
Abstract
Objectives
To compare real-world, long-term outcomes of laser and anti-vascular endothelial growth factor (VEGF) therapies in patients with retinopathy of prematurity (ROP).
Methods
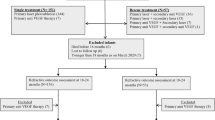
This was a multicentre retrospective study. We included 264 eyes of 139 patients treated for type 1 ROP or aggressive ROP (AROP) who were followed for at least 4 years. Laser treatment was initially performed in 187 eyes (the laser group), and anti-VEGF therapy was initially performed in 77 eyes (the anti-VEGF group). We collected data on sex, birth characteristics, zone, stage, and the presence of plus disease at the time of treatment and best-corrected visual acuity (BCVA), spherical equivalent (SE), and ocular complications (amblyopia and strabismus) in patients aged 4–6 years. We investigated the associations between treatment outcomes (BCVA, SE and the presence of amblyopia and strabismus) and influencing factors, including treatment procedure (anti-VEGF or laser therapy), sex, birth characteristics, zone, stage, and the presence of plus disease, using multivariable analysis and logistic regression analyses.
Results
The initial treatment procedure was not associated with any specific treatment outcome. Subgroup analysis of patients with zone I ROP revealed that the anti-VEGF-treated eyes had significantly better BCVA and higher SE than laser-treated eyes (p = 0.004, p = 0.009, respectively). Female patients presented significantly better BCVA, less amblyopia and less strabismus than male patients (p < 0.001, p = 0.029, p = 0.008, respectively).
Conclusions
In zone I ROP, anti-VEGF therapy led to better visual acuity and less myopic refractive error than laser treatment.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Retinopathy of prematurity (ROP) is one of the most common causes of visual disability and blindness in children [1]. Laser photocoagulation of the avascular retina is the standard treatment for ROP [2] and is highly successful [3]. In the 2000s, anti-vascular endothelial growth factor (VEGF) intravitreal therapy was introduced as a new treatment modality for ROP [4, 5]. The BEAT-ROP study showed that the recurrence rate was lower with intravitreal injection of bevacizumab (IVB) than with laser treatment in zone I stage 3 ROP [6]. The RAINBOW study showed that the treatment success rate was relatively higher with intravitreal injection of ranibizumab (IVR) than with laser treatment in type 1 ROP other than zone II stage 2 plus disease [7]. Recently, in some countries, ranibizumab has been approved for ROP treatment. It is expected that the number of treatments for ROP using anti-VEGF drugs will increase in the future.
Because it is difficult to assess visual outcomes such as visual acuity, refractive error, and the presence of amblyopia or strabismus in infants, long-term follow-up after treatment is essential. Several previous researchers compared the long-term treatment outcomes of laser photocoagulation and anti-VEGF therapy for ROP, but the number of eyes treated for ROP was relatively small [8,9,10,11,12,13]. In these studies, it was reported that best-corrected visual acuity (BCVA) did not differ between the two therapy groups [8,9,10,11,12], and more amblyopia was observed in laser-treated eyes than in anti-VEGF-treated eyes [13]. Laser treatment of posterior ROP requires the destruction of a large area of the avascular retina and sometimes involves the destruction of the retina close to the fovea. Therefore, we expect a better long-term visual outcome with anti-VEGF therapy than with laser therapy in posterior ROP. However, no reports have compared the long-term treatment outcomes of laser and anti-VEGF therapy in zone I ROP. Birth characteristics, such as gestational age or birth weight, stage of ROP, and presence of plus disease might be potential confounders of the relationship between the long-term visual outcome and treatment procedure (anti-VEGF or laser). However, few reports used multivariable methods to estimate the association between the long-term visual outcome and treatment procedure after adjusting the impact of confounding factors.
Therefore, we compared the real-world, long-term visual outcomes of laser and anti-VEGF therapy according to ROP zone in a large cohort using multivariable methods.
Methods
Study design
This was a multicentre, retrospective cohort study conducted in the following 10 institutions in the Japan Clinical Retina Study (J-CREST) group: University of Tsukuba, Sapporo City General Hospital, Tokushima University Graduate School, Nara Medical University, Shiga University of Medical Science, Nagoya City University Graduate School of Medical Sciences, Kurume University, Mie University Graduate School of Medicine, St. Marianna University School of Medicine, and Kobe University Graduate School of Medicine. This study was approved by the institutional review board of each participating institution (Approval number: R03-081) and was conducted in accordance with the tenets of the Declaration of Helsinki. The institutional review board approved the use of opt-out patient consent.
The inclusion criteria were as follows: born between 2001 and 2016, history of treatment for type 1 ROP or aggressive ROP (AROP), and observed until at least 4 years of age. After anti-VEGF therapy was introduced as a new treatment modality for ROP in each institution, the decision to treat with laser or anti-VEGF was made by the parents after the pros and cons of each treatment were fully explained. Laser photocoagulation was performed using an argon green laser indirect ophthalmoscope at all institutions. The dose of IVB was 0.625 mg/0.025 ml, and the dose of IVR was 0.20 mg/0.020 ml. The off-label use of IVB or IVR was approved by the institutional review board of each institution, and written informed consent was obtained from the parents.
The following parameters were collected from the patients’ records: sex; gestational age; birth weight; 1- and 5-min Apgar scores; zone of ROP at initial treatment, stage of ROP at initial treatment in eyes with classic ROP, presence of plus disease or AROP at initial treatment, and the initial treatment procedure (laser photocoagulation or anti-VEGF therapy). Zone I involvement at any stage with plus disease or at stage 3 without plus disease or zone II involvement at stage 2 or 3 with plus disease were defined as type 1 ROP [14]. The outcome parameters were BCVA, spherical equivalent (SE), and the presence of amblyopia and strabismus. We collected data on the outcome parameters at the age of 5 years. In cases where data were not available at age 5, data were collected at age 4 or 6. The age at the time of data collection for treatment outcomes was also collected. BCVA was measured with the Landolt chart and expressed as a logarithm of minimal angle resolution (logMAR).
Statistical analysis
Continuous variables are presented as the mean ± standard deviation (SD). Unpaired t-tests were used to compare gestational age, birth weight, 1- and 5-min Apgar scores, BCVA, and SE between the laser and anti-VEGF groups. Fisher’s exact probability tests were used to compare sex, ROP zone, stage of ROP or presence of AROP, presence of plus disease, and presence of amblyopia and strabismus. We investigated the association between treatment outcomes (BCVA, SE and the presence of amblyopia) and influential factors, including treatment procedure (anti-VEGF or laser), using multiple regression and logistic regression with generalized estimating equations (GEEs) to account for the correlation between patient eyes. We also investigated the association between the presence of strabismus and influential factors using logistic regression analysis. Variables, such as age at the time of data collection for treatment outcomes, sex, gestational age, birth weight, 1- and 5-min Apgar score, zone of ROP, stage of ROP, and presence of AROP and plus disease, might be associated with treatment outcome or the choice of treatment. Therefore, these variables were included as influential factors in the multivariate model to obtain an adjusted measure of association. All analyses were conducted using SPSS (version 27, IBC Corp., Chicago, IL, USA) and SAS (version 9.4, SAS Institute Inc., Cary, NC, USA.). A p value <0.05 was considered statistically significant. No correction was made for multiple statistical testing.
Results
A total of 264 eyes of 139 patients were analysed in this study. Of the 264 eyes, 187 eyes were initially treated with laser therapy, and 77 eyes were initially treated with anti-VEGF therapy (75 eyes were treated with bevacizumab, and 2 eyes were treated with ranibizumab). Of the 187 laser-treated eyes, because of reactivation or undertreatment, 62 eyes were treated with additional laser therapy and 11 eyes were treated with additional anti-VEGF therapy. Of the 77 anti-VEGF-treated eyes, 30 eyes were treated with additional laser therapy with or without reactivation of ROP (20 eyes and 10 eyes, respectively). In the laser group, 1 eye developed retinal detachment (RD), and multiple surgeries were performed. In the anti-VEGF group, no eyes developed RD. The baseline characteristics are shown in Table 1. There was a statistically significant difference in 5-min Apgar score between the laser group and the anti-VEGF group (p < 0.001).
The mean age at the time of data collection for treatment outcomes was 5.4 ± 0.50 years (range: 4.3–6.7) in the laser group and 5.3 ± 0.6 years (range: 4.5–6.9) in the anti-VEGF group (p = 0.220). Visual acuity could not be assessed in 22 eyes (12 eyes in the laser group, 10 eyes in the anti-VEGF group) because of neurological complications. The mean BCVA was 0.15 ± 0.35 (Snellen BCVA = 20/28) in the laser group and 0.21 ± 0.36 (Snellen BCVA = 20/32) in the anti-VEFG group (p = 0.239).
Refractive error could not be assessed in 7 eyes (4 eyes in the laser group and 3 eyes in the anti-VEGF group) because of developmental delay, bullous keratopathy, or corectopia. The mean SE was −1.77 ± 3.31 D in the laser group and −1.09 ± 3.68 D in the anti-VEFG group (p = 0.156).
The presence of amblyopia was not assessed in 25 eyes (13 eyes in the laser group and 12 eyes in the anti-VEGF group), and the presence of strabismus was not assessed in 2 cases (one in the anti-VEGF group, the other in the laser group) because of neurological complications. Fifty-four eyes (30.0%) had amblyopia in the laser group, and 18 eyes (25.4%) had amblyopia in the anti-VEGF group (p = 0.743). Twenty-two patients (22.4%) had strabismus in the laser group, and 12 patients (30.8%) had strabismus in the anti-VEGF group (p = 0.381).
Table 2 lists the results of the multivariable analysis of visual outcomes and influential factors. The treatment procedure (laser or anti-VEGF therapy) was not associated with any visual outcomes. In contrast, older age at the time of data collection for treatment outcomes was significantly correlated with less amblyopia (p = 0.038), males had significantly worse BCVA, more amblyopia, and more strabismus than females (p < 0.001, p = 0.029, p = 0.008, respectively), zone I eyes had a significantly higher myopic refractive error (p < 0.001), and eyes with plus disease had significantly more amblyopia (p = 0.036).
Subgroup analysis: eyes with zone I ROP at initial treatment
Eighty eyes of 41 patients had zone I ROP at initial treatment. Forty-eight eyes of 25 patients were initially treated with laser therapy, and 32 eyes of 16 patients were initially treated with anti-VEGF therapy. Table 3 lists the characteristics of patients with zone I ROP at initial treatment. There was a statistically significant difference in birth weight, 5-min Apgar scores, and presence of plus disease at the initial treatment between the laser group and the anti-VEGF group (p = 0.045, p = 0.005, p = 0.020, respectively).
Table 4 lists the results of the multivariable analysis of visual outcomes and influential factors. The eyes treated with anti-VEGF therapy had significantly better BCVA and a lower myopic refractive error than those treated with laser therapy (p = 0.004, p = 0.009, respectively). Older age at the time of data collection for treatment outcomes was significantly correlated with a higher myopic refractive error (p = 0.046), stage and AROP were significantly associated with BCVA and SE (p = 0.032, p = 0.009, respectively), and plus disease was significantly associated with BCVA (p = 0.031).
Subgroup analysis: eyes with zone II ROP at initial treatment
One hundred eighty-four eyes of 98 patients were zone II ROP at initial treatment. One hundred thirty-nine eyes of 74 patients were initially treated with laser therapy, and 45 eyes of 24 patients were initially treated with anti-VEGF therapy. Supplementary Table displays a list of the characteristics of patients with zone II ROP at initial treatment. There was a statistically significant difference in 5-min Apgar score between the laser group and the anti-VEGF group (p = 0.013, respectively).
Table 5 shows the results of the multivariable analysis of visual outcomes and influential factors. The treatment procedure (laser or anti-VEGF therapy) was not associated with any visual outcomes. In contrast, older age at the time of data collection for treatment outcomes was significantly correlated with less amblyopia (p = 0.024), and males had significantly worse BCVA, more amblyopia, and more strabismus than females (p < 0.001, p = 0.017, p = 0.024, respectively). Birth weight was significantly correlated with BCVA, and the 1-min Apgar score was significantly correlated with SE (p = 0.012, p = 0.014, respectively).
Discussion
Analysis of all type 1 ROP and AROP patients revealed that anti-VEGF therapy was performed for infants with lower 5-min Apgar score, and subgroup analysis with zone I ROP revealed that anti-VEGF therapy was performed for infants with lower birth weight and lower 5-min Apgar score. It was reported that anti-VEGF therapy could be performed without intubation and with lighter anaesthesia than laser therapy [8]; thus, infants with a worse general condition might be more likely to be treated with anti-VEGF therapy. Moreover, in this study, anti-VEGF therapy tended to be performed for eyes with a lower stage, lower zone, and more plus disease; however, this finding did not reach statistical significance. In zone I ROP, anti-VEGF therapy was performed for more plus disease. Gundlach et al. [13] reported that eyes receiving anti-VEGF therapy were significantly more likely to have posterior disease than those receiving laser therapy. Anti-VEGF therapy has been reported to cause tractional retinal detachment in eyes with severe fibrovascular tissue [15]. This may explain why anti-VEGF therapy was relatively more often used for lower-stage eyes in this study. It was reported that regression time was shorter in anti-VEGF therapy than laser therapy [16]; thus, we considered that the eyes with ROP considered to be severe because of the presence of plus disease were often treated with anti-VEGF therapy in this study.
Because the characteristics of the two groups were different, we used a logistic regression model and multiple regression analysis to assess the relationship between the type of initial treatment and visual outcomes. The analysis of all type 1 ROP and AROP cases revealed that the type of treatment was not associated with any visual outcomes. In contrast, the subgroup analysis of zone I ROP revealed that the eyes treated with anti-VEGF therapy had significantly better BCVA and a lower myopic refractive error than those treated with laser. In the previous studies, the number of eyes with zone I ROP was small (48, 159, 010, 011, 412, 1013 eyes) [8,9,10,11,12,13], and no previous study has compared the long-term visual outcomes of laser and anti-VEGF therapy for zone I ROP. This was the first report demonstrating the difference in long-term visual outcomes between laser and anti-VEGF therapy for zone I ROP. It was unclear why eyes treated with anti-VEGF therapy for zone I ROP had better BCVA than eyes treated with laser for zone I ROP. Several researchers have investigated the foveal structure of eyes treated for ROP. They reported that in laser-treated eyes, the foveal inner retinal thickness was greater [9, 10], the avascular zone in the fovea was smaller [10, 11], and the grade of foveal hypoplasia was lower [12] than those in anti-VEGF-treated eyes, while there was no significant difference in BCVA between anti-VEGF-treated eyes and laser-treated eyes. In these studies, the proportion of zone II eyes was high (84.2% to 100%). We speculated that in eyes treated with laser therapy, macular structural abnormalities might be more severe in eyes treated for zone I ROP than in eyes treated for zone II ROP, and consequently, in zone I ROP, better BCVA was observed in anti-VEGF-treated eyes than laser-treated eyes. However, in this study, optical coherence tomography imaging data were not obtained; thus, the relationship between foveal microstructure and visual acuity was unclear. Further studies are warranted to assess the relationship between BCVA and retinal structures in eyes treated for zone I ROP. Geloneck et al. [17] investigated refractive error in 2½-year-old children in the BEAT-ROP study cohort. They reported that, in eyes treated for zone I ROP, the SE was lower in the eyes treated with laser therapy than in those treated with bevacizumab, which was consistent with our results. Our finding in zone I ROP indicated that anti-VEGF therapy may be superior to laser therapy in terms of late visual outcomes, such as visual acuity and refractive error.
In zone II ROP, the initial treatment procedure was not associated with any specific treatment outcome. Previous studies compared the long-term treatment outcomes of laser and anti-VEGF therapy for in zone II type 1 ROP [10, 11]. They reported that BCVA did not differ between the two therapy groups, which is consistent with our results.
In this study, males had worse BCVA and more amblyopia and strabismus than females in the all-zone analysis and the zone II analysis. A nationwide population study investigating the 10-year epidemiology of and risk factors for ROP in Taiwan also showed that male sex was significantly associated with the presence of ROP [18]. A meta-analysis also showed that male sex was associated with an increased risk of severe ROP [19]. We considered that males may not only be more prone to ROP or severe ROP but also have poorer visual outcomes following ROP treatment than females. However, the reason for the worse visual prognosis in male patients was unclear. Several studies showed that male sex was associated with adverse outcomes of prematurity, such as intraventricular haemorrhage, and periventricular leukomalacia [19,20,21]. We speculate that these neurologic complications might affect visual outcomes.
In this study, older children had significantly less amblyopia in all zone analyses and in the zone II analysis. Several studies investigated the prevalence of amblyopia in children, and reported that the prevalence of amblyopia tended to decrease with increasing age [22, 23]. We speculated that younger children are more likely to be over diagnosed with amblyopia. As age increases, the diagnosis of amblyopia may be modified to not be amblyopia, and accordingly, the prevalence of amblyopia might decrease with ageing. In this study, older children had a significantly lower SE in zone I ROP. Yotsukura et al. [24] investigated the prevalence of myopia in children, and they reported that it increased with age, which is consistent with our results.
In this study, eyes with zone I stage 1 ROP had significantly worse BCVA than eyes with zone I stage 2 or 3, or AROP. We speculated that eyes treated for zone I stage 1 ROP might be more rapidly progressive or have more severe plus disease than those treated for zone I stage 2 or 3 ROP. It might be contributed worse BCVA in eyes treated for zone I stage 1 ROP than those treated for zone I stage 2 or 3 ROP. The reason why BCVA was better in eyes with zone I AROP than in eyes with zone I stage 1 ROP was unclear. Gschließer et al. reported that the level of inter-expert agreement of diagnosis of stage or aggressive posterior ROP was not high [25]. These incomplete inter-expert agreements of diagnosis might attribute these results.
The limitations of this study include that it was a retrospective, non-randomised study. We used multivariable methods to estimate the association between the long-term visual outcome and treatment procedure after adjusting for the impact of confounding factors such as birth characteristics and ROP features. However, there may have been treatment choice biases that only a prospective randomised controlled trial could address. The treatment criteria were unclear due to the retrospective design. Among the ten facilities, some were in urban areas, and some were in rural areas, which may have influenced the treatment strategy. For instance, in one institution in a rural area, all eyes initially treated with anti-VEGF therapy underwent laser photocoagulation before hospital discharge to reduce hospital visits after discharge. This delayed laser therapy may have influenced the results of this study. We have no biometry data, such as axial length, anterior chamber depth, or foveal microstructure; therefore, the reason for better outcomes for zone I ROP in the anti-VEGF group than in the laser group is unclear. Further randomised prospective studies with well-defined treatment criteria and various biometric measurements are warranted.
In conclusion, for zone I ROP, eyes treated with anti-VEGF therapy had better BCVA and a lower myopic refractive error than those treated with laser therapy, while for zone II ROP, there was no difference in treatment outcomes between the two treatments. Thus, we considered anti-VEGF therapy to be a better option than laser therapy in eyes with zone I type 1 ROP or zone I AROP.
Summary
What was known before
-
Several previous researchers compared the long-term treatment outcomes of laser photocoagulation and anti-VEGF therapy for ROP, and they reported that visual acuity did not differ between laser-treated eyes and anti-VEGF treated eyes.
-
However, no data comparing the treatment results of anti-VEGF treatment and laser therapy according to ROP zone are available.
What this study adds
-
We found that in zone I ROP, anti-VEGF therapy offered significantly better visual acuity and significantly less myopic refractive error than did laser treatment.
-
Anti-VEGF therapy may be a better treatment modality than laser therapy for zone I ROP.
Data availability
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
References
Blencowe H, Lawn JE, Vazquez T, Fielder A, Gilbert C. Preterm-associated visual impairment and estimates of retinopathy of prematurity at regional and global levels for 2010. Pediatr Res. 2013;74:35–49.
Hartnett ME, Penn JS. Mechanisms and management of retinopathy of prematurity. N Engl J Med. 2012;367:2515–26.
Hurley BR, McNamara JA, Fineman MS, Ho AC, Tasman W, Kaiser RS, et al. Laser treatment for retinopathy of prematurity: evolution in treatment technique over 15 years. Retina. 2006;26:S16–17.
Chung EJ, Kim JH, Ahn HS, Koh HJ. Combination of laser photocoagulation and intravitreal bevacizumab (Avastin) for aggressive zone I retinopathy of prematurity. Graefes Arch Clin Exp Ophthalmol. 2007;245:1727–30.
Mintz-Hittner HA, Kuffel RR Jr. Intravitreal injection of bevacizumab (avastin) for treatment of stage 3 retinopathy of prematurity in zone I or posterior zone II. Retina. 2008;28:831–8.
Mintz-Hittner HA, Kennedy KA, Chuang AZ. Efficacy of intravitreal bevacizumab for stage 3+ retinopathy of prematurity. N Engl J Med. 2011;364:603–15.
Stahl A, Lepore D, Fielder A, Fleck B, Reynolds JD, Chiang MF, et al. Ranibizumab versus laser therapy for the treatment of very low birthweight infants with retinopathy of prematurity (RAINBOW): an open-label randomised controlled trial. Lancet. 2019;394:1551–9.
Murakami T, Sugiura Y, Okamoto F, Okamoto Y, Kato A, Hoshi S, et al. Comparison of 5-year safety and efficacy of laser photocoagulation and intravitreal bevacizumab injection in retinopathy of prematurity. Graefes Arch Clin Exp Ophthalmol. 2021;259:2849–55.
Lee YS, See LC, Chang SH, Wang NK, Hwang YS, Lai CC, et al. Macular structures, optical components, and visual acuity in preschool children after intravitreal bevacizumab or laser treatment. Am J Ophthalmol. 2018;192:20–30.
Chen YC, Chen SN. Foveal microvasculature, refractive errors, optical biometry and their correlations in school-aged children with retinopathy of prematurity after intravitreal antivascular endothelial growth factors or laser photocoagulation. Br J Ophthalmol. 2020;104:691–6.
Zhao J, Wu Z, Lam W, Yang M, Chen L, Zheng L, et al. Comparison of OCT angiography in children with a history of intravitreal injection of ranibizumab versus laser photocoagulation for retinopathy of prematurity. Br J Ophthalmol. 2020;104:1556–60.
Deng X, Cheng Y, Zhu XM, Linghu DD, Xu H, Liang JH. Foveal structure changes in infants treated with anti-VEGF therapy or laser therapy guided by optical coherence tomography angiography for retinopathy of prematurity. Int J Ophthalmol. 2022;15:106–12.
Gundlach BS, Kokhanov A, Altendahl M, Suh SY, Fung S, Demer J, et al. Real-world visual outcomes of laser and anti-VEGF treatments for retinopathy of prematurity. Am J Ophthalmol. 2021;238:86–96.
Good WV. Final results of the Early Treatment for Retinopathy of Prematurity (ETROP) randomized trial. Trans Am Ophthalmol Soc. 2004;102:233–48.
Yonekawa Y, Wu WC, Nitulescu CE, Chan RVP, Thanos A, Thomas BJ, et al. Progressive retinal detachment in infants with retinopathy of prematurity treated with intravitreal bevacizumab or ranibizumab. Retina. 2018;38:1079–83.
Mueller B, Salchow DJ, Waffenschmidt E, Joussen AM, Schmalisch G, Czernik C, et al. Treatment of type I ROP with intravitreal bevacizumab or laser photocoagulation according to retinal zone. Br J Ophthalmol. 2017;101:365–70.
Geloneck MM, Chuang AZ, Clark WL, Hunt MG, Norman AA, Packwood EA, et al. Refractive outcomes following bevacizumab monotherapy compared with conventional laser treatment: a randomized clinical trial. JAMA Ophthalmol. 2014;132:1327–33.
Kang EY, Lien R, Wang NK, Lai CC, Chen KJ, Hwang YS, et al. Retinopathy of prematurity trends in Taiwan: a 10-year nationwide population study. Invest Ophthalmol Vis Sci. 2018;59:3599–607.
van Westering-Kroon E, Huizing MJ, Villamor-Martínez E, Villamor E. Male disadvantage in oxidative stress-associated complications of prematurity: a systematic review, meta-analysis and meta-regression. Antioxidants. 2021;10:1490.
Tioseco JA, Aly H, Essers J, Patel K, El-Mohandes AA. Male sex and intraventricular hemorrhage. Pediatr Crit Care Med. 2006;7:40–44.
Shim SY, Cho SJ, Kong KA, Park EA. Gestational age-specific sex difference in mortality and morbidities of preterm infants: a nationwide study. Sci Rep. 2017;7:6161.
Faghihi M, Hashemi H, Nabovati P, Saatchi M, Yekta A, Rafati S, et al. The prevalence of amblyopia and its determinants in a population-based study. Strabismus. 2017;25:176–83.
Chia A, Dirani M, Chan YH, Gazzard G, Au Eong KG, Selvaraj P, et al. Prevalence of amblyopia and strabismus in young singaporean chinese children. Invest Ophthalmol Vis Sci. 2010;51:3411–7.
Yotsukura E, Torii H, Inokuchi M, Tokumura M, Uchino M, Nakamura K, et al. Current prevalence of myopia and association of myopia with environmental factors among schoolchildren in Japan. JAMA Ophthalmol. 2019;137:1233–9.
Gschließer A, Stifter E, Neumayer T, Moser E, Papp A, Pircher N, et al. Inter-expert and intra-expert agreement on the diagnosis and treatment of retinopathy of prematurity. Am J Ophthalmol. 2015;160:553–60.
Author information
Authors and Affiliations
Contributions
TM: study design, acquisition of data, analysis of data, interpretation of data, drafting article, final approval of article. FO: study design, drafting article and final approval of article. TK, KS, TN, SOb, SOg, YN, HT, TJ and KU: study design, acquisition of data, critical revision of article and final approval of article. RI: study design, analysis of data, critical revision of article and final approval of article. TO: supervision, study design, critical revision of article and final approval of article.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
This study was approved by the Institutional Review Board at the Tsukuba University Hospital (Approval number: R03-081).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Murakami, T., Okamoto, F., Kinoshita, T. et al. Comparison of long-term treatment outcomes of laser and anti-VEGF therapy in retinopathy of prematurity: a multicentre study from J-CREST group. Eye 37, 3589–3595 (2023). https://doi.org/10.1038/s41433-023-02559-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-023-02559-z
- Springer Nature Limited