
Abstract
Background
Hemiplegic migraines represent a heterogeneous disorder with various presentations. Hemiplegic migraines are classified as sporadic or familial based on the presence of family history, but both subtypes have an underlying genetic etiology. Mutations in the ATP1A2 gene are responsible for Familial Hemiplegic type 2 (FHM2) or the sporadic hemiplegic migraine (SHM) counterpart if there is no family history of the disorder. Manifestations include migraine with aura and hemiparesis along with a variety of other symptoms likely dependent upon the specific mutation(s) present.
Case presentation
We report the case of an adult man who presented with headache, aphasia, and right-sided weakness. Workup for stroke and various infectious agents was unremarkable during the patient’s extended hospital stay. We emphasize the changes in the Magnetic Resonance Imaging (MRI) over time and the delay from onset of symptoms to MRI changes in Isotropic Diffusion Map (commonly referred to as Diffusion Weighted Imaging (DWI)) as well as Apparent Diffusion Coefficient (ADC).
Conclusions
We provide a brief review of imaging findings correlated with signs/symptoms and specific mutations in the ATP1A2 gene reported in the literature. Description of the various mutations and consequential presentations may assist neurologists in identifying cases of Hemiplegic Migraine, which may include transient changes in ADC and DWI imaging throughout the course of an attack.
Similar content being viewed by others

Background
Migraines affect more than 10 % of the population worldwide [1]. Migraines are clinically categorized into subtypes, dependent on the presence of and types of associated auras. Hemiplegic migraine (HM) is a subtype of migraine with aura, in which the aura has motor involvement, normally hemiparesis [2]. HM can be further classified as familial (FHM) if at least one first-degree or second-degree relative also meets the criteria for HM; otherwise it is classified as sporadic [3]. Currently, three genes have been identified to be associated with FHM: CACNA1A (FHM1), ATP1A2 (FHM2), and SCN1A (FHM3) [2]. Penetrance for FHM 1, 2, and 3 appears to be high and is estimated to be approximately 80 % [2, 4, 5]. Data on the prevalence of FHM is lacking, but one study of a Danish population found it to be 0.01 % [6].
Patients with FHM typically present with their first attack within the first two decades of life. During acute attacks, many patients are initially worked up for possible stroke due to the associated hemiparesis [6, 7]. Within FHM2, there is immense variability in the clinical presentation, duration of attacks, and imaging findings. Some authors have reported perfusion computed tomography (CT) images that show hypoperfusion, others reported hyperperfusion, and some reported both throughout the attack [8, 9]. Magnetic Resonance Imaging (MRI) findings seem to vary depending on the FHM type. Cortical hyperintensities and swelling on MRI have been well described for FHM1 patients. Less is known about MRI findings for FHM2 [10].
Here, we describe a patient who presented to the emergency room with a headache, hemiparesis, and aphasia. During his extended hospital stay, we report a series of MRI studies obtained over the course of the acute attack. Genetic testing revealed a missense mutation in the ATP1A2 characteristic of FHM2.
Case presentation
A 25-year-old right-handed man presented to the emergency department with a headache, right-sided weakness, confusion, and aphasia which began the previous night (day 0). On day 0, the patient awoke late in the afternoon with a headache and some confusion according to his family. The patient then went back to sleep until the following morning. Upon awakening, the patient exhibited right-sided weakness and difficulty speaking in addition to the headache and confusion. His mother also reported the patient was nauseous and had episodes of vomiting throughout the night. The patient had a questionable history of migraine with prolonged aura. Prior to the onset of the headache, the patient was in his usual state of health. Unique to this experience, which prompted his parents to bring him to the emergency room, was the persistence of headaches, hemiplegia, and difficulty speaking. A level II stroke alert prompted a CT of his head and Computed Tomography Angiography (CTA) of his head and neck; both were negative for any signs of a stroke, stenosis, or occlusion. The consulting neurologist diagnosed the patient with atypical migraine since the symptoms were similar to those previously experienced by the patient in prior attacks. The patient was instructed to return for possible MRI of the brain if symptoms persisted and was referred to an outpatient neurology visit for follow-up. The patient was discharged with a diagnosis of atypical migraine and with instructions for follow-up or to return to the emergency department if symptoms worsened. The patient returned the following day (day 2) due to the persistence of symptoms. Thus, the patient was admitted for observation with right-sided weakness, aphasia, and fever. At 5:00 PM on day two, the patient recorded a temperature of 100.9℉. During the next several days, the patient’s temperature ranged from 98.3℉ − 102.6℉. The patient was febrile to a temperature max of 102.6℉ recorded on day 4 at 4:00 AM. The patient’s fever subsequently broke by at 6:00 AM of day 4. Of interest, the patient reported two female cousins with similar symptoms.
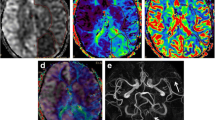
The neurological findings and fever prompted empiric treatment for meningitis. A lumbar puncture (LP) was ordered to assess for infectious etiologies. The patient was unable to be interviewed due to aphasia. History obtained from the patient’s parents revealed the patient had been working outside at a car shop and taking several stimulant weight loss supplements in the days immediately prior to admission. The clinical exam showed an alert, dysarthric patient with global aphasia and weakness in the right upper and lower extremities. The first MRI was obtained approximately two days after symptom onset. T2-fluid-attenuated inversion recovery (FLAIR) showed no signs of acute intracranial abnormality but did show scattered hyperintensities in the white matter of frontal lobes bilaterally (Fig. 1).

MRI obtained on day 2 did not reveal any acute intracranial abnormality. However, scattered, non-enhancing punctate T2-FLAIR hyperintensities in subcortical white matter were present bilaterally in the frontal lobes. Day 4: Diffuse DWI and T2-FLAIR hyperintensities throughout the left cerebral hemisphere cortices, most pronounced over the lateral convexity. Possible associated T2 shinethrough rather than restricted diffusion. Associated sulcal effacement from gyral swelling. Day 7:Diffuse DWI and T2-FLAIR hyperintensities throughout the left cerebral hemisphere cortices similar to the MRI findings obtained on day 4. Subtle hypointensity on ADC in left cerebral hemisphere cortices and posterior temporal lobe. Day 11: Diffuse DWI and T2-FLAIR hyperintensities throughout the left cerebral hemisphere cortices similar to previous MRI findings. Mild hypointensity on ADC in the left cerebral hemisphere corticesand temporal lobe is more prominent compared to previous MRIs. Day 15: Diffuse DWI and T2-FLAIR hyperintensities throughout the left cerebral hemisphere cortices similar to previous MRIs. Mild hypointensity on ADC in left cerebral hemisphere cortices is even more prominent compared to previous MRIs. Day 154:Previously demonstrated left cerebral hemisphere cortical swelling and restricted diffusion has resolved. No new parenchymal signal abnormality or abnormal enhancement. Scattered non-enhancing punctate T2-FLAIR hyperintensities were present in subcortical white matter of bilateral frontal lobes similar to the first MRI
On the day following his admission (day 3), the results of the patient’s LP showed clear, colorless fluid which was negative for xanthochromia. Glucose and protein were within normal limits while white blood cells and red blood cells showed 2 cells/mm3 and 1 cells/mm3 respectively. Polymerase Chain Reaction (PCR) was negative for enterovirus, herpes-simplex virus (HSV) 1 and 2, and cryptococcal antigens. The culture of the cerebrospinal fluid (CSF) was ultimately negative for bacterial species, but his fever persisted. He underwent seizure-like activity which prompted treatment with 1 mg Intravenous (IV) Lorazepam and subsequent resolution of the episode. A loading dose of 1000 mg of IV Levetiracetam followed by 500 mg twice a day as well as further workup was ordered. Another MRI was obtained the day following his seizure-like activity (day 4), which showed diffuse diffusion-weighted imaging (DWI) and T2/FLAIR hyperintensities throughout the left cerebral hemisphere cortices. Electroencephalogram (EEG) was ordered and returned abnormal results indicative of global central nervous system (CNS) dysfunction and focal dysfunction of the left hemisphere. Encephalitis was suspected, but the exact etiology was still unknown.
Empiric treatment for bacterial meningitis was discontinued on day 5 following negative LP and advice from infectious disease consultations. With a tick-borne molecular panel still pending, empiric treatment with doxycycline was advised. HIV, fungal, bacterial, and viral agents all returned negative. On day 7, the patient experiences a generalized tonic-clonic (GTC) seizure which resulted in the decision to start long-term EEG and repeat MRI. The repeat MRI showed similar findings to the previous MRI - T2/FLAIR hyperintensity of the left cerebral cortex without enhancement and associated sulcal effacement. At this time, the differential was still broad including encephalitis of viral, neoplastic, autoimmune, or idiopathic origins. A steroid regimen was employed.
Figure 1 highlights the MRI findings throughout the course of the patient’s hospital stay as well as the resolution and follow-up visits. Day 11 was notable for more prominent hypointensity on Apparent Diffusion Coefficient (ADC) in the left cerebral hemisphere cortices and temporal lobe. MRI on day 15 revealed even more prominent hypointensity on ADC. Continuous EEG recording was started on day 12 and continued for 9 days. The findings from EEG were largely non-specific but included left-hemispheric slowing with mild diffuse slowing. By the end of the EEG recordings, the left hemispheric attenuation had largely resolved.
To rule out germ cell tumor, CT of the chest, abdomen and pelvis was obtained on day 16 and showed no evidence of neoplasm. Despite the lack of success identifying a causal agent, the patient showed signs of clinical improvement with the persistence of the aphasia. Due to the negative LPs, the negative pan CT, and non-specific EEG findings, the differential now included limbic encephalitis, autoimmune, prion disease, Transient Headache and Neurologic Deficits With Cerebrospinal Fluid Lymphocytosis (HaNDL syndrome) and last, but not least, the Rasmussen syndrome. LP, anti-Hu/Ma, anti-Ta, anti-NR1, anti-AQP4, anti-CASPR2, anti-LGI1, anti-Yo, oligoclonal bands, ANA, anti-double stranded DNA, complement C3 and C4, SSA-SSB antibody, RNP-SM antibody, encephalitis antibody evaluation (ANNA-1/anti-Hu, ANNA-2/anti-Ri, ANNA-3, PCA-1/anti-Yo, PCA-2, PCA-TR/anti-Tr, AGNA/anti-SOX1, Amphiphysin Ab, anti-CRMP5/anti-CV2, anti-GAD65, anti-MA2/Ta anti-myelin, AQP4/Ab/NMO-IgG), an epilepsy autoimmune evaluation (AChR Ganglionic Neuronal Ab, AMPA-R Ab, Amphiphysin Ab, AGNA-1, ANNA-1/anti-Hu, ANNA-2/anti-Ri, ANNA-3, CASPR2-IgG, CRMP-5-IgG, DPPX Ab, GABA-B-R Ab, anti-GAD65, anti-GFAP, LGI1-IgG CBA, mGluR1 Ab, NMDA-R Ab, N-Type Calcium Channel Ab, P/Q-Type Calcium Channel Ab, PCA-2, PCA-Tr), a neurology antibody order (ANNA-1/anti-Hu, ANNA-2/anti-Ri, PCA-1/anti-Yo, PCA-TR/anti-Tr, AGNA/anti-SOX1, anti-Ma2/Ta, anti-Zic4, anti-CRMP5/anti-CV2, amphiphysin Ab, anti-GAD65) and protein 14-3-3 were ordered as part of the follow-up. The decision was made to start the patient on a course of IVIG while additional investigations were still pending. The patient showed improvement after starting the IVIG and was discharged on multiple medications including lamotrigine, levetiracetam, magnesium chloride, riboflavin, valproate sodium and instructions with close follow-ups. At the outpatient follow-up with neurology, the patient showed significant improvements in language, showed no stroke-like symptoms, and denied any seizure-like activity. The rest of the laboratory investigations were unremarkable except genetic testing. The analysis of four genes (ATP1A2, CACNA1A, SCN1A, PRRT2), was positive for a heterozygous, AD mutation in ATP1A2 (c.2936 C > T p. P979L). The patient had a recurrence of seizure which resulted in another short hospital stay.
Discussion and conclusions
The ATP1A2 gene mutation found in FHM2 patients affects an ATPase found primarily in the CNS, specifically in hippocampal astrocytes and pyramidal cells. Dysfunction of this protein is thought to lead to increased extracellular K+, intracellular Na+, and intracellular Ca2+, all contributing to cortical spread depression which has been hypothesized to be the pathophysiological mechanism of the migraine aura [9, 11,12,13,14]. Various mutations in the ATP1A2 gene lead to phenotypically heterogeneous presentations of FMH2 which have been previously described [9]. The various presentations of mutations in ATP1A2 often require ruling out life-threatening causes of hemiparesis, such as stroke and infectious meningoencephalitis [7, 15]. One common finding amongst FHM2 patients is the presence of a fever [6, 9, 10, 15], also frequently found in FHM1 patients [14, 16].
Table 1 includes clinical presentations, imaging findings, and genetic testing if performed for patients with hemiplegic migraines with an ATP1A2 mutation undergoing severe attacks published in the last ten years [6, 9, 10, 15, 17,18,19,20,21,22,23,24]. Perfusion studies on FHM2 patients have demonstrated both hypo- and hyperperfusion. This could potentially be explained by a biphasic change in cerebral blood flow experienced during acute attacks [8]. A previous theory suggested that the aura phase was related to hypoperfusion and headache with hyperperfusion [7]. However, the finding that aura symptoms can persist when imaging studies demonstrate hyperperfusion opposes this theory. More research is needed to understand the relationship, if any, between perfusion changes and clinical signs/symptoms of FHM patients. Dynamic MRI changes during attacks are demonstrated in both previous reports as well as this patient.
The symptoms experienced by our patient during the acute attack were not associated with MRI changes within the initial days of migraine onset. This is consistent with previous findings described by Roth et al. [10] which suggested that changes in imaging tend to be found later during the course of an attack. This dissociation of clinical symptoms and imaging findings is not unique to FHM patients and is also notably found in Reversible Cerebral Vasoconstriction Syndrome [25]. In our patient, cortical swelling and restricted diffusion in the left cerebral hemisphere was appreciated by day 4 of the attack and persisted throughout the series of MRI images obtained during the course of the patient’s hospital stay. A unique feature of our patient’s imaging findings is the hypointensities observed on ADC. This finding was not reported in the studies included in Table 1. Belvís at al. [26] describe transient changes in ADC seen during a persistent visual aura which seems similar to the findings observed in our patient. Future studies of the condition may benefit from the inclusion of transcranial doppler or angiography to further observe these reversible vasospasms.
Consistent with similar cases described in literature, these imaging changes resolved overtime. The reversible encephalopathy that can occur during these migraine attacks has been described by the studies summarized in Table 1, which illustrates the diversity of findings observed during attacks in patients with various mutations in ATP1A2. The patient presented here provides a chance to examine five MRIs obtained throughout the course of the prolonged attack as well as an MRI obtained after resolution of symptoms. The importance of this paper is to describe not only the phenotypic changes, but also the imaging findings across the course of attacks in patients with various mutations in the ATP1A2 gene (FMH2). When possible, we present the mutation, clinical features and imaging findings found during various days into each described encounter. This attempt to combine and present findings may be a useful resource for clinicians to appreciate the heterogeneous nature of the disease described from the genetic, clinical and imaging perspectives in various mutations of ATP1A2.
Many patients experiencing a FHM attack are treated with various antivirals, antibacterials, antiepileptics, corticosteroids, and migraine medications. Unique to our patient’s treatment plan was the use of IVIG for presumed autoimmune encephalitis as encephalitis can present similarly. IVIG was started on day 18 and symptoms improved on day 19. Granted, this observation cannot be solely attributed to IVIG targeting an immune etiology as it may represent a naturally resolving attack, especially given the original baseline health, timeline of symptoms, and the genetic confirmation of FHM. Immunological interventions have historically not been the treatment of choice in FHM patients. Here they were used after bacterial meningitis had been ruled out, but while various investigations were still pending.
Multiple mutations and resultant phenotypic findings have been described in patients with FHM2. Here, we summarize a number of studies that describe imaging findings found at the time of various clinical signs and symptoms with respect to the specific mutation present in ATP1A2. We also present transient changes in MRI sequences during an acute attack in this FHM2 patient, which highlights some nuanced findings such as hypointensities present on ADC imaging.
Availability of data and materials
The dataset referenced for this study can be de-identified and made available by request to the corresponding author with appropriate data usage agreements.
Abbreviations
- HM:
-
Hemiplegic Migraine
- FHM:
-
Familial Hemiplegic Migraine
- SHM:
-
Sporadic Hemiplegic Migraine
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- CTA:
-
Computed tomography angiography
- LP:
-
Lumbar puncture
- FLAIR:
-
Fluid-attenuated inversion recovery
- PCR:
-
Polymerase chain reaction
- HSV:
-
Herpes-simplex virus
- CSF:
-
Cerebrospinal fluid
- IV:
-
Intravenous
- DWI:
-
Diffusion-weighted imaging
- EEG:
-
Electroencephalogram
- CNS:
-
Central nervous system
- GTC:
-
Generalized tonic-clonic
- ADC:
-
Apparent diffusion coefficient
- HaNDL:
-
Transient headache and neurologic deficits with cerebrospinal fluid lymphocytosis
- ANNA:
-
Antineuronalnuclear antibody type 1
- anti-PCA:
-
Purkinje cell cytoplasmic antibody
- AGNA:
-
Anti-glianuclear antibody
- CRMP:
-
Collapsinresponse mediator protein
- GAD:
-
Glutamicacid decarboxylase
- AQP4:
-
Aquaporin-4
- AMPA:
-
Alpha-amino-3-hydroxyl-5-methyl-4-isoxazolepropionicacid
- CASPR:
-
Contactin-associatedprotein
- DPPX:
-
Dipeptidyl-peptidase-likeprotein 6
- GABA-B-R:
-
Gamma-aminobutyricacid-B receptor
- GFAP:
-
Glialfibrillary acidic protein
- LGI-1:
-
Leucine-richglioma-inactivated
- mGluR1:
-
Metabotropic glutamate receptor 1
- NMDA-R:
-
N-methyl-d-aspartatereceptor
- APT/CEST-MRI:
-
Amideproton transfer chemical exchange saturation transfer magnetic resonanceimaging
- cMRI:
-
Cardiovascularmagnetic imaging resonance
- MRA:
-
Magnetic resonance angiography
- SPECT:
-
Single-photon emission computed tomography
References
Woldeamanuel YW, Cowan RP. Migraine affects 1 in 10 people worldwide featuring recent rise: A systematic review and meta-analysis of community-based studies involving 6 million participants. J Neurol Sci. 2017;372:307–15. doi:https://doi.org/10.1016/j.jns.2016.11.071.
Jen JC. Familial Hemiplegic Migraine. In: Adam MP, Ardinger HH, Pagon RA, et al., eds. GeneReviews®. Seattle (WA): University of Washington, Seattle; 1993.
Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia. 2004;24(Suppl 1):9–160. doi:https://doi.org/10.1111/j.1468-2982.2003.00824.x.
Jurkat-Rott K, Freilinger T, Dreier JP, Herzog J, Gobel H, Petzold GC, et al. Variability of familial hemiplegic migraine with novel A1A2 Na+/K+-ATPase variants. Neurology. 2004;62:1857–61.
Riant F, De Fusco M, Aridon P, Ducros A, Ploton C, Marchelli F, et al. ATP1A2 mutations in 11 families with familial hemiplegic migraine. Hum Mutat. 2005;26:281.
Blicher JU, Tietze A, Donahue MJ, Smith SA, Østergaard L. Perfusion and pH MRI in familial hemiplegic migraine with prolonged aura. Cephalalgia. 2016;36(3):279–83. doi:https://doi.org/10.1177/0333102415586064.
Lindahl AJ, Allder S, Jefferson D, Allder S, Moody A, Martel A. Prolonged hemiplegic migraine associated with unilateral hyperperfusion on perfusion weighted magnetic resonance imaging. J Neurol Neurosurg Psychiatry. 2002;73(2):202–3. doi:https://doi.org/10.1136/jnnp.73.2.202.
Iizuka T, Tominaga N, Kaneko J, Sato M, Akutsu T, Hamada J, et al. Biphasic neurovascular changes in prolonged migraine aura in familial hemiplegic migraine type 2. J Neurol Neurosurg Psychiatry. 2015;86(3):344–53. doi:https://doi.org/10.1136/jnnp-2014-307731.
Martínez E, Moreno R, López-Mesonero L, Vidriales I, Ruiz M, Guerrero AL, et al. Familial hemiplegic migraine with severe attacks: a new report with ATP1A2 mutation. Case Rep Neurol Med. 2016;2016:3464285. doi:https://doi.org/10.1155/2016/3464285.
Roth C, Ferbert A, Huegens-Penzel M, Siekmann R, Freilinger T. Multimodal imaging findings during severe attacks of familial hemiplegic migraine type 2. J Neurol Sci. 2018;392:22–7. doi:https://doi.org/10.1016/j.jns.2018.06.019.
Burstein R, Noseda R, Borsook D. Migraine: multiple processes, complex pathophysiology. J Neurosci. 2015;35:6619–29.
Faraguna U, Nelson A, Vyazovskiy VV, Cirelli C, Tononi G. Unilateral cortical spreading depression affects sleep need and induces molecular and electrophysiological signs of synaptic potentiation in vivo. Cereb Cortex. 2010;20:2939–47.
Leao AA. Spreading depression of activity in the cerebral cortex. J Neurophysiol. 1944;7:359–90.
Mourand I, Menjot de Champfleur N, Carra-Dallière C, Le Bars E, Roubertie A, Bonafé A, et al. Perfusion-weighted MR imaging in persistent hemiplegic migraine. Neuroradiology. 2012;54(3):255–60. doi:https://doi.org/10.1007/s00234-011-0946-z.
Iizuka T, Takahashi Y, Sato M, Yonekura J, Miyakawa S, Endo M, et al. Neurovascular changes in prolonged migraine aura in FHM with a novel ATP1A2 gene mutation. J Neurol Neurosurg Psychiatry. 2012;83(2):205–12. doi:https://doi.org/10.1136/jnnp-2011-300843.
Fernandez DM, Hand CK, Sweeney BJ, Parfrey NA. A novel ATP1A2 gene mutation in an Irish familial hemiplegic migraine kindred. Headache. 2008;48(1):101–8. doi:https://doi.org/10.1111/j.1526-4610.2007.00848.x.
Asghar SJ, Milesi-Hallé A, Kaushik C, Glasier C, Sharp GB. Variable manifestations of familial hemiplegic migraine associated with reversible cerebral edema in children. Pediatr Neurol. 2012;47(3):201–4. doi:https://doi.org/10.1016/j.pediatrneurol.2012.05.006.
Guedj E, Belenotti P, Serratrice J, Ene N, Pineau S, Donnet A, et al. Partially reversible cortical metabolic dysfunction in familial hemiplegic migraine with prolonged aura. Headache. 2010;50(5):872–7. doi:https://doi.org/10.1111/j.1526-4610.2010.01634.x.
Hermann A, Engelandt K, Rautenstrauss B, Reichmann H, Jacobasch E. Hemiplegic migraine with reversible cerebral vasoconstriction caused by ATP1A2 mutations. J Neurol. 2013;260(8):2172–4. doi:https://doi.org/10.1007/s00415-013-7010-3.
Murphy OC, Merwick A, OʼMahony O, Ryan AM, McNamara B. Familial hemiplegic migraine with asymmetric encephalopathy secondary to ATP1A2 mutation: a case series. J Clin Neurophysiol. 2018;35(1):e3–7. doi:https://doi.org/10.1097/WNP.0000000000000387.
Rispoli MG, Di Stefano V, Mantuano E, De Angelis MV. Novel missense mutation in the ATP1A2 gene associated with atypical sporadic hemiplegic migraine. BMJ Case Rep. 2019;12(10):e231129. Published 2019 Oct 5. doi:https://doi.org/10.1136/bcr-2019-231129.
Schwarz G, Anzalone N, Baldoli C, Impellizzeri M, Minicucci F, Comi G, et al. Pediatric sporadic hemiplegic migraine (ATP1A2 gene): a case report and brief literature review. Neurol Sci. 2018;39(Suppl 1):69–71. doi:https://doi.org/10.1007/s10072-018-3405-3.
Toldo I, Cecchin D, Sartori S, Calderone M, Mardari R, Cattelan F, et al. Multimodal neuroimaging in a child with sporadic hemiplegic migraine: a contribution to understanding pathogenesis. Cephalalgia. 2011;31(6):751–6. doi:https://doi.org/10.1177/0333102410392068.
Wilbur C, Buerki SE, Guella I, Toyota EB, Evans DM, McKenzie MB, et al. An infant with epilepsy and recurrent hemiplegia due to compound heterozygous variants in ATP1A2. Pediatr Neurol. 2017;75:87–90. doi:https://doi.org/10.1016/j.pediatrneurol.2017.06.003.
Miller TR, Shivashankar R, Mossa-Basha M, Gandhi D. Reversible Cerebral Vasoconstriction Syndrome, Part 2: Diagnostic Work-Up, Imaging Evaluation, and Differential Diagnosis. AJNR Am J Neuroradiol. 2015;36(9):1580–8. doi:https://doi.org/10.3174/ajnr.A4215.
Belvís R, Ramos R, Villa C, Segura C, Pagonabarraga J, Ormazabal I, et al. Brain apparent water diffusion coefficient magnetic resonance image during a prolonged visual aura. Headache. 2010;50(6):1045–9.
Acknowledgements
We acknowledge Geisinger Health System for their support. We also would like to acknowledge the patient and his parents for their consent to share these findings.
Disclosure statement
The authors have no conflict of interest to share.
Funding
None.
Author information
Authors and Affiliations
Contributions
DF, MP and RZ contributed to the design and depth of the manuscript. DF and MP researched the necessary background information. DF reviewed the patient’s records to synthesize the case report as well as contributed to the literature review and imaging selections. MP conducted most of the literature review and designed the summary table. RZ interviewed and examined the patient. RZ also reviewed all imaging and advised on findings. All authors contributed to manuscript revision. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent for publication was obtained from the patient. A copy of the consent form is available for review by the Editor of this journal.
Competing interests
All authors declare that there are no conflicts of interest
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Fear, D., Patel, M. & Zand, R. Serial magnetic resonance imaging findings during severe attacks of familial hemiplegic migraine type 2: a case report. BMC Neurol 21, 173 (2021). https://doi.org/10.1186/s12883-021-02201-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12883-021-02201-z