
Abstract
Background/objectives
We investigated if breastfeeding duration and current dietary patterns (DP) were associated with glucose and lipid metabolism biomarkers in women from the Nutritionist’s Health Study.
Subjects/methods
This is a cross-sectional analysis of 200 healthy undergraduates and nutrition graduates aged ≤45 years. Total [<6; ≥6 months] and predominant [<3; ≥3 months] breastfeeding were recalled using questionnaires. Diet were assessed using a food frequency questionnaire. DP obtained by factor analysis by principal component were categorized into tertiles of adherence (T1 = reference). Glucose and lipid biomarkers were categorized into tertiles (T1 + T2 = reference). Logistic regression was applied considering minimal sufficient adjustment recommended by directed acyclic graphs.
Results
Median (interquartile range) age and BMI were 23.0 (20.0; 28.5) years and 22.6 (20.7; 25.4) kg/m2, respectively. Mean ± SD values of glucose, LDL-c and HDL-c were 82.0 ± 9.0, 101.1 ± 29.6 and 54.4 ± 12.4 mg/dL, respectively. Women breastfed for <6 months had higher chance of being classified into T3 of insulin (OR = 2.87; 95%CI = 1.28–6.40). Predominant breastfeeding < 3 months was associated with insulin levels (OR = 2.27; 95%CI = 1.02–5.02) and HOMA-IR (OR = 2.36; 95%CI = 1.06−5.26). Breastfeeding was not associated with lipids. The Processed pattern was directly associated with LDL-c (T3: OR 6.08; 95%CI 1.80–20.58; P-trend = 0.004), while the Prudent pattern was inversely associated with LDL-c (T3: OR 0.26; 95%CI 0.08–0.87; P-trend = 0.029) and LDL-c/HDL-c ratio (T3: OR 0.28; 95%CI 0.08–0.97; P-trend = 0.046).
Conclusion
Early feeding could be a protective factor against insulin resistance development, while current DP were associated with lipid profile. This evidence indicates that from early life until early adulthood, dietary habits might influence women’s cardiometabolic risk profile.
Similar content being viewed by others


Introduction
Glucose and lipid metabolism disturbances are important risk factors for cardiovascular disease, a major public health problem worldwide [1]. Insulin resistance and increased LDL-c should be monitored to prevent cardiovascular events [2, 3]. In studies of risk factors for cardiovascular diseases, the female sex has been underrepresented, despite being recognized biological and psychosocial gender differences [4].
The impact of diet on glucose and lipid metabolism and cardiometabolic outcomes may also differ between sexes [5,6,7,8,9]. Once these abnormalities are more common after menopause [4], most studies have assessed its impact in middle-aged women [8, 10,11,12]. Considering that menopausal hormonal changes could modify the effect of diet on metabolic outcomes [13], assessment of dietary patterns at a younger age could be more appropriate to investigate whether modifiable dietary habits are associated with predictors of cardiometabolic disease, such as glucose and lipid metabolism biomarkers.
Few studies used dietary patterns approaches to evaluate this association in women during early adulthood [5, 6, 14, 15]. Dietary patterns analysis considers interaction and synergic effects of food groups and nutrients and has been recommended in nutritional epidemiology to evaluate associations with health outcomes [16, 17].
Cardiometabolic diseases programming starts early in life, especially during the first 1000 days of life [18]. A potential protective effect of breastfeeding against these diseases has been investigated. Few studies on the association of early life feeding with glucose and lipid metabolism biomarkers in adults have reported inconsistent results [19,20,21,22,23,24,25,26,27]. Evidence of breastfeeding protection against type 2 diabetes is consistent in high-income countries [25, 28, 29], but not in low- and middle-income countries [21].
Once early life diet may affect glucose and lipid metabolism, investigations in young adults are desirable to prevent cardiovascular outcomes. Our hypothesis was that longer breastfeeding as well as current adherence to healthier dietary patterns were associated with a favorable metabolic profile. By including young women, the Nutritionist’s Health Study (NutriHS) offers a unique opportunity to examine associations of breastfeeding duration and current dietary patterns with glucose and lipid biomarkers.
Subjects and methods
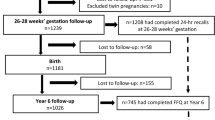
This is a sub-study of the NutriHS, which is a cohort conducted with nonpregnant undergraduates and nutrition graduates, approved by the Research Ethics Committee of the School of Public Health of the University of São Paulo, Brazil [30]. Eligibility criteria were met by 1478 participants recruited between 2014 and 2017. For the purpose of this sub-study, 101 men, 34 women >45 years, 2 with diagnosis of cancer and 10 with diabetes were excluded, resulting in 1331 women. Self-reported data were collected at baseline using electronic structured questionnaires (http://www.fsp.usp.br/nutrihs/index.html) (Fig. 1).

Flow chart of inclusion and exclusion criteria
To detect differences in proportions of glucose and lipid biomarkers categories according to exposures, with a power of 80% and a two-tailed level of significance of 5%, 124 participants were needed. A random subset of 200 participants had biomarkers levels determined. For seven participants, there was insufficient plasma sample for insulin determination (Fig. 1).
Retrospective cohort design was considered when breastfeeding was the main exposure and a cross-sectional analysis when current dietary patterns were exposures.
Before answering questionnaires about early life events, participants consulted their mothers or birth cards. Early life feeding was assessed considering total breastfeeding [<6; ≥6 months (reference)] and predominant breastfeeding, which refers to the age of introduction of formula, animal milk or solid food [<3; ≥3 months (reference)]. Birthweight and maternal characteristics, such as education level, prepregnancy body mass index (BMI), and gestational diabetes were also obtained.
Age, family income, graduation level (undergraduates attending the first half or the second half of the nutrition course; graduates/nutritionists), smoking habit, and alcohol intake were assessed. Physical activity was evaluated using the International Physical Activity Questionnaire [31] validated in Brazilians [32] and expressed as tertiles of METs from moderate to vigorous-intensity activities (first + second versus third tertile).
Dietary intake regarding the previous 12 months was assessed using a validated food frequency questionnaire [33]. Daily energy intake was estimated according to the USDA National Nutrient Database for Standard Reference [34]. Dietary patterns were identified by factor analysis by principal component as previously described [35]. The four dietary patterns (Processed, Prudent, Brazilian, and Lacto-vegetarian) together explained 27% of diet variance. The Processed pattern was characterized by high intake of salted pastries, noodles, roots/soups, fried white meat, processed and pork meat, fast-food, snacks, industrialized sauces and beverages, alcoholic beverages, and sweets. The Prudent pattern was characterized by high intake of fruits, yogurt, oats, nuts, vegetables, salad oil, salt, roots/soups, roasted white meat, beef, eggs, brown rice, lentil, whole grain bread, and tea. The Brazilian pattern was directly associated with intake of white rice, bean, processed meat, beef, salt, white bread, spreading fat, whole milk, and coffee, and inversely associated with brown rice, lentil, and nuts. The Lacto-vegetarian pattern was associated with high intake of alcoholic beverages, brown rice, whole grain bread, oats, spreading fat, cheese, and skimmed milk, and low intake of animal protein sources, salad oil, salt, and white rice. Dietary pattern scores were categorized into tertiles (first = low; second = moderate; third = high adherence), having the first as reference.
A random sub-sample of participants was invited to a face-to-face interview. Weight was measured using a digital scale with accuracy to the nearest 100 g and height using a stadiometer with 0.1 cm of precision. Fasting plasma glucose was determined by the glucose oxidase method and insulin by immunofluorimetric assay (Monobind Inc., Lake Forest, CA, USA). Insulin resistance was evaluated using homeostasis model assessment (HOMA-IR) [36]. Total cholesterol, HDL-c, and triglycerides were measured using enzymatic colorimetric method and LDL-c estimated by Friedewald formula [37]. LDL-c/HDL-c ratio was calculated. Biomarkers (outcomes) were categorized into tertiles and the first two were grouped (reference), while the highest was isolated (first + second versus third tertile) considering that our sample was within the near normal ranges.
Statistical analyses
Categorical variables were described as absolute and relative frequencies. Kolmogorov–Smirnov test was used to verify normal distribution of continuous variables, described as mean (standard deviation), or median (interquartile range).
Logistic regression was performed to estimate odds ratios (OR) and 95% confidence interval of being classified into the third tertile of biomarkers. Confounding variables were selected according to minimal sufficient adjustment sets recommended by Direct Acyclic Graphs (DAG), constructed using the Daggity software [38] (Supplementary Figs. 1 and 2). When breastfeeding was the main exposure, models were adjusted for maternal education and birthweight. Adjustment for gestational diabetes was indicated, but since only three cases were present, these were excluded (Supplementary Fig. 1). When dietary pattern was the main exposure, three models were performed: model 1 considered the four dietary patterns and energy intake; model 2 adding adjustments for age, moderate-to-vigorous physical activity, smoking habit, frequency of alcohol intake, total breastfeeding duration, and birthweight as suggested by the DAG (Supplementary Fig. 2); model 3 adding BMI to test a possible mediation effect (data not shown). Linear P-trend across tertiles of patterns was estimated. All models showed goodness-of-fit according to Hosmer-and-Lemeshow test (p value > 0.05).
Significance was considered at a level of 5%. Analyses were performed using Stata Statistical Software (release 12, 2011, StataCorp LP, College Station, TX).
Results
The sub-sample of 200 women had median values (interquartile range) of age of 23.0 (20.0; 28.5) years, BMI of 22.6 (20.7; 25.4) kg/m2 and energy intake of 9188 (7447; 11,943) kJ/day [2195 (1779; 2853) kcal/day]. Except for lower frequencies of graduates and alcohol intake in the sub-sample, other characteristics did not differ from the entire NutriHS sample (Table 1), assuring reasonable representativeness. Most participants of the sub-sample were undergraduates (96%), did not smoke nor consume alcohol and had normal BMI. Approximately 81% were born with adequate weight and a quarter was breastfed for <6 months or had predominant breastfeeding for <3 months.
Mean or median values of glucose and lipid metabolism biomarkers of the entire sample were within the normal ranges. Looking at the highest tertiles, only mean value of LDL-c (133.8 ± 21.2 mg/dL) was slightly above the recommendation (Table 2).
Women breastfed for <6 months had a higher chance to be classified into the third tertile of insulin (OR = 2.87; 95%CI 1.28; 6.40). Predominant breastfeeding <3 months was also associated with insulin levels (OR = 2.27; 95%CI 1.02; 5.02) and HOMA-IR (OR = 2.36; 95%CI 1.06; 5.26). Birthweight showed to be a confounder on these associations, since macrosomia was directly associated with insulin levels and HOMA-IR. Breastfeeding was not associated with lipid biomarkers. Maternal education <11 years was inversely associated with the offspring’s HDL-c during adult life (Table 3).
Table 4 shows associations between three major dietary patterns identified and metabolic biomarkers, considering adjustment for variables of current and early life (model 2). Significant association of total breastfeeding duration with insulin was maintained independently of current dietary patterns (OR = 4.18; P = 0.003). Considering predominant breastfeeding duration instead of total breastfeeding, its association with HOMA-IR was also maintained (OR = 2.57; P = 0.038). The Processed pattern was directly associated with LDL-c (P-trend = 0.004) and participants with moderate adherence to this pattern had a higher chance to be classified into the third tertile of plasma glucose (P = 0.007) and LDL-c/HDL-c ratio (P = 0.032), although a linear trend was not found. The Prudent pattern was associated with a lower chance of classification into the highest tertiles of LDL-c (P-trend = 0.029) and LDL-c/HDL-c ratio (P-trend = 0.046). Participants with moderate adherence to the Prudent pattern had a lower chance to be classified into the third tertile of triglyceridemia (P = 0.043) and plasma glucose (P = 0.033), but such associations were not dose-response since were not significant for those with the highest adherence. Participants with moderate adherence to the Brazilian pattern had a lower chance to be classified into the highest tertile of LDL-c (P = 0.003; P-trend = 0.326), while high adherence to this pattern seemed to be directly associated with insulin levels (P-trend = 0.005) and HOMA-IR (P-trend = 0.003) (Table 4). The Lacto-vegetarian pattern had the lowest explained variance (not shown in table); this was associated with HDL-c (T3: OR = 0.36; 95%CI = 0.13; 0.97; P-trend = 0.044) and LDL-c/HDL-c ratio (T3: OR = 3.82; 95%CI = 1.27; 11.49; P-trend = 0.017). BMI was not considered a mediating factor, since its inclusion in the model 2 did not change any effect size (OR changed <10%) and the statistical significance was maintained (except for the association between moderate adherence to the Prudent pattern and triglycerides).
Discussion
In this study of young women, both early feeding and current dietary patterns were associated with glucose and lipid metabolism biomarkers. A relevant aspect was to focus on the female sex that has been less investigated in literature. The inverse association of longer breastfeeding with insulin levels and HOMA-IR suggests that breastfeeding could exert a protective effect against insulin resistance later in life. High adherences to the Prudent and Processed patterns in adulthood were inversely and directly associated with an unfavorable lipid profile, respectively. This indicates that dietary habits since early life until present time might influence the cardiometabolic risk profile of young women even when their biomarkers are still within the near normal ranges.
Women who had shorter breastfeeding exhibited a higher chance of higher insulin levels and HOMA-IR, which could be interpreted as decreased insulin sensitivity. Plasma glucose of our participants was unable to differentiate subsets according to the breastfeeding duration. These findings are in line with a meta-analysis, which reported that breastfed infants showed lower insulin levels and lower chance of type 2 diabetes later in life, but mean glucose was not different from bottle-fed subjects [28]. Our study was also in agreement with others involving adolescents, in which exclusive breastfeeding in the first 3 months of life was inversely associated with insulin levels and HOMA-IR but not with plasma glucose [39], or adults from developed [20] and middle-income countries [21]. Middle-aged participants of the Dutch Famine Cohort, who were exclusively breastfed before leaving the maternity hospital, showed lower fasting glucose, insulin and proinsulin levels compared to those who were bottle-fed [19]. As far as we know, few studies have investigated associations of breastfeeding duration with biomarkers of glucose metabolism or diabetes incidence in healthy adults, and inconsistent results have been reported [24, 29].
Our suggestion of a protective role of longer breastfeeding duration against insulin resistance has biological plausibility. Human milk has lower energy and protein content than conventional formulas, which could contribute to lower insulin like growth factor-1 concentration and prevent accelerated growth during childhood, known to be associated with metabolic diseases later in life [40, 41]. Also, human milk contains hormones involved in energy balance and insulin sensitivity, such as leptin and adiponectin [42]. In addition to breastfeeding, intra-utero conditions—reflected by the birthweight—may be also important for associations of glucose metabolism disturbances in adulthood.
The lack of association between breastfeeding and lipid biomarkers in our study agrees with previous studies [24, 25, 27], but differs from others [19, 26]. Another possible link between breastfeeding and metabolic disturbances in adulthood could be dietary habits [35, 43], which in turn were associated with glucose and lipid biomarkers [5,6,7,8, 44]. Our group previously reported an association of breastfeeding duration with adherence to the Prudent pattern [35]. We verified that although both breastfeeding and current dietary patterns were associated with glucose and lipid biomarkers, it seemed to affect preferentially one or another metabolic pathway. We speculate that early feeding could be associated with the development of glucose metabolism disturbance, while current diet could be associated with abnormal lipid profile.
It is important to emphasize that although the Brazilian pattern has been directly associated with insulin levels and HOMA-IR in our fully adjusted models (Model 2), confidence intervals seemed to be affected considering all the confounders. Thus, these results should be interpreted with caution, considering that not seem to be accurate; and that the Brazilian diet was previously inversely associated with cardiometabolic risk factors [5].
We verified that our Prudent pattern was inversely associated with LDL-c and LDL-c/HDL-c ratio, thus indicating a favorable lipid profile. On the other hand, adherence to the Processed pattern was directly associated with LDL-c. Although our cross-section design does not allow inferring causality, these significant associations in young women, without cardiometabolic diseases, are suggestive of a role of diet in lipid profile. As the FFQ used refers to the previous year consumption, bias of reversal causality is less likely. Considering that dietary habits are modifiable in face of nutritional counselling, we highlight the relevance of monitoring lipid biomarkers before middle age, when preventive measure could be more effective.
In our study, most participants and their mothers before pregnancy had normal BMI and the association of dietary patterns with glucose and lipid biomarkers did not seem to be BMI-mediated. We speculate that the role of BMI as a mediating factor could be different in samples composed of older participants and with higher prevalence of obesity and comorbidities. Evidences suggest that maternal adiposity could contribute to explain the inter-generational transmission of obesity [45, 46]. Previous findings of the NutriHS showed positive association between maternal prepregnancy BMI and DXA-determined general and central adiposity measures of their daughters during adulthood (unpublished data), which could deteriorate the cardiometabolic profile later in life. Without disregarding a genetic component, we suggest that environmental factors should be contributing to explain these associations. We previously reported that maternal prepregnancy BMI was also associated with offspring’s adherence to the Prudent and Processed patterns [35]. Thus, we reinforce the importance of obesity prevention before conception in attempt to minimize a vicious cycle of body weight accumulation and its comorbidities.
In agreement with our results, in young Finnish women, a health-conscious pattern similar to our Prudent pattern, was inversely associated with total cholesterol and LDL-c and this was unaffected by BMI adjustment [14]. In the same study, a pattern characterized by traditional foods (sausage, pork meat, and potatoes) also present in our Processed pattern, was directly associated with LDL-c, as in ours, and with insulin levels. It is important highlight that dietary patterns differ according to socioeconomic and cultural characteristics and might not be reproducible among different populations [17]. To the best of our knowledge, in young Brazilian women, only one study previously examined dietary patterns and its association with metabolic biomarkers. In line with our results, the Common-Brazilian pattern was inversely associated with LDL-c, and also with other lipid particles [5].
Our Prudent pattern resembles the Dietary Approach to Stop Hypertension, which has been inversely associated with cardiovascular risk [15, 47]. High intakes of fruits, vegetables, nuts, and whole grains in these patterns should have contributed to high dietary fiber and phytochemicals contents, known to be beneficial to risk factors such as LDL-c [48]. On the other hand, a combination of unhealthier dietary habits in our Processed pattern (high intake of processed meats, simple carbohydrates, fried foods and alcoholic beverages) could explain to the deleterious association found [49].
A strength of our study refers to peculiarities of participants, who had nutrition knowledge to manage tools to assess diet and may be conscious about the relevance of providing good quality data, enhancing chances of reliable answers. On the other hand, the specificity of our sample of highly educated young women does not allow us to generalize our findings to samples with different characteristics. The use of DAGs was also strength, since it minimizes insufficient or over adjustments [38]. As far as we know, no previous study used DAG to investigate associations of early and current dietary habits with metabolic outcomes.
A limitation of this study refers to the cross-sectional design, which makes it impossible to assess temporality and causality. Regarding the association between early feeding and biomarkers, the retrospective cohort design could imply in recall bias of breastfeeding duration, which could represent a limitation of our study. Nonetheless, it was reported that breastfeeding duration can be accurately recalled 20 years later [50].
Conclusions
Both early feeding and current dietary habits were associated with biomarkers of glucose and lipid metabolism of young women, suggesting that they could influence risk of metabolic disturbances. It is possible that longer breastfeeding may confer protection against insulin resistance in adult life. Eating habits were associated with lipid profile even in young and healthy women. Further investigations with prospective design in early adulthood are needed.
References
WHO. Global status report on noncommunicable diseases. Geneva: WHO Library Cataloguing-in-Publication Data; 2014.
Pirillo A, Bonacina F, Norata GD, Catapano AL. The interplay of lipids, lipoproteins, and immunity in atherosclerosis. Curr Atheroscler Rep. 2018;20:12.
Bonora E, Formentini G, Calcaterra F, Lombardi S, Marini F, Zenari L, et al. HOMA-estimated insulin resistance is an independent predictor of cardiovascular disease in type 2 diabetic subjects: prospective data from the verona diabetes complications study. Diabetes Care. 2002;25:1135–41.
Maas AH, van der Schouw YT, Regitz-Zagrosek V, Swahn E, Appelman YE, Pasterkamp G, et al. Red alert for women’s heart: the urgent need for more research and knowledge on cardiovascular disease in women: proceedings of the workshop held in Brussels on gender differences in cardiovascular disease, 29 September 2010. Eur Heart J. 2011;32:1362–8.
Olinto MT, Gigante DP, Horta B, Silveira V, Oliveira I, Willett W. Major dietary patterns and cardiovascular risk factors among young Brazilian adults. Eur J Nutr. 2012;51:281–91.
Pimenta AM, Toledo E, Rodriguez-Diez MC, Gea A, Lopez-Iracheta R, Shivappa N, et al. Dietary indexes, food patterns and incidence of metabolic syndrome in a Mediterranean cohort: The SUN project. Clin Nutr. 2015;34:508–14.
Xu SH, Qiao N, Huang JJ, Sun CM, Cui Y, Tian SS, et al. Gender differences in dietary patterns and their association with the prevalence of metabolic syndrome among Chinese: a cross-sectional study. Nutrients. 2016;8:180.
Lee J, Kim J. Association between dietary pattern and incidence of cholesterolemia in Korean Adults: the korean genome and epidemiology study. Nutrients 2018;10:1.
Nanri A, Mizoue T, Yoshida D, Takahashi R, Takayanagi R. Dietary patterns and A1C in Japanese men and women. Diabetes Care. 2008;31:1568–73.
Ruiz-Cabello P, Coll-Risco I, Acosta-Manzano P, Borges-Cosic M, Gallo-Vallejo FJ, Aranda P, et al. Influence of the degree of adherence to the Mediterranean diet on the cardiometabolic risk in peri and menopausal women. The Flamenco project. Nutr Metab Cardiovasc Dis. 2017;27:217–24.
AlEssa HB, Malik VS, Yuan C, Willett WC, Huang T, Hu FB, et al. Dietary patterns and cardiometabolic and endocrine plasma biomarkers in US women. Am J Clin Nutr. 2017;105:432–41.
Kang SH, Cho KH, Do JY. Association between the modified dietary approaches to stop hypertension and metabolic syndrome in postmenopausal women without diabetes. Metab Syndr Relat Disord. 2018;16:282–9.
Cho YA, Kim J, Cho ER, Shin A. Dietary patterns and the prevalence of metabolic syndrome in Korean women. Nutr Metab Cardiovasc Dis. 2011;21:893–900.
Mikkilä V, Räsänen L, Raitakari OT, Marniemi J, Pietinen P, Rönnemaa T, et al. Major dietary patterns and cardiovascular risk factors from childhood to adulthood. The Cardiovascular Risk in Young Finns Study. Br J Nutr. 2007;98:218–25.
Saneei P, Fallahi E, Barak F, Ghasemifard N, Keshteli AH, Yazdannik AR, et al. Adherence to the DASH diet and prevalence of the metabolic syndrome among Iranian women. Eur J Nutr 2015;54:421–8.
Wirfält E, Drake I, Wallström P. What do review papers conclude about food and dietary patterns? Food Nutr Res. 2013;57. https://doi.org/10.3402/fnr.v57i0.20523. (Published online).
Hu FB. Dietary pattern analysis: a new direction in nutritional epidemiology. Curr Opin Lipidol 2002;13:3–9.
Gluckman PD, Cutfield W, Hofman P, Hanson MA. The fetal, neonatal, and infant environments-the long-term consequences for disease risk. Early Hum Dev. 2005;81:51–9.
Ravelli AC, van der Meulen JH, Osmond C, Barker DJ, Bleker OP. Infant feeding and adult glucose tolerance, lipid profile, blood pressure, and obesity. Arch Dis Child. 2000;82:248–52.
Parikh NI, Hwang SJ, Ingelsson E, Benjamin EJ, Fox CS, Vasan RS, et al. Breastfeeding in infancy and adult cardiovascular disease risk factors. Am J Med. 2009;122:656–63.e1.
Fall CH, Borja JB, Osmond C, Richter L, Bhargava SK, Martorell R, et al. Infant-feeding patterns and cardiovascular risk factors in young adulthood: data from five cohorts in low- and middle-income countries. Int J Epidemiol. 2011;40:47–62.
Owen CG, Whincup PH, Cook DG. Breast-feeding and cardiovascular risk factors and outcomes in later life: evidence from epidemiological studies. Proc Nutr Soc. 2011;70:478–84.
Kelishadi R, Farajian S. The protective effects of breastfeeding on chronic non-communicable diseases in adulthood: a review of evidence. Adv Biomed Res. 2014;3:3.
Pirilä S, Taskinen M, Viljakainen H, Mäkitie O, Kajosaari M, Saarinen-Pihkala UM, et al. Breast-fed infants and their later cardiovascular health: a prospective study from birth to age 32 years. Br J Nutr. 2014;111:1069–76.
Horta BL, Loret de Mola C, Victora CG. Long-term consequences of breastfeeding on cholesterol, obesity, systolic blood pressure and type 2 diabetes: a systematic review and meta-analysis. Acta Paediatr. 2015;104:30–7.
Owen CG, Whincup PH, Kaye SJ, Martin RM, Davey Smith G, Cook DG, et al. Does initial breastfeeding lead to lower blood cholesterol in adult life? A quantitative review of the evidence. Am J Clin Nutr. 2008;88:305–14.
Hayosh O, Mandel D, Mimouni FB, Lahat S, Marom R, Lubetzky R. Prolonged duration of breastfeeding does not affect lipid profile in adulthood. Breastfeed Med. 2015;10:218–21.
Owen CG, Martin RM, Whincup PH, Smith GD, Cook DG. Does breastfeeding influence risk of type 2 diabetes in later life? A quantitative analysis of published evidence. Am J Clin Nutr. 2006;84:1043–54.
Al Mamun A, O’Callaghan MJ, Williams GM, Najman JM, Callaway L, McIntyre HD. Breastfeeding is protective to diabetes risk in young adults: a longitudinal study. Acta Diabetol 2015;52:837–44.
Folchetti LG, Silva IT, Almeida-Pititto B, Ferreira SR. Nutritionists’ Health Study cohort: a web-based approach of life events, habits and health outcomes. BMJ Open. 2016;6:e012081.
Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35:1381–95.
Matsudo S, Araújo T, Matsudo V, Andrade D, Andrade E, Oliveira L, et al. Questionario Internacional de Atividade Física (IPAQ): estudo de validade e reprodutibilidade no Brasil. Ativ Fis e Saúde 2001;6:5–18.
Selem SS, Carvalho AM, Verly-Junior E, Carlos JV, Teixeira JA, Marchioni DM, et al. Validity and reproducibility of a food frequency questionnaire for adults of São Paulo, Brazil. Rev Bras. Epidemiol 2014;17:852–9.
USDA. National Nutrient Database for Standard Reference, Release 28 (online). Basic Report, Nutrient data for 11114, Cabbage, savoy, raw. United States Department of Agriculture, Agricultural Research Service; 2016.
Eshriqui I, Folchetti LD, Valente AMM, de Almeida-Pititto B, Ferreira SRG. Breastfeeding duration is associated with offspring’s adherence to prudent dietary pattern in adulthood: results from the Nutritionist’s Health Study. J Dev Orig Health Dis. 2019:1–10. https://doi.org/10.1017/S204017441900031X. (Published online).
Matthews DR, Hosker JP, Rudenski AS, Naylor BA, Treacher DF, Turner RC. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985;28:412–9.
Friedewald WT, Levy RI, Fredrickson DS. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem. 1972;18:499–502.
Textor J, Hardt J, Knüppel S. DAGitty: a graphical tool for analyzing causal diagrams. Epidemiology 2011;22:745.
Hui LL, Kwok MK, Nelson EAS, Lee SL, Leung GM, Schooling CM. The association of breastfeeding with insulin resistance at 17 years: Prospective observations from Hong Kong’s “Children of 1997” birth cohort. Matern Child Nutr. 2018;14:e12490. https://doi.org/10.1111/mcn.12490. (Published online).
Singhal A, Lucas A. Early origins of cardiovascular disease: is there a unifying hypothesis? Lancet 2004;363:1642–5.
Wang X, Xing KH, Qi J, Guan Y, Zhang J. Analysis of the relationship of insulin-like growth factor-1 to the growth velocity and feeding of healthy infants. Growth Horm IGF Res. 2013;23:215–9.
Savino F, Liguori SA, Sorrenti M, Fissore MF, Oggero R. Breast milk hormones and regulation of glucose homeostasis. Int J Pediatr. 2011;2011:803985.
Robinson S, Ntani G, Simmonds S, Syddall H, Dennison E, Sayer AA, et al. Type of milk feeding in infancy and health behaviours in adult life: findings from the Hertfordshire Cohort Study. Br J Nutr. 2013;109:1114–22.
Choi JH, Woo HD, Lee JH, Kim J. Dietary patterns and risk for metabolic syndrome in korean women: a cross-sectional study. Med (Baltim). 2015;94:e1424.
Paliy O, Piyathilake CJ, Kozyrskyj A, Celep G, Marotta F, Rastmanesh R. Excess body weight during pregnancy and offspring obesity: potential mechanisms. Nutrition. 2014;30:245–51.
Tan HC, Roberts J, Catov J, Krishnamurthy R, Shypailo R, Bacha F. Mother’s pre-pregnancy BMI is an important determinant of adverse cardiometabolic risk in childhood. Pediatr Diabetes. 2015;16:419–26.
Siervo M, Lara J, Chowdhury S, Ashor A, Oggioni C, Mathers JC. Effects of the dietary approach to stop hypertension (DASH) diet on cardiovascular risk factors: a systematic review and meta-analysis. Br J Nutr. 2015;113:1–15.
Anderson JW, Hanna TJ. Impact of nondigestible carbohydrates on serum lipoproteins and risk for cardiovascular disease. J Nutr. 1999;129 Suppl 7:1457S–66S.
Gershuni VM. Saturated fat: part of a healthy diet. Curr Nutr Rep. 2018;7:85–96.
Natland ST, Andersen LF, Nilsen TI, Forsmo S, Jacobsen GW. Maternal recall of breastfeeding duration twenty years after delivery. BMC Med Res Methodol. 2012;12:179.
Acknowledgements
We thank NutriHS research team and participants, who were committed to collect and provide, respectively, good quality data.
Funding
This work was supported by the São Paulo Foundation for Research Support—FAPESP, Brazil, which played no role in the study design; data collection; analysis or interpretation of data; or in drafting the manuscript.
Author information
Authors and Affiliations
Contributions
Conception and design of the study: SRGF and BAP. Collection of data: LDF, BAP, AMMV, IE, and SRGF. Data analysis and interpretation: IE and SRGF. Drafting of the manuscript: IE and SRGF. Revision of the manuscript: IE, SRGF, BAP, AMMV and LDF. Approval of the final version of the manuscript: IE, SRGF, BAP, AMMV and LDF.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
41430_2019_516_MOESM1_ESM.docx
Suplementary Figure 1. Directed Acyclic Graph (DAG) for the association between breastfeeding and glucose and lipid metabolism biomarkers
41430_2019_516_MOESM2_ESM.docx
Suplementary Figure 2. Directed Acyclic Graph (DAG) for the association between dietary patterns and glucose and lipid metabolism biomarkers
Rights and permissions
About this article

Cite this article
Eshriqui, I., Folchetti, L.D., Valente, A.M.M. et al. Early life feeding and current dietary patterns are associated with biomarkers of glucose and lipid metabolism in young women from the Nutritionist’s Health Study. Eur J Clin Nutr 74, 509–517 (2020). https://doi.org/10.1038/s41430-019-0516-8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41430-019-0516-8
- Springer Nature Limited