
Abstract
Background
Socioeconomic deprivation has been associated with lower breast cancer (BC) survival, but the influence of stage at diagnosis on this association merits further study. Our aim was to investigate this association using the Loire-Atlantique/Vendee Cancer Registry (France).
Methods
Twelve-thousand seven-hundred thirty-eight women living in the area covered by the registry and diagnosed with invasive breast carcinoma between 2008 and 2015 were included in the study. They were censored at maximal 6 years. Deprivation was measured by the French European Deprivation Index. Excess hazard and net survival were estimated for deprivation level, stage and age at diagnosis using a flexible excess mortality hazard model.
Results
After adjustment by stage, women living in the most deprived areas had a borderline non-significant higher excess mortality hazard (+25% (95% CI: −3%; +62%)) compared to those living in the least deprived areas. Stage-adjusted 5-year net survival differed significantly between these two subgroups (respectively, 88.2% (95% CI:85.2%-90.5%) and 92.5% (95% CI:90.6%-93.9%)).
Conclusion
BC survival remained lower in deprived areas in France, despite universal access to cancer care. Intensification of prevention measures could help to reduce advanced BC, responsible for the majority of deaths from BC. A better understanding of remaining social disparities is crucial to implement specific interventions.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
The reduction of social inequalities in health is a political objective in many countries. In France, tackling socioeconomic and territorial inequalities is one of the priorities of the 10-year cancer control strategy 2021–2030 and was previously a priority of the 2014–2019 National Cancer Plan [1, 2].
Breast cancer (BC) remains by far the most common cancer and the leading cause of death from cancer in women, globally and in France [3, 4].
Survival, a key measurement of the overall effectiveness of healthcare systems in cancer management, is fortunately increasing for most cancer sites in all countries [5, 6]. The breast is one of the cancer sites with the best prognosis, 88% at 5 years in France [7]. However it has been previously reported that affluent populations have a higher incidence rate of BC while women living in more deprived areas have a higher burden of BC mortality [8,9,10]. This paradox could in part reflect differences in exposure to BC risk factors and in the use of the health system for cancer diagnosis/screening and treatment [11,12,13]. When studying the impact of socioeconomic position on survival, it is crucial to account for other factors that are likely to be associated with deprivation and survival. In particular, it is necessary to determine whether or not the observed survival differences according to socioeconomic position are fully explained by such factors.
Stage at diagnosis is a major determinant of cancer survival and influences the choice of treatments offered [14, 15]. It was previously shown that in women with a low socioeconomic position or living in deprived areas, the disease had more frequently spread at diagnosis and survival rates were lower [10, 16,17,18,19,20,21,22,23,24,25,26,27,28]. In these previous studies, a population-based registry design was preferentially chosen to examine the relationship between BC survival, socioeconomic status and stage taking advantage of the exhaustive records of all cancer cases. However, some of these studies used old data, mainly recorded in the 90’s and early 2000’s [10, 16,17,18,19,20, 26]. Moreover, age-related inclusion criteria were sometimes applied, in addition to statistical methods with limitations, for instance the use of overall survival instead of net survival [10, 16,17,18, 21]. As the link between BC survival, stage and socioeconomic deprivation may vary according to country and health system, further investigations are needed to better understand this relationship, especially in France, which has a universal health coverage system.
In France, individual socioeconomic characteristics are not available in cancer registries but the contextual socioeconomic environment of patients can be approximated by ecological deprivation indices such as the French version of the European Deprivation Index (F-EDI) [29]. From the substantial database of the French Network of Cancer Registries (FRANCIM), Poiseuil et al. recently demonstrated a significant association between social deprivation and overall BC survival using an original non-parametric approach in line with another French study [30, 31]. The main weakness of these studies was the lack of principal prognostic factors, especially stage at diagnosis.
Thus, the aim of our study was to investigate BC survival according to socioeconomic environment taking into account stage at diagnosis and using a recent novel approach (flexible excess mortality hazard models) and data from a large French population-based cancer registry.
Materials and methods
Study population
The 13,151 adult (≥18 years) women newly diagnosed with primary invasive breast carcinoma (lymphoma and sarcoma excluded) between 2008 and 2015, living in Loire-Atlantique and Vendee (French departments) at diagnosis were eligible for this study.
Eligible cases were identified from Loire-Atlantique/Vendee Cancer Registry, with the following International Classification of Diseases for Oncology third edition (ICD-O-3) topography codes (C50.X) and malignant morphology codes (M8000-8575, 8980, 8982, 8983) with the exception of mammary Paget disease alone (M8540) (see Supplementary Material for the detailed list of exclusion codes).
Loire-Atlantique/Vendee Cancer Registry registers all the incident cancer cases occurring in these two departments from different sources including cytopathology laboratories, the medical information departments of public and private hospitals, the regional cancer network, health insurance organisation departments and general and specialist practitioners. Owing to regulatory constraints, French Cancer Registries do not record incident cases that are notified by death certificates only. The data quality and completeness of the Cancer Registry are certified every 5 years by the national Registries Evaluation Committee (CER). The last certification was obtained on 01/01/2021 for 5 years.
Loire-Atlantique (1.4 million of inhabitants in 2019) and Vendée (685,000 inhabitants in 2019) are two metropolitan French Departments, in western France, with the population in Vendée being more rural and older than in Loire-Atlantique. Nantes (319,000 inhabitants in 2019), located in Loire-Atlantique, is the biggest urban city of the area and the sixth largest city in France. These two departments are affluent (see Supplementary Material for more information about these two areas).
Follow-up
An active search for vital status on 30 June 2018 was carried out for all cases. The information was collected via the French national civil registration file (RNIPP).
The endpoint was 5-year survival, calculated as the difference between the date of BC diagnosis and the date of death or the last date that the patient was known to be alive.
Data collection
In addition to data routinely collected in Loire-Atlantique/Vendee Cancer Registry, extensive information was collected from medical records: mode of detection, tumour characteristics at diagnosis (clinical and pathological TNM stages, Scarff-Bloom-Richardson (SBR) grade, oestrogen (ER) and progesterone (PR) receptor status, human epidermal growth factor receptor-2 (HER2) status) and therapeutic management. According to the 7th TNM classification for malignant tumours, stage at diagnosis was defined from the pathological stage if surgery was the first treatment or from clinical stage in the case of neoadjuvant or non-surgical treatment [32].
The socioeconomic environment of patients was assessed using the F-EDI based on the 2011 national census. Ten components best reflecting individual deprivation are included in the calculation of the F-EDI score: overcrowding, no access to a system of central or electric heating, non-owner, unemployment, foreign nationality, no access to a car, unskilled worker or farmer worker, household with 6 or more persons, low level of education and single parent education [29]. An F-EDI score is assigned to each IRIS (“Ilots Regroupés pour l’Information Statistique”), the smallest geographic unit for which census data are available (on average 2,000 individuals with relatively homogeneous social characteristics) [29, 33]. The categorical version (national quintiles) of the F-EDI was used, from Quintile 1 corresponding to the most affluent IRIS to Quintile 5 corresponding to the most deprived IRIS. For each recorded BC case, the patient’s’ residential address at time of diagnosis was geocoded using Geographic Information Systems (ArcGIS 10.2, ESRI Redlands, California, USA) and allocated to an IRIS. Hence, a F-EDI quintile was attributed to each BC case by the ERISC/MapInMed platform (French national methodological platform for the study and reduction of health social inequalities in oncology) [34].
Ethical statement
The Loire-Atlantique/Vendee Cancer Registry is approved by the French National Commission for Information Technologies and Liberties (CNIL) for the collection of nominal data on cancer patients without informed consent, for research purposes and in the strictest confidentiality. However, each cancer patient living in the geographic area covered by the registry is informed that their data may be recorded in the registry database and that they can oppose this registration. Only fully anonymized data are published.
Statistical analysis
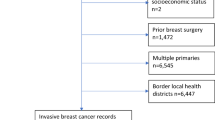
A total of 12,738 patients (96.9% of those eligible were included in the analyses (Fig. 1, flow chart).

Flow chart.
Analyses were conducted within the excess mortality framework [35]. The excess mortality hazard is the mortality directly or indirectly due to cancer. It is obtained by subtracting the expected mortality derived from general population life tables (produced by French national institute of statistics and economics studies and stratified by age, sex, calendar year and French department), from the observed mortality in the registry, relying on the assumption that BC represents a small part of overall mortality.
The excess mortality hazard according to age (as continuous variable), F-EDI quintile (as categorical variable), stage (as categorical variable) and time (as continuous variable) was estimated using flexible parametric excess mortality models and a multidimensional penalised splines approach [36, 37]. Firstly, time and age dependence was examined separately for F-EDI quintiles and stage (AIC comparisons). The proportional excess hazards assumption for F-EDI quintiles appeared reasonable. A constant relative effect of deprivation on mortality over time, regardless of age, was applied. Conversely, the effect of stage was strongly time and age dependent (non-proportional excess hazard), i.e., the relative effect of stage varied according to time since diagnosis and age at diagnosis. Thus, we incorporated flexible functions to account for the time and age dependence of stage within the final excess mortality model. From the excess mortality models, it is possible to estimate specific excess hazard and net survival for each combination of age, stage and/or deprivation. In the Results section, we plotted these two indicators as a function of time since diagnosis for the whole cohort and for five different age at diagnosis, stratified by F-EDI quintile and/or stage.
The adjustment on additional prognostic factors was not feasible because of the complexity of the estimation procedure [36]. However, we performed stratified analyses by each factor (SBR grade, hormonal profile, initial treatment, mode of detection) to study the consistency of the relation between stage-adjusted survival and deprivation.
For these analyses, follow-up was censored at 6 years. We retained 1 year of follow-up beyond 5 years in order to stabilise the 5-year estimates of excess mortality rates, as recommended for the used models [36].
Fisher exact tests and Student tests were used to compare patients according to sociodemographic and tumour characteristics.
All analyses were carried out using the statistical software R version 3.6.1 (survPen Package, [38]).
Results
A total of 12,738 women with BC were included in the study. Median age at diagnosis was 61 years (range: 22–99). Of these, 1,742 (13.7%) died during the follow-up period. When compared to women living in the most affluent areas (Quintile 1), women with a higher level of deprivation were older, and their cancer was more advanced and was detected more frequently by clinical signs than by screening. Surgery was the first treatment offered in 84.1% of cases, and less frequent in the elderly (81% in the >75 y/o vs. 98% in the <50 y/o and 97% in the 50–74 y/o, data not shown). There was no significant difference in the distribution of SBR grade and phenotypic subtype according to the deprivation level (Table 1).
A significant gradient of deprivation was detected in relation to BC survival before adjustment for stage at diagnosis (Table 2). Compared to women living in the most affluent areas (Quintile 1), those living in the most deprived areas (Quintile 5) had a 60% (95% CI: 22%–109%) higher excess mortality hazard. In other words, as the effect of deprivation was non-time-dependent and non-age-dependent (see Methods), excess mortality was 60% higher for Quintile 5 than Quintile 1, regardless of age and follow-up time (Supplementary Fig. 2A). Consequently, significant differences in net survival were observed according to deprivation level. For example, for 50-year-old women, the 5-year net survival was 94.5% (95% CI: 93.5%–95.3%) and 91.3% (95% CI: 89.1%–93.1%), respectively, in Quintile 1 and Quintile 5 (Supplementary Fig. 3A). Overall, the 5-year net survival was 92.8% (95% CI: 91.2%–94.1%) for Quintile 1 vs. 87.6% (95% CI: 84.2%–90.3%) for Quintile 5 (Table 2).
Stage at diagnosis had a strong effect on BC survival. For all ages and at any follow-up time, excess mortality increased with stage (Supplementary Fig. 2B). The magnitude of this effect was most pronounced in older patients (≥70 year old) with metastatic cancer (stage IV). In addition, middle-aged women had a lower excess mortality hazard than the youngest women for stage I–III. Therefore, 5-year net survival was slightly better in 60 year-old than in 40 year-old women; for instance, 94.4% (95% CI: 93.3%–95.4%) vs 93.0% (95% CI: 91.3%–94.4%) for stage II (Supplementary Fig. 3B). Moreover, the time of the highest excess hazard differed according to age and stage (Supplementary Fig. 2B). For non-metastatic BC, the hazard stabilised at its maximum value at around 2–3 years after diagnosis regardless of age whereas age had a strong influence in stage IV cancer. For patients over 60 years of age, the highest level of excess mortality was observed just after diagnosis while in the youngest patients this occurred during the third year following the BC diagnosis.
The effect of deprivation on survival was clearly attenuated after adjustment for stage at diagnosis, and did not reach the significance threshold (Table 2). The most deprived patients had a 25% (95% CI: −3%; +62%) higher excess mortality hazard compared to the most affluent patients, leading to significant 5-year net survival differences (respectively, in these two subgroups 88.2% (95% CI: 85.2%–90.5%) and 92.5% (95% CI: 90.6%–93.9%)).
Figure 2 shows the age-specific representation of the excess hazard by stage at diagnosis over time for the two extreme deprivation quintiles (Quintile 1 and Quintile 5) while Supplementary Fig. 4 gives the associated net survival. These representations were very similar to those presented solely by stage (Supplementary Fig. 2B). Indeed, when the deprivation level increased, excess mortality rose but the dynamic form of the excess hazard remained stable over time for each stage regardless of age at diagnosis. For example, 50-year-old women with stage III BC had a 5-year net survival equal to 84.9% (95% CI: 81.4%–87.7%) if they lived in the most affluent areas (Quintile 1) vs. 81.4% (76.1%–85.6%) in the most deprived areas (Quintile 5).

Adjusted excess mortality hazard and their 95% confidence interval according to stage atdiagnosis for the extreme deprivation quintiles (Q1, Q5) for the 12,738 women with breast carcinoma diagnosed in 2008–2015, living in Loire-Atlantique or Vendee at diagnosis, overall and by different ages at diagnosis.
Another interesting finding was, although not significant, that the more advanced the disease at diagnosis, the more pronounced the effect of deprivation on net survival. Among patients with stage I cancer, the survival gap between those living in Quintile 1 areas and those living in Quintile 5 areas could be considered negligible (−0.5) whereas this was estimated at 2.0 points in patients with stage II cancer and was 9.2 points in metastatic patients (stage IV) (Fig. 3).

Adjusted net survival and their 95% confidence interval for the 12,738 women with breastcarcinoma diagnosed between in 2008–2015 and living in Loire-Atlantique or Vendee according todeprivation quintiles and by stage at diagnosis.
Complementary analyses (stratification by SBR grade, hormonal profile, initial treatment or mode of detection) did not show any impact on the reported excess hazard ratios of deprivation, for models which converged (Supplementary Table 2).
Discussion
This population-based study showed that deprivation was associated with poorer overall and stage-specific BC net survival regardless of time elapsed after diagnosis. Differences in net survival between women living in the two extreme deprivation quintiles were comparable at all ages and persisted after adjustment for stage (survival gap of 4.3 points). A significant 60% and a borderline non-significant 25% higher excess mortality were observed respectively before and after adjustment by stage in the most deprived women compared to the least deprived ones. The survival gap due to deprivation increased from stage I to stage IV, although not statistically significant.
Our study was the first conducted in France to concomitantly assess the impact of stage at diagnosis and deprivation on BC survival. In our country, to minimise socioeconomic health inequalities, the universal free health insurance provides a complete free coverage of medical care for a definite list of severe or long-term diseases, including cancers, independently of the patient’s chosen healthcare structure [39]. Despite the specific features of our healthcare system, as in other studies, our results highlighted the importance of considering tumour stage at diagnosis when studying the impact of socioeconomic factors in cancer survival [10, 16,17,18,19,20,21,22,23].
Firstly, we found that the deprivation effect was non-age dependent raising questions about underlying inequalities mechanisms. Secondly, stage accounted for a large portion of the deprivation-associated survival differences. Although definition of stage and statistical methods varies across studies, the effect of deprivation on survival after adjustment for disease stage was found to be attenuated in these studies, as in our research [10, 16, 19, 20]. On the contrary, the association between deprivation and breast cancer survival was found to be stronger than without adjustment in 3 studies [17, 20, 27]. The difference in stage at diagnosis is likely to be partly related to the lesser use of, or access to, screening mammograms and to medical services, and also to a lower level of awareness of BC in women living in more deprived areas. Indeed, the existing literature supports the proposition that women living in deprived areas were less likely to see a general practitioner or gynaecologist during the last year before the BC diagnosis [40,41,42]. In the subgroup of women targeted by the organised screening programme (50–74 y/o in France), deprived women were more susceptible to have unrepeated mammography [40,41,42]. A lack of healthcare-seeking behaviours or access to care difficulties can delay BC detection and contribute to the diagnosis of more advanced BC.
Thirdly, significant differences in BC survival between the two extreme quintiles remained after adjustment for stage. The survival gap was more pronounced at more advanced stages, but was not statistically significant. This survival effect could be attributed to socioeconomic inequalities through complex mechanisms, which our study could not fully explain [15]. Cancer spread at diagnosis limits effective treatment options and increases the risk of treatment-related complications, recurrence and metastatic progression [14, 43]. Moreover, patients usually removed from healthcare resources for geographic reasons (referral centres farther away, less medical doctors in rural areas) or by choice (belief, financial difficulties, lack of social support) may be less compliant with treatment and less inclined to receive specific treatments in referral facilities [44, 45]. Comorbidities and unhealthy lifestyle habits, more frequent in deprived women, may lead to non-optimal treatment and to treatment-related complications [15]. These differences in health management were supported in our study by the fact that the likelihood that women, at an equivalent stage and age, would receive treatment, decreased with increasing deprivation levels. For instance, in 50–74-year-old women with stage I cancer, 99.7% of those living in the most affluent areas had surgery versus 98.3% of those living in the most deprived areas. However, we had not any supplementary information about the reasons of receiving different treatments and stratified analysis by initial treatment did not modify the survival effect of deprivation. Another hypothesis that could explain differences in socioeconomic survival disparities is that some tumour characteristics (such as aggressive behaviour (HER2/triple negative/SBR3)) may be more prevalent in deprived women [15]. This hypothesis can be ruled out since our study found no differences in tumour aggressiveness by deprivation level and stratified analysis (by SBR grade and hormonal profile).
In addition, higher screening rates in the most affluent patients could contribute to an artificial increase in adjusted stage net survival and the underestimation of survival differences. The comparable results obtained across age and stage groups, as well as in stratified analyses by mode of detection did not support this hypothesis. In line with our results, it appears important to continue efforts to reduce social inequalities by implementing targeted actions in all age groups.
In addition, higher screening rates in the most affluent patients could contribute to an artificial increase in adjusted stage net survival and the underestimation of survival differences. The comparable results we obtained across age and stage groups, as well as in stratified analysis by mode of detection did not support this hypothesis. In line with our results, it appears important to continue efforts to reduce social inequalities by implementing targeted actions in all age groups.
The absence of individual socioeconomic variables in cancer registries represents a limitation since ecological measurements may underestimate social inequalities in comparison with individual measurements [46]. However, by avoiding selection bias, ecological indexes are suitable to measure deprivation [47]. In addition previous researches have shown consistent results whether socioeconomic status was measured by individual indices, such as level of education or income, or by ecological indicators based on the geographic area of residence for most cancer sites [16, 22, 31, 48,49,50,51]. With regard to our choice of deprivation index, F-EDI includes both the objective and subjective poverty of the population, thus making it possible to consider overall deprivation. F-EDI is also available for all of the smallest units on the entire French mainland and has been developed in several European countries to allow geographic comparisons [46]. Another point is that our results may not reflect the situation elsewhere in France because of the regional design of the study. Indeed, Loire-Atlantique and Vendée are two affluent departments (according to F-EDI, 7% of the women live in the most deprived areas and 29% in the least ones vs. around 20% in each of them at the national level). However, we can underline that in comparison to Poiseuil’s and Tron’s study, who used a large multi-centric sample, with a higher proportion of French women living in the most deprived areas (21%), we found a similar univariate effect of deprivation on BC survival (1.64 (1.44–1.87) vs. 1.60 (1.22–2.09) in our study) conducting to a very close survival deprivation gap (5.2 points vs. 5.1 points in our study) [30, 31].
In our study, a non-parametric approach was used to study age, stage and deprivation in the context of BC survival. Compared to the Pohar-Perme estimator, one of the indicators used most frequently in the context of net survival, the excess mortality hazard framework allows consideration of the time-dependent and non-linear effects of variables [36, 37]. Despite the lack of significance of excess hazard ratios for the effect of deprivation after adjustment on stage, the survival gradient according to deprivation level remained, leading to significant differences in overall net survival between the two extreme quintiles. By stage, a similar trend was observed. The non statistically significant effect of deprivation was probably related to a lack of power due to small numbers of deprived cases, in particular for some stages.
In the absence of life tables for the general French population stratified by deprivation level, the excess hazard for women living in the most deprived areas may probably be overestimated. Nevertheless a previous study conducted a sensitivity analysis using an approximated stratification by deprivation level and their results were similar [30]. Another limitation of our study is the limited prognostic variables, which can be included in the model, due to its structural complexity. However, stratified analyses showed no impact on the reported associations, for models which converged.
The major strength of this study is its design. Indeed, population-based cancer registries provided non-biased information, which allowed assessment of survival without a selection bias. Another strength is that of data quality with few missing data. The exhaustive record of all BC cases ensures that our sample is representative of the Loire-Atlantique/Vendee population and allows the description of survival heterogeneity according to deprivation. Moreover, the Loire-Atlantique/Vendee Cancer Registry has been recording detailed data, especially stage at diagnosis, for all BC cases for 30 years.
French healthcare features notwithstanding, our study provides new information regarding the simultaneous impact of social environment and stage at diagnosis on the excess mortality due to BC in women, using flexible excess hazard modelling. The poorer BC survival observed in women living in more deprived areas was largely, but not entirely, explained by more advanced-stage BC. Socioeconomic inequalities in survival remained in all age groups. The awareness of all public health players, especially primary care providers, and the implementation of targeted actions in the most deprived areas, in terms of primary and secondary prevention, diagnosis and regular follow-up, could help to reduce social inequalities in BC survival. Further studies focused on access to medical care facilities treatment provided and medical follow-up after BC treatment are needed to explain the remaining influence of deprivation on survival according to stage. They will be helpful for the implementation of targeted actions.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
French National Cancer Institute (INCa). Stratégie décennale de lutte contre les cancers 2021–2030 [in French] [Internet]. [cited 2021 Aug 31]. Available from: https://www.e-cancer.fr/Institut-national-du-cancer/Strategie-de-lutte-contre-les-cancers-en-France/La-strategie-decennale-de-lutte-contre-les-cancers-2021-2030
Plan Cancer 2014–2019. Guérir et prévenir les cancers: donnons les mêmes chances à tous, partout en France [in French] [Internet]. [cited 2021 Aug 30]. Available from: https://www.e-cancer.fr/Institut-national-du-cancer/Strategie-de-lutte-contre-les-cancers-en-France/Les-Plans-cancer/Le-Plan-cancer-2014-2019
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424.
Defossez G, Le Guyader-Peyrou S, Uhry Z, Grosclaude P, Remontet L, Colonna M, et al. Estimations nationales de l’incidence et de la mortalité par cancer en France métropolitaine entre 1990 et 2018. Étude à partir des registres des cancers du réseau Francim. Résultats préliminaires. Rapport. [Internet]. Saint-Maurice (Fra): Santé Publique France; 2019 [cited 2021 Jul 21] p. 161. Available from: http://www.santepubliquefrance.fr/
Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Nikšić M, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018;391:1023–75.
Sant M, Chirlaque Lopez MD, Agresti R, Sánchez Pérez MJ, Holleczek B, Bielska-Lasota M, et al. Survival of women with cancers of breast and genital organs in Europe 1999-2007: results of the EUROCARE-5 study. Eur J Cancer. 2015;51:2191–205.
Molinié F, Trétarre B, Arveux P, Woronoff AS, Lecoffre C, Lafay L, et al. Survie des personnes atteintes de cancer en France métropolitaine 1989-2018—Sein [Internet]. Boulogne-Billancourt (Fra.): Institut national du cancer; 2020 Sept [cited 2021 Jul 21] p. 12. Available from: https://e-cancer.fr/
Bryere J, Tron L, Menvielle G, Launoy G, French Network of Cancer Registries (FRANCIM). The respective parts of incidence and lethality in socioeconomic differences in cancer mortality. An analysis of the French network Cancer registries (FRANCIM) data. Int J Equity Health. 2019;18:189.
Pollock AM, Vickers N. Breast, lung and colorectal cancer incidence and survival in South Thames Region, 1987-1992: the effect of social deprivation. J Public Health Med. 1997;19:288–94.
Walsh PM, Byrne J, Kelly M, McDevitt J, Comber H. Socioeconomic disparity in survival after breast cancer in ireland: observational study. PLoS ONE. 2014;9:e111729.
Deborde T, Chatignoux E, Quintin C, Beltzer N, Hamers FF, Rogel A. Breast cancer screening programme participation and socioeconomic deprivation in France. Prev Med. 2018;115:53–60.
Menvielle G, Rey G, Jougla E, Luce D. Diverging trends in educational inequalities in cancer mortality between men and women in the 2000s in France. BMC Public Health. 2013;13:823.
Ouédraogo S, Dabakuyo-Yonli TS, Roussot A, Pornet C, Sarlin N, Lunaud P, et al. European transnational ecological deprivation index and participation in population-based breast cancer screening programmes in France. Prev Med. 2014;63:103–8.
Cardoso F, Kyriakides S, Ohno S, Penault-Llorca F, Poortmans P, Rubio IT, et al. Early breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2019;30:1194–220.
Afshar N, English DR, Milne RL. Factors explaining socio-economic inequalities in cancer survival: a systematic review. Cancer Control. 2021;28:10732748211011956.
Booth CM, Li G, Zhang-Salomons J, Mackillop WJ. The impact of socioeconomic status on stage of cancer at diagnosis and survival: a population-based study in Ontario, Canada. Cancer. 2010;116:4160–7.
Kaffashian F, Godward S, Davies T, Solomon L, McCann J, Duffy SW. Socioeconomic effects on breast cancer survival: proportion attributable to stage and morphology. Br J Cancer. 2003;89:1693–6.
Haynes R, Pearce J, Barnett R. Cancer survival in New Zealand: ethnic, social and geographical inequalities. Soc Sci Med. 2008;67:928–37.
Jansen L, Eberle A, Emrich K, Gondos A, Holleczek B, Kajüter H, et al. Socioeconomic deprivation and cancer survival in Germany: an ecological analysis in 200 districts in Germany. Int J Cancer. 2014;134:2951–60.
Schrijvers CT, Mackenbach JP, Lutz JM, Quinn MJ, Coleman MP. Deprivation and survival from breast cancer. Br J Cancer. 1995;72:738–43.
Trewin CB, Johansson ALV, Hjerkind KV, Strand BH, Kiserud CE, Ursin G. Stage-specific survival has improved for young breast cancer patients since 2000: but not equally. Breast Cancer Res Treat. 2020;182:477–89.
Skyrud KD, Bray F, Eriksen MT, Nilssen Y, Møller B. Regional variations in cancer survival: Impact of tumour stage, socioeconomic status, comorbidity and type of treatment in Norway. Int J Cancer. 2016;138:2190–200.
Rutherford MJ, Hinchliffe SR, Abel GA, Lyratzopoulos G, Lambert PC, Greenberg DC. How much of the deprivation gap in cancer survival can be explained by variation in stage at diagnosis: an example from breast cancer in the East of England. Int J Cancer. 2013;133:2192–200.
Kumachev A, Trudeau ME, Chan KKW. Associations among socioeconomic status, patterns of care and outcomes in breast cancer patients in a universal health care system: Ontario’s experience. Cancer. 2016;122:893–8.
Allgood PC, Duffy SW, Kearins O, O’Sullivan E, Tappenden N, Wallis MG, et al. Explaining the difference in prognosis between screen-detected and symptomatic breast cancers. Br J Cancer. 2011;104:1680–5.
Li R, Daniel R, Rachet B. How much do tumor stage and treatment explain socioeconomic inequalities in breast cancer survival? Applying causal mediation analysis to population-based data. Eur J Epidemiol. 2016;31:603–11.
Finke I, Behrens G, Maier W, Schwettmann L, Pritzkuleit R, Holleczek B, et al. Small-area analysis on socioeconomic inequalities in cancer survival for 25 cancer sites in Germany. Int J Cancer. 2021;149:561–72.
Zadnik V, Žagar T, Tomšič S, Mihor A, Lokar K. Cancer Patients’ Survival According to Socioeconomic Environment in a High-Income Country with Universal Health Coverage. Cancers (Basel). 2022;14:1620.
Pornet C, Delpierre C, Dejardin O, Grosclaude P, Launay L, Guittet L, et al. Construction of an adaptable European transnational ecological deprivation index: the French version. J Epidemiol Community Health. 2012;66:982–9.
Poiseuil M, Tron L, Woronoff AS, Trétarre B, Dabakuyo-Yonli TS, Fauvernier M, et al. How do age and social environment affect the dynamics of death hazard and survival in patients with breast or gynecological cancer in France? Int J Cancer. 2021;68:1233–57.
Tron L, Belot A, Fauvernier M, Remontet L, Bossard N, Launay L, et al. Socioeconomic environment and disparities in cancer survival for 19 solid tumor sites: An analysis of the French Network of Cancer Registries (FRANCIM) data. Int J Cancer. 2019;144:1262–74.
Sobin LH, Gosporadowicz MK, Wittelkind C. TNM classification of malignant tumors. 7th ed. 2011. https://www.amazon.com/Classification-Malignant-Tumours-Leslie-Sobin/dp/1444332414
Guillaume E, Pornet C, Dejardin O, Launay L, Lillini R, Vercelli M, et al. Development of a cross-cultural deprivation index in five European countries. J Epidemiol Community Health. 2016;70:493–9.
Cancers & Preventions—UMR 1086 UCN.Caen. Plate-forme méthodologique nationale pour l’étude et la réduction des inégalités sociales en cancérologie (ERISC). [cited 2021 Dec 12]. Available from: http://cancerspreventions.fr/inegalites-sociales/plateforme-2/
Estève J, Benhamou E, Croasdale M, Raymond L. Relative survival and the estimation of net survival: elements for further discussion. Stat Med. 1990;9:529–38.
Fauvernier M, Roche L, Uhry Z, Tron L, Bossard N, Remontet L, et al. Multi‐dimensional penalized hazard model with continuous covariates: applications for studying trends and social inequalities in cancer survival. J R Stat Soc C. 2019;68:1233–57. https://onlinelibrary.wiley.com/doi/10.1111/rssc.12368
Remontet L, Uhry Z, Bossard N, Iwaz J, Belot A, Danieli C, et al. Flexible and structured survival model for a simultaneous estimation of non-linear and non-proportional effects and complex interactions between continuous variables: Performance of this multidimensional penalized spline approach in net survival trend analysis. Stat Methods Med Res. 2019;28:2368–84.
Fauvernier M, Remontet L, Uhry Z, Bossard N, Roche L. survPen: an R package for hazard and excess hazard modelling with multidimensional penalized splines. J Open Source Softw. 2019;4:1434 https://joss.theoj.org/papers/10.21105/joss.01434
ALD [Internet]. [cited 2022 Aug 11]. Available from: https://www.ameli.fr/assure/droits-demarches/maladie-accident-hospitalisation/affection-longue-duree-ald/affection-longue-duree-maladie-chronique
Sicsic J, Franc C. Obstacles to the uptake of breast, cervical, and colorectal cancer screenings: what remains to be achieved by French national programmes? BMC Health Serv Res. 2014;14:465.
Duport N. Characteristics of women using organized or opportunistic breast cancer screening in France. Analysis of the 2006 French Health, Health Care and Insurance Survey. Rev Epidemiol Sante Publique. 2012;60:421–30.
Ferrat E, Le Breton J, Djassibel M, Veerabudun K, Brixi Z, Attali C, et al. Understanding barriers to organized breast cancer screening in France: women’s perceptions, attitudes, and knowledge. Fam Pract. 2013;30:445–51.
Redig AJ, McAllister SS. Breast cancer as a systemic disease: a view of metastasis. J Intern Med. 2013;274:113–26.
Thomson CS, Hole DJ, Twelves CJ, Brewster DH, Black RJ, Scottish Cancer Therapy Network. Prognostic factors in women with breast cancer: distribution by socioeconomic status and effect on differences in survival. J Epidemiol Community Health. 2001;55:308–15.
Aarts MJ, Hamelinck VC, Bastiaannet E, Coebergh JWW, Liefers GJ, Voogd AC, et al. Small but significant socioeconomic inequalities in axillary staging and treatment of breast cancer in the Netherlands. Br J Cancer. 2012;107:12–7.
Lamy S, Molinié F, Daubisse-Marliac L, Cowppli-Bony A, Ayrault-Piault S, Fournier E, et al. Using ecological socioeconomic position (SEP) measures to deal with sample bias introduced by incomplete individual-level measures: inequalities in breast cancer stage at diagnosis as an example. BMC Public Health. 2019;19:857.
Bryere J, Pornet C, Copin N, Launay L, Gusto G, Grosclaude P, et al. Assessment of the ecological bias of seven aggregate social deprivation indices. BMC Public Health. 2017;17:86.
DeRouen MC, Schupp CW, Koo J, Yang J, Hertz A, Shariff-Marco S, et al. Impact of individual and neighborhood factors on disparities in prostate cancer survival. Cancer Epidemiol. 2018;53:1–11.
Hagedoorn P, Vandenheede H, Vanthomme K, Gadeyne S. Socioeconomic position, population density and site-specific cancer mortality: a multilevel analysis of Belgian adults, 2001-2011. Int J Cancer. 2018;142:23–35.
Diez Roux AV. A glossary for multilevel analysis. J Epidemiol Community Health. 2002;56:588–94.
Dalton SO, Olsen MH, Johansen C, Olsen JH, Andersen KK. Socioeconomic inequality in cancer survival—changes over time. A population-based study, Denmark, 1987-2013. Acta Oncol. 2019;58:737–44.
Acknowledgements
We would like to thank those who provided data to the registry: pathologists (CHD Vendée, CH Saint-Nazaire, CHU Nantes, IHP group, Kerlo-Morin laboratory, CRLCC Nantes-Angers, CHU Angers, laboratories from Ille-et-Vilaine and Nouvelle-Aquitaine), oncologists, public and private hospital medical data processing departments, and medical practitioners as well as the medical departments of the national health insurance programmes, the screening coordination centre and Cancer Regional Network. We would like to thank ERISC/MapInMed platform (French national methodological platform for the study and reduction of health social inequalities in oncology) for the attribution of F-EDI value.
Funding
This work was prepared within the framework of the SIRIC ILIAD programme supported by the French National Cancer Institute (INCa), the French Ministry of Health, and the Institute of Health and Medical Research (INSERM); SIRIC ILIAD INCa-DGOS-Inserm_12558 grant. The Loire-Atlantique/Vendee Cancer Registry is supported for the routine collection of data by the French National Cancer Institute (INCa), Santé Publique France, Direction Générale de l’Offre de Soins (DGOS), local institutions (Conseil Régional des Pays de la Loire, ARS des Pays de la Loire, CHU Nantes, CHD Vendée, Institut de Cancérologie de l’Ouest) and the League Against Cancer (comités de Loire-Atlantique et de Vendée).
Author information
Authors and Affiliations
Contributions
FM, ACB had the idea for the study. C Delacôte, SD, SAY, ACB, FM contributed to the conception and design of the analysis. ADT, GR, MV, SA collected the data. C Delacôte performed the analysis. C Delacôte, SD, SAY, C Delpierre, ACB, FM contributed to the interpretation. The first draft of the work was written by C Delacôte and all authors commented on previous versions of the manuscript. All authors revised the manuscript critically for important intellectual content and approved the final version for publication. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval and consent to participate
This study is based on data from the Loire-Atlantique/Vendee Cancer Registry, a member of the French network of cancer registries (FRANCIM). It has received the approval of the French regulatory authorities for the collection and analysis of medical data: the Comité Consultatif sur le Traitement de l’Information en matière de Recherche dans le Domaine de la Santé (ethical approval) and the Commission Nationale Informatique et Libertés (legal framework and data protection). In conformity with French law, patients were informed individually of the nature of the information provided, the purpose of data processing, their right of access, rectification and objection. The ethics committee, in accordance with French law, did not request informed consent. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or a comparable ethical standard. All methods were performed in accordance with the relevant guidelines and regulations.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Delacôte, C., Delacour-Billon, S., Ayrault-Piault, S. et al. Is survival rate lower after breast cancer in deprived women according to disease stage?. Br J Cancer 128, 63–70 (2023). https://doi.org/10.1038/s41416-022-02024-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41416-022-02024-w
- Springer Nature Limited