
Abstract
Introduction
We report two cases of fracture-dislocation of the thoracolumbar spine without neurological deficit and outline the putative mechanisms responsible for the escape of neural tissues from injurious forces and the surgical management strategies for this type of injury. We also review similar cases described in the literature.
Case reports
A 24-year-old female with post-traumatic fracture dislocation at the T10–T11 level without neurological deficit, along with a right femoral shaft fracture, was managed with laminectomy of T10–T11 levels with bilateral facetectomy and transpedicular screws and with an intramedullary interlocking nail for the femur fracture. Another 26-year-old female (post-traumatic fracture dislocation at the T12 - L1 level treated by open reduction and pedicle screw instrumentation elsewhere) presented with implant failure and re-dislocation which was managed with laminectomy of T12- L1 levels, facetectomy and discectomy, and deformity correction, followed by 9 mm × 25 mm bullet cage insertion and fixation using transpedicular screws. Neurological function was preserved postoperatively. Both individuals returned to household activity 6 months postoperatively.
Discussion
Fracture-dislocations of the thoracolumbar spine without neurological deficit have been infrequently reported. The mechanism responsible for the preservation of normal neurological function; is either posterior element fractures leading to free-floating laminae or a fracture-separation of the vertebral arch, in which pedicle fractures allow the posterior elements to remain nearly aligned, with preservation of the spinal canal integrity and maintenance of normal spinal cord function. These fracture-dislocations need to be managed carefully to achieve a good outcome.
Similar content being viewed by others


Introduction
A thoracolumbar fracture is the most common injury of the spine accounting for more than half of all spinal trauma cases [1, 2]. Thoracolumbar fracture-dislocations are, however, uncommon and represent <3% of these injuries [3]. Vertebral fracture-dislocations which cause disruption of the whole spinal column occur due to high-energy trauma and involve trauma to both static and dynamic stabilising elements such as the vertebral bodies, discs, facets, ligaments and muscles due to a combination of shear, rotation and flexion–extension forces [4]. Traumatic dislocation is usually associated with fractures and is complicated by injury to neural structures of varying severity [5, 6]. The spine should be stabilised at the earliest possible opportunity to allow for neurological and musculoskeletal healing in a stable environment [7, 8]. However, fracture-dislocations of the thoracolumbar spine without neurological deficit have been infrequently reported [9,10,11,12,13,14,15,16,17,18,19] (Table 1). These cases with fracture-dislocation without neurological deficit may suffer unintended variable neurological deficit secondary to reduction manoeuvres and fixation errors.
We present here two cases of fracture-dislocation of the thoracolumbar spine without neurological deficit along with a review of similar cases described in the literature. We also outline the putative mechanisms responsible for the escape of neural tissues from injurious forces and management strategies useful for this type of injury.
Case reports
A 24-year-old woman with no prior medical history, presented to our hospital with complaints of back pain and deformity, with associated injury in the right thigh following a road accident (she was a motorcycle passenger thrown away after striking with a vehicle). Initial radiographs showed fracture dislocation at the T10–T11 level with a femoral shaft fracture (Fig. 1a, b).

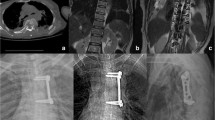
Preoperative anteroposterior (a) and lateral (b) radiographs showing fracture-dislocation at T10 T11 level. Preoperative sagittal (c) and axial (d, e) CT Scan. Preoperative mid-sagittal (f) and axial (g, h) T2 MRI images showing fracture-dislocation site partly auto-reduced. i Intra-operative photograph showing a complete tear in the interspinous ligament. Postoperative anteroposterior (j) and lateral (k) radiographs showing reduced fracture-dislocation fixed with pedicle screw and rod construct with the cross connector. l Postoperative anteroposterior and lateral radiographs (6-month Post-Op).
The computed tomography (CT) and MRI showed more than 50% anterolisthesis at T10-T11 with anterior wedging of T11. The spinal cord at this level was abutted by the superior margin of the retropulsed T11 vertebral body; however, AP canal dimension was found to be adequate (14.1 mm) (Fig. 1c–e, f–h). There was no obvious traumatic cord injury. Fracture of the posterior elements of T10 was noted involving the bilateral laminae, inferior facets and pedicles and the right T11 rib. No other vertebral fractures were identified on initial images. There was no sign of direct injury to the skin in the area of the thoracolumbar spine. The neurological examination revealed no deficits.
As the individual presented to us neurologically intact with T10–11 fracture-dislocation with right femoral shaft fracture, our primary goal was to provide biomechanical stability without compromising the neurological status. We applied in-bed traction to the individual as she also had a right femoral shaft fracture.
Every precaution was taken during the transportation of the woman from the ward to the operation table. She was placed in the prone position and a standard posterior midline exposure with subperiosteal dissection of the paraspinal musculature was performed over two levels above and two levels below the fracture-dislocation level. Cautious dissection was performed across the fracture-dislocation, so as not to inadvertently injure the possibly exposed neural elements. Several injuries could be seen from back to front- tears in the paravertebral muscles, a complete tear in the inter- and supraspinous ligaments between T10 and T11, complete bilateral tear of the articular capsules of the facet joints T10–T11 along with facet fractures (Fig. 1i).
Bilateral transpedicular screws were inserted in eight pedicles from T8 to T12 (except for T10). Laminectomy and facetectomy at T10–T11 levels were performed. It was ensured that there was no residual spinal cord compression and cord pulsation was visible. Two rods were applied and a reduction tower was used for reducing the rods to T9 pedicle screws with gentle force. The dislocation reduced completely with these procedures. Cross connector was applied. Haemostasis was achieved with an absorbable gelatin sponge and haemostatic agents. In addition, decortication of the posterior elements and autologous bone grafting was performed before drainage and wound closure. The individual remained neurology intact. The individual sat on second postoperative day with a thoracolumbar sacral orthosis (TLSO). The TLSO was continued for about 3 months. After 1-week, the shaft femur was managed with an interlocking nail. The woman was followed up 2 weeks, 6 weeks, 3 and 6 months postoperatively, at which point she returned to household work (Fig. 1j–l).
Another 26-year-old female was involved in a road traffic accident in Dec 2017. She originally presented to a nearby local hospital with complaints of back pain and radiculopathy, where a diagnosis of thoracolumbar fracture-dislocation was made. Two days after the injury, fixation was done with rods and pedicle screws at T10 and L1 levels. Six months later the woman had back pain and skin impingement with the implant; therefore the implants were removed.
Subsequently, the individual presented to us with complaints of spinal deformity and pain. There were no neurological deficits. Radiographs, CT and MRI revealed fracture dislocation at the T12-L1 level with the broken implant and with broken screws in the proximal and distal vertebrae (Fig. 2a–f). There was no clinical or laboratory evidence of infection. CBC, ESR and CRP were in the normal range. She was planned for surgery with the aim to correct the deformity, decompress the canal and to provide an anterior structural support (bullet cage with bone graft) and for long-segment fixation with pedicle screws.

a Preoperative anteroposterior and lateral radiographs showing fracture-dislocation at T12- L1 level with a broken screw at the proximal and distal levels. b, c Preoperative sagittal CT Scan. b-Right parasagittal, c-Left parasagittal. d Preoperative Axial CT Scan. Preoperative sagittal T1 (e) and T2 (f) MRI images. g Postoperative anteroposterior and lateral radiographs showing reduced fracture-dislocation fixed with pedicle screw, cage and rod construct with the cross connector.
Every precaution was taken during the transportation of the woman from the ward to the operation table. She was placed in the prone position and a standard posterior midline exposure was made through the same previous incision. Cautious dissection was performed across the fracture-dislocation, so as not to inadvertently injure the possibly exposed neural elements.
Bilateral pedicle screws were inserted at T9, T10, L2, L3; unilateral pedicle screws were inserted in right T11, T12 and left L1 vertebrae. After laminectomy and facetectomy at T12-L1 level, rods were applied into distal screws and slowly manoeuvred over the proximal screws. The dislocation was reduced with these procedures. Discectomy was performed at the same level from the right side, followed by the insertion of bone graft in the disc space. A bullet PEEK (poly ethyl ether ketone) cage filled with bone graft (size 9 mm × 25 mm) was inserted at T12-L1 disc level anteriorly from the right side. The bone graft was added in the surrounding area and posterolaterally. Compression was done under neuromonitoring. Cross connector was applied. Haemostasis was achieved. Postoperative anteroposterior and lateral radiographs revealed that the reduced fracture-dislocation was fixed with pedicle screw, cage and rod construct with cross connector (Fig. 2g). Intraoperative samples for microscopy and culture did not reveal any microbial growth. Her post-operative course was uneventful and the wound healed normally. The individual sat on the second day post-surgery with a TLSO. The TLSO was continued for about 3 months.
Discussion
We report two cases of thoracolumbar fracture-dislocation without neurological deficit, one acutely post-injury and the other after a failed initial surgery. Spinal cord sparing in a complete fracture-dislocation is possibly due to spontaneous decompression caused by accompanying posterior element fractures. In our first case, posterior elements of the affected vertebrae had fractured and displaced posteriorly, leading to widening of the spinal canal and no compromise in space available for the cord. Fractured pedicles and facets separate the vertebral body from the posterior vertebral arch (pedicles, facets, laminae and spinous process). This separation may allow for severe vertebral body dislocation, and the spinal cord may still have enough space to avoid any injury. The main management principles for such cases are to realign and stabilise the involved vertebrae to avoid future neural deficits. Surgical reduction with due precautions and fusion have been recommended for managing thoracolumbar fracture-dislocation [4, 7, 8]. We used log-rolling for every movement prior to surgical stabilisation to avoid the risk of any insult to neural structures. A posterior approach with long-segment instrumentation (at least 2 levels above and 2 levels below), was performed due to the severe instability of the injured spine [7, 11,12,13].
In our second case, the bone stock was deficient on the left side at T12- L1 level, as the inferior endplate of T12 had eroded on the left side. Therefore, for providing anterior structural support, we inserted a PEEK bullet cage from the right side, where the end plates were relatively preserved. Wide laminectomy and facetectomy are particularly important in such cases to allow smooth reduction without any risk to neural tissues. We also performed a discectomy at T12, L1 level for further release and created a space for insertion of the cage. Bone graft was packed in the void of T12-L1 disc space and adjacent to the cage, and some graft was also applied posterolaterally. This inserted bone graft provided the appropriate milieu for a circumferential fusion. We opted for a bullet PEEK cage. Similar material properties of PEEK to host bone, as compared to titanium, reduces the risk of subsidence [20]. Neuromonitoring also assumes importance in such old neglected cases, as there is a risk of deterioration during reduction manoeuvre.
The mechanism responsible for the preservation of normal neurological function, as reported by most authors [9,10,11,12,13,14,15,16,17,18,19], is either posterior element fractures leading to free-floating laminae or a fracture-separation of the vertebral arch, in which pedicle fractures allow the posterior elements to remain nearly aligned, with preservation of the spinal canal integrity and maintenance of normal spinal cord function, despite the severe displacement of the affected vertebral body. Phadnis et al. reported a case of a 21-year-old man with complete fracture-dislocation at L1-L2 level with normal motor function and paraesthesia in the right L2 dermatome. They advocated that the aim of surgery in such cases are’ (1) Primum non-nocere—do no more harm. (2) Posterior decompression and prevention of secondary damage to the thecal sac. (3) Anatomic reduction and restoring mechanical stability [13]”. Zeng et al. have also reported such a case along with a review of relevant literature and agree that the mechanism of neural escape in such cases is ‘Spontaneous decompression’ resulting from fractured pedicles and facets, which separate the vertebral body from the vertebral arch (pedicles, facets, lamina and spinous process) [16].
Enishi et al. have reported two such cases, which were managed by anterior subtotal corpectomy and reconstruction combined with posterior decompression. The mechanism of neural escape was different in the two cases. One case had bilateral pedicle fracture, but in the other case, rotational displacement and collapse of the broken vertebrae decompressed the dura and widened the spinal canal [18].
Rahimizadeh et al. also reported such a case and speculated about the possibility of the existence of a preservation mechanism for the functional integrity of the cord despite gross spinal fracture-dislocation. They reproduced the injury on a plastic model and simulated a corresponding model using 3D Slicer software with the help of CT data, along with a detailed description of the pathomechanism of neurologic sparing. It was interpreted that a mechanism other than saving fractures could have protected the cord in spite of the near-complete dislocation. They demonstrated that violent hyperflexion in combination with shearing rotational stress affected the intervertebral L1-L2 disc. Continued shearing forces, accompanied by rotational forces with the spinal cord as a hinge, led to the corresponding facet joints getting engaged and locked, with the spinal canal still remaining aligned [19].
References
Patel AA, Dailey A, Brodke DS, et al. Thoracolumbar spine trauma classification: the thoracolumbar injury classification and severity score system and case examples. J Neurosurg Spine. 2009;10:201–6.
Fakurnejad S, Scheer JK, Patwardhan AG, et al. Biomechanics of thoracolumbar burst fractures: methods of induction and treatments. J Clin Neurosci. 2014;21:2059–64.
Denis F. Spinal instability as defined by the three-column spine concept in acute spinal trauma. Clin Orthop Relat Res. 1984;189:65–76.
Wood KB, Li W, Lebl DS, Ploumis A. Management of thoracolumbar spine fractures. Spine J. 2014;14:145–64.
Guigui P, Lassale B, Deburge A. Fracture etluxationsrécentes du rachis dorsal et lombaire de l’adulte. Encycl Med Chir.15-829-A-10 In: Appareil Locomoteur. Paris: Elsevier; 1998. pp 1–10.
Frankel HL, Hancock DO, Hyslop G, Melzak J, Michaelis LS, Ungar GH, et al. The value of the postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. Paraplegia. 1969;7:179–92.
Wang F, Zhu Y. Treatment of complete fracture-dislocation of thoracolumbar spine. J Spinal Disord Technol. 2013;26:421–6.
Magerl F, Aebi M, Gertzbein SD, et al. A comprehensive classification of thoracic and lumbar injuries. Eur Spine. J. 1994;3:184–201.
Weber SC, Sutherland GH. An unusual rotational fracture-dislocation of the thoracic spine without neurologic sequelae internally fixed with a combined anterior and posterior approach. J Trauma Acute Care Surg. 1986;26:474–9.
Korovessis P, Sidiropoulos P, Dimas A. Complete fracture-dislocation of the thoracic spine without neurologic deficit: case report. J Trauma Acute Care Surg. 1994;36:122–4.
Akay KM, Baysefer A, Kayali H, et al. Fracture and lateral dislocation of the T12-L1 vertebrae without neurological deficit—case report. Neurol Med Chir. 2003;43:267–70.
Phadnis AS, Tan CJ, Raman AS, et al. Fracture and complete dislocation of the spine with a normal motor neurology. Inj Extra. 2006;37:479–83.
Hsieh CT, Chen GJ, Wu CC, et al. Complete fracture-dislocation of the thoracolumbar spine without paraplegia. Am J Emerg Med. 2008;26:633.e5–7.
Solera JMR, de la Haba AMC, León MSH, Parra EG.Fracture-dislocation of the upper thoracic spine without neurologic associated injury: two cases report.Trauma Cases Rev.2015;1:022. https://doi.org/10.23937/2469-5777/1510022.
Sugiura K, Sakai T, Adachi K, Inoue K, Endo S, Tamaki Y, et al. Complete fracture-dislocation of the thoracolumbar spine with no critical neurological deficit: a case report. J Med Investig. 2016;63:122–6.
Zeng J, Gong Q, Liu H, Rong X, Ding C. Complete fracture-dislocation of the thoracolumbar spine without neurological deficit: a case report and review of the literature. Medicines. 2018;97:e0050.
Evans LJ. Images in clinical medicine. Thoracolumbar fracture with preservation of neurologic function. N Engl J Med 2012;367:19–39.
Enishi T, Katoh S, Sogo T. Surgical treatment for significant fracture-dislocation of the thoracic or lumbar spine without neurologic deficit: a case series. J Orthop Case Rep. 2014;4:43–5.
Rahimizadeh A, Asgari N, Rahimizadeh A. Complete thoracolumbar fracture-dislocation with intact neurologic function: explanation of a novel cord saving mechanism. J Spinal Cord Med. 2017;26:1–10.
Heary RF, Parvathreddy N, Sampath S, Agarwal N. Elastic modulus in the selection of interbody implants. J Spine Surg.2017;3:163–7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Kumar, S., Kumar, P., Patralekh, M.K. et al. Fracture-dislocation of the thoracolumbar spine without neurological deficit: a report of two cases and literature review. Spinal Cord Ser Cases 6, 67 (2020). https://doi.org/10.1038/s41394-020-0315-4
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41394-020-0315-4
- Springer Nature Limited
This article is cited by
-
The difference and clinical application of modified thoracolumbar fracture classification scoring system in guiding clinical treatment
Journal of Orthopaedic Surgery and Research (2023)