomas such as soft tissues of the limbs can not be simultaneously explored. Even experienced radiologists cannot comprehensively consider giving an accurate diagnosis. Some scholars suggested that a whole-body MRI examination should be uesed to exclude multiple schwannomas [13]. This patient had a clear history of uterine and oophorectomy surgery, and the MRI report still suggested an ovarian-derived malignant mass, possibly due to the heterogeneity of schwannoma and internal cystic changes similar to the appearance of an ovarian malignant tumor.
Ultrasonography has an important role in detecting pelvic tumors. However, pelvic schwannoma has no specific ultrasound signs and usually presents as a homogeneous hypoechoic, well-defined mass, with internal cystic changes and calcification, which is easily confused with tumors derived from uterus and ovary. With technological advances in the quality of ultrasound resolution, pelvic nerves can be visualized, a novel ultrasound imaging, ‘pelveoneurosonography’ has the potential to evaluate pelvic nerves and track the source of the tumor [13]. However, the specific effects need to be further verified by prospective studies. For patients with multiple schwannomas, ultrasound may have advantages. It can easily detect suspicious masses in other parts than the pelvis and abdominal cavity, especially in the limbs. When the probe presses the tumor and symptoms of nerve irritation occur during the examination, it is helpful to confirm the diagnosis of neurogenic tumors. This patient underwent multiple limbs schwannoma resections, and this time the right thigh mass was also diagnosed as a neurogenic tumor by ultrasound. If all these information can be taken into account, the pelvic mass may be obtained closer to the correct diagnosis before surgery. There is no consensus on the recommendation of ultrasound-guided tumor biopsy, given the difficulties of interpretation, or the risk of bleeding and infection [12, 13]. However, gynecologic ultrasound is also an optimal modality for the surveillance of retroperitoneal pelvic schwannoma, especially if the patient is asymptomatic [13].
In this case, PET/CT was performed for suspected gynecological malignancy, showing an increased accumulation of FDG in the pelvic mass and the right thigh mass, all of which were misdiagnosed as malignant lesions. According to the previous report, the large accumulation of FDG in schwannomas might result from the potential ability of schwann cells to transport glucose for axonal repolarization in the peripheral nerve system [14]; however, a consensus has not been reached on the precise mechanism of FDG accumulation in schwannomas. In our experience, when there are multiple schwannomas, PET/CT examination may be unreliable, and it is easy to misdiagnose multiple lesions as metastases. Therefore, the application of PET/CT is not recommended.
Surgical resection of the entire schwannoma is the optimal treatment. Care to avoid injury to adjacent structures and to accomplish a complete excision of the mass is essential for the safe performance of this surgery. Resection without the correct technique can cause permanent neurological deficits and pain and recurrence in up to 54% of patients [15]. Schwannomas are solitary, well-circumscribed, encapsulated tumors and do not invade local tissues. Due to these characteristics they are easily dissected from adjacent tissues. The laparoscopic approach is an effective and minimally invasive option for the resection of retroperitoneal pelvic schwannoma. However, for large retroperitoneal schwannoma, laparotomy should also be considered in order to ensure complete resection. Because patients with schwannomatosis often may undergo multiple operations at different sites during their lifetime, an interdisciplinary approach is the optimal strategy to manage benign schwannoma [15]. This patient of our study will undergo elective surgery on the right thigh mass.
To sum up, although retroperitoneal pelvic schwannoma is rare, it should be considered in the differential diagnosis of pelvic masses, especially in patients with a history of neurogenic mass or the presence of neurogenic mass elsewhere. Accurate diagnosis of retroperitoneal pelvic schwannoma ramains a challenge. Management and diagnostic experience in the course of this case, although limited, emphasizes the importance of a complete preoperative history collection, physical examination, and detailed imaging evaluation, which can improve the outcome of surgical treatment. The final diagnosis is established at histopathological examination.
Availability of data and materials
The datasets used during the current study are available from the corresponding author on reasonable request.
Abbreviations
- MRI:
-
Magnetic resonance imaging
- CT:
-
Computed tomography
- FDG:
-
F-fluorodeoxyglucose
- PET:
-
Positron emission tomography
- NF:
-
Neurofibromatosis
References
Erdoğan F, Say F, Barış YS. Schwannomatosis of the sciatic nerve: a case report. Br J Neurosurg. 2021;18:1–4.
Dawley B. A retroperitoneal femoral nerve schwannoma as a cause of chronic pelvic pain. J Minim Invasive Gynecol. 2008;15:491–3.
Tong RS, Collier N, Kaye AH. Chronic sciatica secondary to retroperitoneal pelvic schwannoma. J Clin Neurosci. 2003;10:108–11.
Kühn JP, Wagner M, Bozzato A, Linxweiler M. Multiple schwannomas of the facial nerve mimicking cervical lymphoma: a case report. J Med Case Rep. 2021;15:436.
Tamura R. Current understanding of neurofibromatosis type 1, 2, and schwannomatosis. Int J Mol Sci. 2021;22(11):5850.
Watson JT, Hernandez JA, Bartlett R. Multiple schwannomas of the lower extremity. J Am Podiatr Med Assoc. 2020;110:1–4.
Chen CH, Jeng CJ, Liu WM, Shen J. Retroperitoneal schwannoma mimicking uterine myoma. Taiwan J Obstet Gynecol. 2009;48:176–7.
Ibraheim M, Ikomi A, Khan F. A pelvic retroperitoneal schwannoma mimicking an ovarian dermoid cyst in pregnancy. J Obstet Gynaecol. 2005;25:620–1.
Aran T, Guven S, Gocer S, Ersoz S, Bozkaya H. Large retroperitoneal schwannoma mimicking ovarian carcinoma: case report and literature review. Eur J Gynaecol Oncol. 2009;30:446–8.
Li Q, Gao C, Juzi JT, Hao X. Analysis of 82 cases of retroperitoneal schwannoma. ANZ J Surg. 2007;77:237–40.
Schraepen C, Donkersloot P, Duyvendak W, et al. What to know about schwannomatosis: a literature review. Br J Neurosurg. 2022;36(2):171–4.
Zohra BF, Amine N, Hajar Z, et al. Retroperitoneal pelvic schwannoma: a rare case report and review of the literature. Radiol Case Rep. 2024;19(8):3028–32.
Fischerova D, Santos G, Wong L, et al. Imaging in gynecological disease (26): clinical and ultrasound characteristics of benign retroperitoneal pelvic peripheral-nerve-sheath tumors. Ultrasound Obstet Gynecol. 2023;62(5):727–38.
Hamada K, Ueda T, Higuchi I, et al. Peripheral nerve schwannoma: two cases exhibiting increased FDG uptake in early and delayed PET imaging. Skeletal Radiol. 2005;34:52–7.
Benato A, D’Alessandris QG, Murazio M, et al. Integrated neurosurgical management of retroperitoneal benign nerve sheath tumors. Cancers (Basel). 2023;15(12):3138.
Acknowledgements
PET/CT and pathology data were obtained from the Department of Nuclear Medicine and the Department of Pathology of Peking Union Medical College Hospital, respectively. The authors would like to thank the patient for giving informed consent for the publication of the study.
Funding
This research was supported by 2019 PUMCH Science Fund for Junior Faculty (grant no. pumch201911591), and National High Level Hospital Clinical Research Funding (grant no. 2022-PUMCH-A-090).
Author information
Authors and Affiliations
Contributions
XW, HM and QF contributed to reviewing the case, drafting the manuscript and critically revising the manuscript. ZQ and WP contributed to editing the images and reviewing the case.The authors approved the final version of the article and agree to be accountable for all aspects of the work.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
This study was performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from the patient for the publication of this report and any accompanying images.
Consent for publication
The patient consented to the submission of the clinical report to the journal.
Competing interests
The authors declare that they have no conflicts of interest and nothing to disclose.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wu, X., Meng, H., Fan, Q. et al. Image features and clinical analysis of retroperitoneal pelvic schwannoma: a case report. BMC Neurol 24, 230 (2024). https://doi.org/10.1186/s12883-024-03715-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-024-03715-y