
Abstract
While the conventional fabrication of removal partial dentures through the lost-wax technique is a time-tested technique, it is recognised as a 'complicated, error-prone, time-consuming and expensive process'. This has financial implications and can lead to increased chair time for the patient and dentist, resulting from low precision and ill-fitting frameworks. The use of computer-aided design and computer-aided manufacture brings removable prosthodontics into the digital era and opens up a host of benefits to the practitioner and laboratory technician. This paper introduces the benefits and downsides to adopting a digital workflow, and looks at the various alternative manufacturing techniques, which allow the clinician and technician to streamline their processes and make use of novel denture materials.
Key points
-
CAD-CAM systems are increasingly being adopted in the design and fabrication of removable prostheses.
-
The digital workflow is more time-efficient, can eliminate technique sensitivity and allows for easier collaborative discussions between patient, clinician and technician.
-
Computer-aided manufacture allows for the introduction of newer materials with advantageous properties when compared to traditional materials.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
The advantages of computer-aided design and computer-aided manufacturing (CAD-CAM) to fabricate removable partial denture (RPD) frameworks lie in the opportunities to exploit advances in digital technology by enabling the use of new materials and novel methods of production.1 Introducing new denture materials into the market is not simply a question of material science advances; materials may be available in the industrial setting, but without comparable means of production in a dental setting, such materials are inaccessible. Part one of this series will look at the developments in design and manufacturing in dental technology that enable use of a wider range of dental materials. The second part of the series will focus on the materials, which have been adopted because of these advances in technology.
A key innovation that facilitated the adoption of such new materials has been the introduction of the concept known as the digital workflow, a sequential process utilising a combination of data, guidelines and tasks to streamline a process for optimal productivity. While the digital manufacturing process is routinely used in laboratories, up until recently, CAD-CAM systems have largely been used to design and fabricate fixed prostheses. More recently, advances in this workflow facilitate their use in the fabrication of removable prostheses.1
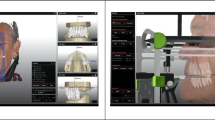
Unlike the conventional workflow in which an analogue impression is taken using impression materials, the digital workflow starts with the acquisition of a digital impression to replicate the patient's intraoral hard and soft tissues. This can be achieved using one of three methods: an intraoral scanner directly digitising the intraoral hard/soft tissues, the scanning and digitising of an analogue impression, or scanning and digitising of the master cast.1 The clinician and laboratory technicians then use software to design the RPD framework digitally. This process involves all the technical steps necessary in conventional prosthodontics including surveying, outlining saddle areas, denture support, retentive features etc. These steps are carried out using digital dental software, conveying advantages such as speed and reproducibility. In addition, it also allows all the information to be displayed on a single image, enabling the clinician to visualise the denture design with greater ease, and enhances communication between the laboratory and clinician (Fig. 1).2 This digital design can facilitate the provision of a trial denture should this be required as part of the planning of the case.

Images showing the design process using a digital workflow. a) Analysing hard and soft tissue undercuts. b) Mapping of saddles and provisional outline of framework. c) Finished framework design
Following the design process comes the fabrication steps, which include several advanced manufacturing processes that have been common in the industrial setting for precision components for many years. These manufacturing processes can be subcategorised into two groups: reductive manufacture, such as milling, and additive manufacture, such as printing and laser sintering. These will be discussed further later in the paper.1
While conversion to such a digital workflow requires a significant financial investment at the outset, it also confers numerous advantages. The adoption of such high-precision CAD-CAM technology is 'expected to improve the fit, aesthetics and functional components of RPDs while reducing costs and labour, thus increasing efficiency and manufacturing outcomes'.3 One other such advantage is that it readily allows the introduction of newer materials, which previously could not be processed within most commercial dental production laboratories. Once the denture has been completed, the final CAD image can be stored digitally. This could then be utilised to manufacture a second denture with relative ease should the denture be lost or broken.
A significant obstacle in the application of the partial denture workflow was the difficulty and high costs associated with manufacturing the metal framework. However, this workflow is well suited to the application of newer materials as well as novel means of manufacturing more traditional materials.
History of denture manufacturing
Traditionally, dentures have been fabricated using two framework material types: polymethyl methacrylate (PMMA) or cobalt-chrome (CoCr).
Metal partial denture frameworks have been manufactured using the lost-wax casting technique.4 This is one of the oldest techniques for manufacturing metals and is used widely in dentistry to construct fixed and removable prosthodontic frameworks. The laboratory processing stages are outlined in Figure 2. This process, however, is not without its disadvantages. This is a demanding and highly technique-sensitive process, with the possibility for errors to be introduced at each stage.5 The construction of frameworks in the conventional manner is heavily dependent on technician skill, with small errors potentially leading to altered properties of the material.6 Indeed, Rudd and Rudd identified up to 243 potential errors in the fabrication of an RPD and made recommendations on how to avoid or overcome these.6,7,8 Many of the errors discussed could still occur when a digital workflow is adopted; however, many are related to human error and therefore would be reduced using CAD-CAM.

Lost-wax casting technique laboratory process
If the metal alloy is not sufficiently heated, it may not fill in the form totally. Conversely, if heated up too much, it might cause the investment material to crack. Similarly, if the metal alloy is cooled too quickly, this can also lead to deterioration of the material's properties.
As with manufacturing of metal frameworks, the laboratory stages for constructing conventional PMMA dentures are a similarly laborious process, with the potential for multiple errors (Fig. 3). Porosities can be introduced in the denture base during polymerisation where monomer contraction, evaporation of the monomer or poor temperature control has occurred. These porosities can have deleterious effects on the denture base properties. Extensive porosities weaken the prosthesis, promote staining, make polishing challenging, encourage colonisation of oral microorganisms, and affect the bond strength between the artificial teeth and denture base resin.9

Conventional laboratory process for construction of acrylic prostheses
The above techniques have been used for many years, with little change and innovation. We now have the opportunity to embrace digital technology, which opens the doors to innovations in techniques and materials.
Novel manufacturing techniques
The conventional techniques discussed above are not easily transferable to novel non-metal materials, such as aryl ketone polymer (AKP; these will be discussed in more detail in part two). The closest comparable application for polymeric materials to the lost-wax casting process would be a lost wax pressing technique. This type of manufacturing process may be used in the fabrication of certain ceramic materials such as lithium disilicate in fixed prosthodontics - eg IPS e.Max Press (Ivoclar Vivadent). However, with the high-impact polymer materials described in part two of this series, the effect of temperature on additives and polymer structures can preclude the use of lost-wax pressing of partial denture frameworks due to the deleterious effects upon material properties.
To simplify this next section, the methods of construction have been broadly divided into two categories: reductive manufacturing and additive manufacturing (Table 1).
Reductive (or subtractive) manufacturing
Reductive manufacturing, as the name indicates, is a means of production whereby there is the physical removal of material from a prefabricated block. In the construction of denture frameworks and baseplates, reductive manufacturing typically uses computer-controlled milling.10
Milling
Milling is the technique by which denture frameworks are cut from a block of the chosen material by a computer numerical controlled (CNC) machine. The CAM software utilises a CAD model to dictate the sequencing, tools, and tool motion, direction and magnitude.10 In dentistry, three-axis milling systems are most commonly used, allowing the burs to move in three axes (x, y and z). The computer programs the machine for the process to be undertaken in the most efficient way, thereby reducing milling time. Milling can be advantageous due to its reduction in manufacturing deficiencies such as porosities and inhomogeneous consistencies, the latter being avoided as the framework/denture is being milled from a consistent block of the same material.10
While used commonly in fixed prosthodontics, milling is less widely used with removable prosthodontics. This is partly due to it not necessarily being the most appropriate technique for RPDs since their components can have complex shapes and varying thicknesses. Milling does not provide the accuracy of laser sintering, as the cutting tools have specific thickness limitations that in turn constrain accuracy.11 A large proportion of the literature is focused on the accuracy of fixed prosthesis. Tooth-supported restorations manufactured by conventional methods tend to exhibit better fit than milled restorations. It has been found that milled titanium crowns exhibited larger marginal opening than cast titanium crowns.12 In addition, lithium disilicate milled veneers have been found to exhibit marginal gaps twice the size of those of pressed veneers, contributing to increased microleakage.13 Whilst this shows casting has a better degree of accuracy than milling, further in vitro and clinical research is required to determine whether this can be applied successfully to the intricacies of complex RPD designs..
When milling, attachment points are maintained between the block and the milled denture which allow for the cutting components to approach the material from different angles (Fig. 4). It can be a challenge to establish an appropriate attachment point with the milling machine; therefore, components can suffer deflection during the process.14 There may also be deformation or breaking at thin or narrow areas during manufacturing.15

RPD milled from AKP showing the attachment points between the framework and AKP block
Despite its relative success, this technique has proven uneconomical when used for the construction of RPDs made of base metal alloys, as the materials rapidly wear the machining tools. Milling of blanks with high hardness requires heavy cutting forces for efficient milling. Titanium and densely sintered zirconia have high material hardness and therefore generate higher thermal energy, which reduces the life span of the tools as well as making them more susceptible to failure and wear.10 As such, for milling to be an economically viable option, it may be used with alternate denture materials, such as high-impact materials like polyetheretherketone (PEEK) and polyetherketoneketone (PEKK), or in the fabrication of a milled framework in a burnout plastic, which can be used in a conventional lost-wax casting technique.
Additive manufacturing
Additive manufacturing, also known as three dimensional (3D) printing, uses CAM to generate a physical 3D structure constructed by depositing successive layers of material which are fused into precise predetermined shape in a passive production.1 As with reductive manufacturing, additive manufacturing can be utilised in removable prosthetics in many ways; it can be used to fabricate a pattern in a suitable burnout plastic material, which is then used in the traditional lost-wax process or can be used to directly fabricate a prosthesis in a definitive material. This allows for the elimination of the waxing step and therefore reduces the potential for errors as discussed in the introduction.14
One common term that is often encountered when discussing additive manufacturing is rapid prototyping (RP). It is often used interchangeably with terms such as 3D printing; however, they are different. RP is an application of additive manufacturing technology, rather than being the method itself. By definition, RP is 'a general term used for several additive layer manufacturing techniques'16 (Fig. 5).

a, b) CAD used to 3D-print a complete denture base. c) A guide can then be used to aid tooth positioning which is added using conventional techniques by a technician
Rapid prototyping
RP is a technique by which the denture framework may be constructed using 3D printers. While CAM is already widely used within the fabrication of all ceramic fixed prostheses, its use for metal frameworks is still novel. Initially, RP was utilised for polymer denture bases; however, advances in technology have now enabled its use to fabricate the RPD metal framework directly.14
In addition to its use with novel polymer base dentures, the use of RP may also be used for manufacturing CoCr alloy metal frameworks.14 While this technique may be used for metals such as titanium, it has notable shortfalls, such as its inability to rapidly prototype titanium clasps, which need to be cast then laser-welded onto the framework.17 Commonly used RP techniques include stereolithography (SLA), selective laser melting (SLM) and selective laser sintering (SLS).
Stereolithography
SLA was the first documented technique to construct resin frameworks, utilising ultraviolet laser beams to solidify photosensitive liquid resin layer by layer into a 3D polymer.17 The framework is then rinsed with solvent and cured in an ultraviolet oven. This technique is utilised in prosthodontics to print patterns, thereby eliminating any human error associated with manual wax-ups. Computing errors are still a problem, however, and are still to be fully eliminated.18 These 3D patterns can then be used to cast alloys using conventional methods.17,19 The performance of these resins can be greatly influenced by the power, wavelength and type of laser used, physical and chemical properties of the photopolymer resins, along with the speed and resolution of the scanning systems.19 The use of photopolymerisation processes such as SLA presents a reproducible and consistent technique, which is a more cost-effective option for laboratories where a higher-priced SLM machine is not feasible. It can, however, be a time-consuming process with multiple casting steps still required.17,19
SLA requires special supports to hold the prosthesis during the printing process which requires planning and removal after fabrication, both of which can be time-consuming.18
Selective laser melting
SLM is 'an additive CAM continuous layering build-up process in which elemental metal or alloy powder deposition is closely followed by laser melting to create a finished shape under computer control'.16
Originally introduced in the aerospace and automotive industries and later adopted into medicine and dentistry, SLM produces metal components directly from a 3D CAD model. A targeted high-power laser beam applies heat to fine layers of metal or metal powder. This results in local melting and fusing of the particles (Fig. 6).

SLM technique for construction of partial denture framework. The roller spreads the metal powder onto the production platform where it is then melted in layers using the laser to produce the denture framework. The powder which has not been lasered is removed and can be reused reducing waste. Image courtesy of Colin Sullivan
While SLM requires a high initial cost, it performs better than milling and casting techniques in primary economic areas: labour, time, waste of materials and consumables, recycling and productivity. The technique eliminates many physical manufacturing steps including spruing, investing, burnout, casting and devesting. Of note, being a technique reliant on CAD, the quality of outcome is hardware- or software-dependent, owing its performance to the ability of the 3D CAD file to be reproduced. Conversely, traditional casting is a more technician-dependent fabrication technique.11 Furthermore, being digital does not solve all potential sources of error. SLM is technique-sensitive, given the multiple variables, and hence does not solve all the potential sources of error.
Alloy properties need to be considered, such as melting temperature, laser beam absorption/reflection coefficients and thermal conductivity.11
Aside from efficiency, the metal itself has superior qualities compared to traditional casting. Casting is a technique that often encounters technical errors, including internal porosity and possible distortion of cast structures.11 CoCr frameworks manufactured with SLM meanwhile have a more homogenous microstructure due to local melting and rapid solidification of metallic power. Increased homogeneity and small grain size, in turn, leads to improved mechanical properties and fatigue resistance.20 These superior physical properties benefit the clinician and patient. This has even been found to confer a higher patient satisfaction.18 Thus, the result is not only less labour-intensive but also a framework with superior properties.19
Selective laser sintering
The Journal of Prosthetic Dentistry defines SLS as 'an additive CAM technique of sintering plastics, glass or ceramics into 3D structures'16 (Fig. 7).

RPDs manufactured using Renishaw plc's selective laser sintering equipment. These will then be finished and polished conventionally by a technician. Image courtesy of Renishaw plc.
SLS shares many of the advantages of SLM, including the elimination of many labour-intensive stages. In SLS, a computer-directed CO2 laser is used to selectively fuse powdered material into a 3D model. Each layer is selectively sintered based on data provided by a CAD file before being lowered and a further layer of powder is spread. This continues until the entire object is constructed.21 While SLM involves full melting of metal powder into a homogenous part, SLS leads to fusing on a molecular level, enabling its use for various thermoplastic materials.21 As the fabricated object is supported by powdered layers, unlike in SLA, no special support material is required, allowing construction of complex geometric patterns and ease post-processing.22 On completion of production, the powder that has not been scanned and fused is removed; this can then be reused, thus reducing the high levels of waste typical in other manufacturing techniques such as milling.22
The major advantage of SLS is the large range of materials that can be used.22 This has enabled the use of novel materials within prosthodontics. While SLS requires a significant capital investment, it allows for quick fabrication of removable prostheses with high precision and at a low running cost.20 Both SLM and SLS allow customised prostheses without extensive manual pre- or post-processing steps.17
Compared to frameworks fabricated by conventional casting methods, those fabricated by SLS show superior fatigue resistance and improved mechanical properties.20 The SLS system can manufacture components as small as 0.5 mm and therefore produces highly accurate prostheses.22
Discussion
While being familiar with the various manufacturing methods will give the clinician an insight into their role in modern prosthodontics, it is important to be able to differentiate the relative merits and disadvantages of adopting them into practice. By this stage, the reader should be familiar with conventional processing techniques and the shortfalls they may introduce. This section will therefore aim to objectively look at the advantages and disadvantages of modern manufacturing techniques.
Advantages
The use of CAD has transformed the ease at which denture design can be undertaken. Where previously a dental surveyor was required to determine the path of insertion, analyse the depth of undercut and analyse prosthetic space, this can now be carried out via the digital software (Fig. 1). This digital design simplifies the fabrication process, saving time and improving communication, allowing for collaborative discussions between patient, clinician and technician. In addition, this allows for replication or replacement of a denture with the same design without the need to restart the process.18
The ability to digitally design and mill the framework is more time-efficient and less technique-sensitive than lost-wax casting. Furthermore, CAD-CAM allows the production of a highly precise prosthesis.23 This does, however, come at an increased cost compared to the traditional lost-wax technique.24
Conventional fabrication techniques for metal-free denture materials include compression moulding, injection moulding and fluid resin technique. However, with the development of digital techniques, these may now be fabricated by milling and, in the case of nylon-based polyamide materials, 3D printing.18 Digital production has enabled the use of novel metal-free denture materials, which can overcome some of the limitations of current metal RPDs.25
Additionally, digital production can be more environmentally friendly due to reduced waste of alloy, wax and investment materials, and the recycling potential of uncured metal power after SLS.18 Additive manufacturing techniques also allow for the production of large objects with detailed morphology, irregularities, undercuts and voids.10
The accuracy of CAD-CAM-fabricated RPDs is an evolving and progressing field. Anecdotally, it appears that the outcomes have been good. However, there is a limited amount of literature to support these claims. A 2020 systematic review of the literature included only seven studies.26 Six of these studies explored the differences between conventional manufacturing methods with different digital techniques and different materials, looking into the overall gaps (the mean discrepancy between the frameworks and the reference cast). A gap from 0-50 μm was considered close contact (no gap) and a gap from 50-311 μm was defined as a clinically acceptable gap. The results concluded that the digital technique for RPD framework manufacturing was accurate, with the fit of the frameworks being within acceptable limits, albeit still less accurate than conventional techniques.26
Another clinical evaluation of nine RPD frameworks evaluated SLS frameworks made from either an intraoral scan or an optical scan of the cast and found that both digital workflows resulted in fewer inaccuracies than the traditional laying down of a wax pattern and lost-wax casting workflow for CoCr frameworks.27
Disadvantages
CAD-CAM is not without its detractors, and some practitioners of removable prosthetics still question the viability and practicality of intraoral scanning of soft tissues. While scanning of teeth and implant components intraorally has proved to be successful, the ability to record digitally the soft tissue contours of edentulous saddles and the functional width and depth of sulci is proving to be more challenging. This could introduce errors that might not arise were the impressions cast in a conventional manner.28
While digital workflows are becoming more frequently utilised, they have not yet completely replaced the analogue workflow as shortcomings remain. The initial cost of the machines is high, and it requires time and expertise to learn to use them appropriately.18 In addition, while the technology allows for fabrication of frameworks, tooth setup, finishing and polishing still need to be carried out manually as in conventional casting techniques (Figures 4 and 8).18

Finishing and polishing of an AKP denture
The staircase effect can be another limitation, occurring due to the layering nature of additive manufacturing, which then produces an external surface with a stepped and coarse morphology. Reducing layer thickness and width of the curing beam can act to improve this; however, this leads to an increased production time.18
Conclusion
The use of digital workflows for partial denture fabrication is increasing, with a number of commercial laboratories now offering this service. This paper aims to inform the reader of the different available techniques for RPD manufacturing. Traditional casting with the lost-wax technique is not conducive to manufacturing with novel materials and therefore advances in digital production have enabled use of a wider range of materials. Digital production has many advantages and current scientific evidence appears promising.
References
Bilgin M, Baytaroglu E, Erdem A, Dilber E. A review of computer-aided design/computer-aided manufacture techniques for removable denture fabrication. Eur J Dent 2016; 10: 286-291.
Wu J, Wang X, Zhao X, C Z, Gao B. A study on the fabrication method of removable partial denture framework by computer-aided design and rapid prototyping. Rapid Prototyp J 2012; 18: 318-323.
Campbell S, Cooper L, Craddock H et al. Removable partial dentures: The clinical need for innovation. J Prosthet Dent 2017; 118: 273-280.
Arnold C, Hey J, Schweyen R, Setz J. Accuracy of CAD-CAM-fabricated removable partial dentures. J Prosthet Dent 2018; 119: 586-592.
Diwan R, Talic Y, Omar N, Sadig W. Pattern waxes and inaccuracies in fixed and removable partial denture castings. J Prosthet Dent 1997; 77: 553-555.
Rudd R, Rudd K. A review of 243 errors possible during the fabrication of a removable partial denture: part I. J Prosthet Dent 2001; 86: 262-276.
Rudd R, Rudd K. A review of 243 errors possible during the fabrication of a removable partial denture: Part II. J Prosthet Dent 2001; 86: 262-276.
Rudd R, Rudd K. A review of 243 errors possible during the fabrication of a removable partial denture: part III. J Prosthet Dent 2001; 86: 277-288.
Ghani F, Moosa R. Effect of Curing Methods and Temperature on Porosity in Acrylic Resin Denture Bases. J Pak Dent Assoc 2012; 21: 127-135.
Abduo J, Lyons K, Bennamoun M. Trends in computer-aided manufacturing in prosthodontics: a review of the available streams. Int J Dent 2014; 2014: 783948.
Koutsoukis T, Zinelis S, Eliades G, Al-Wazzan K, Rifaiy M, Al Jabbari Y. Selective Laser Melting Technique of Co-Cr Dental Alloys: a review of structure and properties and comparative analysis with other available techniques. J Prosthodont 2015; 24: 303-312.
Han H, Yang H, Lim H, Park Y. Marginal accuracy and internal fit of machine-milled and cast titanium crowns. J Prosthet Dent 2011; 106: 191-197.
Abduo J, Lyons K, Swain M. Fit of zirconia fixed partial denture: a systematic review. J Oral Rehabil 2010; 73: 866-876.
Lima J M, Anami L C, Araujo R M, Pavanelli C A. Removable Partial Dentures: Use of Rapid Prototyping. J Prosthodont 2014; 23: 588-591.
Ye H, Ning J, Li M et al. Preliminary Clinical Application of Removable Partial Denture Frameworks Fabricated Using Computer-Aided Design and Rapid Prototyping Techniques. Int J Prosthodont 2017; 30: 348-353.
Anonymous. The Glossary of Prosthodontic Terms: Ninth Edition. J Prosthet Dent 2017; DOI: 10.1016/j.prosdent.2016.12.001.
Quadri S, Kapoor B, Singh G, Tewari R. Rapid prototyping: An innovative technique in dentistry. J Oral Res Rev 2017; 9: 96-102.
Almufleh B, Tamimi F, Caron E, Alageel O. 3D-Printed Removable Partial Dentures. In Digital Restorative Dentistry. pp 95-114. Switzerland: Springer, 2019.
Alifui-Segbaya F, Williams R, George R. Additive Manufacturing: A Novel Method for Fabricating Cobalt-Chromium Removable Partial Denture Frameworks. Eur J Prosthodont Restor Dent 2017; 25: 73-78.
Alageel O, Abdallah M, Alsheghri A, Song J, Caron E, Tamimi F. Removable partial denture alloys processed by laser-sintering technique. J Biomed Mater Res B Appl Biomater 2018; 106: 1174-1185.
Torabi K, Farjood E, Hamedani S. Rapid Prototyping Technologies and their Applications in Prosthodontics, a review of literature. J Dent (Shiraz) 2015; 16: 1-9.
Liu Q, Leu M C, Schmitt S M. Rapid prototyping in dentistry: technology and application. Int J Adv Manuf Technol 2005; 29: 317-335.
Benakatti V, Sajjanar A, Acharya A. Polyetheretherketone (PEEK) in Dentistry. J Clin Diag Res 2019; 13: 10-12.
Harb I, Abdel-Khalek E, Hegazy S. CAD/CAM Constructed Poly(etheretherketone) (PEEK) Framework of Kennedy Class I Removable Partial Denture: A Clinical Report. J Prosthodont 2019; DOI: 10.1111/jopr.12968.
Gray D, Barraclough O, Ali Z, Nattress B. Modern partial dentures - part 2: a review of novel metal-free materials and innovations in polymers. Br Dent J 2021; in press.
Pereira A L C, de Medeiros A K B, de Sousa Santos K, de Almeida É O, Barbosa G A S, da Fonte Porto Carreiro A. Accuracy of CAD-CAM systems for removable partial denture framework fabrication: A systematic review. J Prosthet Dent 2021; 125: 241-248.
Tregerman I, Renne W, Kelly A, Wilson D. Evaluation of Removable Partial Denture Frameworks Fabricated Using 3 Different Techniques. J Prosthet Dent 2019; 122: 390-395.
Kattadiyil M, Mursic Z, AlRumaih H, Goodacre C. Intraoral scanning of hard and soft tissues for partial removable dental prosthesis fabrication. J Prosthet Dent 2014; 112: 444-448.
Author information
Authors and Affiliations
Contributions
Dr Olivia Barraclough, Dr David Gray, Dr Zaid Ali and Professor Brian Nattress have all equally contributed to writing and editing this manuscript.
Corresponding author
Ethics declarations
The authors declare no conflicts of interest.
Rights and permissions
About this article

Cite this article
Barraclough, O., Gray, D., Ali, Z. et al. Modern partial dentures - part 1: novel manufacturing techniques. Br Dent J 230, 651–657 (2021). https://doi.org/10.1038/s41415-021-3070-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-021-3070-4
- Springer Nature Limited