
Abstract
Background Dental caries in children's permanent teeth remains a global burden. In contrast to the traditional approach of treating the disease through surgical operative intervention, minimum intervention has increasingly been recommended for managing children with dental caries.
Aim This scoping review aimed to describe the literature related to the provision of minimum intervention dentistry for children with caries and to identify research gaps.
Methods Electronic databases (Medline via Ovid, PubMed, Web of Science and Scopus) were searched, together with grey literature databases, and key organisation websites. Data was extracted on a piloted extraction template and a thematic analysis was undertaken.
Results Sixty-seven relevant articles were identified. No empirical literature was identified that assessed a complete minimum intervention care pathway to managing caries. Five themes were identified from the scoping literature: evidence base, clinician attitude and skills, practice implementation, acceptability and environmental factors.
Conclusions The majority of articles were opinion papers. There is a paucity of empirical evidence supporting the clinical and cost-effectiveness of a minimum intervention pathway for children with dental caries in primary dental care. The scoping review has identified some potential barriers to the implementation of such a care pathway, including regulatory and remunerative frameworks and clinical training/education.
Key points
-
Describes the process of carrying out a scoping review of the literature on minimum intervention dentistry for children with dental caries.
-
Describes the literature on minimum intervention dentistry and children with dental caries.
-
Suggests further research is needed to explore the clinical and cost-effectiveness of a minimum intervention dentistry care pathway for children with dental caries.
Similar content being viewed by others


Background
Dental caries is one of the most common non-communicable diseases (NCDs) worldwide and remains a significant public health problem. The Global Burden of Diseases Study 2017 reported that untreated dental caries was the most prevalent condition, with 2.3 billion people affected by untreated dental caries in permanent teeth, and for primary teeth 532 million children affected.1 In the United Kingdom, it is one of the most common childhood NCDs, with nearly a half of 15-year-olds and a third of 12-year-olds having obvious decay experience in their permanent teeth, and it follows social gradients with the most deprived being more affected.2
Management of dental caries has been addressed traditionally using a mechanistic, surgical operative approach.3 This approach has typically involved the removal of all the affected tooth tissue usually under a local anaesthetic and restoration by filling the cavity with a restorative material. The use of a drill and injections are procedures commonly reported by children as causing anxiety and fear. Furthermore, dental restorations in permanent teeth have a finite longevity and replacements are required periodically. This places the tooth and the patient in a cycle of lifelong restorative care, frequently leading to the eventual loss of the tooth.4
Advances in the understanding of the caries disease process have shown that carious lesions in the early stages can be reversed,5 together with an understanding that dentine-pulp complex reactions are protective, promoting the maintenance of tooth vitality. These, coupled with advances in dental biomaterials and adhesion, underpinned by the fact that dental restorations have a finite lifespan, support the management of a patient with dental caries in a more minimally invasive operative manner.
Different terminology appears to be used for this approach;6,7,8,9,10 throughout this article, we use the term 'minimum intervention dentistry' (MID). There is variation surrounding the components of MID11 and how this approach can be implemented for children with established dental caries presenting in primary care.12,13,14,15,16 The aim of this scoping review was to describe the literature related to the provision of MID for children with caries and to identify research gaps.
Methods
A scoping review was undertaken according to the approach developed by Arksey and O'Malley.17 For this scoping review of MID and children with carious teeth, the research question was: 'What is the nature of the literature on minimum intervention dentistry and children with caries?' The clinical scope was kept broad to capture as much literature in this area as possible since the aim was to identify what literature existed as well as the research gaps. Literature relevant to the target population of children defined as under 18 years old was included.
A search was conducted on electronic databases including Medline via Ovid, Web of Science, PubMed and Scopus. After a preliminary search, the terms 'minimum intervention' OR 'minimal intervention' were used with the term 'dentistry' or 'caries' to identify relevant evidence. These keywords were felt to cover the range of terms used for techniques following a minimum interventive approach. The search was limited to articles in the English language due to translation costs and time available. Articles published between 1970 to September 2020 were included since the term 'minimum intervention dentistry' was commonly used from the 1990s; thus, 1970 allowed a large leeway. Databases that searched for grey literature were included (Open Grey and Ethos).
The inclusion criteria were:
-
The keywords 'minimum intervention' or 'minimal intervention' being included in the title and/or abstracts or as keywords
-
All types of research design (randomised control trials, cohort trials, case-control studies, cross-sectional studies, opinion articles)
-
Articles in English language
-
Articles published from January 1970 to September 2020.
The exclusion criteria were papers:
-
Relating solely to clinical conditions other than dental caries
-
Relating solely to cosmetic dentistry and/or facial aesthetics
-
Published before 1970
-
Where abstracts and texts could not be obtained
-
In languages other than English
-
Where MID was not or could not be related to children
-
Describing in vitro or animal-based studies.
Reference lists and manual searching was conducted. Certain UK-based organisations' websites were also searched to identify relevant literature, including British Dental Association, National Institute for Health and Care Excellence, Faculty of General Dental Practice (UK) and General Dental Council.
The papers were processed in Endnote and duplicates removed. A data extraction spreadsheet was designed using the initial topics and themes from a preliminary literature review. The data extraction form was piloted (BD, ZM, CD) on five articles in order to aid consistency and agreement. The initial themes that were identified from the literature review were discussed and further themes were added to the data extraction form.
An optional sixth stage, that of a consultation exercise, is advocated by Arksey and O'Malley.17 Levac et al. propose that the consultation stage improves the academic rigour and is an essential component in a scoping review.18 The consultation stage aimed to help identify any relevant missed literature, to provide further insights into the findings of the scoping review and help prioritise future research. The consultation stage involved group and individual discussions, with purposively selected groups of stakeholders. These stakeholders included four practice owners, three associate dentists (from three different NHS dental practices), two dental therapists (from two dental practices), a dental nurse, practice manager and six patients who were part of a patient and public group meeting.
Results
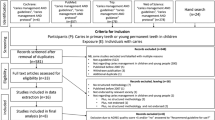
The electronic searches from the databases revealed a total of 753 papers; 338 duplicates were removed. After removal of these duplicates, the remaining 415 articles had their titles screened to see if they were applicable to the area of study. Those that showed relevance to the topic of MID and caries were further assessed. Abstract screening revealed 139 papers that required full-text screening. Sixty-three articles were included from the electronic search results. Hand searching using reference lists identified four further articles. In total, 67 papers satisfied the inclusion criteria (see online supplementary information). A flowchart of the search and screening process is detailed in Figure 1.

Flowchart of the search strategy
Article characteristics
Of the 67 included articles, the first authors of the articles were from a variety of countries. Australia (n = 18) and the UK (n = 17) were the most common countries of origin, with France (n = 9) and the United States of America (n = 5) the next most frequent.
Publications were from 24 different journals. The most common journal of publication was the British Dental Journal (n = 23), with the Australian Dental Journal the next most frequent (n = 12).
Results showed that most of the studies were opinion papers (n = 48), with six reporting a randomised control trial (RCT), seven questionnaire-based cross-sectional studies, one interview-based qualitative study, one retrospective cohort study and four reviews (two systematic reviews and two literature reviews).
'Components' included in minimum intervention dentistry
The included papers were investigated for the components of MID they included. Components were placed into domains of: a) detection; b) diagnosis; c) prevention; and d) minimally invasive interventions. As some components were applicable in more than one domain, they were included in all relevant domains (Fig. 2).

Components included in the domains of minimum intervention dentistry
Detection
Twelve components were used or described in the literature for the detection stage of MID. As expected, the visual and tactile method of detection was the most common method advocated (n = 23). Radiography was also advocated in 14 papers. The use of the International Caries Detection and Assessment System (ICDAS) was included in 14 papers. The use of additional detection aids such as light fluorescence were advocated by 14 papers.
Diagnosis
The inclusion of a caries risk assessment tool appeared in 21 papers. These advocated the use of a structured caries risk assessment (CRA) method with caries management by risk assessment being the most common (n = 8). Other CRA tools included the Cariogram (n = 5). The use of salivary tests as part of a CRA were included in 12 papers. Also, the use of light fluorescence technology appeared in three papers.
Prevention
The literature has identified several components that may be used alone or in combination. The most common professional intervention was fluoride varnish (n = 23), followed by oral health education (n = 14) and fissure sealants (n = 13; resin-based sealants [n = 9] and glass ionomer-based sealants [n = 9]).
Minimally invasive interventions
Minimally invasive interventions and techniques included adhesive restorative materials (n = 28), atraumatic restorative treatment (ART) (n = 17) and micro-invasive management of non-cavitated lesions (n = 8). With regards to how much caries should be removed, selective caries removal appeared as the most common (n = 14), with the stepwise technique mentioned in two papers. A number of caries removal instruments were specifically mentioned including air-abrasion (n = 6), chemo-mechanical (n = 6) and sono-abrasion (n = 5).
In summary, the literature revealed broad agreement that the principal domains of MID were detection/diagnosis (identifying the problem), prevention, minimally invasive operative interventions and recall. The stages of detection and diagnosis were often combined as one domain. There were a wide range of components that could be included to execute each domain.
Analysis of papers by 'theme'
Five themes, four of which were sub-divided into sub-themes, emerged from the scoping review literature (see Table 1). Several papers expressed more than one theme.
Evidence base
There were three sub-themes highlighted: limitations of the traditional approach, the clinical effectiveness and the cost-effectiveness of minimum intervention dentistry. The scoping review identified several papers, mainly opinion pieces, that criticised the traditional approach to caries management and highlighted its potential disadvantages when compared to minimum intervention and its components.12,13,14,15,16 While the review found several opinion pieces that claimed minimum intervention dentistry was effective based on evidence from its individual components,15,19,20,21,22,23 the scoping review failed to identify any definitive trials of the efficacy or effectiveness of a complete minimum intervention care pathway for children with dental caries in their permanent teeth. Two papers described RCTs. However, they evaluated the ART approach and did not include other minimum intervention domains.21,24 These studies stated that the ART was as effective as conventional treatment. Similarly, while many articles suggested the cost-effectiveness of minimum intervention was important, no health economic evaluations were conducted. This theme highlights the large gap in the literature into the clinical and cost-effectiveness of minimum intervention pathways in primary dental care compared to standard care.
Clinical skills and attitude
This theme, which included 27 papers, was sub-divided into two subthemes: i) clinicians' attitudes and knowledge; and ii) teaching and education. The majority of papers included in this theme were opinion papers. The empirical papers consisted of two cross-sectional studies and one qualitative paper. There was an apparent lack of knowledge among primary dental care clinicians about the minimum intervention approach and some suggestion of reluctance on their behalf to learn to deliver it, particularly when the evidence base in primary dental care was perceived to be lacking. The impact of historical undergraduate teaching in favouring the traditional surgical approaches over minimum intervention may be influencing this perception. It was suggested that minimum intervention training needs to be more prevalent in undergraduate programmes and postgraduate courses, with hands-on practical experience favoured.
Implementation in primary dental care
Theme three included two subthemes: i) the current use of minimum intervention in primary dental care; and ii) the utilisation of the whole oral healthcare team. The literature, mostly opinion pieces, suggested that the current use of the minimum intervention pathway in primary dental care was low, although many of the individual techniques/procedures are used separately. The literature generally advocates utilisation of the whole oral healthcare team to deliver it, although randomised control trials were only available for dental therapists using ART.25,26,27
Acceptability to patients and parent/carers
Acceptability of minimum intervention to patients and parent/carers is a recurring theme including empirical questionnaire-based studies,19,27,28,29,30 and authors state that minimum intervention offers a more 'patient-friendly' approach to caries management. A trial conducted in public health clinics in Australia by Arrow and Klobas assessed acceptability of the ART compared to the standard care approach.27 The study utilised a facial image scale-based questionnaire and found similar levels of dental anxiety between the two arms.
Environmental factors
This includes sub-themes of: a) regulatory and remunerative frameworks; and b) medico-legal concerns. The scoping review identified the regulatory and remuneration system as an important factor that will impact on the implementation of minimum intervention oral care delivery. Remuneration systems appear to reward dental professionals better for itemised restorative treatments than for prevention.14,31,32,33,34,35 Similarly, medico-legal concerns about changing clinical practice to a minimum intervention approach may be a factor that impacts provision by clinicians. Opinion papers have suggested the risk of litigation of such a minimum intervention approach was low.36,37 This is based on the presumption that a minimum intervention care pathway is a 'well-proved and well-accepted' procedure,36 also being well established. Such an argument is open to debate given the lack of definitive research supporting this.
Stakeholder consultation
The results described above were discussed during a consultation with public and patient involvement (PPI) groups and dental professional stakeholders. The stakeholders were able to discuss the themes and endorse the areas for future research relating to minimum intervention dentistry. In addition, they identified several other gaps including:
-
The importance of research relating to the progression of caries
-
The costs of delivering minimum intervention in primary dental care including equipment costs, costs associated with training of the oral healthcare team and any building alterations required
-
Children's perspectives on the appearance of teeth
-
The environmental impact of minimum intervention dentistry compared to traditional approaches.
In summary, the stakeholder consultation stage of the scoping review supported the results and added valuable insights to inform future research.
Summary and the research gaps
The scoping literature has identified several gaps in the research and uncertainties regarding the minimum intervention care pathway. These are summarised in Table 2. There were no studies found that assessed the whole minimum intervention care pathway versus the traditional approach for managing children with caries in their permanent teeth.
Discussion
This scoping literature review is the first to describe the literature related to the provision of minimum intervention dental care for children with caries. It aimed to identify related themes and research gaps to inform future research. The majority of articles were opinion papers and the review found no empirical studies that assessed implementation and acceptability of the whole minimum intervention care pathway.
Previous randomised control trials performed in general practice have assessed healthcare interventions as single entities without considering that they form part of a care pathway delivered to patients in a complex environment. In clinical settings, healthcare delivered by professionals including dental professionals can consist of a number of different interventions under varying contextual influences. These cannot really be said to be just simple interventions that should be looked at in isolation. For example, treatment of a carious cavity in an individual would involve detection, diagnosis, risk assessment, consultation with the patient regarding preferences, possibly care delivered by differing dental professionals and maybe even in a variety of environments. Complex interventions are common in the health service setting and their evaluations pose specific challenges. The Medical Research Council has published guidance on developing, evaluating and implementing complex interventions, and this field is evolving.38,39
Minimum intervention care as described above is a complex longitudinal intervention made up of several interacting components within defined domains, delivered possibly in different organisational settings, with several outcomes of interest, involving variable stakeholder behaviours and tailored to the individual patient.
The literature highlighted the variation between authors in the terminology and components of minimum intervention dentistry. While many opinion pieces describe minimum intervention dentistry as an evidence-based approach, there remains a lack of research on its clinical and cost-effectiveness compared to usual care. This may be due to the historic focus on individual components of minimum intervention delivery. However, it should be regarded as a complex longitudinal intervention comprised of interacting domains11 and so evaluation of the whole pathway is required.40 For example, if detection of carious lesions is not optimal at baseline, then analysis of clinical outcome measures at final follow-up may show reduced effectiveness of an intervention with no significant difference from a control. In practice, this is important and an understanding of how one domain can affect another in any care pathway is important.
An important aim of the scoping review was to identify gaps in the literature which will help to design future studies and help plan implementation of minimum intervention care. Gaps included undergraduate training, impact of regulatory and remunerative frameworks, workforce skill mix and medico-legal aspects.41
In this review, no papers were found to focus on children and their carers' perspectives of minimum intervention dentistry. For patient-focused care, the views of children and carers must be considered and explored. The stakeholder consultation suggested that the aesthetic impact should be included which may require child-focused research approaches with children and their parents/carers.42
The search methods for this review focused on searching for studies that discussed or evaluated the entire minimum intervention pathway. As such, the many terms used to describe minimum intervention dentistry would be identified in the electronic searches using the broad search terms described in the method section. However, a potential limitation of this review is that separate searches were not conducted for each individual domain of minimum intervention. A search of the literature for all domains, including minimally invasive dentistry, would result in a huge number of articles but likely add little to the scoping review findings. Reference list checking, grey literature searching and stakeholder and consultation with two cariologists were also conducted to limit omission of key articles. The inclusion of English language-only articles may also be a limitation of the review.
The lack of consensus of terminology can cause not only difficulty when searching for literature, but also when trying to understand what components may be included. The term 'minimally invasive dentistry' may also compound the problem. In 2016, the FDI updated their policy on minimal intervention dentistry as 'to conserve remineralisable and intact tooth tissue to help retain teeth throughout life. Tooth tissue should not be removed unnecessarily. The major components include: 1) early detection of carious lesions and assessment of caries risk and activity; 2) remineralisation of demineralised enamel and dentine; 3) optimal measurements to keep sound teeth sound; 4) tailor-made dental recalls; 5) minimally invasive operative interventions to ensure tooth survival; 6) repairing rather than replacing defective restorations'.
Moving forward, the terms 'minimum intervention oral care' and 'minimally invasive dentistry' have been presented to further try to clarify this discipline. Minimum intervention oral care (MIOC) has been defined as individualised patient care delivery, with responsibilities from the oral healthcare team and patient, using research and development in disease detection and diagnosis, susceptibility assessment, prevention/control regimes and minimally invasive operative treatments, with the goal of maintaining lifelong oral health. The term minimally invasive dentistry (MID) is now solely used to describe all operative interventions at the tooth level, which should be biological, respecting and preserving dental/oral hard and soft tissues, being as minimally destructive as possible. State-of-the-art operative technologies/bioactive materials should be mastered and used. This is one of the four interlinking domains that make up the MIOC framework.43
Conclusions
The majority of articles about minimum intervention dentistry and caries in children were opinion pieces with limited empirical studies. The scoping review consistently identified a minimum intervention care pathway to consist of the domains of detection and diagnosis, prevention, restoration and recall. It also shows that several components can be included in these domains. Themes that were identified were evidence base, clinical skill and attitude, practice implementation, acceptability and environment influences. There is a paucity of evidence supporting the clinical and cost-effectiveness of minimum intervention for children with dental caries in primary dental care. In addition, several other gaps in the research were identified including effectiveness, acceptability and barriers to implementation. A controlled trial to determine the clinical and cost-effectiveness of the entire minimum intervention oral care pathway in children is required. However, the scoping review identified factors to consider in implementation and acceptability of minimum intervention dentistry. Further feasibility work would help to provide insight into key parameters before conducting a full-scale trial.
References
GBD 2017 Oral Disorders Collaborators, Bernabe E, Marcenes W et al. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J Dent Res 2020; 99: 362-373.
Pitts N, Chadwick B, Anderson T. Child Dental Health Survey 2013 Report 2: Dental Disease and Damage in Children England, Wales and Northern Ireland. 2015. Available at https://digital.nhs.uk/data-and-information/publications/statistical/children-s-dental-health-survey/child-dental-health-survey-2013-england-wales-and-northern-ireland (accessed April 2021).
Black G V. A work on operative dentistry. Chicago: Medical Dental Publishing, 1908.
Elderton R J. The prevalence of failure of restorations: a literature review. J Dent 1976; 4: 207-210.
Koulourides T, Feagin F, Pigman W. Remineralization of dental enamel by saliva in vitro. Ann N Y Acad Sci 1965; 131: 751-757.
Dawson A S, Makinson O F. Dental treatment and dental health. Part 1. A review of studies in support of a philosophy of Minimum Intervention Dentistry. Aust Dent J 1992; 37: 126-132.
Dawson A S, Makinson O F. Dental treatment and dental health. Part 2. An alternative philosophy and some new treatment modalities in operative dentistry. Aust Dent J 1992; 37: 205-210.
FDI World Dental Federation. FDI policy statement on Minimal Intervention Dentistry (MID) for managing dental caries: Adopted by the General Assembly: September 2016, Poznan, Poland. Int Dent J 2016; 67: 6-7.
Frencken J E, Peters M C, Manton D J, Leal S C, Gordan V V, Eden E. Minimal intervention dentistry for managing dental caries - a review: report of a FDI task group. Int Dent J 2017; 62: 223-243.
Tyas M J, Anusavice K J, Frencken J E, Mount G J. Minimal intervention dentistry-a review. FDI Commission Project 1-97. Int Dent J 2000;50: 1-12.
Craig P, Dieppe P, Macintyre S et al. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ 2008; DOI: 10.1136/bmj.a1655.
Banerjee A. 'MI'opia or 20/20 vision? Br Dent J 2013; 214: 101-105.
Banerjee A. 'Minimum intervention' - MI inspiring future oral healthcare? Br Dent J 2017; 223: 133-135.
Calache H, Hopcraft M S, Martin J M. Minimum intervention dentistry - A new horizon in public oral health care. Aust Dent J 2013; 58 Suppl 1: 17-25.
Featherstone J D B, Doméjean S. Minimal intervention dentistry: Part 1. from 'compulsive' restorative dentistry to rational therapeutic strategies. Br Dent J 2012; 213: 441-445.
Innes N P, Manton D J. Minimum intervention children's dentistry - the starting point for a lifetime of oral health. Br Dent J 2017; 223: 205-213.
Arksey H, O'Malley L. Scoping studies: Towards a methodological framework. Int J Soc Res Methodol 2005; 8: 19-32.
Levac D, Colquhoun H, O'Brien K K. Scoping studies: advancing the methodology. Implement Sci 2010; 5: 69.
de Menezes Abreu D M, Leal S C, Mulder J, Frencken J E. Pain experience after conventional, atraumatic, and ultraconservative restorative treatments in 6-to 7-yr-old children. Eur J Oral Sci 2011; 119: 163-168.
Freitas M F L, Santos J M, Fuks A, Bezerra A C B, Azevedo T D P L. Minimal Intervention Dentistry Procedures: a Ten Year Retrospective Study. J Clin Pediatr Dent 2014; 39: 64-67.
Mandari G J, Frencken J E, van't Hof M A. Six-year success rates of occlusal amalgam and glass-ionomer restorations placed using three minimal intervention approaches. Caries Res 2003; 37: 246-253.
Mickenautsch S, Yengopal V. Extent and quality of systematic review evidence related to minimum intervention in dentistry: essential oils, powered toothbrushes, triclosan, xylitol. Int Dent J 2011; 61: 179-192.
Tyas M J, Anusavice K J, Frencken J E, Mount G J. Minimal intervention dentistry - a review - FDI Commission Project 1-97. Int Dent J 2000; 50: 1-12.
Mandari G J, Truin G J, van't Hof M A, Frencken J E. Effectiveness of three minimal intervention approaches for managing dental caries: survival of restorations after 2 years. Caries Res 2001; 35: 90-94.
Arrow P, Klobas E. Minimum intervention dentistry approach to managing early childhood caries: a randomized control trial. Community Dent Oral Epidemiol 2015; 43: 511-520.
Arrow P, Klobas E. Child oral health-related quality of life and early childhood caries: a non-inferiority randomized control trial. Aust Dent J 2016; 61: 227-235.
Arrow P, Klobas E. Minimal intervention dentistry for early childhood caries and child dental anxiety: a randomized controlled trial. Aust Dent J 2017; 62: 200-207.
Brennan D S, Balasubramanian M, Spencer A J. Restorative treatment for initial, cavitated and gross coronal carious lesions. Aust Dent J 2016; 61: 350-356.
Burke F J T, McHugh S, Shaw L et al. UK dentists' attitudes and behaviour towards Atraumatic Restorative Treatment for primary teeth. Br Dent J 2005; 199: 365-369.
Frencken J E. Atraumatic restorative treatment and minimal intervention dentistry. Br Dent J 2017; 223: 183-189.
Dawett B, Atkins B, Banerjee A. A guide to building 'MI' oral healthcare practice. Br Dent J 2017; 223: 223-227.
Doméjean S, Banerjee A, Featherstone J D B. Caries risk/susceptibility assessment: its value in minimum intervention oral healthcare. Br Dent J 2017; 223: 191-197.
Mickenautsch S. An introduction to minimum intervention dentistry. Singapore Dent J 2005; 27: 1-6.
Mickenautsch S, Rudolph M J. Minimal intervention dentistry (MI) for South Africa. SADJ 2004; 59: 327, 329.
Schwendicke F, Foster Page L A, Smith L A, Fontana M, Thomson W M, Baker S R. To fill or not to fill: a qualitative cross-country study on dentists' decisions in managing non-cavitated proximal caries lesions. Implement Sci 2018; 13: 54.
D'Cruz L. Dento-legal considerations about an MI approach. Br Dent J 2017; 223: 199-201.
Mackenzie L, Banerjee A. Minimally invasive direct restorations: a practical guide. Br Dent J 2017; 223: 163-171.
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. Int J Nurs Stud 2013; 50: 587-592.
Craig P, Petticrew M. Developing and evaluating complex interventions: reflections on the 2008 MRC guidance. Int J Nurs Stud 2013; 50: 585-587.
Squires J E, Valentine J C, Grimshaw J M. Systematic reviews of complex interventions: framing the review question. J Clin Epidemiol 2013; 66: 1215-1222.
Brocklehurst P R, Williams L, Burton C, Goodwin T, Rycroft-Malone J. Implementation and trial evidence: a plea for fore-thought. Br Dent J 2017; 222: 331-335.
Marshman Z, Gibson B J, Owens J et al. Seen but not heard: a systematic review of the place of the child in 21st-century dental research. Int J Paediatr Dent 2007; 17: 320-327.
Banerjee A. Minimum intervention oral healthcare delivery - is there consensus? Br Dent J 2020; 229: 393-395.
Funding
The project was funded by the National Institute for Health Research (NIHR) through a Doctoral Research Fellowship. The views and opinions expressed by the authors in this publication are those of the authors and do not necessarily reflect those of the NIHR.
Author information
Authors and Affiliations
Contributions
BD, CD, AB, DP and ZM contributed towards the conception of the design. BD, DP and ZM contributed towards data aquistion and analysis. All authors contributed towards interpretation, drafted and critically revised the manuscript.
Corresponding author
Ethics declarations
None to disclose.
Supplementary Information
Rights and permissions
About this article

Cite this article
Dawett, B., Deery, C., Banerjee, A. et al. A scoping literature review on minimum intervention dentistry for children with dental caries. Br Dent J (2022). https://doi.org/10.1038/s41415-022-4038-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41415-022-4038-8
- Springer Nature Limited
This article is cited by
-
A dental student's experiences of Minimal Intervention Dentistry
BDJ Student (2024)