
Abstract
The interaction of anticipatory and reflexive changes in the grip force of the right hand was tested for the effect on the grip force developed by the thumb and index finger of the left hand. The test task for the right hand was the same in all test variants, to hold a cup where a weight fell (with the thumb and index finger). Three different tasks were chosen for the left hand. In the first task, the left fingers touched a sensor with a negligible grip force. In the second task, the subject had to hold a force sensor loaded with a 200-g load. In the third task, the subject was instructed to slowly increase the grip force by fingers of both hands. In response to the impact of the falling weight, an involuntary increase was observed in the grip force of the right-hand fingers, depending on the available visual information of the falling weight and being independent of the motor task performed by left hand. When the subject’s eyes were closed, the grip force increased in all tasks as a response to the impact of the weight fall. When the subject’s eyes were open, an automatic increase in the right-hand grip force occurred 200–300 ms before the impact. The left-hand grip force changed in different ways. In the first and second tasks, the grip force of the left hand did not change despite the changes in the grip force of the right hand in response to the impact of the falling weight. In case of a coordinated slow increase in the grip forces of both hands, an increase in the grip force was observed in the unaffected left hand before the impact and during the response to the impact, like in the right hand. Thus, a common motor task for both hands led to similar changes in grip force, which were recorded in both right and left hands not only during the response to an external stimulus, but also during anticipation. Movement planning was assumed to involve the organization of left–right interaction at the supraspinal level, probably, at the level of motor cortex interactions between the left and right hemispheres.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
Movements of right and left limbs may be coordinated at different levels. As early as 1910, Sherrington [1] described a cross reflex where unilateral stimulation of peripheral nerves causes a contralateral response due to interactions of neurons from different sides of the spine. Bilateral neuronal activity coordination probably plays an important role in the functions of the postural control and locomotor system. Voluntary movements of hands and fingers are mostly governed by the contralateral cortex. However, the ipsilateral cortex also shows changes in activity [2]. Bilateral interactions of neurons are therefore possible at the cortical level as well. It is still unclear to what extent changes in activity of the ipsilateral cortex are associated with the planning and execution of a movement or are a sensory reflection of the movement. We studied the grip force of the thumb and index finger for both left and right hands while one hand hold an object and experienced a unilateral external influence. Anticipation to an external influence is known to increase the grip force to prevent the object from sliding from the hand [3]. When an object is held with two hands, muscular activity increases in both of them [4]. The response to a unilateral external influence during a bimanual movement is known to differ depending on how well the hand movements are coordinated [5, 6]. In particular, when both of the hands control the position of one object, a unilateral influence on one hand quickly induces a response in the other, unaffected hand. When the hands control the objects that are not related to each other, a rapid adjustment is observed only in the affected hand. The quick response of the unaffected hand may result from both facilitation of afferent cross feedbacks at a local level and the interaction of motor centers at a higher level.
We have studied how the grip force changes in left- and right-hand fingers when two different objects are held by different hands and a unilateral influence is applied to the object held with the right hand. To exert the external effect, a weight was dropped in a cap held with the right hand [7]. When a subject observes the weight falling, the right-hand fingers that hold the cap increase the grip force both before the impact and during the response to the impact [3, 7]. In this work, the effect of an anticipated unilateral influence was studied in conditions where the left- and right-hand efforts were coordinated to different extents. Changes in left-hand grip force were studied in conditions where changes in left- and right-hand grip forces were not associated with each other and where left- and right-hand fingers acted synchronously to slowly increase the grip force. We assumed that a common motor task performed with both of the hands may induce changes in left-hand grip force not only during the response to a weight impact, but also during its anticipation. We discuss the mechanisms that may sustain the cross effects while the hands interact during a unilateral external influence.
METHODS
Ten healthy subjects were involved in the study. A subject sat in an armchair during tests. The subject’s right forearm rested horizontally on a comfortable support, the arm was vertical, and the angle at the elbow joint was approximately 90°. The thumb and index finger of the subject’s right hand hold a rigid metal bracket, which was connected through a flexible cable to a 60-cm beam. The beam could freely rotate about the axis located in the center (see the scheme of experiments in [7]). Strain gauge sensors were built in the bracket to measure the grip force of right-hand fingers and the vertical force acting on the bracket. The distance between the fingers was 40 mm. The beam was balanced with a counterweight so that a minimal effort (approximately 1 N) was enough to hold it horizontally. A cap with the bottom covered with plasticine was placed on the beam. A cylindrical weight (1.8 cm in diameter, 5 cm in height) was held with an electromagnet 70 cm above the cap and fell into the cap when the electromagnet circuit was broken.
The subject’s left hand rested on a comfortable support and held a force sensor with its fingers to measure their grip force. Three different test variants were used for the left hand. First, the subject’s left-hand fingers touched the force sensor placed on a desk with a negligible force. Second, the subject’s left fingers held the sensor loaded with a 2-N load. In either variant, the subject’s right hand held a sensor connected with the cap where the weight fell. In the third variant, the subject was instructed to synchronously increase the grip forces of both of the hands from approximately 0.5 to 6–8 N over 5–8 s. The subjects monitored the changes in grip force on a monitor screen several times during training tasks. After training, the subjects were able to increase the grip force as necessary with the eyes closed or open without monitoring the changes. The weight was dropped into the cap held with the right hand at various time points while the subject slowly increased the grip forces of the two hands; the weight fall was accompanied by an involuntary increase in right-hand grip force. All test variants were performed with the subject’s eyes open or closed.
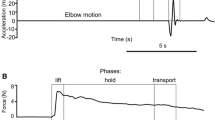
The mean grip force was measured over four different time intervals before and after the fall of the weight, and the measurements were used as parameters to characterize the motor task performance. The time point where the falling weight hit the cap was used as a reference point. The time intervals to obtain the mean grip force before and after the weight fall are shown in Fig. 1a. The first interval was used to measure the baseline grip force before a weight fall; the grip force was averaged over the interval from –500 to –400 ms of the impact (Baseline1). The second interval was chosen to precede the period of time when the subject might start increasing the grip force in anticipation of a weight impact, observing the falling weight. The grip force before an anticipatory increase was averaged over the interval from –300 to –200 ms (Baseline2). The average grip force immediately preceding an impact of the falling weight in tests with visual control corresponded to an anticipatory increase in grip force. The anticipatory increase was measured over the interval from –20 to –5 ms (Anticipation). The impact response (Impact) was measured as a maximal force observed in the interval 100–300 ms after a impact. In tests performed with eyes closed, a comparison of the Baseline1, Baseline2, and Anticipation values characterized the stability of maintaining the grip force in variants 1 and 2. In variant 3, the values made it possible to estimate the rate at which the grip forces were increased synchronously. In tests with eyes open, Anticipation characterized the preparation to an impact of the falling weight. The anticipatory increase in force and the response to a weight impact overlapped the voluntary increase in grip force. A comparison of the grip force between the third and fourth intervals in the presence or absence of visual control made it possible to estimate the effect of a voluntary increase in force on the parameters. An additional analysis was therefore performed for the difference in grip force between tasks with and without visual control over the motor task.

Changes in the grip forces of the (1) right and (2) left hands during an external influence (an impact by a falling weight) on a cap held with the right hand (3). The subject had to hold the cap with the right hand when the weight fell and hit it. The left-hand grip force was different in different tasks: (a) the left hand touched a force sensor, (b) the left hand held a 200-g object, or (c) the left and right hands slowly and synchronously increased the grip force. The results were averaged over several tests performed by one subject. The task was performed with the eyes (a) open (the subject observed the weight falling) or (b) closed (the subject did not observe the weight falling). The intervals where the grip forces Baseline1, Baseline2, Anticipation, and Impact were measured are shown in Fig. 1a at the bottom of the upper plot. Force bar, 4 N for right-hand grip force and loading and 2N for left-hand grip force. Time bar, 500 ms.
To analyze the changes in grip force for each hand and each visual control condition, two-way ANOVA was carried out with two factors, grip force at different time points of a motor task performed with or without visual control (Baseline1, Baseline2, Anticipation, and Impact) and motor task variant (variants 1, 2, and 3).
RESULTS
Figure 1 shows the changes in grip force that were observed for the left and right hands of a typical subject while the subject held the beam with the cap and the weight fell. The pattern detected for the right hand depended on whether the subject received visual feedback and was similar in all test variants in each of the visual control conditions. When a subject observed the weight falling, the right-hand grip force started increasing 100–200 ms before the impact. When a subject’s eyes were closed, the grip force increased 60–80 ms after the impact. As for the left hand, changes in grip force depended on the task conditions. Changes in grip force in response to a weight fall were not observed in variant 1, when the left-hand fingers only touched the force sensor, regardless of whether the subject’s eyes were open or closed (Fig. 1a). Nonsignificant changes in grip force were detected in variant 2, when the left hand held a load (Fig. 1b). When the grip force was synchronously linearly modulated in both of the hands with eyes closed, a reflex increase in grip force after the impact was observed for the left hand, like for the right one. When the subject’s eyes were open, an increase in left-hand grip force occurred before the impact, like in the case of the right hand. Thus, both reflex and anticipatory changes in grip force were observed for the left hand as well when a common motor task was performed by the two hands, while such changes were usually restricted to the right hand.
Group-averaged grip forces observed for the right and left hands in different test variants are shown in Fig. 2. The changes in grip force were analyzed for each hand and each visual control condition by two-way ANOVA. The first factor was grip force at different time points of the motor task (Baseline1, Baseline2, Anticipation, and Impact); the second factor was motor task variant (variants 1, 2, and 3).

Group-averaged changes in (a–c) right- and (d–f) left-hand grip forces at different time points of the task where a weight fell into a cap held with the right hand. Ordinate, grip force (N). The grip force was measured before the weight fell (и1 for Baseline1), before the grip force started to increase in preparation to a impact (и2 for Baseline2), at the moment of impact (и3 for Anticipation), and during a response to the impact (и4 for Impact) (see Methods). The task was performed with the eyes (a) open (the subject observed the weight falling) or (b) closed (the subject did not observe the weight falling). (*) A significant difference was detected between the tasks performed with or without visual control.
In the case of the right hand and eyes closed, ANOVA revealed significant difference between different test variances and different time points of the motor task. A significant interaction was shown for the two factors (F(6, 48) = 7.71, p < 0.00001). Thus, the grip force changed differently in different conditions. A post-hoc analysis showed that the Baseline1, Baseline2, Anticipation, and Impact values did not differ between variants 1 and 2 (Figs. 2a, 2b) and were lower than Impact. The average grip force in variant 3 was higher than in variants 1 and 2 (Fig. 2c). This could be explained by the fact that the subjects slowly increased the grip force as instructed in variant 3. Baseline1 was lower than Baseline2 and Baseline2 was lower than Anticipation in these test conditions (p < 0.05, Tukey’s test). The grip force after an impact was higher than Baseline1, Baseline2, and Anticipation in variant 3. In addition, Impact in variant 3 was higher than in variants 1 and 2 (p < 0.05, Tukey’s test).
When the subject’s eyes were open, an increase in right-hand grip force was observed not only after the impact, but before the impact as well. ANOVA showed that changes in right-hand grip force differed in different conditions (F(6, 54) = 4.11, p < 0.002). Like in the tests with eyes closed, the average grip force in variant 3 was higher than in variants 1 and 2 (F(2, 18) = 10.53, p < 0.001). The grip forces detected before (Anticipation) and after (Impact) the impact were higher than Baseline1 and Baseline2 in all test conditions (Figs. 2a–2c). The right-hand grip force before (Anticipation) and after (Impact) the weight fall in variant 3 was higher than in variants 1 and 2 because the subjects increased the grip force in variant 3 as instructed. Because the average grip force in variant 3 was higher than in the other variants, ANOVA was carried out for the difference in grip force between the motor tasks performed with or without visual control. The difference in grip force in different time intervals was used as the first factor, and test conditions were the second factor. Differences between the time points did not significantly differ between the test variants (F(6, 48) = 0.99, p > 0.44). In all test variants, the difference in grip force was significantly higher only before the fall, while nonsignificant differences were observed at the other time intervals during the motor task (Figs. 2a–2c, p < 0.05, Tukey’s test). This, the right-hand grip force similarly increased during preparation for the impact in different test conditions (Table 1). The instruction to slowly increase the grip force did not change the anticipatory increase in grip force.
The left-hand grip force did not change during the test in variants 1 and 2 regardless of whether the subject’s eyes were open or closed. In variant 3, changes in grip force depended on whether the subject observed the weight falling. When the eyes were closed while performing the motor task, the left-hand grip force changed differently in different test conditions by ANOVA (F(6, 54) = 22.11, p < 0.0001). The grip force in variant 1 was lower than in variants 2 and 3 according to the instructions given to the subject (Fig. 2d). Changes in grip force during the test were nonsignificant in variants 1 and 2 (p > 0.05, Tukey’s test; Figs. 2d, 2e) both before and after the weight fall. In variant 3, the grip force gradually increased before the impact (p < 0.05, Tukey’s test). Baseline1 was lower than Baseline2; Baseline2 was lower than Anticipation (Fig. 2f, p < 0.05, Tukey’s test) the grip force after the fall was higher than Baseline1, Baseline2, and Anticipation (p < 0.05, Tukey’s test).
When the subject’s eyes were open, the left-hand grip force again changed differently in different test conditions (F(6, 48) = 13.69, p < 0.0001). The grip force in variant 1 was lower than in variants 2 and 3. Variants 2 and 3 did not significantly differ in mean grip force (p > 0.05, Tukey’s test). Nonsignificant changes in grip force were observed in different time intervals in variants 1 and 2. The Anticipation value increased in variant 2 by 0.21 ± 0.07 N as compared with Baseline2; the change was nonsignificant (p > 0.05, Tukey’s test; Fig. 2e). The grip force increased during motor test performance in variant 3. Baseline1 was higher than Baseline2, and Anticipation increased significantly relative to Baseline2 (p < 0.05, Tukey’s test). A response to the weight fall was higher than Anticipation, Baseline1, and Baseline2 in variant 3.
Because the mean grip force in variant 1 was lower than in the other test variants, ANOVA was carried out for the difference in left-hand grip force in different time intervals of the motor task performed with or without visual control (grip force in a particular interval was the first factor; test conditions were the second factor). ANOVA showed that the difference in left-hand grip force differed between the variants (F(6, 48) = 4.81, p < 0.001). In variants 1 and 2, the difference in grip force did not significantly differ between different time points during the task performed with or without visual control (Table 1). In variant 3, the difference observed before the impact and in response to the impact was higher than Baseline1 and Baseline2 (p > 0.05, Tukey’s test). Thus, an external influence on the right hand did not affect the grip force of the left hand when independent movements were performed by the two hands. When a common motor task was performed by the two hands, the reflex and anticipatory changes in grip force were observed in the left hand as well, while the latter was usually restricted to the right hand.
DISCUSSION
In the task of holding a cap where a weight fell, the involuntary increase in the grip force of right-hand fingers depended on whether visual information about the weight falling was available, but was independent of the motor task variant. When the subject’ eyes were closed, the grip force increased in response to the weight impact in all test variants. When the subject’s eyes were open, an involuntary increase in right-hand grip force was observed 200–300 ms before the weight hit the cap. The involuntary increase in right-hand grip force was not affected when the subjects were additionally instructed to slowly and synchronously increase the grip force of both right and left hands, regardless of whether the subject’s eyes were open or closed. The left-hand grip force changed differently in different conditions. When the grip forces produced by the two hands were independent of each other, changes induced by a weight fall in the right-hand grip force did not affect the left-hand grip force. When the grip forces of the two hands were increased in a coordinated manner, the unaffected left hand increased the grip force both before the weight impact and in response to the impact.
When the two hands are involved in holding an object, a response to an external factor is known to occur not only in the affected hand, but also in the unaffected contralateral hand [8, 9]. The latency that precedes an increase in grip force in response to an external disturbing factor indicates that the response may be associated not only with activation of local neuronal mechanisms, but also with activation of spinal–brainstem and spinal–cortical connections. The response of the hand that was not affected by an external factor may accordingly arise because afferent feedbacks excite cross influences at various nervous system levels, including the level of intercortical interactions [5]. An increase in the grip force of the unaffected hand was additionally observed during preparation to a weight impact in our study, that is, in the period when afferent signals of exposure to a disturbing factor were still absent. The finding therefore indicates that the facilitation of cross influences is associated with interactions at the level of motor centers responsible for the movement. A similar conclusion has been made in a study where the two hands manipulate a common object [5]. Activity of the primary motor cortex is known to determine the anticipatory changes [10, 11]. Preparation to an anticipated external influence is known to develop with age, as motor skills are acquired by children [12]. Our findings make it possible to assume that cross interactions of the left and right hands occur at the level of transcallosal influences from the left and right motor cortical areas during movement planning [13].
CONCLUSIONS
When the right and left hands hold different objects with the thumb and index finger and a unilateral external influence is applied to the right hand, the changes in grip forces depend on the extent to which the motor tasks of the two hands are associated. An external influence on the object held by the right hand did not change the left-hand grip force when uncoordinated motor tasks were performed by the two hands. The right-hand grip force changed depending on whether the external influence was anticipated or not. A weight falling in a cap held with the right hand was used as an external influence in our study. The fall was unexpected when the subject’s eyes were closed. When the subject observed the weight falling, preparation to the weight impact was detectable. The right-hand grip force started to increase 200 ms before the weight hit the cap when the fall was anticipated and only 60–80 ms after the impact when the fall was unexpected. The left-hand grip force did not change in the tasks where the left hand touched a force sensor or held a 200-g object.
When the left and right hand slowly and synchronously increased the finger grip force, an external influence on the right hand changed the grip force not only in the right, but also in the left hand. In the case of an unexpected external influence, an increase in right- and left-hand grip forces occurred in response to the weight impact. In the case where the weight falling was observed by the subject, an increase in right- and left-hand grip forces was detected not only in response to the impact, but also before the impact. Thus, cross effects occurred not only in response to an external influence, but also during preparation to the influence. It is possible to assume that, while a movement is planned, cross influences are organized at the supraspinal level and, probably, at the level of interactions between the motor cortical areas of the left and right hemispheres.
REFERENCES
Sherrington, C.S., Flexion-reflex of the limb, crossed extension-reflex, and reflex stepping and standing, J. Physiol., 1910, vol. 40, nos. 1–2, p. 28.
Diedrichsen, J., Wiestler, T., and Krakauer, J.W., Two distinct ipsilateral cortical representations for individuated finger movements, Cereb. Cortex, 2013, no. 6, vol. 23, p. 1362.
Johansson, R.S. and Westling, G., Programmed and triggered actions to rapid load changes during precision grip, Exp. Brain Res., 1988, vol. 71, no. 1, p. 72.
White, O., Dowling, N., Bracewell, R.M., et al., Hand interactions in rapid grip force adjustments are independent of object dynamics, J. Neurophysiol., 2008, vol. 100, no. 5, p. 2738.
Mutha, P.K. and Sainburg, R.L., Shared bimanual tasks elicit bimanual reflexes during movement, J. Neurophysiol., 2009, vol. 102, no. 6, p. 3142.
Omrani, M., Diedrichsen, J., and Scott, S.H., Rapid feedback corrections during a bimanual postural task, J. Neurophysiol., 2013, vol. 109, no. 1, p. 147.
Kazennikov, O.V. and Lipshits, M.I., Influence of preliminary information about the mass on anticipatory muscle activity during the catching of a falling object, Hum. Physiol., 2010, vol. 36, no. 2, p. 198.
Marsden, C.D., Merton, P.A., and Morton, H.B., Human postural responses, Brain, 1981, vol. 104, no. 3, p. 513.
Ohki, Y. and Johansson, R.S., Sensorimotor interactions between pairs of fingers in bimanual and unimanual manipulative tasks, Exp. Brain Res., 1999, vol. 127, no. 1, p. 43.
Kazennikov, O.V. and Lipshits, M.I., Participation of primary motor cortex in the programming of muscle activity during catching of a falling object, Hum. Physiol., 2011, vol. 37, no. 5, p. 108.
Pruszynski, J.A., Omrani, M., and Scott, S.H., Goal-dependent modulation of fast feedback responses in primary motor cortex, J. Neurosci., 2014, vol. 34, no. 13, p. 4608.
Eliasson, A.C., Forssberg, H., Ikuta, K., et al., Development of human precision grip, vol. anticipatory and triggered grip actions during sudden loading, Exp. Brain Res., 1995, vol. 106, no. 3, p. 425.
Berlot, E., Prichard, G., O’Reilly, J., et al., Ipsilateral finger representations in the sensorimotor cortex are driven by active movement processes, not passive sensory input, J. Neurophysiol., 2019, vol. 121, no. 2, p. 467.
Funding
This work was supported by the Russian Foundation for Basic Research (project no. 18-015-00266).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interests. The authors declare that they have no actual or potential conflict of interest in relation to this article.
Statement of compliance with standards of research involving humans as subjects. All procedures were in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments and were approved by the local Ethics Committee at the Kharkevich Institute of Information Transmission Problems (Moscow). Written informed consent was voluntarily given by all individual study participants after being informed about the potential risks and benefits and the nature of the study.
Additional information
Translated by T. Tkacheva
Rights and permissions
About this article

Cite this article
Kazennikov, O.V., Kireeva, T.B. & Shlykov, V.Y. Left–Right Interaction during Anticipatory Motor Adjustment. Hum Physiol 45, 628–633 (2019). https://doi.org/10.1134/S0362119719060069
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1134/S0362119719060069