
Abstract
Given advantages in reperfusion therapy leading to mild stroke, less apparent cognitive deficits can be overseen in a routine neurological examination. Despite the widespread use of the Montreal Cognitive Assessment (MoCA), age- and education-specific cutoffs for the detection of post-stroke cognitive impairment (PSCI) are not established, hampering its valid application in stroke. We aimed to establish age- and education-specific MoCA cutoffs to better discriminate patients with and without acute PSCI. Patients with acute ischemic stroke underwent the MoCA and a detailed neuropsychological assessment. PSCI was defined as a performance < − 1.5 SD in ≥ 2 cognitive domains. As secondary data analysis, the discriminant abilities of the MoCAraw-score (not adding + 1 as correction for ≤ 12 years of education, YoE) cutoffs were automatically derived based on Youden Index and evaluated by receiver operating characteristic analyses across age- (< 55, 55–70, > 70 years old) and education-specific (≤ 12 and > 12 YoE) groups. 351 stroke patients (67.4 ± 14.1 years old; 13.1 ± 2.8 YoE) underwent the neuropsychological assessment 2.7 ± 2.0 days post-stroke. The original MoCA cutoff < 26 falsely classified 26.2% of examined patients, with poor sensitivity in younger adults (34.8% in patients < 55 years > 12 YoE) and poor specificity in older adults (55.0%, in > 70 years ≤ 12 YoE). By maximizing both sensitivity and specificity, the optimal MoCAraw cutoffs were: (i) < 28 in patients aged < 55 with > 12 YoE (sensitivity = 69.6%, specificity = 77.8%); (ii) < 22 and < 25 in patients > 70 years with ≤ 12 and > 12 YoE (sensitivity = 61.6%, specificity = 90.0%; sensitivity = 63.3%, specificity = 84.0%, respectively). In other groups the optimal MoCAraw cutoff was < 26. Age and education level should be considered when interpreting MoCA-scores. Though new age- and education-specific cutoffs demonstrated higher discriminant ability for PSCI, their performance in young stroke and adults with higher education level was low due to ceiling effects and MoCA subtests structure, and cautious interpretation in these patients is warranted.
Trial registration: ClinicalTrials.gov Identifier: NCT05653141.
Similar content being viewed by others


Introduction
Post-stroke cognitive impairment (PSCI), defined as a stroke-induced deficit in any cognitive domain1, is frequent and may affect even young adults and patients without any residual neurological deficits2. Previous reviews and meta-analyses reported a prevalence of PSCI between 7 and 75%3,4,5, depending on the study design, stroke type (ischemic or hemorrhagic stroke), assessment period (acute or chronic), pre-stroke cognitive status (unimpaired, pre-stroke mild cognitive impairment, or dementia), recurrent or first-ever stroke, diagnostic criteria (number of affected domains), and applied cognitive assessment tool (neuropsychological test battery or brief cognitive test).
Overall, PSCI was shown to impact negatively on functional stroke outcome and activities of daily living6. Despite the high prevalence of PSCI and its negative functional impact6, a gold-standard cognitive screening tool for PSCI is missing1. Stroke might affect different cognitive domains7,8; thus the cognitive assessment should evaluate at least attention, processing speed, executive functions, episodic memory, language, and visuo-constructive abilities1. Recent guidelines recommend an early cognitive assessment already in the acute stroke phase to tailor important therapeutic decisions and patient triage. To date, the most widely used cognitive tests to investigate PSCI are screening tools (i.e., Montreal Cognitive Assessment [MoCA]9 and Mini-Mental State Examination), which are feasible even in the acute stroke phase10. However, being primarily developed for neurodegenerative diseases, these two tools were shown to be less sensitive in the detection of PSCI11,12,13 and consequently PSCI remains frequently underdiagnosed and underestimated14. In contrast, Pendlebury et al. reported the MoCA as an appropriate brief cognitive tool for the detection of PSCI, though with low sensitivity to single non-memory domains15. Therefore, the authors recommended a revision of its cutoffs depending on the aim (screening or diagnosis)15.
Some studies on both healthy and patient populations have stressed the impact of education and age16,17,18,19,20 on the MoCA-score, which have been inconsistently reported as risk factors for PSCI5. Due to their impact on cognitive performance, recent guidelines recommend the use of education- and age-adjusted norms in the detection of PSCI1. In their original study, Nasreddine et al. suggested the cutoff of < 26 as indicative of affected cognition and correction for education by adding 1 point to the MoCAraw-score in individuals with ≤ 12 years of education9. A more recent study on healthy elderly demonstrated an effect of age on the MoCA-score with a linear performance decrease in healthy aging21. Moreover, the original MoCA cutoff < 26 was not validated, and both age- and education-specific cutoffs in the stroke population have not yet been investigated despite the high heterogeneity in age and years of education in this population. In line with the point, several studies adapted the MoCA cutoff for the detection of mild cognitive impairment in neurodegenerative diseases22,23,24. For stroke, two studies identified MoCA cutoff in the acute stroke phase predictive for long-term cognitive impairment, but not for the detection of PSCI in the acute stroke phase itself25,26. These studies also did not consider the impact of age and level of education on cognitive performance. However, valid cutoffs for the detection of PSCI in the acute stroke phase are needed1,14, as the differentiation between patients with and without PSCI is crucial at this time point when the main therapeutic and triage decisions are made, and the main gain of cognitive function and therapeutic response occurs27,28. The issue became more relevant with the availability of reperfusion therapy leading to mild stroke and therefore less apparent cognitive deficits that might be easily overseen in the routine neurological examination.
Given the great advantages of the MoCA in the acute stroke setting in terms of administration time and feasibility, and the knowledge on the impact of normal ageing on MoCA performance, we aimed to determine age- and education-specific MoCA cutoffs and assess their discriminant ability for the detection of PSCI in the acute stroke phase based on a standardized and normalized neuropsychological test battery.
Methods
Standard protocol approvals, registrations, and patient consents
Written informed consent was obtained from all participants before data collection. The study was approved by the local Ethics Committee (Kantonale Ethikkommission Bern KEK 2020-02273) and followed ethical criteria for human research.
Study population and participant recruitment
This study presents a secondary analysis of our prospective longitudinal cohort study investigating post-stroke cognitive impairment (ClinicalTrials.gov Identifier: NCT05653141). We analysed the data of stroke patients recruited in our prospective longitudinal study admitted to the Stroke Center of the University Hospital of Bern between December 16, 2020, and October 10, 2023. Adult patients (age ≥ 18 years) with a first-ever ischemic stroke in the anterior circulation territory confirmed by MRI examination with symptom onset ≤ 10 days were eligible. Exclusion criteria were: (1) involvement of additional stroke territories; (2) history of stroke in records or MRI-evidence of previous stroke; (3) neurological or psychiatric comorbidities biasing or precluding the cognitive assessment (e.g. brain tumor, current depression, dementia, reduced vigilance, delirium); (4) evidence of pre-stroke cognitive decline according to a structural interview with the informant based on the 7-item Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE)29 completed with the patient’s relative or other informant prior inclusion (score of > 3.29 indicates prior cognitive decline)30; (5) contraindication for MRI examination; (6) other native language than German, French or Italian; (7) symptom onset > 10 days; (8) participation in interventional studies influencing outcome; and (9) presence of aphasia based on the clinical assessment and Token Test (stanine < 8)7,31. Detailed information regarding the inclusion and exclusion criteria is provided as a flowchart of patients’ recruitment in Supplementary material (Figure S1). We focused on non-aphasic patients because (i) cognitive deficits in this patient group are less apparent and more difficult to capture, in contrast to aphasic symptoms that are usually apparent in the routine neurological examination and are included in NIH Stroke Scale (NIHSS), and (ii) aphasia might bias the cognitive performance in other cognitive domains hampering the interpretation of neuropsychological performance.
All patients underwent standard treatment according to the European Stroke Organization (ESO) guidelines and the local Stroke Guidelines.
Patients assessment
Demographic and clinical data were acquired during hospitalization through direct interviews with patients and from medical records. Trained neurologists assessed stroke severity using the NIHSS at admission and 24 h post-stroke. Years of education were computed based on guidelines by The Consortium to Establish a Registry for Alzheimer’s Disease32.
Neuropsychological assessment
A trained psychologist administered in one session in a predetermined order the MoCA followed by a standardized multi-domain neuropsychological assessment in the subject’s primary language. Only patients with a stable neurological condition and sufficient vigilance were included and tested. Considering the duration and demand of the test battery, efforts were made to ensure the optimal testing conditions to reduce fatigue and the test burden. The test battery was structured to be performed at the bedside in one session and in a predefined order to ensure inter-individual comparability. Detailed information on the neuropsychological assessment and applied standardization has been reported previously7 and in Supplementary material (Table S1). The neuropsychological test battery was designed (i) to assess main cognitive domains in accordance with the guideline recommendations1,33; (ii) to take ~ 60 min to be feasible in the acute stroke phase34; and (iii) to have independent validated norms7. In summary, the neuropsychological test battery assessed performance in verbal learning32, verbal and figural episodic memory32, constructive abilities32, short-term and working memory35, processing speed32, executive functions32, selective attention36, and spatial neglect36. Individual performance was represented by z-scores adjusted for age35, sex, and education32. PSCI was defined as at least moderate (z-score < − 1.48 or percentile rank < 7) deficit in ≥ 2 tested cognitive domains7,37,38.
Originally, according to Nasreddine et al.9 patients with ≤ 12 years of education receive + 1 on the total raw score (i.e., MoCA(+1) score). As this correction for level of education has not yet been validated, we did not add 1 point in patients with ≤ 12 years of education and operated with the MoCA raw score (i.e., MoCAraw) without any adjustments.
Statistical analysis
Continuous variables with normal distribution were summarized by mean and standard deviation (mean ± SD), and compared using parametric tests; non-normally distributed variables were summarized as median and interquartile range (IQR) and compared using non-parametric statistics. Categorical variables were summarized by numbers and percentages and compared with χ2 test.
To ensure the applicability of the cutoffs in the routine clinical practice, and to incorporate the age- and education-adjustments, the total sample was stratified by (i) age: < 55 years old (i.e., young stroke adults)39, 55–70, and > 70 years old40; and (ii) education level: low (≤ 12 years of education) versus high (> 12 years of education), resulting in 6 groups. The applied cutoff for years of education ≤ 12 is the internationally most often used one for the definition of lower versus higher education level. The optimal MoCAraw cutoffs were automatically selected based on the Youden Index41 using the cutpointr package in R42. For a given cutoff, the Youden Index is calculated as ‘sensitivity + specificity-1’41 and characterizes the cutoff’s performance with a value ranging between 0 and 1 indicating the worst and the perfect performance respectively. Since we aimed to determine MoCA cutoffs to better discriminate patients with and without PSCI, we opted for the Youden Index which relies on maximizing both sensitivity and specificity41. The definition of cutoffs with maximal sensitivity and specificity according to the Youden Index increases the rate of correctly identified patients both with PSCI (sensitivity) and without PSCI (specificity). The discriminative abilities of the defined MoCAraw cutoffs in the detection of PSCI were examined using receiver operator characteristic curves for each group and compared with those of MoCA(+1) < 26. For each cutoff, the sensitivity, specificity, false negative, false positive, true positive, true negative rates, areas under the curves (AUCs), positive (LR+) and negative (LR−) likelihood ratios with 95% CI were calculated. The latter two measures are discussed as the most appropriate ones for the assessment of cutoffs’ diagnostic performance43. LR+ is the ratio of the proportion of patients who have the target condition and a positive test to the proportion of patients without the target condition who also test positive. LR− is the ratio of the proportion of patients who have the target condition who test negative to the proportion of patients without the target condition who also test negative44. Higher LR+ and a lower LR− indicate the better performance of a test45.
All analyses were performed using R statistical software version 4.1.2 (R Studio Version 4.1.2); two-tailed statistics are reported.
Results
Patients characteristics
We prospectively included 351 patients with acute first-ever ischemic stroke, from whom 206 (58.7%) patients underwent recanalization therapy. Consequently, most patients suffered only mild stroke (NIHSS 24 h = 2 [0–3.5]; range 0–23, NIHSS ≤ 5 in 86.6% of patients). Stroke severity was comparable across age groups (Kruskal–Wallis test χ2 = 0.609, p = 0.737). Table 1 reports patients’ demographic and clinical characteristics.
All patients underwent the neuropsychological assessment and the MoCA test 2.7 ± 2.0 days post-stroke. The median MoCAraw-score was 24 (21–27), 57.5% of patients (n = 202) performed below the original cutoff of < 26 which was suggested to be indicative of pathological performance9. MoCA-scores differed across demographic groups, with higher scores in patients with higher than lower education (median MoCAraw 26 [23–27] versus 22 [18–25] respectively, Mann–Whitney W = 22,373, p < 0.001) and with younger age (median MoCAraw 27 [24–28] in patients < 55 years, 25 [22–27] in patients 55–70 years, and 23 [20–26] in > 70 years, Kruskal–Wallis test χ2 = 31.422, p < 0.001; Table 2). According to the detailed neuropsychological assessment, 70.7% of patients (n = 248) had PSCI (at least moderately affected performance [z-score < − 1.48] in ≥ 2 cognitive domains). The prevalence of PSCI was comparable across age groups (66.2%, 69.7%, and 73.1% in ascending order for age groups, χ2 = 1.146, p = 0.564), however, patients with higher education had less prevalent PSCI (61.5% vs. 81.1%, χ2 = 15.258, p < 0.001; Table 2). The prevalence of PSCI according to the neuropsychological testing and MoCA(+1) cutoff < 26 differed significantly across patient groups with the largest mismatch in younger adults (66.2% vs. 32.3% correspondingly, χ2 = 13.572, p < 0.001) and adults with higher education level (61.5% vs. 46.0% correspondingly, χ2 = 8.432, p = 0.004). In the total sample, 27.8% (n = 69) of patients with PSCI had a MoCA(+1)-score ≥ 26 i.e., were false negative cases, and 22.3% (n = 23) of patients without PSCI had a MoCA(+1)-score < 26 i.e., were false positive cases. Thus, altogether 26.2% of patients from the whole sample have been falsely classified based on the MoCA(+1) cutoff < 26.
Age- and education-specific MoCA cutoffs and their comparisons with the original cutoff
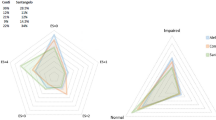
Based on the Youden Index, we calculated the age- and education-specific MoCAraw cutoffs and compared their discriminative abilities to the original MoCA(+1) cutoff of < 26 (Table 2). Figure 1 and Figures S2–S4 display the sensitivity, specificity, and AUC of the original cutoff of MoCA(+1) < 26 and the newly defined MoCAraw cutoffs, across different patient groups.

Diagnostic accuracy of MoCA cutoffs across patients groups stratified by age and level of education. The new defined cutoffs provided higher sensitivity for younger stroke adults and higher specificity for older ones. (A) Sensitivity of the new defined MoCAraw cutoffs (black) and of the original MoCA(+1) cutoff < 26 (blue). (B) Specificity of the new defined MoCAraw cutoffs (black) and of the original MoCA(+1) cutoff < 26 (blue).
In patients < 55 years old with ≤ 12 years of education, the optimal MoCAraw cutoff according to the Youden Index was < 26 (sensitivity = 75.0%; specificity = 75.0%; AUC = 0.763; LR+ = 3.00, 95% CI [0.54–16.69]; LR− = 0.33, 95% CI [0.13–0.86]) showing better performance compared to the original MoCA(+1) cutoff of < 26 (sensitivity = 60.0%, specificity = 75.0%, AUC = 0.675, LR+ = 2.40 [0.42–13.60], LR− = 0.53 [0.24–1.16]). Please note, that the new MoCAraw cutoff < 26 differs from the original MoCA(+1) cutoff of < 26 as we did not add + 1 to the raw score for patients with lower education. In patients < 55 years old with > 12 years of education, the optimal MoCAraw cutoff according to the Youden Index was < 28 (sensitivity = 69.6%, specificity = 77.8%, AUC = 0.818, LR+ = 3.14 [1.27–7.74], LR− = 0.39 [0.20–0.76]) showing better performance compared to the original MoCA(+1) cutoff (sensitivity = 34.8%, specificity = 100%, AUC = 0.674, LR+ = infinite, LR− = 0.65 [0.48–0.88], Figure S2).
In patients 55–70 years old with ≤ 12 years of education, the optimal MoCAraw cutoff according to the Youden Index was < 26 (sensitivity = 82.5%, specificity = 100.0%, AUC = 0.898, LR+ = infinite, LR− = 0.18 [0.09–0.34]) showing better performance compared to the original MoCA(+1) cutoff (sensitivity = 77.5%, specificity = 100%, AUC = 0.887, LR+ = infinite, LR− = 0.23 [0.13–0.40]). Again, please note, the MoCAraw differed from the MoCA(+1) as we did not add + 1 for patients with lower education. In patients 55–70 years old with > 12 years of education, the optimal MoCAraw cutoff according to the Youden Index was < 26 (sensitivity = 65.1%, specificity = 82.8%, AUC = 0.811, LR+ = 3.78 [1.65–8.63], LR− = 0.42 [0.27–0.65], Figure S3). Thus, for this group, the original cutoff was confirmed.
In patients > 70 years old with ≤ 12 years of education, the optimal MoCAraw cutoff according to the Youden Index was < 22 (sensitivity = 61.6%, specificity = 90.0%, AUC = 0.827, LR+ = 6.16 [1.63–23.24], LR− = 0.43 [0.31–0.59]) showing much better specificity, but worse sensitivity compared to the original MoCA(+1) cutoff (sensitivity = 86.3%, specificity = 55.0%, AUC = 0.707, LR+ = 1.92 [1.17–3.14], LR− = 0.25 [0.12–0.50]). In patients > 70 years old with > 12 years of education, the optimal MoCAraw cutoff value according to the Youden Index was < 25 (sensitivity = 63.3%, specificity = 84.0%, AUC = 0.781, LR+ = 3.96 [1.57–9.95], LR− = 0.44 [0.29–0.66]) showing overall better performance compared to the original MoCA(+1) cutoff (sensitivity = 75.5%, specificity = 68.0%, AUC = 0.718, LR+ = 2.36 [1.30–4.27], LR− = 0.36 [0.21–0.63], Figure S4).
In conclusion, the original MoCA(+1) cutoff < 26 had lower sensitivity compared to new cutoffs in young stroke adults due to a high number of false negative cases (53.5% versus 27.9% with the new cutoff) and lower specificity in older adults > 70 years old due to a high number of false positive cases (37.8% vs. 13.3% with the new cutoff; Table 2).
The new cutoffs were automatically derived to maximize both sensitivity and specificity, as indicated by the Youden Index. Nonetheless, it is acknowledged that the emphasis on either sensitivity or specificity may vary depending on the aim. Table S2 provides a comprehensive overview of the sensitivity, specificity, accuracy, and AUC of MoCAraw cutoffs ranging from 22 to 28 for each group.
Discussion
The MoCA is a quick and feasible brief cognitive tool, but its cutoff for the detection of PSCI in the acute stroke phase has been barely investigated. To increase the utility of the MoCA in detection of PSCI, we investigated the performance of the original cutoff across age- and education-specific patient groups and defined new cutoffs with higher discriminant ability. The original MoCA(+1) cutoff showed low sensitivity in younger stroke adults (< 55 years old) and low specificity in older adults (> 70 years old). The newly defined cutoffs demonstrated better performance by considering age and level of education.
In previous studies, the most often reported cutoffs for the detection of PSCI in the acute stroke phase were 22/2311,25,46,47, which were confirmed by recent meta-analyses as the cutoffs showing better diagnostic accuracy in stroke patients48,49. Similarly, Salvadori and colleagues reported < 22 as the best cutoff to longitudinally predict PSCI at 6 to 9 months26. For the subacute phase and after 3 months post-stroke, the most frequently reported cutoff was < 2650,51. In the present study, 70.7% of included patients suffered from PSCI based on the neuropsychological assessment, whereas 57.5% had a MoCA-score < 26 and only 25.9% had a MoCA-score < 22, stressing that neither the original9 nor the recently suggested stroke-specific cutoffs11,25,26,46,47 represents a reliable cutoff in the detection of PSCI. This can be explained by the fact that previous studies identified and tested the cutoffs without considering age and levels of education. These two demographic factors have been shown to influence cognitive performance16,17,18,19,20 and should be considered in the interpretation of cognitive assessment1. In line with the point, previous studies providing normative data for the MoCA stressed the importance of considering age and level of education to increase its reliability and validity in clinical practice and research detecting MCI18,19,20. In contrast to neurodegenerative diseases, the stroke population shows higher heterogeneity in age by including all age decades and hence the consideration of age in the assessment of cognitive performance is unavoidable. In the present study, we showed that age and level of education significantly impact MoCA performance after stroke. By considering age and years of education, we identified new MoCAraw cutoffs for patients with ≤ 12 years of education: < 26 and < 22, for patients ≤ 70 and > 70 years old correspondingly. For patients with > 12 years of education, the cutoffs were: < 28, < 26, and < 25 for < 55, 55–70, and > 70 years old correspondingly (Table 3).
The cutoff of < 26 was optimal in patients aged 55–70 both with higher and lower years of education, and in those aged < 55 with ≤ 12 years of education. However, it should be considered that the MoCAraw differs from the original MoCA(+1), as patients with ≤ 12 years of education did not receive correction with + 1 point. Specifically, in patients with ≤ 12 years of education, a MoCAraw of 26 corresponds to an original MoCA(+1) of 279. In young stroke adults < 55 years old, the newly defined cutoffs increased the sensitivity at the expense of specificity. Conversely, in older patients (> 70 years old) the newly defined cutoffs increased the specificity at the expense of sensitivity. The choice of the cutoff in favour of a higher sensitivity or specificity depends on the diagnostic aims21: e.g. whether the overall correct differentiation between patients with and without pathology is needed or whether the screening for pathology with higher sensitivity is more appropriate. The former represented the aim of the present study, and correspondingly the new cutoffs performed better when the performance was evaluated with Youden Index, AUC, LR+, and LR−. In the present study we report a comprehensive overview of the discriminant ability of MoCA cutoffs between 22 and 28, for six demographic groups.
Our study sample was characterised by mainly mild stroke severity. Despite this, PSCI was present in 70.7% of patients. In patients with evident and severe neurological impairment, like aphasia and motor deficits, it is easier to decide on further patient care, triage, and rehabilitation indication, while less apparent cognitive deficits can be overseen in a routine neurological examination. In these patients, it is therefore essential to assess cognitive functions in the acute stroke phase1, at least with a screening tool or a short neuropsychological assessment, which must have acceptable discriminant ability. With the MoCA(+1) cutoff < 26, PSCI would be underdiagnosed in every second patient < 55 years old, and these patients would not have received the necessary rehabilitation, despite the high daily demand considering the ability to drive, to work, and family responsibilities associated with high societal burden52. Conversely, in elderly patients > 70 years old, the original MoCA(+1) cutoff < 26 would erroneously diagnose PSCI in more than one-third of them, which might lead to wrong triage, and unnecessary increase the costs for assistance service and care or admission to nursing homes. In line with the point, the low specificity of the original MoCA(+1) cutoff was also shown for dementia diagnosis with 40% of people without dementia being incorrectly diagnosed53. This stresses the low validity of the original MoCA(+1) cutoff and the importance of adapting it based on age and education level18 when screening for PSCI.
Although the new cutoffs performed better than the MoCA(+1) < 26 cutoff, some factors limiting the validity of MoCA are to be considered. First, though the MoCA incorporates tests for essential cognitive domains, some relevant cognitive domains are omitted but were assessed in the neuropsychological testing (e.g. visuospatial neglect, learning abilities, figural memory, processing speed). Second, several cognitive tasks in MoCA are too simple and insensitive for younger adults or subjects with higher education level leading to the ceiling effect and consequently poor MoCA validity in the detection of PSCI. For example, digit span backward in the MoCA test with only 3 numbers corresponds to normal performance in subjects aged ≥ 6535. Another critical aspect is the weighting of the specific deficits. For example, tasks for executive functions (short trail-making test, abstraction, working memory) are scored with 4/30, whereas the orientation might be overrepresented in MoCA with 6/30. The structure of MoCA subtests, their weighting, and ceiling effects can explain the still not optimal discrimination ability in young adults and subjects with higher education level as e.g. in patients aged < 55 and > 70 with higher educational level the sensitivity was < 70% (= poor).
The present study has some limitations. We excluded patients with aphasia, due to the impact of language deficit on cognitive performance. Cognitive deficits in patients with aphasia are also frequent, but as aphasia as a cognitive syndrome is more apparent in the clinical routine examination than e.g. executive deficits, the presence of PSCI in them is usually not misdiagnosed. Further, though the new cutoffs enhanced the MoCA’s ability to differentiate patients with and without PSCI, they increased the implementation demand by operating with 4 different cutoffs. Due to the small sample size in some groups, we decided not to perform an internal cross-validation, and further external validation is needed. Furthermore, the new cutoffs for patients aged > 70 years largely improved the specificity though by reducing the sensitivity and increasing LR−. However, as the aim of the study was improvement of diagnostic ability, the newly automatically identified cutoffs performed overall significantly better in this group especially when considering LR+. However, the choice of a cutoff with higher sensitivity or specificity depends on the screening aims, therefore we provided transparently the discriminant abilities for cutoffs range 22–28 for all six demographic groups in the Supplements. Some sub-cohorts in the present study were small and larger samples or further adjustments, e.g. for sex, could allow further fine-tuning of the discriminant ability of MoCA cutoffs. However, we do believe that the limitations of MoCA test discussed above—subtests structure and ceiling effects—do not allow an excellent identification of PSCI across young stroke adults and patients with higher education level. In addition, one might doubt whether the binary cutoffs for global cognition are helpful in patient care. Rather the development of a new unitary approach assessing cognitive profiles in stroke—e.g. similar to the Oxford Cognitive Screen54—but specific for different age and level of education groups might represent a more promising option to improve the detection of PSCI. The strengths of the present study include (i) the application of comprehensive neuropsychological assessment for the evaluation of PSCI, (ii) the application of strict criteria for the definition of PSCI, and iii) the development of cutoffs considering age and level of education.
To summarize, age and education level should be considered in evaluation of MoCA performance. The newly defined cutoffs increase the ability to differentiate stroke survivors with and without PSCI and thus potentially improving further patients’ care, triage, and rehabilitation. However, despite these improvements, the performance of the MoCA in the detection of PSCI in young stroke adults and adults with higher education level was suboptimal and cautious interpretation in these patients is warranted.
Data availability
Anonymized data will be shared upon reasonable request by a qualified investigator to the corresponding author after approval of the local ethics committee.
References
Quinn, T. J. et al. European Stroke Organisation and European Academy of Neurology joint guidelines on post-stroke cognitive impairment. Eur. Stroke J. 6, I–XXXVIII (2021).
Jokinen, H. et al. Post-stroke cognitive impairment is common even after successful clinical recovery. Eur. J. Neurol. 22, 1288–1294 (2015).
Barbay, M., Diouf, M., Roussel, M., Godefroy, O. & Group, G. S. Systematic review and meta-analysis of prevalence in post-stroke neurocognitive disorders in hospital-based studies. Dement. Geriatr. Cogn. Disord. 46, 322–334 (2018).
Sexton, E. et al. Systematic review and meta-analysis of the prevalence of cognitive impairment no dementia in the first year post-stroke. Eur. Stroke J. 4, 160–171 (2019).
Pendlebury, S. T. & Rothwell, P. M. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: a systematic review and meta-analysis. Lancet Neurol. 8, 1006–1018 (2009).
Obaid, M., Flach, C., Marshall, I., Wolfe, D. A. & Douiri, A. Long-Term outcomes in stroke patients with cognitive impairment: A population-based study. Geriatrics 5, 32 (2020).
Gallucci, L. et al. Post-stroke cognitive impairment remains highly prevalent and disabling despite state-of-the-art stroke treatment. Int. J. Stroke https://doi.org/10.1177/17474930241238637 (2024).
Milosevich, E., Moore, M. J., Pendlebury, S. & Demeyere, N. Domain-specific cognitive impairment 6 months after stroke: the value of early cognitive screening. Int. J. Stroke 1, 255 (2023).
Nasreddine, Z. S. et al. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 53, 695–699 (2005).
Brambilla, M. et al. Comparison of Oxford Cognitive Screen and Montreal Cognitive Assessment feasibility in the stroke unit setting. A pilot study. Cereb. Circul.-Cogn. Behav. 2, 100021 (2021).
Godefroy, O. et al. Is the Montreal Cognitive Assessment superior to the Mini-Mental State Examination to detect poststroke cognitive impairment? A study with neuropsychological evaluation. Stroke 42, 1712–1716 (2011).
Chan, E. et al. Underestimation of cognitive impairments by the Montreal Cognitive Assessment (MoCA) in an acute stroke unit population. J. Neurol. Sci. 343, 176–179 (2014).
Demeyere, N. et al. Domain-specific versus generalized cognitive screening in acute stroke. J. Neurol. 263, 306–315 (2016).
Verdelho, A. et al. Cognitive impairment in patients with cerebrovascular disease: A white paper from the links between stroke ESO Dementia Committee. Eur. Stroke J. 6, 5–17 (2021).
Pendlebury, S. T., Mariz, J., Bull, L., Mehta, Z. & Rothwell, P. M. MoCA, ACE-R, and MMSE versus the National Institute of Neurological Disorders and Stroke-Canadian Stroke Network vascular cognitive impairment harmonization standards neuropsychological battery after tia and stroke. Stroke 43, 464–469 (2012).
Malek-Ahmadi, M. et al. Age-and education-adjusted normative data for the Montreal Cognitive Assessment (MoCA) in older adults age 70–99. Aging Neuropsychol. Cogn. 22, 755–761 (2015).
Chertkow, H., Nasreddine, Z., Johns, E., Phillips, N. & McHenry, C. The Montreal Cognitive Assessment (MoCA): Validation of alternate forms and new recommendations for education corrections. Alzheimer’s Dementia 7, S157 (2011).
Thomann, A. E. et al. The Montreal Cognitive Assessment: normative data from a German-speaking cohort and comparison with international normative samples. J. Alzheimer’s Disease 64, 643–655 (2018).
Pereiro, A. X. et al. Normative data for the Montreal Cognitive Assessment (MOCA) in a Spanish sample of community-dweller adults. Eur. Geriatr. Med. 8, 240–244 (2017).
Borland, E. et al. The Montreal Cognitive Assessment: normative data from a large Swedish population-based cohort. J. Alzheimer’s Disease 59, 893–901 (2017).
Malek-Ahmadi, M., O’Connor, K., Schofield, S., Coon, D. W. & Zamrini, E. Trajectory and variability characterization of the Montreal cognitive assessment in older adults. Aging Clin. Exp. Res. 30, 993–998 (2018).
Milani, S. A., Marsiske, M. & Striley, C. W. Discriminative ability of Montreal Cognitive Assessment subtests and items in racial and ethnic minority groups. Alzheimer Disease Assoc. Disord. 33, 226 (2019).
Hoops, S. et al. Validity of the MoCA and MMSE in the detection of MCI and dementia in Parkinson disease. Neurology 73, 1738–1745 (2009).
Carson, N., Leach, L. & Murphy, K. J. A re-examination of Montreal Cognitive Assessment (MoCA) cutoff scores. Int. J. Geriatr. Psychiatry 33, 379–388 (2018).
Salvadori, E. et al. Predictive value of MoCA in the acute phase of stroke on the diagnosis of mid-term cognitive impairment. J. Neurol. 260, 2220–2227 (2013).
Salvadori, E., Cova, I., Mele, F., Pomati, S. & Pantoni, L. Prediction of post-stroke cognitive impairment by Montreal Cognitive Assessment (MoCA) performances in acute stroke: Comparison of three normative datasets. Aging Clin. Exp. Res. 34, 1–9 (2022).
Murphy, T. H. & Corbett, D. Plasticity during stroke recovery: from synapse to behaviour. Nat. Rev. Neurosci. 10, 861–872 (2009).
Umarova, R. M. et al. Predictors and signatures of recovery from neglect in acute stroke. Ann. Neurol. 79, 673–686 (2016).
Jorm, A. A short form of the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE): Development and cross-validation. Psychol. Med. 24, 145–153 (1994).
Ehrensperger, M. M., Berres, M., Taylor, K. I. & Monsch, A. U. Screening properties of the German IQCODE with a two-year time frame in MCI and early Alzheimer’s disease. Int. Psychogeriatr. 22, 91–100 (2010).
Huber, W., Poeck, K., Weniger, D. & Willmes, K. AAT-Aachener Aphasie Test (Hogrefe, 1983).
Morris, J. C., Mohs, R. C. & Rogers, H. Consortium to establish a registry for Alzheimer’s Disease (CERAD) clinical and neuropsychological. Psychopharmacol. Bull. 24, 641 (1989).
Hachinski, V. et al. National Institute of Neurological Disorders and Stroke-Canadian Stroke Network vascular cognitive impairment harmonization standards. Stroke 37, 2220–2241 (2006).
Umarova, R. M. et al. Cognitive reserve impacts on disability and cognitive deficits in acute stroke. J. Neurol. 266, 2495–2504 (2019).
Wechsler, D. Wechsler adult intelligence scale–Fourth Edition (WAIS–IV). San Antonio, TX: NCS Pearson 22, 816–827 (2008).
Gauthier, L., Dehaut, F. & Joanette, Y. The bells test: A quantitative and qualitative test for visual neglect. Int. J. Clin. Neuropsychol. 11, 49–54 (1989).
Mistridis, P. et al. Considering the base rates of low performance in cognitively healthy older adults improves the accuracy to identify neurocognitive impairment with the Consortium to Establish a Registry for Alzheimer’s Disease-Neuropsychological Assessment Battery (CERAD-NAB). Eur. Arch. Psychiatry Clin. Neurosci. 265, 407–417 (2015).
Berres, M., Monsch, A. U., Bernasconi, F., Thalmann, B. & Stähelin, H. B. Normal ranges of neuropsychological tests for the diagnosis of Alzheimer’s disease. in Medical Infobahn for Europe 195–199 (IOS Press, 2000).
Scott, C. A., Li, L. & Rothwell, P. M. Diverging temporal trends in stroke incidence in younger vs. older people: A systematic review and meta-analysis. JAMA Neurol. 79, 1036–1048 (2022).
Feigin, V. L. et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 20, 795–820 (2021).
Youden, W. J. Index for rating diagnostic tests. Cancer 3, 32–35 (1950).
Thiele, C. & Hirschfeld, G. cutpointr: Improved estimation and validation of optimal cutpoints in R. J. Stat. Software 98, 1–27 (2021).
McGee, S. Simplifying likelihood ratios. J. General Intern. Med. 17, 647–650 (2002).
Boyd, J. C. Statistical analysis and presentation of data. Evid.-Based Lab. Med. 113–140 (2007).
Campbell, J. M. et al. Diagnostic test accuracy: methods for systematic review and meta-analysis. JBI Evid. Implement. 13, 154 (2015).
Zuo, L. et al. Screening for cognitive impairment with the Montreal Cognitive Assessment in Chinese patients with acute mild stroke and transient ischaemic attack: a validation study. BMJ Open 6, e011310 (2016).
Swartz, R. H. et al. Validating a pragmatic approach to cognitive screening in stroke prevention clinics using the Montreal Cognitive Assessment. Stroke 47, 807–813 (2016).
Shi, D., Chen, X. & Li, Z. Diagnostic test accuracy of the Montreal Cognitive Assessment in the detection of post-stroke cognitive impairment under different stages and cutoffs: A systematic review and meta-analysis. Neurol. Sci. 39, 705–716 (2018).
Wei, X. et al. Which cut-off value of the Montreal Cognitive Assessment should be used for post-stroke cognitive impairment? A systematic review and meta-analysis of studies on diagnostic test accuracy. Int. J. Stroke 18, 908 (2023).
Tu, Q. et al. Reliability, validity, and optimal cutoff score of the Montreal Cognitive Assessment (Changsha version) in ischemic cerebrovascular disease patients of Hunan Province, China. Dementia Geriatr. Cogn. Disorders Extra 3, 25–36 (2013).
Munthe-Kaas, R. et al. Test accuracy of the Montreal cognitive assessment in screening for early poststroke neurocognitive disorder: the nor-COAST study. Stroke 52, 317–320 (2021).
Feigin, V. L. et al. Pragmatic solutions to reduce the global burden of stroke: A World Stroke Organization-Lancet Neurology Commission. Lancet Neurol. 22, 1160–1206 (2023).
Davis, D. H. et al. Montreal Cognitive Assessment for the detection of dementia. Cochrane Database Syst. Rev. (2021).
Demeyere, N., Riddoch, M. J., Slavkova, E. D., Bickerton, W.-L. & Humphreys, G. W. The Oxford Cognitive Screen (OCS): Validation of a stroke-specific short cognitive screening tool. Psychol. Assess. 27, 883 (2015).
Funding
This work is funded by the Synapsis Foundation and Heidi Seiler Foundation (Grant number 2019-PI05).
Author information
Authors and Affiliations
Contributions
L.G. conceptualization, data curation, formal analysis, investigation, methodology, project administration, visualization, writing and reviewing the manuscript. C.S. methodology, visualization, writing and reviewing the manuscript. A.U.M. supervision, writing and reviewing the manuscript. S.K. conceptualization, writing and reviewing the manuscript. M.A. resources, writing and reviewing the manuscript. R.M.U. funding, supervision, conceptualization, data curation, formal analysis, investigation, methodology, project administration, visualization, writing and reviewing the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Gallucci, L., Sperber, C., Monsch, A.U. et al. Improving diagnostic accuracy of the Montreal Cognitive Assessment to identify post-stroke cognitive impairment. Sci Rep 14, 20125 (2024). https://doi.org/10.1038/s41598-024-71184-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-71184-x
- Springer Nature Limited