
Abstract
The normal reference value of the global longitudinal left atrial strain during the reservoir phase (LASr) by 3D speckle-tracking echocardiography (3DSTE) is needed to define the abnormal and normal spectra and to compare and interpret the obtained values. The present study is a meta-analysis of 3DSTE-derived normal reference value of the longitudinal LASr and an attempt to determine probable contributing factors in the variations of reported ranges. The databases of PubMed, Scopus, and Embase were searched for the following keywordS: “Left atrial/left atrium” and “strain/speckle/deformation” and "three-dimensional/3-dimensional/three dimensional/3 dimensional/three dimension/3 dimension/three-dimension/3-dimension/3D/3-D". The studies selected included those on adult healthy subjects without cardiovascular risk factors. A random-effect model was used to calculate the global 3DSTE-derived longitudinal LASr, and meta-regression was applied to determine inter-study heterogeneity. Our search yielded 316 adult subjects from 5 studies. The mean value of the global 3DSTE-derived longitudinal LASr was 27.5% (95% CI, 25.2–29.8%). There was significant heterogeneity between the studies. The meta-regression analysis revealed the publication year, the heart rate, and systolic and diastolic blood pressure as the sources of heterogeneity. The current meta-analysis determined a normal reference value of the global 3DSTE-derived longitudinal LASr of 27.5% (95% CI, 25.2–29.8%). The heterogeneity between studies may be explained by the publication year, the heart rate, and systolic and diastolic blood pressure.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
The left atrium (LA) is a chamber between the pulmonary veins and the left ventricle (LV). The LA wall is thin by comparison with the LV wall. The chamber regulates LV filling and works in interaction with the LV. The LA has 3 phasic functions during the cardiac cycle: reservoir, whereby blood is stored during the LV systole; conduit, whereby blood is transferred to the LV in early diastole; and contraction, whereby blood is pushed into the LV in late diastole1.
The LA phasic functions can be evaluated by several modalities such as echocardiography, computed tomography, and cardiac magnetic resonance imaging2. The phasic functions of the LA can also be evaluated by several echocardiographic methods such as 2D or 3D volumetric parameters, pulsed-wave Doppler, tissue Doppler imaging, and myocardial deformation imaging3. Not only are the deformation markers less load-dependent2 and less affected by tethering motion, but also they are angle independent4. The use of 2D speckle-tracking echocardiography (2DSTE) has been widespread for the evaluation of the LA phasic functions, and the modality has received attention from echocardiography societies, which have presented standardization recommendations5. However, 3D deformation markers have been validated in experimental and human studies6, and deformational parameters obtained by 3D speckle-tracking echocardiography (3DSTE) have more agreement with cardiac magnetic resonance tagging than those obtained by 2DSTE7. By comparison with 2DSTE, 3DSTE is not affected by out-of-plane motion or twisting motion produced by motion in the third direction8. Moreover, 3DSTE is a feasible and reproducible method6,8 that has been applied to evaluate the LA phasic functions in various clinical conditions such as atrial fibrillation, hypertrophic cardiomyopathy, hypertension, and healthy subjects9,10,11,12,13.
Whereas 2DSTE-derived normal values for the LA deformation indices have already been presented14, 3DSTE-derived normal reference values for the LA deformation indices have yet to be determined. Normal reference values are necessary for the recognition of abnormal values, and they can lead to more clinical application of the LA assessment by 3DSTE.
The measurement of the longitudinal LA strain during the reservoir phase by 3DSTE (3DLASr) or 2DSTE (2DLASr) has been done in most published articles in this field rather than strain values in other directions or phases15. Accordingly, in the present study, we sought to determine not only normal reference values for the longitudinal 3DLASr in adults through a systematic review and a meta-analysis but also the cause of variations in values.
Methods
Search profile
The conduct of the present study was in keeping with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines16. The databases of PubMed, Scopus, and Embase were searched for the following keywords: “Left atrial/left atrium" and “strain/speckle/deformation” and "three-dimensional/3-dimensional/three dimensional/3 dimensional/three dimension/3 dimension/three-dimension/3-dimension/3D/3-D" (Supplement 1). Another strategy was to perform a reference search to identify related studies. The search was restricted to the English language. The search was done on April 29, 2021, and the study was registered at PROSPERO on March 13, 2021 (CRD42021236533).
Study selection
Studies were included if they reported longitudinal LASr as numbers (the mean and the standard deviation vs only the mean in figures) in healthy subjects. Exclusion criteria consisted of animal studies, review articles, case reports, letters to editors, editorials, and conference abstracts. Also excluded were studies without control groups, studies with control groups containing healthy subjects aged below 18 years, studies featuring control group patients with cardiovascular risk factors, studies with inadequate descriptions of control groups regarding the absence of cardiovascular risk factors, and studies reporting the averaged values of the LA segments rather than the global value. This stage was done independently by 3 investigators (T.M., R.M.B., and A.H.). Disagreements were resolved according to consensus between A.H. and T.D.
Data collection
The eligible articles were reviewed by the three investigators (T.M., R.M.B., and A.H.) independently. Study characteristics, clinical data, echocardiographic method characteristics, echocardiography data, and 3DLASRr were extracted. The disagreements were resolved according to consensus between A.H. and T.D. Among the studies that used the same data set, the studies selected were those that (a) included control subjects not matched with a case group, (b) were not confined to a special subgroup, and (c) had more control subjects.
Statistical analysis
The statistical analysis was done by Stata software, version 16 (College Station, TX: StataCorp LLC). The mean and the 95% confidence interval (CI) of 3DLASr were computed by the random-effects model. The Cochrane’s Q test (P < 0.1) and the I2 statistic were used for the evaluation of heterogeneity between the studies. The results were illustrated as a forest plot. Clinical and demographic data, if reported by more than 2 studies, were considered a possible source of 3DLASr variations and evaluated by meta-regression to estimate their effects on the variation of the normal reference value of 3DLASr. The results were presented as β and 95% CI. The stability of the estimated normal reference value of 3DLASr was presented through a comparison between the random-effects model and a fixed-effects model by excluding a study conducted with General Electric software and by excluding the studies that had less CI overlap with other studies. Publication bias was assessed by the Egger test (P < 0.1).
The quality of the studies, including internal and external validity criteria, was assessed by the quality evaluation tool, presented by Downs and Black (1998)17. The tool has also been used by other researchers14,18. Similar to other meta-analyses in this field14,18, in the present study, criteria considered for study quality included inter and intraobserver variability, the blindness of the operators who obtained images and analyzed videos, the reporting of the heart rate and systolic and diastolic blood pressure, and the approach to the computation of 3DLASr. The quality of the selected studies was checked by T.M., R.M.B., and A.H. independently, and disagreements were resolved by consensus between A.H. and T.D.
Results
Study selection
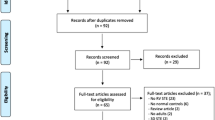
Figure 1 demonstrates the PRISMA flowchart of this study. Our search procedure identified 1198 studies. After the exclusion of duplications, 787 articles were entered in the screening stage. The titles and abstracts of these studies were reviewed to identify the studies that fulfilled our inclusion and exclusion criteria. Sixty-eight studies were eligible for full-text review. Reference search was not added to other studies. Sixty-three studies were excluded based on the exclusion criteria (Supplemental Table 1S). Ultimately, 5 studies were included. The baseline data of these studies are presented in Table 1. These studies were conducted on a total of 316 subjects. Four studies were performed with Toshiba software and 1 study with General Electric software. The mean age range of the subjects was 32 to 54 years, and sex composition was 44–79% for males. The other presented data were compatible with healthy subjects. Two studies measured 2DLASr and 3DLASr concomitantly9,13.

The image illustrates the study design and the preferred reporting items for systematic reviews and meta-analyses flowchart, presenting the selection process of studies. The reasons for full-text exclusion are demonstrated in Supplemental Table 1S.
Normal strain value
The pooled normal value for the global longitudinal 3DLASr was 27.5% (95% CI, 25.2–29.8%). The range of the global longitudinal 3DLASr was 23.7–31.0%. The heterogeneity between the studies was significant (Q = 29, P < 0.001, I2 = 85.7%) (Fig. 2).

The image depicts the normal range of the longitudinal 3D speckle-tracking echocardiography-derived left atrial strain during the reservoir phase.
The sensitivity analysis with fixed effects models presented the mean value for the global longitudinal 3DLASr of 26.9% (95% CI, 26.1–27.8%). Following the exclusion of the General Electric software-based study, the mean value of the global longitudinal 3DLASr was 28.4% (95% CI, 27.0–29.7%) according to the random-effects model. The Toshiba-based study forest plot is presented in Fig. 3. Following the exclusion of 2 studies, one of which was the General Electric software-based study, on account of having less CI overlap with the other studies, the mean value for the global longitudinal 3DLASr was 27.8% (CI, 26.7–28.9%).

The image shows the normal range of the longitudinal 3D speckle-tracking echocardiography-derived left atrial strain during the reservoir phase analyzed by Toshiba software.
The origin of heterogeneity was evaluated by meta-regression. The publication year (β = − 0.60, P = 0.026), the heart rate (β = 1.78, P ≤ 0.001), and systolic (β = − 0.28, P ≤ 0.001) and diastolic (β = − 1.30, P = 0.002) blood pressure were recognized as the sources of inter-study heterogeneity (Table 2).
The assessment of publication bias revealed no significant publication bias for the global longitudinal 3DLASr (P = 0.150 for the Egger test).
Two studies9,13 reported 2DLASr values of 35.8 ± 7.7% and 39.4 ± 12.1% and 3DLASr values of 28.1 ± 7.4% and 23.7 ± 7.6%, respectively. The mean difference value and the standard deviation of these two methods in these investigations were 7.7 ± 8.1% and 15.7 ± 12.1%, respectively, with a P value of less than 0.001 in both studies.
Quality of studies
The included studies satisfied five to eight items of 11 items designed for quality evaluation. One study satisfied fewer than 50% of the items, two studies satisfied 55% of the items, and two studies satisfied about 70% of the items. All the studies described their objectives, outcomes, main findings, and strain imaging protocol. Intra- and interobserver variability was reported by four out of the five studies (Supplemental Table 2S).
Discussion
We are the first to present the normal reference value of the global longitudinal 3DLASr through a meta-analysis. The LA works in interaction with the LV during the cardiac cycle. At the ventricular systole, blood enters the LA through the pulmonary veins while the LV contracts, which pulls the mitral annulus toward the LV apex to help the LA expand15. Thus, the LA deformation during the LV systole is dependent on the innate properties of the LA and LV function. Accordingly, LASr can reflect fibrosis in the LA myocardium19 and the properties of the LV such as the LV end-diastolic pressure20. Previous research has provided the clinical values of LASr in the prediction of clinical conditions such as exercise capacity21 and LV dysfunction grading22, as well as future cardiovascular events such as survival and the recurrence of atrial fibrillation23,24.
A major method for the evaluation of the LA function is 2DSTE5, with meta-analyses having already presented the normal reference value for its markers14. Still, this method has some weaknesses. A fixed plane is required for 2DSTE, which means that speckles during cardiac cycles should not exit the defined plane. The translational motion of the heart or myocardial motion in another direction precludes the satisfaction of this assumption. The evaluation of the global strain needs images from multiple planes during different cardiac cycles. Although 3DSTE provides images more rapidly than 2DSTE and does not require imaging in multiple planes and during a different cardiac cycle, it suffers from lower spatial and time resolution and stitch artifacts due to multi-beat acquisition6,8,25. There is a paucity of research on the comparison between 2 and 3DSTE for the prediction of clinical events, but it has been demonstrated that 3DSTE is stronger for the prediction of atrial fibrillation recurrence and the differentiation of patients with paroxysmal atrial fibrillation from the control group9,26.
Comparison of 2DLASr and 3DLASr in the two included studies revealed that 2DLASr was more than 3DLASr in both investigations, which is compatible with the findings of a previous meta-analysis14. The meta-analysis reported an approximate normal reference value for 2DLASr of 39.4% (95% CI, 38.0–40.8%), which is more than the value we obtained for 3DLASr (ie, 27.5%) (95% CI, 25.2–29.8%). The aforementioned comparisons between the 2 methods may explain the difference between these two values. It is worthy to cite that our meta-analysis on 3DLASr is on a lower scale than previous meta-analyses on 2DLASr.
Demographic characteristics
We did not find age and sex as a source of heterogeneity, which chimes in with the finding of a previous meta-analysis regarding 2DLASr14. Although it does not mean that factors such as age exert no effects on the LA reservoir function, it does indicate that these factors are not a source of variability in the normal reference value presented in the included studies. A reduction in 2DLASr in tandem with increasing age has been demonstrated in several studies27,28,29,30,31, but we stress that the age range in the studies included in the present meta-analysis was not wide (32–54 years). A previous investigation demonstrated an increase in 3DLASr after 50 years32. In most of the studies included in our meta-analysis, the participants were younger than 50 years of age30.
Sex was not a determinant of 2DLASr in most studies subjected to meta-analysis27,28,29,30,31. In a study that evaluated 3DLASr in men and women, the results showed no difference between the two sexes vis-à-vis this marker32. Likewise, we did not find sex to be a source of inter-study heterogeneity.
Comparison of 2DLASr between European and Asian races in a previous investigation demonstrated no difference between the two ethnic groups30, which is concordant with our findings.
Whereas a meta-analysis on 2DLASr found a correlation between the body surface area and 2DLASr14, only three studies reported the body surface area with a very narrow range in our meta-analysis.
Hemodynamic variables
The heart rate is the source of heterogeneity in studies regarding 2DLASr14. Nonetheless, several studies have demonstrated that the heart rate is not an independent determinant of 2DLASr28,29,31. Our results showed the heart rate as the source of inter-study heterogeneity. It is worthy of note that the range of the heart rate in the studies included in our meta-analysis was narrow (65–69 bpm), with only three studies having reported the heart rate as the mean and the standard deviation. It is, therefore, possible that the heart rate by chance presented itself as a source of inter-study heterogeneity.
Blood pressure in healthy subjects is associated with 2DLASr29,31. The findings of our study are compatible with the studies reporting this association.
Echocardiography data
The LV systolic function is correlated with the LA reservoir function28,33. The LV ejection fraction is a marker of the LV systolic function, and 3DLASr is a marker of the LA reservoir function. In our study, the mean LV ejection fraction was within the normal range, so the LV ejection fraction was not a source of heterogeneity between the included studies. The LA volume index was correlated with 2DLASr in some studies27,30,31. The LA volume index in the included studies was lower than that in studies that confirmed the correlation between 2DLASr and the LA volume index27,31.
Subvolume numbers (4 vs 6) were not correlated with 3DLASr. The increased subvolume was accompanied by an increased frame rate as an index of temporal resolution, but it seems that it was not a determinant of heterogeneity between the included studies.
Our exclusion of the single General Electric software-based study resulted in no significant changes in the normal range of LASr.
We found the publication year to be a source of heterogeneity. It is possible that the time elapsed since the first 3DLASr measurement is allied to more expertise in this regard.
The finding of the source of heterogeneity in our study by meta-regression was affected by the low number of studies included. In addition, not all the included studies provided the details of the study population such as the body mass index or the body surface area, clinical data such as blood pressure, or echocardiography data such as the LA volume index, precluding an in-depth analysis. The factors may, therefore, be a source of heterogeneity between studies.
Publication bias
The results of our meta-analysis showed no significant publication bias, although the limited number of included studies precluded exact results. It should be, however, noted that we searched studies via a hierarchical method whereby three independent researchers reviewed all abstracts and selected full texts; additionally, all discrepancies were resolved according to consensus between two of the researchers. This checking method lessened the probability of missing related manuscripts.
Our study results yielded the normal reference range of 3DLASr, although the range was obtained from a low number of suitable studies. Our findings can be used in clinical practice until future studies provide more robust data regarding 3DLASr among healthy normal subjects. These values may assist in the longitudinal assessment of patients who suffer from chronic conditions such as heart failure with reduced or preserved ejection fractions or those who were exposed to acute events such as myocardial infarction because they can depict changes from the normal range to the abnormal range.
Our study revealed a need for more studies regarding the normal reference value of 3DLASr because of the dearth of high-quality studies in this field. Indeed, the majority of the studies that were suitable for our meta-analysis did not measure deformation in other directions or during the conduit or contraction phase. In addition, data are absent regarding the comparison of 3DLASr and the value obtained by cardiac magnetic resonance imaging.
Study limitations
The present meta-analysis incorporated five studies on a total of 316 subjects. This sample size is low by comparison with studies via 2DSTE. We are hopeful that the publication of more studies investigating deformation in other directions and in other phasic times will contribute to more optimal meta-analyses since we were not able to provide values for these markers in our study.
The studies included in our meta-analysis were observational or case–control, which are associated with high heterogeneity compared with randomized control trials because of the objective entity of these types of studies34.
The software that is used for 3DSTE is semiautomatic, and the competency of the operators who obtain deformation data is unknown. In our meta-analysis, we considered the same value for all the studies included. The absence of large-scale studies yielding preliminary normal reference values should be addressed in the future.
We could not conclusively assess the difference in vendors since we had four studies performed with Toshiba software and only one study conducted with General Electric software.
The fact that the study populations in the case and control groups of all the studies incorporated in the current meta-analysis were Asian also prevented us from demonstrating any possible differences concerning the normal reference value of 3DLASr between ethnicities.
Another weakness of note is that we analyzed study data, and not patient data, on account of the unavailability of the former. We also assessed the quality of the included studies according to the checklist used in similar meta-analyses in this field14,35. Although this checklist prevents significant bias in the evaluation of studies, it is not objective totally36. What can also be deemed a limitation is that we did not exclude any studies because of low quality. Still, the overall quality of the included studies, albeit not excellent, was by no means poor insofar as they satisfied about 60% of the required items on average.
Finally, we were not able to conduct a stratified meta-analysis by considering the quality of studies because of the innate properties of quality37.
Conclusions
We demonstrated a mean global 3DSTE-derived longitudinal LASr of 27.5% (95% CI, 25.2–29.8%) in normal healthy subjects. The heterogeneity in different normal reference values was related to the publication year, the heart rate, and systolic and diastolic blood pressure. Further studies in this field are required to confirm the normal reference value of the LA deformation markers obtained by 3DSTE.
Data availability
The data sets analyzed in the current study are available from the corresponding author on reasonable request.
References
Kebed, K. Y., Addetia, K. & Lang, R. M. Importance of the left atrium: More than a bystander?. Heart Fail. Clin. 15, 191–204. https://doi.org/10.1016/j.hfc.2018.12.001 (2019).
Thomas, L. et al. Evaluation of left atrial size and function: Relevance for clinical practice. J. Am. Soc. Echocardiogr. 33, 934–952. https://doi.org/10.1016/j.echo.2020.03.021 (2020).
Hoit, B. D. Assessment of left atrial function by echocardiography: Novel insights. Curr. Cardiol. Rep. 20, 96. https://doi.org/10.1007/s11886-018-1044-1 (2018).
Voigt, J. U. & Cvijic, M. 2- and 3-dimensional myocardial strain in cardiac health and disease. JACC Cardiovasc. Imaging 12, 1849–1863. https://doi.org/10.1016/j.jcmg.2019.01.044 (2019).
Badano, L. P. et al. Standardization of left atrial, right ventricular, and right atrial deformation imaging using two-dimensional speckle tracking echocardiography: A consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging 19, 591–600. https://doi.org/10.1093/ehjci/jey042 (2018).
Nabeshima, Y., Seo, Y. & Takeuchi, M. A review of current trends in three-dimensional analysis of left ventricular myocardial strain. Cardiovasc. Ultrasound 18, 23. https://doi.org/10.1186/s12947-020-00204-3 (2020).
Amzulescu, M. S. et al. Improvements of myocardial deformation assessment by three-dimensional speckle-tracking versus two-dimensional speckle-tracking revealed by cardiac magnetic resonance tagging. J. Am. Soc. Echocardiogr. 31, 1021-1033.e1. https://doi.org/10.1016/j.echo.2018.04.009 (2018).
Muraru, D., Niero, A., Rodriguez-Zanella, H., Cherata, D. & Badano, L. Three-dimensional speckle-tracking echocardiography: Benefits and limitations of integrating myocardial mechanics with three-dimensional imaging. Cardiovasc. Diagn. Ther. 8, 101–117. https://doi.org/10.21037/cdt.2017.06.01 (2018).
Mochizuki, A. et al. Assessment of left atrial deformation and synchrony by three-dimensional speckle-tracking echocardiography: Comparative studies in healthy subjects and patients with atrial fibrillation. J. Am. Soc. Echocardiogr. 26, 165–174. https://doi.org/10.1016/j.echo.2012.10.003 (2013).
Aly, M. F., Brouwer, W. P., Kleijn, S. A., van Rossum, A. C. & Kamp, O. Three-dimensional speckle tracking echocardiography for the preclinical diagnosis of hypertrophic cardiomyopathy. Int. J. Cardiovasc. Imaging 30, 523–533. https://doi.org/10.1007/s10554-014-0364-5 (2014).
Piros, G. Á. et al. Left atrial ejection force correlates with left atrial strain and volume-based functional properties as assessed by three-dimensional speckle tracking echocardiography (from the MAGYAR-Healthy Study). Rev. Port. Cardiol. 35, 83–91. https://doi.org/10.1016/j.repc.2015.09.017 (2016).
Esposito, G. et al. Improving performance of 3D speckle tracking in arterial hypertension and paroxysmal atrial fibrillation by using novel strain parameters. Sci. Rep. 9, 7382. https://doi.org/10.1038/s41598-019-43855-7 (2019).
Nabeshima, Y., Kitano, T. & Takeuchi, M. Reliability of left atrial strain reference values: A 3D echocardiographic study. PLoS ONE 16, e0250089. https://doi.org/10.1371/journal.pone.0250089 (2021).
Pathan, F., D’Elia, N., Nolan, M. T., Marwick, T. H. & Negishi, K. Normal ranges of left atrial strain by speckle-tracking echocardiography: A systematic review and meta-analysis. J. Am. Soc. Echocardiogr. 30, 59-70.e8. https://doi.org/10.1016/j.echo.2016.09.007 (2017).
Yuda, S. Current clinical applications of speckle tracking echocardiography for assessment of left atrial function. J. Echocardiogr. https://doi.org/10.1007/s12574-021-00519-8 (2021).
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 6, e1000097. https://doi.org/10.1371/journal.pmed.1000097 (2009).
Downs, S. H. & Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Commun. Health 52, 377–384. https://doi.org/10.1136/jech.52.6.377 (1998).
Levy, P. T. et al. Normal ranges of right ventricular systolic and diastolic strain measures in children: A systematic review and meta-analysis. J. Am. Soc. Echocardiogr. 27(549–60), e3. https://doi.org/10.1016/j.echo.2014.01.015 (2014).
Lisi, M. et al. Left atrial strain by speckle tracking predicts atrial fibrosis in patients undergoing heart transplantation. Eur. Heart J. Cardiovasc. Imaging https://doi.org/10.1093/ehjci/jeab106 (2021) ((in press)).
Fan, J. L. et al. Correlation of left atrial strain with left ventricular end-diastolic pressure in patients with normal left ventricular ejection fraction. Int. J. Cardiovasc. Imaging 36, 1659–1666. https://doi.org/10.1007/s10554-020-01869-7 (2020).
Patel, R. B. et al. Associations of cardiac mechanics with exercise capacity: The multi-ethnic study of atherosclerosis. J. Am. Coll. Cardiol. 78, 245–257. https://doi.org/10.1016/j.jacc.2021.04.082 (2021).
Borde, D. et al. Left atrial strain as a single parameter to predict left ventricular diastolic dysfunction and elevated left ventricular filling pressure in patients undergoing off-pump coronary artery bypass grafting. J. Cardiothorac. Vasc. Anesth. 35, 1618–1625. https://doi.org/10.1053/j.jvca.2020.11.066 (2021).
Vasquez, N. et al. Low left atrial strain is associated with adverse outcomes in hypertrophic cardiomyopathy patients. J. Am. Soc. Echocardiogr. 32, 593-603.e1. https://doi.org/10.1016/j.echo.2019.01.007 (2019).
Koca, H. et al. Decreased left atrial global longitudinal strain predicts the risk of atrial fibrillation recurrence after cryoablation in paroxysmal atrial fibrillation. J. Interv. Cardiac Electrophysiol. 58, 51–59. https://doi.org/10.1007/s10840-019-00573-4 (2020).
Seo, Y., Ishizu, T., Atsumi, A., Kawamura, R. & Aonuma, K. Three-dimensional speckle tracking echocardiography. Circ. J. 78, 1290–1301. https://doi.org/10.1253/circj.cj-14-0360 (2014).
Mochizuki, A. et al. Left atrial strain assessed by three-dimensional speckle tracking echocardiography predicts atrial fibrillation recurrence after catheter ablation in patients with paroxysmal atrial fibrillation. J. Echocardiogr. 15, 79–87. https://doi.org/10.1007/s12574-017-0329-5 (2017).
Sugimoto, T. et al. Echocardiographic reference ranges for normal left atrial function parameters: Results from the EACVI NORRE study. Eur. Heart J. Cardiovasc. Imaging 19, 630–638. https://doi.org/10.1093/ehjci/jey018 (2018).
Sun, B. J. et al. Normal reference values for left atrial strain and its determinants from a large Korean multicenter registry. J. Cardiovasc. Imaging 28, 186–198. https://doi.org/10.4250/jcvi.2020.0043 (2020).
Liao, J. N. et al. Age, sex, and blood pressure-related influences on reference values of left atrial deformation and mechanics from a large-scale Asian population. Circ. Cardiovasc. Imaging 10, e006077. https://doi.org/10.1161/CIRCIMAGING.116.006077 (2017).
Morris, D. A. et al. Normal values and clinical relevance of left atrial myocardial function analysed by speckle-tracking echocardiography: Multicentre study. Eur. Heart J. Cardiovasc. Imaging 16, 364–372. https://doi.org/10.1093/ehjci/jeu219 (2015).
Meel, R. et al. Left atrial volume and strain parameters using echocardiography in a black population. Eur. Heart J. Cardiovasc. Imaging 18, 350–355. https://doi.org/10.1093/ehjci/jew062 (2017).
Nemes, A. et al. Normal reference values of three-dimensional speckle-tracking echocardiography-derived left atrial strain parameters (results from the MAGYAR-Healthy Study). Int. J. Cardiovasc. Imaging 35, 991–998. https://doi.org/10.1007/s10554-019-01559-z (2019).
Ramkumar, S. et al. Association of the active and passive components of left atrial deformation with left ventricular function. J. Am. Soc. Echocardiogr. 30, 659–666. https://doi.org/10.1016/j.echo.2017.03.014 (2017).
Delgado-Rodríguez, M. Systematic reviews of meta-analyses: Applications and limitations. J. Epidemiol. Commun. Health 60, 90–92. https://doi.org/10.1136/jech.2005.035253 (2006).
Truong, V. T. et al. Normal ranges of left ventricular strain by three-dimensional speckle-tracking echocardiography in adults: A systematic review and meta-analysis. J. Am. Soc. Echocardiogr. 32, 1586-1597.e5. https://doi.org/10.1016/j.echo.2019.07.012 (2019).
Levy, P. T. et al. Reference ranges of left ventricular strain measures by two-dimensional speckle-tracking echocardiography in children: A systematic review and meta-analysis. J. Am. Soc. Echocardiogr. 29, 209-225.e6. https://doi.org/10.1016/j.echo.2015.11.016 (2016).
Greenland, S. & O’Rourke, K. On the bias produced by quality scores in meta-analysis, and a hierarchical view of proposed solutions. Biostatistics 2, 463–471. https://doi.org/10.1093/biostatistics/2.4.463 (2001).
Author information
Authors and Affiliations
Contributions
Conception: A.H. Work design: A.H., T.D., R.M., T.M. Data acquisition: A.H., T.D., R.M., T.M. Analysis: A.J. Interpretation of data: A.H., T.D., R.M., T.M., A.J. Drafting of the manuscript: A.H., T.D., R.M., T.M., A.J. Substantive revision of the manuscript: A.H., T.D., R.M., T.M., A.J. Approved submitted version: A.H., T.D., R.M., T.M., A.J. All the authors agree both to be personally accountable for their own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated and resolved and the resolution is documented in the literature.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mohseni-Badalabadi, R., Mirjalili, T., Jalali, A. et al. A systematic review and meta-analysis of the normal reference value of the longitudinal left atrial strain by three dimensional speckle tracking echocardiography. Sci Rep 12, 4395 (2022). https://doi.org/10.1038/s41598-022-08379-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-08379-7
- Springer Nature Limited
This article is cited by
-
Incremental diagnostic and prognostic utility of left atrial deformation in heart failure using speckle tracking echocardiography
Heart Failure Reviews (2024)
-
New Insights in Strain Mechanics (LA, RA, and RV)
Current Cardiovascular Imaging Reports (2023)