
Abstract
This paper aims to update the reader on how minimally invasive (MI) techniques may be used to improve the longevity of carious or defective/compromised first permanent molars (cFPMs) in young children. Clinical and radiographic diagnosis and the prognostic factors will be discussed in view of recent studies showing that these teeth can be kept in function and have an improved prognosis as the child gets older. Clinical protocols for their care, based on the latest evidence and techniques for MI restorations, together with longevity information of possible restorative options, are described. This paper also explores the rationale behind enforced extractions and related morbidity, in order to help oral healthcare practitioners to determine the optimal management of these key elements in the dentition for the benefit of the patients.
Key points
-
Dental practitioners treating young children frequently face cavitated carious or hypomineralised first permanent molars in their clinical practice.
-
The use of improved minimally invasive techniques and materials, such as high-viscosity glass ionomers, may improve the prognosis of compromised first permanent molars in young children and reduce the need for extractions under general anaesthesia.
-
Compromised first permanent molars may be able to survive longer in the oral cavity of young children, postponing definitive restorative treatment for later in life.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Compromised first permanent molars with caries or enamel defects (cFPMs) are a challenge to manage in children. In fact, there are few varied restorative guidelines to follow, leaving practitioners to weigh up the pros and cons of restoration vs extraction, without clear guidance about how the judgement of poor prognosis is derived. This dilemma and uncertainty about the long-term prognosis of these teeth leads to inconsistencies in the ethos of care and a disparity of treatment offered.1 Only orthodontic guidelines about the optimal time for extraction of cFPMs that are already judged to be of 'poor' prognosis are available2,3 and the result is that clear differences in treatment options offered to patients are observed worldwide. In France, for instance, only 26% of paediatric dentists would extract a cFPM in a nine-year-old child,4 compared to 58% of specialists indicating extractions in the UK.1
Scientific evidence has shown that the caries process can be arrested at any stage, with dietary and biofilm control/modulation, even in the presence of cavitation.5 Arrested caries and mild enamel defects will probably remain lifelong 'scars', while extraction can be considered as a physical 'amputation'. So, practitioners are faced with the decision to either maintain a 'scarred' tooth or plan for extraction at the optimal time to achieve post-eruptive space closure, balancing the burden of lifelong restorative care against a costly and painful hospital general anaesthetic (GA) admission. A recent report from one of the largest dental hospitals in the UK showed that 19.4% of the paediatric patients undergoing GA had extractions of cFPMs. Interestingly, in 36% of the children undergoing first permanent molar (FPM) removal, the most severe teeth extracted had radiographic changes limited to the outer/middle third of dentine.6 Thus, the dilemma to be addressed is: what should be done with the mild/moderate cases of cFPMs? Does the patient really need prophylactic removal of these teeth? How does one define clinically a 'mild'/'moderate' case? What is the expected longevity/cost of the restorations placed in those situations? This manuscript intends to discuss how minimally invasive (MI) techniques could be applied to help practitioners to more effectively establish prognosis of cFPMs in children by increasing the longevity of the restorations and reducing the amount of GA extractions.
Determining the prognosis of cFPMs based on clinical and radiographic findings
Caries susceptibility in FPMs decreases with the patient's age, as the occlusion develops. There is a significant reduction in occlusal biofilm accumulation in erupting first molars at the age of six compared to fully erupted first molars at the age of 12.7 This reduction is even greater by 15 years of age.8
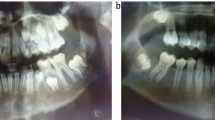
Hypomineralised enamel in FPMs affects approximately 14% of the worldwide population,9 but it is generally confined to the outer 2/3 of the crown, leaving the cervical enamel intact.10 The defective enamel is more porous, has fewer distinct morphological features and is less mineralised than normal.10,11 Hypomineralisation defects have a multifactorial aetiology, involving both environmental and genetic causes such as common childhood illness, pyrexia and infection,12 single-nucleotide polymorphisms of enamel formation genes13 and immune response regulators.14 The more clinically stained (darker) the enamel, the more severely affected it is, and this is when tissue breakdown generally begins.15,16 However, hypomineralised defects often appear much 'worse' clinically than they do radiographically. These findings suggest that a large proportion of the tooth is structurally sound. Figure 1 shows examples of extracted FPMs showing hypomineralisation defects and the corresponding radiographic image.

Clinical and radiographic criteria for interim treatment options and needs in cFPMs. a) Mild case: localised white creamy and/or yellow-brown discolourations (white arrows) without post-eruptive breakdown (PEB) or carious cavitation. No radiographic signs/changes restricted to the enamel-dentine junction (black arrow). b) Moderate case: yellow-brown discolourations with enamel-restricted PEB. Radiographic changes are restricted to outer dentine (black arrow). c) Severe case: discolourations merging into PEB or cavitation involving dentine. Atypical restorations may be present. Radiographic involvement into middle third of dentine or beyond (red circle). Generally, the radiographic involvement in hypomineralised teeth is less than would be expected for equivalent carious teeth
Table 1 collates a description of radiographic signs/symptoms and histology to categorise the severity/restorability of cFPMs based on the Scottish Dental Clinical Effectiveness Program (SDCEP) clinical guidance,17 the radiographic International Caries Detection and Assessment System (ICDAS)18 and a hypomineralisation scoring system,19 in order to provide an evidence-based management guide for practitioners.
It is important to take into consideration the severity of cFPMs in relation to the ability of the patient to cooperate with dental treatment. In this regard, a pragmatic clinical study managed cFPMs in children according to the severity of the defects, level of cooperation of the child, sensitivity and the possibility of achieving adequate moisture control. Their results showed that after 24 months of follow-up, 77% of teeth showing post-eruptive breakdown (PEB) in only one or two surfaces and 54% of those showing extensive PEB (severe defects) restored with resin composite did not need re-intervention. For glass-ionomer cement (GIC) restorations, these numbers were 47.8% and 40.2%, respectively. The mean time for first retreatment was 18 months for resin composite and 12 months for GIC restorations.20 Refer to Figure 1 for examples of mild, moderate and severe hypomineralised cFPM cases.
Choice of restorations for cFPMs
There is growing clinical and scientific evidence that MI operative techniques should be used to restore cFPMs.21 The improved adhesion and mechanical properties of modern bio-interactive dental restorative materials, techniques and standards for selective carious dentine removal, and the use of fluoride compounds that enhance resistance to tissue dissolution mean that retaining these teeth could be less traumatic for the growing adolescent, allowing them to serve in function for many more years.22 Dentine subjacent to hypomineralised enamel seems to have similar adhesive properties to unaffected teeth,23 possibly explaining the low failure rates or loss of complete restorations in severely affected teeth.24 Available evidence shows that direct resin composites have a 60% success rate in cFPMs in eight-year-olds after 18 months,25 while cast metal or indirect resin composite restorations have an 87.6% success rate in cFPMs of 8-13-year-olds after 36 months.26 Finally, conventional GIC restorations have a 40% success rate in cFPMs in 5-10-years-old after 24 months,20 while survival rates for high-viscosity GICs in FPMs of 6-9-years-old are 78% after 12 months.27
If these compromised teeth could be restoratively managed and kept in function for some more years, by the time the patient reaches adulthood, they could then be treated with a more definitive restoration, improving thus the overall longevity of the final tooth-restoration complex.
As the 8-10-year-old child grows older and becomes more emotionally mature, behaviour control during dental treatment becomes less of an issue and dental treatment may be accomplished without the need for hospital-based interventions.
Longevity of the tooth-restoration complex
The measures of success of MI restoration of cFPMs are restoration longevity and tooth survival (retention in function). The MI restoration also needs to maintain anatomical form as well as provide marginal adaptation and suitable surface texture, and there are well known criteria used to evaluate this, such as the United States Public Health Service (USPHS)28 and World Dental Federation (FDI) criteria.29 The standards for good-quality restorations can be kept by application of the MI management options for reviewing restorations (the so-called five Rs [5Rs]): review, refurbishment, resealing, repair and replacement.30
A study of the longevity of restorations performed in molar teeth (regardless of caries/defects), including more than three million patients and more than 25 million courses of dental treatment undertaken in the UK, reported that 83% of the molars were kept in function for 15 years after being restored. When the teeth were restored at 18 years of age, 90% of them survived in function for >15 years. Sub-grouping into specific restorative materials, 96% were resin composite-restored molars, 93% were GIC-restored molars and 85% were full-coverage crowned molars, which had survived extraction for ten years after restoration.31
MI techniques for cFPMs
If the child and family are willing to keep cFPMs during the childhood period into adolescence, periodic annual review and control will be necessary to review the restorations using the MI '5Rs' principles.30 GDPs have a key role here in 'topping up', and keeping good-quality restorative work and tooth function during this period. See Table 2 for a summary of MI treatment protocols to manage cFPMs in young children.
Non-invasive caries control and remineralisation/desensitisation of hypomineralised teeth
First-line care planning for children presenting with cFPMs should include the basic prevention guidelines stated in the Delivering better oral health toolkit.32 Effective tooth brushing last thing at night and at least on one another occasion during the day with a fluoridated toothpaste (1,350-1,500 ppm, age-dependent) and reducing the frequency and amount of sugary food and drinks should be encouraged for all patients.
Young patients with cFPMs frequently have oral hygiene issues due to the sensitivity of the affected teeth and position of the teeth dependent upon eruption stage. These factors make tooth-brushing procedures difficult for the child/carer and favours undisturbed biofilm accumulation. Although currently opinion-based, sensitivity issues in cFPMs can be managed with casein phosphopeptide-amorphous calcium fluoride/phosphate (CPP-ACF/CPP-ACP), painted over the affected tooth surface by the child/parent immediately after conventional tooth-brushing procedures before bedtime for a minimum of eight weeks. There is still poor evidence that remineralisation therapy with CPP-ACF/CPP-ACP is effective in this regard. Only one in vitro study has shown that the degree of mineralisation can be improved in hypomineralised enamel by the application of CPP-ACF,33 and two in vivo studies have reported improvements in the sensitivity of molar-incisor hypoplasia (MIH)-affected teeth after CPP-ACP paste application (GC Tooth Mousse, GC, Tokyo, Japan).34,35
Micro-invasive caries control (fissure sealants)
Another strategy to improve sensitivity and help in reducing biofilm accumulation is the application of fissure sealants. If there is no sensitivity and moisture control can be achieved effectively, conventional resin-based sealants are the best treatment option for mild cases, where PEB is not (extensively) present (Fig. 2a). For cases of partially erupted and/or sensitive cFPMs, a fissure sealant performed with conventional GICs using the 'finger-pressing' technique may be a good interim option to keep the patient pain-free and stimulate/allow effective biofilm control.36 GICs are more hydrophilic than resin-based materials and therefore are less technique-sensitive to moist environments, while they also do not need strong acid etching before application, which very frequently causes poor child cooperation during such a simple dental procedure (Fig. 2b). It is advised to manually and professionally clean the relevant tooth surface and condition the surface with 10% polyacrylic acid for 20 seconds before placing the GIC sealant.

Examples of treatment options for cFPMs of different severities. a) Mild case: treated with resin (or glass-ionomer)-based sealants, depending on moisture control and sensitivity to cold air/water/acid. b) Moderate case: treated with restoration/fissure sealant with a glass hybrid GIC (Equia Forte, GC Corporation). c) Severe case: where sensitivity is present, managed with SDF application (Riva Star, SDI) and a glass hybrid restoration over the exposed dentine
Carious tissue removal
The tenet behind the contemporary operative management of carious tissue has moved away from the classic surgical 'drill and fill' pathway of treatment (non-selective carious dentine removal to hard, sound tissue), with its related consequences including pain, unnecessary removal of tooth structure and an increased risk of pulp exposure. MI selective tissue excavation is evidence-based, and demands an individualised judgement by the clinician and shared decisions with patients and parents.37
Contemporary carious dentine removal advocates three main protocols which can be applied to the treatment of cFPMs, including:38
-
1.
Selective tissue removal to firm dentine: cavity margins and peripheral dentine are excavated until hard (scratchy) dentine is reached. Carious tissue from the pulp floor is removed until 'leathery' dentine is found; in short, residual dentine is left after the feeling of resistance to a hand excavator. This is the treatment of choice for shallow or moderately deep dentine lesions (radiographically extending no deeper than the middle third of dentine)
-
2.
Selective removal to soft dentine: recommended in deep cavitated lesions (extending into the pulpal third or quarter of the dentine) in teeth with vital pulps. Again, peripheral tissues are prepared to hard dentine where possible, to allow an optimal adhesive peripheral sealing. However, soft carious tissue is left over the pulp to avoid exposure and 'stress' to the pulp
-
3.
'Stepwise' removal of carious dentine: this precludes a two-stage intervention where selective removal to soft dentine is performed on the first visit, after which an interim restoration is placed (for example, high-viscosity GIC). After some time (3-9 months), the restoration is removed and the previously retained carious dentine, which is now arrested, is removed until firm dentine is reached. There is clinical evidence, however, that the second procedural stage may be omitted, as it increases risk of pulp exposure, adds additional cost, time and potential discomfort to the patient, and has been rendered unnecessary by modern bio-interactive materials that can seal and heal the underlying tissues. This MI operative management principle may be applied directly to those cases of cFPMs with cavitation/PEB in children during the early mixed dentition period (6-9 years) as a way of achieving stabilisation of the teeth until the patient further develops to comply with more definitive treatments.
Glass hybrid restoratives
More recently, hybrid materials based on GIC technology have evolved by the introduction of ultrafine, highly reactive glass particles dispersed within the conventional glass-ionomer structure and a higher-molecular-weight polyacrylic acid.39 Furthermore, application of a nano-protective, multi-functional monomer coating produces a tougher resin matrix, improving the material's properties.40 Improvements in adhesive and mechanical properties of these GICs could be applied to manage cFPMs in children. A prospective clinical trial showed 98% survival rate (based on longevity criteria for ART restorations) of a glass hybrid restorative material placed upon hand-excavated carious/defective tooth tissue after 12 months,41 which is better than a previous trial using high-viscosity GICs to treat hypomineralised teeth (78%).27 Thus, glass hybrid restoratives are certainly showing potential to increase the 'short-term' prognosis of cFPMs in young children until they are ready for a more definitive restorative intervention.
Resin composite restorations
It is known that the longevity of the dentine/adhesive bond interface is related directly to the quality of the hybrid layer that connects the dental adhesive to the subjacent dentine. Current dental adhesives/bonding agents bond to dentine via this hybrid layer, which is formed when adhesive resin primers penetrate the demineralised dentine, infiltrating the exposed collagen fibre network to create a continuous integrated collagen/resin lattice that bonds the bulk adhesive to the intact dentine.42
In laboratory studies, conventional adhesives may exhibit higher immediate bond strengths to caries-affected dentine compared to self-etch adhesives,43 but both have similar long-term bond strengths to sound dentine.44 The dentine subjacent to hypomineralised enamel does not seem to be affected with respect to its adhesive properties23 and this may explain the low rates of complete restoration loss in hypomineralised teeth.24
On the other hand, bonding to hypomineralised enamel offers reduced adhesion strengths when compared to sound enamel.23,45 A recent clinical trial, using well-defined restoration longevity criteria (USPHS), documented the two-year longevity of resin composite restorations performed on hypomineralised molars,46 where the cavity preparation included only removal of the soft, 'cheese-like' enamel. The success rates (58.1%) were lower compared to when all the hypomineralised enamel was removed (81.2%), approaching the success found in sound enamel (87.1%). Conservative MI removal of soft enamel followed by treatment with 5% NaOCl increased the success rates to 78.1%. Overall, almost half of the compromised molars survived two years in a 'perfect' restored condition.
Other studies have reported cumulative 18-month survival rates of 68.4% and 54.6% for resin composite restorations performed in 6-8-year-old children with conservative hypomineralised enamel removal using self-etch or total-etch adhesives, respectively.25
Silver diamine fluoride
Silver diamine fluoride (SDF) is a clinically applied treatment that, when painted onto teeth, reduces sensitivity, halts active caries and controls further caries progression.47,48 It is licensed to date in the UK for the management of dentine sensitivity only. The main disadvantage of SDF is that carious lesions will be stained black, which may raise aesthetic concerns.49 This discolouration is caused by the oxidation of ionised silver into metallic silver, and is indicative that silver has precipitated on the tooth and the caries process has been arrested.50 Discolouration after one 38% SDF application lasts for up to 24 months, with an average of 12 months.51
In an attempt to combine SDF's property of arresting the caries process as well as masking the poor aesthetic appearance of the black lesions, glass-ionomer restorations have been advocated to cover SDF lesions.52 This approach may be useful in severe cFPMs in children, presenting with acute hypersensitivity. Adhesion between the glass-ionomer material appears not to be impaired by SDF itself53 (Fig. 2c).
Extraction of cFPMs
Conventional restorative procedures and materials are invasive, upsetting for many children to tolerate and their longevity is poor, especially in the worst affected teeth. This is aggravated by the fact that providing adequate analgesia in cases with hypersensitivity is challenging, making it difficult for an 8-10-year-old to accept treatment and impacting adversely the quality of the final restoration provided.54
A recent study into the cost-effectiveness of different treatment options for MIH-affected cFPMs within the German healthcare system has shown that, assuming that spontaneous orthodontic alignment occurs after extraction of severely compromised FPMs, timed extractions are the best practice to reach a functional and sound dentition in the long term.55 However, the term 'severely compromised' is ambiguous and there was no recognised definition. In the UK, the current accepted practice is to extract these teeth when the child is between 8-10 years of age, even though this often means a costly and upsetting hospital GA admission.
Current orthodontic UK clinical guidelines state that the optimal timing for removal of permanent FPMs that are judged to have a poor prognosis is when there is radiographic evidence of the beginning of calcification of the furcation of the second permanent molars, in children with a standard occlusion (angle class I) and when there are no other teeth missing.2,3 Although little guidance is offered for patients with occlusion patterns outside the classic class I, the rationale behind this treatment and the timing of it (normally in 8-10-year-old children) is to facilitate space closure, and one study reported approximately 67% of patients showing spontaneous space closure after extractions.56 However, a recent systematic review has shown that this 'optimal time for extraction of FPMs' is not based upon sound scientific evidence, as all retrieved studies scored 'low' or 'very low' certainty of evidence.57 The consequences are that even carefully considered extractions of cFPMs may still result in an unpredictable outcome.
An improved outcome for spontaneous space closure (85%) has been found if the cFPMs were extracted in cases where the following radiographic characteristics were present:
-
Second premolar is engaged in second primary molar bifurcation
-
Mesial angulation of second permanent molar
-
Third permanent molar present
-
However, the third molar may not be radiographically visible before eight years of age, and thus the confirmation of its presence and subsequent extraction of the cFPM at a slightly later age (but before half the root of the second permanent molar is fully developed) may result in favourable outcomes while prediction of this is poor58
-
Fifteen percent of the patients with MIH defects also have other permanent teeth affected, including second permanent molars,59 and these teeth are also just as likely to become carious in a highly susceptible adolescent, while erupting.
Timed extractions of cFPMs are a sensible approach for some of the most severe cases. For others, it forces the clinician to make a judgement about FPM prognosis very early in the child's life and before the quality of the other unerupted teeth is known.
For the majority of 8-10-year-olds undergoing cFPM extractions, the procedure is performed under GA in hospital. The physical and psychological morbidity associated with tooth extraction under GA sessions includes pain, problems with eating, attention-seeking behaviour, tantrums, crying, nightmares and lack of sleep occurring approximately in 8-20% of children in the week after the procedure.60,61 The experience is upsetting for them, especially coping with hunger from fasting, the post-operative pain and impact on eating, which can lead to cognitive and developmental impairment.62,63 The quality of life for children left without a molar to chew on for four to six years has never been reported.
What further work is needed?
The prognosis of cFPMs and treatment should be based on patient-focused outcomes, such as oral health-related quality of life and patient and family satisfaction, as well as the health economics of the various options. The number and burden of dental GA appointments in the National Health Service (NHS) could be reduced, and more sixes could be saved using the MI approach and supervision of dentition and child development. Figure 3 summarises the suggested care pathways for the different clinical and radiographic findings of cFPMs, from early mixed dentition through to the teenage period.

Suggested care pathways for cFPMs from early mixed dentition to teenage years, aiming to improve the long-term prognosis of these teeth and reducing the need for enforced extractions
Conclusions
A cFPM with caries into the outer third of dentine and/or mild to moderate enamel defects can be restored using MI techniques. The new challenge for the clinician and the paediatric specialist is to consider the clinical and radiographic findings more carefully to determine the long-term prognosis of these teeth in individual patients in view of the current available MI techniques.
This decision needs to take into account the child, the family, their potential future attendance pattern and the child's own growth and development and changing caries susceptibility as they mature into adulthood.
It's time to set the criteria for judging the prognosis of cFPMs based on modern restorative techniques and evidence of treatment outcomes. The key points are:
-
cFPMs become less prone to caries once the child reaches 15 years of age
-
Hypomineralised cFPMs appear worse clinically than they do radiographically
-
Dentine underlying hypomineralised enamel seems to have similar adhesive properties to sound teeth, possibly explaining the low failure rates/loss of complete restorations in hypomineralised teeth
-
The restorative MI treatment choice requires periodic (every 6-12 months) review and repair using the '5Rs' principles when necessary
-
Radiographically, caries affecting the inner third of dentine could be managed successfully using MI techniques
-
Behaviour control during treatment will become simpler as the child matures into adolescence/adulthood
-
Fifteen percent of the patients with MIH defects in FPMs also have other permanent teeth affected, including second permanent molars
-
Restored molar teeth can survive for over 15 years.
References
Taylor G D, Pearce K F, Vernazza C R. Management of compromised first permanent molars in children: Cross-sectional analysis of attitudes of UK general dental practitioners and specialists in paediatric dentistry. Int J Paediatr Dent 2019; 29: 267-280.
Cobourne M T, Williams A, Harrison M. National clinical guidelines for the extraction of first permanent molars in children. Br Dent J 2014; 217: 643-648.
Ashley P, Noar J. Interceptive extractions for first permanent molars: A clinical protocol. Br Dent J 2019; 227: 192-195.
Sayagh M, Maniere-Ezvan A, Vernet C, Muller-Bolla M. Therapeutic decisions in the presence of decayed permanent first molars in young subjects: A descriptive inquiry. Int Orthod 2012; 10: 318-336.
Thylstrup A, Bruun C, Holmen L. In vivo caries models: Mechanisms for caries initiation and arrestment. Adv Dent Res 1994; 8: 144-157.
Agel M, Banerjee A, Neves A A, Costa L S, Hosey M T. First permanent molar extractions under general anaesthesia: A CEDACORE survey. J Dent Res 2018; 97(Special Issue B): 2678.
Carvalho J C, Ekstrand K R, Thylstrup A. Dental plaque and caries on occlusal surfaces of first permanent molars in relation to stage of eruption. J Dent Res 1989; 68: 773-779.
Carvalho J C, Figueredo C S, Mestrinho H D. Clinical report on plaque formation, distribution and maturation within the primary, mixed and permanent dentitions. Eur J Paediatr Dent 2009; 10: 193-199.
Zhao D, Dong B, Yu D, Ren Q, Sun Y. The prevalence of molar incisor hypomineralization: Evidence from 70 studies. Int J Paediatr Dent 2018; 28: 170-179.
Jalevik B, Dietz W, Noren J G. Scanning electron micrograph analysis of hypomineralized enamel in permanent first molars. Int J Paediatr Dent 2005; 15: 233-240.
Xie Z H, Mahoney E K, Kilpatrick N M, Swain M V, Hoffman M. On the structure-property relationship of sound and hypomineralized enamel. Acta Biomater 2007; 3: 865-872.
Fatturi A L, Wambier L M, Chibinski A C et al. A systematic review and meta-analysis of systemic exposure associated with molar incisor hypomineralization. Community Dent Oral Epidemiol 2019; 47: 407-415.
Jeremias F, Pierri R A, Souza J F et al. Family-based genetic association for molar-incisor hypomineralization. Caries Res 2016; 50: 310-318.
Bussaneli D G, Restrepo M, Fragelli C M B et al. Genes regulating immune response and amelogenesis interact in increasing the susceptibility to molar-incisor hypomineralization. Caries Res 2019; 53: 217-227.
Farah R A, Swain M V, Drummond B K, Cook R, Atieh M. Mineral density of hypomineralised enamel. J Dent 2010; 38: 50-58.
Neves A B, Americano G C A, Soares D V, Soviero V M. Breakdown of demarcated opacities related to molar-incisor hypomineralization: A longitudinal study. Clin Oral Investig 2019; 23: 611-615.
SDCEP. Prevention and management of dental caries in children: Dental clinical guidance (second edition). 2018. Available at https://www.sdcep.org.uk/wp-content/uploads/2018/05/SDCEP-Prevention-and-Management-of-Dental-Caries-in-Children-2nd-Edition.pdf (accessed September 2020).
Ismail A I, Sohn W, Tellez M et al. The International Caries Detection and Assessment System (ICDAS): An integrated system for measuring dental caries. Community Dent Oral Epidemiol 2007; 35: 170-178.
Chawla N, Messer L B, Silva M. Clinical studies on molarincisorhypomineralisation part 2: Development of a severity index. Eur Arch Paediatr Dent 2008; 9: 191-199.
Ha N, Kim Y, Kim H, Nam S. A prognostic assessment of first permanent molars showing molar-incisor hypomineralization based on restorative materials and defect class. J Korean Acad Pediatr Dent 2017; 44: 263-271.
Leal S C. Minimal intervention dentistry in the management of the paediatric patient. Br Dent J 2014; 216: 623-627.
Oliveira D C, Favretto C O, Cunha R F. Molar incisor hypomineralization: Considerations about treatment in a controlled longitudinal case. J Indian Soc Pedod Prev Dent 2015; 33: 152-155.
Kramer N, Bui Khac N N, Lucker S, Stachniss V, Frankenberger R. Bonding strategies for MIH-affected enamel and dentin. Dent Mater 2018; 34: 331-340.
Lygidakis N A. Treatment modalities in children with teeth affected by molar-incisor enamel hypomineralisation (MIH): A systematic review. Eur Arch Paediatr Dent 2010; 11: 65-74.
Souza J F, Fragelli C B, Jeremias F, Paschoal M A B, Santos-Pinto L, Loiola-Cordeiro R C. Eighteen-month clinical performance of composite resin restorations with two different adhesive systems for molars affected by molar incisor hypomineralization. Clin Oral Investig 2017; 21: 1725-1733.
Dhareula A, Goyal A, Gauba K, Bhatia S K, Kapur A, Bhandari S. A clinical and radiographic investigation comparing the efficacy of cast metal and indirect resin onlays in rehabilitation of permanent first molars affected with severe molar incisor hypomineralisation (MIH): A 36-month randomised controlled clinical trial. Eur Arch Paediatr Dent 2019; 20: 489-500.
Fragelli C M, Souza J F, Jeremias F, de Cássia Loiola Cordeiro R, Santos-Pinto L. Molar Incisor Hypomineralization (MIH): Conservative treatment management to restore affected teeth. Braz Oral Res 2015; DOI: 10.1590/1807-3107BOR-2015.vol29.0076.
Cvar J F, Ryge G. Reprint of criteria for the clinical evaluation of dental restorative materials. 1971. Clin Oral Investig 2005; 9: 215-232.
Hickel R, Peschke A, Tyas M et al. FDI World Dental Federation - Clinical criteria for the evaluation of direct and indirect restorations. Update and clinical examples. J Adhes Dent 2010; 12: 259-272.
Green D, Mackenzie L, Banerjee A. Minimally invasive long-term management of direct restorations: The 5 R's. Dent Update 2015; DOI: 10.12968/denu.2015.42.5.413.
Lucarotti P S, Burke F J. The ultimate guide to restoration longevity in england and wales. Part 6. Molar teeth: Restoration time to next intervention and to extraction of the restored tooth. Br Dent J 2018; 225: 525-536.
Davies G M, Davies R M. Delivering Better Oral Health - An evidence-based toolkit for prevention: A review. Dent Update 2008; DOI: 10.12968/denu.2008.35.7.460.
Crombie F A, Cochrane N J, Manton D J, Palamara J E, Reynolds E C. Mineralisation of developmentally hypomineralised human enamel in vitro. Caries Res 2013; 47: 259-263.
Ozgul B M, Saat S, Sonmez H, Oz F T. Clinical evaluation of desensitizing treatment for incisor teeth affected by molar-incisor hypomineralization. J Clin Pediatr Dent 2013; 38: 101-105.
Pasini M, Giuca M R, Scatena M, Gatto R, Caruso S. Molar incisor hypomineralization treatment with casein phosphopeptide and amorphous calcium phosphate in children. Minerva Stomatol 2018; 67: 20-25.
Frencken J E. The state-of-the-art of ART sealants. Dent Update 2014; DOI: 10.12968/denu.2014.41.2.119.
Schwendicke F, Splieth C, Breschi L et al. When to intervene in the caries process? An expert DELPHI consensus statement. Clin Oral Investig 2019; 23: 3691-3703.
Schwendicke F. Removing carious tissue: Why and how? Mon Oral Science 2018; 27: 56-67.
Najeeb S, Khurshid Z, Zafar M S et al. Modifications in glass ionomer cements: Nano-sized fillers and bioactive nanoceramics. Int J Mol Sci 2016; 17: 1134.
Diem V T, Tyas M J, Ngo H C, Phuong L H, Khanh N D. The effect of a nano-filled resin coating on the 3year clinical performance of a conventional high-viscosity glass-ionomer cement. Clin Oral Investig 2014; 18: 753-759.
Grossi J A, Cabral R N, Ribeiro A P D, Leal S C. Glass hybrid restorations as an alternative for restoring hypomineralized molars in the art model. BMC Oral Health 2018; 18: 65.
Van Meerbeek B, De Munck J, Yoshida Y et al. Buonocore memorial lecture - adhesion to enamel and dentin: Current status and future challenges. Oper Dent 2003; 28: 215-235.
Isolan C P, Sarkis-Onofre R, Lima G S, Moraes R R. Bonding to sound and caries-affected dentin: A systematic review and meta-analysis. J Adhes Dent 2018; 20: 7-18.
Van Meerbeek B, Peumans M, Poitevin A et al. Relationship between bond-strength tests and clinical outcomes. Dent Mater 2009; DOI: 10.1016/j.dental.2009.11.148.
William V, Burrow M F, Palamara J E, Messer L B. Microshear bond strength of resin composite to teeth affected by molar hypomineralization using 2 adhesive systems. Pediatr Dent 2006; 28: 233-241.
Sönmez H, Saat S. A clinical evaluation of deproteinization and different cavity designs on resin restoration performance in MIH-affected molars: Two-year results. J Clin Pediatr Dent 2017; 41: 336-342.
Rosenblatt A, Stamford T C, Niederman R. Silver diamine fluoride: A caries "silver-fluoride bullet". J Dent Res 2009; 88: 116-125.
Gao S S, Zhao I S, Hiraishi N C et al. Clinical trials of silver diamine fluoride in arresting caries among children: A systematic review. JDR Clin Trans Res 2016; 1: 201-210.
Zhao I S, Gao S S, Hiraishi N et al. Mechanisms of silver diamine fluoride on arresting caries: A literature review. Int Dent J 2018; 68: 67-76.
Chu C H, Lo E C. Promoting caries arrest in children with silver diamine fluoride: A review. Oral Health Prev Dent 2008; 6: 315-321.
Yee R, Holmgren C, Mulder J, Lama D, Walker D, van Palenstein Helderman W. Efficacy of silver diamine fluoride for arresting caries treatment. J Dent Res 2009; 88: 644-647.
Alvear Fa B, Jew J A, Wong A, Young D. Silver modified atraumatic restorative technique (SMART): An alternative caries prevention tool. Stomatol Edu J 2016; 3: 18-23.
Puwanawiroj A, Trairatvorakul C, Dasanayake A P, Auychai P. Microtensile bond strength between glass ionomer cement and silver diamine fluoride-treated carious primary dentin. Pediatr Dent 2018; 40: 291-295.
Jalevik B, Klingberg G A. Dental treatment, dental fear and behaviour management problems in children with severe enamel hypomineralization of their permanent first molars. Int J Paediatr Dent 2002; 12: 24-32.
Elhennawy K, Krois J, Jost-Brinkmann P G, Schwendicke F. Outcome and comparator choice in molar incisor hypomineralisation (MIH) intervention studies: A systematic review and social network analysis. BMJ Open 2019; DOI: 10.1136/bmjopen-2018-028352.
Jalevik B, Moller M. Evaluation of spontaneous space closure and development of permanent dentition after extraction of hypomineralized permanent first molars. Int J Paediatr Dent 2007; 17: 328-335.
Wu M, Chen L, Bawole E, Anthonappa R P, King N M. Is there sufficient evidence to support an optimum time for the extraction of first permanent molars? Eur Arch Pediatr Dent 2017; 18: 155-161.
Teo T K, Ashley P F, Derrick D. Lower first permanent molars: Developing better predictors of spontaneous space closure. Eur J Orthod 2016; 38: 90-95.
Mittal N. Phenotypes of enamel hypomineralization and molar incisor hypomineralization in permanent dentition: Identification, quantification and proposal for classification. J Clin Pediatr Dent 2016; 40: 367-374.
Hosey M T, Macpherson L M, Adair P, Tochel C, Burnside G, Pine C. Dental anxiety, distress at induction and postoperative morbidity in children undergoing tooth extraction using general anaesthesia. Br Dent J 2006; DOI: 10.1038/sj.bdj.4813123.
Alohali A A, Al-Rubaian N, Tatsi C, Sood S, Hosey M T. Post-operative pain and morbidity in children who have tooth extractions under general anaesthesia: A service evaluation. Br Dent J 2019; 227: 713-718.
Rodd H, Hall M, Deery C, Gilchrist F, Gibson B J, Marshman Z. 'I felt weird and wobbly.' Child-reported impacts associated with a dental general anaesthetic. Br Dent J 2014; DOI: 10.1038/sj.bdj.2014.333.
Huntington C, Liossi C, Donaldson A N et al. On-line preparatory information for children and their families undergoing dental extractions under general anaesthesia: A phase III randomized controlled trial. Paediatr Anaesth 2018; 28: 157-166.
Acknowledgements
This paper is part of a clinical research collaboration with Brazil entitled: Children Experiencing Dental Anxiety Collaboration on Research and Education (CEDACORE) which was funded by CAPES (Brazil) and Newton Fund British Council (UK). The Ministry of Education, Saudi Arabia is also acknowledged for sponsoring the PhD studentship of Reem Alkhalaf. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Alkhalaf, R., Neves, A., Banerjee, A. et al. Minimally invasive judgement calls: managing compromised first permanent molars in children. Br Dent J 229, 459–465 (2020). https://doi.org/10.1038/s41415-020-2154-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-020-2154-x
- Springer Nature Limited
This article is cited by
-
Perceptions, attitudes, and clinical experiences of Brazilian dental practitioners towards molar incisor hypomineralisation: a cross-sectional study
European Archives of Paediatric Dentistry (2024)
-
Clinical and radiographic performance of preformed zirconia crowns and stainless-steel crowns in permanent first molars: 18-month results of a prospective, randomized trial
BMC Oral Health (2023)
-
Molar-incisor hypomineralisation combat: exploratory qualitative interviews with general dental practitioners in England regarding the management of children with molar-incisor hypomineralisation
British Dental Journal (2022)
-
An update of treatment modalities in children and adolescents with teeth affected by molar incisor hypomineralisation (MIH): a systematic review
European Archives of Paediatric Dentistry (2022)
-
Children’s dental treatment requirements of first permanent molars with poor prognosis
Clinical Oral Investigations (2022)