
Abstract
Background
Avoiding unnecessary biopsies for men with suspected prostate cancer remains a clinical priority. The recently proposed PRIMARY score improves diagnostic accuracy in detecting clinically significant prostate cancer (csPCa). The aim of this study was to determine the best strategy combining PRIMARY score or MRI reporting scores (Prostate Imaging Reporting and Data System [PI-RADS]) with prostate-specific antigen density (PSAD) for prostate biopsy decision making.
Methods
A retrospective analysis of 343 patients who underwent both 68Ga-PSMA PET/CT and MRI before prostate biopsy was performed. PSA was restricted to <20 ng/ml. Different biopsy strategies were developed and compared based on PRIMARY score or PI-RADS with PSAD thresholds. Decision curve analysis (DCA) was plotted to define the optimal biopsy strategy.
Results
The prevalence of csPCa was 41.1% (141/343). According to DCA, the strategies of PRIMARY score +PSAD (strategy #1, strategy #2, strategy #6) had a higher net benefit than the strategies of PI-RADS + PSAD at the risk threshold of 8–20%. The best diagnostic strategy was strategy #1 (PRIMARY score 4-5 or PSAD ≥ 0.20), which avoided 38.2% biopsy procedures while missed 9.2% of csPCa cases. From a clinical perspective, strategies with a lower risk of missing csPCa were strategy #2 (PRIMARY score ≥4 or PSAD ≥ 0.15), which avoided 28.6% biopsies while missed 5.7% of csPCa cases, or strategy #6 (PRIMARY score≥3 or PSAD ≥ 0.15), which avoided 20.7% biopsies while missed only 3.5% of csPCa cases. The limitations of the study were the retrospective single-center nature.
Conclusions
The combination of PRIMARY score +PSAD allows individualized decisions to avoid unnecessary biopsy, outperforming the strategies of PI-RADS + PSAD. Further prospective trials are needed to validate these findings.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Prostate cancer (PCa) is the most commonly diagnosed cancer in men [1]. The European Randomized Screening Study for Prostate Cancer (ERSPC) showed that prostate-specific antigen (PSA)-based screening resulted in a 20% reduction in PCa-specific mortality and a 30% reduction in metastatic disease, but at the expense of many unnecessary biopsy procedures, as well as overdiagnosis and associated overtreatment of indolent prostate cancer [2, 3].
This harm can be mitigated by implementing individualized risk-adapted tools that combine imaging and clinical parameters [4, 5]. Multiparametric magnetic resonance imaging (MRI) has become an integral part in the detection of clinically significant PCa (csPCa) [6]. The main challenges of MRI-derived diagnostic pathway are the low positive predictive value and moderate inter-reader and inter-center repeatability [7,8,9]. PSA density (PSAD) has been proved to be a well-established predictor of csPCa, and several publications have suggested combining MRI with PSAD to define men who can safely avoid biopsy [10,11,12,–13]. However, Falagario et al. has recommended biopsy in men with a Prostate Imaging Reporting and Data System (PI-RADS) 4–5 or PI-RADS 3 if PSAD > 0.2 [14], while another study recommended biopsy in men with PI-RADS ≥ 4 or PSAD ≥ 0.15 [15]. Therefore, the inconsistent combined strategy may limit their performance in external institutions.
The recently updated prostate cancer molecular imaging standardized evaluation (PROMISE V2) criteria has incorporated a 5-point Likert PRIMARY score based on prostate-specific membrane antigen (PSMA) positron emission tomography/computed tomography (PET/CT) [16]. This score combined anatomic localization (peripheral, central, or transition zone), intra-prostatic PSMA activity patterns (none, diffuse, or focal) and a very high maximum standardized uptake value (SUVmax >12) to enhance the diagnosis of primary tumors [17]. The PRIMARY score provided superior diagnostic accuracy and inter-rater agreement compared to MRI alone, with a specificity of 64% and no compromise in sensitivity. However, the positive predictive value (PPV) and negative predictive value (NPV) for PRIMARY score (1-2 low-risk patterns vs 3–5 high-risk patterns) was 76% and 81%, which indicating that the false positive rate and false negative rate were 24% and 19%, respectively. Biopsy according to PRIMARY score ≥3 still resulted in 24% unnecessary biopsy procedures and missed 19% of csPCa cases.
We hypothesized that combining the novel PRIMARY score with PSAD will help reduce unnecessary biopsies. To test our hypothesis, we developed and compared different biopsy strategies combining PRIMARY score or PI-RADS with PSAD to determine the optimal biopsy strategy and the proportion of men who can safely avoid unnecessary biopsies.
Patients and methods
Study population
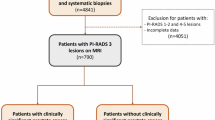
A total of 688 consecutive men who underwent both MRI and 68Ga-PSMA PET/CT prior to biopsy were retrospectively reviewed at our institution from June 2017 to November 2022. Finally, 343 patients were included for the final analysis (Supplementary Fig. 1). Patients with suspicious MRI findings, as well as patients with persistent clinical concern despite a normal MRI underwent 68Ga-PSMA PET/CT and subsequent biopsy. The institutional review board (Ethics Committees of Xijing Hospital, Fourth Military Medical University) approved this study and all subjects signed a written informed consent. This study conforms with the Declaration of Helsinki and national regulations.
PSMA PET protocols
Patients were prepared and images were acquired according to standard clinical protocols. All images were scanned with a Biograph 40 system (Siemens Medical Solutions, Erlangen, Germany). According to the Joint EANM and SNMMI Procedure Guideline [18], a whole-body PET scan was performed 60 min after the intravenous injection of 1.8–2.2 MBq/kg 68Ga-PSMA-11. Low-dose CT scans (pitch 0.8, 50 mA, 120 kV [peak]) of PET attenuation were collected (automatic mA, 120 keV, 512 ×512 matrix, 5-mm slice thickness, 1.0-s rotation time), followed by a PET scan performed with 5 bed positions (3 min/bed, from head to the proximal thighs) performed. Finally, all PET/CT images were sent to multimodal workstations (Syngo TrueD and HD Truepoint Siemens Medical Solutions) for analysis.
PSMA PET and PRIMARY score interpretation
All 68Ga-PSMA PET/CT images were blinded reviewed by two experienced nuclear medicine physicians. Each discrepancy was resolved in consensus with a third nuclear medicine physician. Three-dimensional (3D) spherical regions of interest (ROIs) in PCa lesions were manually delineated to calculate standardized uptake values (SUVs). SUVmax was measured in all volumes of interest. The PRIMARY score was assessed and reported according to the original PRIMARY score study [17]. PRIMARY score 1-2 was regarded as low-risk patterns and PRIMARY score 3–5 was regarded as high-risk patterns.
MRI acquisition protocol and interpretation
All patients underwent MRI and the protocol consisted of T1-weighted imaging (T1WI), T2-weighted imaging (T2WI), and diffusion-weighted imaging (DWI) imaging sequences. The MRI scans were analyzed and reported according to Pl-RADS v2.0 [19] and, since 2019, PI-RADS v2.1 [20]. For MRI analysis, PI-RADS 1-2 was regard as negative and PI-RADS 3–5 was defined as positive.
Histopathology examination
All patients received at least 12-core transrectal ultrasound-guided systematic biopsies (depending on the prostate volume). When possible, additional target biopsies were performed using cognitive fusion techniques. All biopsies were processed and reported according to International Society of Urological Pathology (ISUP) protocols [21]. The ISUP Grade Group was taken from the highest ISUP grade group in the combined dataset (i.e., systematic biopsy +target biopsy). csPCa was defined as any ISUP Grade Group ≥2 based on biopsy histology.
Statistical analysis
Continuous variables were present as median and interquartile ranges and the categorical variables were presented as frequencies and percentages. Prostate volume was calculated by ellipsoid formula (width * height * length * π/6) based on MRI, and PSAD was divided into four groups: <0.10 ng/ml2, 0.10–0.15 ng/ml2, 0.15–0.20 ng/ml2 and ≥0.20 ng/ml2. Six risk stratification strategies based on PRIMARY score + PSAD and six same risk stratification strategies for PI-RADS + PSAD were defined (Supplementary Table 1). The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of each biopsy strategy for detecting csPCa were calculated, as well as the reduction of unnecessary biopsies and the missed csPCa cases. Clinical utility was assessed by decision curve analysis (DCA) [22]. The DCA estimates a net benefit for models by summing the benefits (true positives) and subtracting the harms (false positives). The net benefits of the proposed strategies were compared with that of ‘Biopsy-all’ and ‘Biopsy-none’ to select the optimal strategy. All statistical analyses were performed by IBM SPSS statistics software, version 26.0 (IBM, Inc., Chicago, IL, USA) and R software, version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
Result
Demographics and clinical characteristics
Of the 343 patients enrolled for analysis, 52.5% (180/343) had any form of PCa and 41.1% (141/343) were diagnosed with csPCa. The clinical characteristics were presented in Table 1.
Diagnostic performance
The sensitivity, specificity, PPV and NPV for detecting csPCa at different thresholds of PRIMARY score alone, PSAD alone and PI-RADS alone were presented in Table 2. According to the Youden index, the optimal cutoff for recommending a biopsy was PRIMARY score ≥4, PSAD ≥ 0.20 ng/ml2, and PI-RADS ≥ 4. However, the corresponding proportion of missed csPCa was 18.4% (26/141), 39.0% (55/141), and 24.1% (34/141), respectively.
Effect of PSAD group on diagnostic performance of PRIMARY score
Within each PRIMARY score level, increased PSAD was associated with increased detection of csPCa (Fig. 1). Confirmatory biopsies showed that the prevalence of csPCa was 11.8% (15/127), 21.6% (11/51), 69.7% (115/165) in the PRIMARY score results within PRIMARY score 1–2, PRIMARY score 3 and PRIMARY score 4-5 (Supplementary Table 2). The distribution of csPCa in patients with PSAD < 0.10 ng/ml2, 0.10–0.15 ng/ml2, 0.15–0.20 ng/ml2, and ≥0.20 ng/ml2 were 8.5% (12/141), 14.2% (20/141), 16.3% (23/141), 61.0% (86/141), respectively.

PSAD prostate-specific antigen density, ISUP International Society of Urological Pathology.
In addition, PSAD had a significant effect on the predictive values of PRIMARY score≥3 for the detection of csPCa (Table 3). The lowest PPV (28.9%) was found in patients with PSAD < 0.10 ng/ml2, while the lowest NPV (80.0%) was found in patients with PSAD ≥ 0.2 ng/ml2.
Combined strategies impact on biopsy
According to DCA (Fig. 2) and the net benefit (Supplementary Table 3), the strategies of PRIMARY score + PSAD (strategy #1, strategy #2, strategy #6) had a higher net benefit than the strategies of PI-RADS + PSAD at the risk threshold of 8–20%. The results of different biopsy strategies for detecting and ruling out prostate cancer were presented in Table 4. The best diagnostic strategies were the strategy #1 (PRIMARY score 4-5 or PSAD ≥ 0.20), which avoided 38.2% biopsy procedures and 35.9% overdiagnosis of insignificant PCa while missing 9.2% csPCa. Similar performances were shown with strategy #2 (PRIMARY score ≥4 or PSAD ≥ 0.15) and strategy #6 (PRIMARY score ≥3 or PSAD ≥ 0.15), resulting in 28.6% and 20.7% biopsy avoidance and 5.7% and 3.5% of csPCa missed, respectively.

The strategies were based on (A) PRIMARY score + PSAD or (B) PI-RADS + PSAD. PI-RADS Prostate Imaging Reporting and Data System, PSAD prostate specific antigen density. strategy 1 = PRIMARY score 4-5 or PSAD ≥ 0.20; strategy 2 = PRIMARY score 4-5 or PSAD ≥ 0.15; strategy 3 = PRIMARY score 4-5 or PRIMARY score 3 if PSAD ≥ 0.20; strategy 4 = PRIMARY score 4-5 or PRIMARY score 3 if PSAD ≥ 0.15; strategy 5 = PRIMARY score 3-5 or PSAD ≥ 0.20; strategy 6 = PRIMARY score 3–5 or PSAD ≥ 0.15; strategy 7 = PI-RADS 4–5 or PSAD ≥ 0.20; strategy 8 = PI-RADS 4-5 or PSAD ≥ 0.15; strategy 9 = PI-RADS 4-5 or PI-RADS 3 if PSAD ≥ 0.20; strategy 10 = PI-RADS 4-5 or PI-RADS 3 if PSAD ≥ 0.15; strategy 11 = PI-RADS 3–5 or PSAD ≥ 0.20; strategy 12 = PI-RADS 3–5 or PSAD ≥ 0.15.
Discussion
In this study, we developed and compared different prostate biopsy strategies by combining the PRIMARY score or PI-RADS with PSAD to optimize the diagnostic pathway and reduce unnecessary biopsy procedures, effectively balancing the benefits and harms of biopsy. We found that PSAD significantly affects the performance of the PRIMARY score in detecting csPCa. When combining with PSAD respectively, the PRIMARY score had a higher net benefit and was superior to PI-RADS in the diagnosis of prostate cancer. Further prospective studies were needed to be validated these findings.
Previous research in the diagnosis of PCa by PSMA-PET/CT mainly relied on the SUVmax value. However, the use of different PET instruments and variable PSMA ligands resulted in different optimal SUVmax cutoff values. For instance, the PRIMARY trial suggested an optimal cut-off value of 4.0 [23], while other studies recommended values ranging from 5 to 9 [24,25,26,–27]. To overcome this deficiency, by incorporating tumor location information, PSMA patterns, and very high SUVmax (>12), the PRIMARY score showed higher accuracy and inter-rater agreement in detecting csPCa than SUVmax and mpMRI alone [17].
As a newly proposed scoring system, few studies have investigated the diagnostic performance of the PRIMARY score + PSAD in the diagnosis of prostate cancer, let alone compared with the risk stratification strategies of PI-RADS + PSAD. The European Association of Urology (EAU) guidelines pointed that combining PSAD with the PI-RADS score may help define patients who need biopsy [6]. In the present study, the PRIMARY Score + PSAD strategies (strategy #1, strategy #2, strategy #6) had a higher net benefit at a risk threshold probability of 8% to 20% and were superior to the strategies of PI-RADS + PSAD. Our results provided an evidence-based possibility that combing PRIMARY score with PSAD could provide better guidance for biopsy decisions.
In the present study, according to the DCA, performing biopsy in men with PRIMARY score 4-5 or PSAD ≥ 0.20 (strategy #1) was shown to be the strategy with the highest net benefit in terms of biopsy avoidance and detection of csPCa. Similar performances were shown with strategy #2 (PRIMARY score 4-5 or PSAD ≥ 0.15) and strategy #6 (PRIMARY score 3–5 or PSAD ≥ 0.15). To give a specific example, at a 20% threshold probability, the net benefit of strategy #1 and PRIMARY score ≥3 was 0.312 and 0.302, respectively. According to the previously proposed formula [22], the difference in net benefit was 0.010, meaning that strategy #1 could reduce 4 unnecessary biopsy procedures per 100 patients without missing any csPCa compared to PRIMARY score ≥3. Similarly, strategy #1 compared to PI-RADS ≥ 3 could reduce 10 unnecessary biopsy procedures per 100 patients without missing any csPCa.
The best strategy requires individual decision making, taking into account personal preferences and balancing the benefits and risks of biopsy. Therefore, we present biopsy results based on PRIMARY score and PSAD in Fig. 1 and Table 4, providing an available tool for men regarding their individual risk of csPCa. However, it must be stressed that strategy #1 has a relatively high rate (9.2%) of missed csPCa. In contrast, strategy #2 and strategy#6 missed only 5.7% and 3.5% csPCa cases, respectively. From a clinical perspective, if patients and physicians have particular concerns about the risk of missing csPCa, then strategy #2 and strategy #6 were more appropriate choice compared to strategy #1. Previous research found that the prevalence of csPCa in autopsies from unscreened Caucasian men was 9% [28]. In addition, the Prostate Cancer Prevention Trial (PCPT) found that the prevalence of csPCa in men with benign DRE and a PSA of 2.1–4.0 ng/ml was 5.2% [29]. Therefore, the absence of 5.7% (strategy #2) and 3.5% (strategy #6) of csPCa from an immediate biopsy in this study seems acceptable.
The present study is not without limitations. Firstly, the analysis was retrospective and limited to a single center. PSMA PET/CT has not been the standard of care for the diagnosis of intraprostatic malignancies in the past few years, most of the included patients underwent risk assessment prior to PSMA PET/CT screening, leading to a selection bias. More data from different centers are still needed to further explore inter-center differences. Secondly, the included patients were not from a PSA-based screening population. Although we restricted PSA to <20 ng/mL, it was still high with a median of 9.3 ng/mL, resulting in a high PSAD rate of >0.2 ng/ml2. The diagnostic performance of the PRIMARY score and PSAD might differ in other populations (e.g., a screened population with low median PSA values). External validation of the presented results was needed prior to safely implement. Thirdly, since not all patients in the cohort underwent radical prostatectomy, biopsy pathology was used as a reference rather than the whole-mount pathology, resulting in an imperfect standard bias. Finally, PSMA PET/CT is a relatively new and expensive technology, its cost-effectiveness and long-term outcomes have not been explored fully.
Conclusion
The combination of PRIMARY score + PSAD allows individualized decisions to avoid unnecessary biopsy, outperforming the strategies of PI-RADS + PSAD. Further prospective trials are needed to validate these findings.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
References
Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17–48.
Hugosson J, Roobol MJ, Mansson M, Tammela TLJ, Zappa M, Nelen V, et al. A 16-yr follow-up of the European randomized study of screening for prostate cancer. Eur Urol. 2019;76:43–51.
Schroder FH, Hugosson J, Carlsson S, Tammela T, Maattanen L, Auvinen A, et al. Screening for prostate cancer decreases the risk of developing metastatic disease: findings from the European Randomized Study of Screening for Prostate Cancer (ERSPC). Eur Urol. 2012;62:745–52.
Van Poppel H, Hogenhout R, Albers P, van den Bergh RCN, Barentsz JO, Roobol MJ. A European model for an organised risk-stratified early detection programme for prostate cancer. Eur Urol Oncol. 2021;4:731–9.
Hagens MJ, van Leeuwen PJ. A future prebiopsy imaging-guided pathway to safely omit systematic biopsies and prevent diagnosis of indolent prostate cancer. Eur Urol. 2021;80:690–2.
Mottet N, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer-2020 update. part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2021;79:243–62.
Drost FH, Osses DF, Nieboer D, Steyerberg EW, Bangma CH, Roobol MJ, et al. Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst Rev. 2019;4:CD012663.
Westphalen AC, McCulloch CE, Anaokar JM, Arora S, Barashi NS, Barentsz JO, et al. Variability of the positive predictive value of PI-RADS for prostate MRI across 26 centers: experience of the society of abdominal radiology prostate cancer disease-focused panel. Radiology. 2020;296:76–84.
Smith CP, Harmon SA, Barrett T, Bittencourt LK, Law YM, Shebel H, et al. Intra- and interreader reproducibility of PI-RADSv2: a multireader study. J Magn Reson Imaging. 2019;49:1694–703.
Schoots IG, Padhani AR. Risk-adapted biopsy decision based on prostate magnetic resonance imaging and prostate-specific antigen density for enhanced biopsy avoidance in first prostate cancer diagnostic evaluation. BJU Int. 2021;127:175–8.
Pagniez MA, Kasivisvanathan V, Puech P, Drumez E, Villers A, Olivier J. Predictive factors of missed clinically significant prostate cancers in men with negative magnetic resonance imaging: a systematic review and meta-analysis. J Urol. 2020;204:24–32.
Deniffel D, Healy GM, Dong X, Ghai S, Salinas-Miranda E, Fleshner N, et al. Avoiding unnecessary biopsy: MRI-based risk models versus a PI-RADS and PSA density strategy for clinically significant prostate cancer. Radiology. 2021;300:369–79.
Hansen NL, Barrett T, Koo B, Doble A, Gnanapragasam V, Warren A, et al. The influence of prostate-specific antigen density on positive and negative predictive values of multiparametric magnetic resonance imaging to detect Gleason score 7-10 prostate cancer in a repeat biopsy setting. BJU Int. 2017;119:724–30.
Falagario UG, Jambor I, Lantz A, Ettala O, Stabile A, Taimen P, et al. Combined use of prostate-specific antigen density and magnetic resonance imaging for prostate biopsy decision planning: a retrospective multi-institutional study using the prostate magnetic resonance imaging outcome database (PROMOD). Eur Urol Oncol. 2021;4:971–9.
Washino S, Okochi T, Saito K, Konishi T, Hirai M, Kobayashi Y, et al. Combination of prostate imaging reporting and data system (PI-RADS) score and prostate-specific antigen (PSA) density predicts biopsy outcome in prostate biopsy naive patients. BJU Int. 2017;119:225–33.
Seifert R, Emmett L, Rowe SP, Herrmann K, Hadaschik B, Calais J, et al. Second version of the prostate cancer molecular imaging standardized evaluation framework including response evaluation for clinical trials (PROMISE V2). Eur Urol. 2023;83:405–12.
Emmett L, Papa N, Buteau J, Ho B, Liu V, Roberts M, et al. The PRIMARY score: using intraprostatic (68)Ga-PSMA PET/CT patterns to optimize prostate cancer diagnosis. J Nucl Med. 2022;63:1644–50.
Fendler WP, Eiber M, Beheshti M, Bomanji J, Ceci F, Cho S, et al. 68Ga-PSMA PET/CT: Joint EANM and SNMMI procedure guideline for prostate cancer imaging: version 1.0. Eur J Nucl Med Mol Imaging. 2017;44:1014–24.
Weinreb JC, Barentsz JO, Choyke PL, Cornud F, Haider MA, Macura KJ, et al. PI-RADS prostate imaging - reporting and data system: 2015, Version 2. Eur Urol. 2016;69:16–40.
Turkbey B, Rosenkrantz AB, Haider MA, Padhani AR, Villeirs G, Macura KJ, et al. Prostate imaging reporting and data system version 2.1: 2019 update of prostate imaging reporting and data system version 2. Eur Urol. 2019;76:340–51.
Epstein JI, Egevad L, Amin MB, Delahunt B, Srigley JR, Humphrey PA, et al. The 2014 International Society of Urological Pathology (ISUP) consensus conference on gleason grading of prostatic carcinoma: definition of grading patterns and proposal for a new grading system. Am J Surg Pathol. 2016;40:244–52.
Vickers AJ, Elkin EB. Decision curve analysis: a novel method for evaluating prediction models. Med Decis Mak. 2006;26:565–74.
Emmett L, Buteau J, Papa N, Moon D, Thompson J, Roberts MJ, et al. The additive diagnostic value of prostate-specific membrane antigen positron emission tomography computed tomography to multiparametric magnetic resonance imaging triage in the diagnosis of prostate cancer (PRIMARY): a prospective multicentre study. Eur Urol. 2021;80:682–9.
Jiao J, Kang F, Zhang J, Quan Z, Wen W, Zhao X, et al. Establishment and prospective validation of an SUV(max) cutoff value to discriminate clinically significant prostate cancer from benign prostate diseases in patients with suspected prostate cancer by (68)Ga-PSMA PET/CT: a real-world study. Theranostics. 2021;11:8396–411.
Chen M, Qiu X, Zhang Q, Zhang C, Zhou YH, Zhao X, et al. PSMA uptake on [68Ga]-PSMA-11-PET/CT positively correlates with prostate cancer aggressiveness. Q J Nucl Med Mol Imaging. 2022;66:67–73.
Demirci E, Kabasakal L, Sahin OE, Akgun E, Gultekin MH, Doganca T, et al. Can SUVmax values of Ga-68-PSMA PET/CT scan predict the clinically significant prostate cancer? Nucl Med Commun. 2019;40:86–91.
Fendler WP, Schmidt DF, Wenter V, Thierfelder KM, Zach C, Stief C, et al. 68Ga-PSMA PET/CT detects the location and extent of primary prostate cancer. J Nucl Med. 2016;57:1720–5.
Zlotta AR, Egawa S, Pushkar D, Govorov A, Kimura T, Kido M, et al. Prevalence of prostate cancer on autopsy: cross-sectional study on unscreened Caucasian and Asian men. J Natl Cancer Inst. 2013;105:1050–8.
Thompson IM, Pauler DK, Goodman PJ, Tangen CM, Lucia MS, Parnes HL, et al. Prevalence of prostate cancer among men with a prostate-specific antigen level < or =4.0 ng per milliliter. N Engl J Med. 2004;350:2239–46.
Funding
This study was supported by the National Natural Science Foundation of China (No. 82173204; 82302244, 82220108004), the Innovation Capability Support Program of Shaanxi (2021TD-39), and the Clinical Research Project of AFMU (2021LC2111).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by SG, JZ, JJ, ZL, CC, JC and WY. In the perspective of Nuclear Medicine, FK and JW made the supervision, project administration, review of the manuscript. YW reviewed the pathological result of biopsies. In the perspective of urology, WQ, SM, PW, YJ and WW made the supervision, project administration, review of the manuscript. In addition, WQ and JZ offered the funding. The first draft of the manuscript was written by SG and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The institutional review board (Ethics Committees of Xijing Hospital, Fourth Military Medical University) approved this study and all subjects signed a written informed consent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Guo, S., Zhang, J., Wang, Y. et al. Avoiding unnecessary biopsy: the combination of PRIMARY score with prostate-specific antigen density for prostate biopsy decision. Prostate Cancer Prostatic Dis 27, 288–293 (2024). https://doi.org/10.1038/s41391-023-00782-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41391-023-00782-z
- Springer Nature Limited
This article is cited by
-
Survival benefit of radical prostatectomy in patients with advanced TURP-diagnosed prostate cancer: a population-based real-world study
BMC Surgery (2024)
-
Elucidating the need for prostate cancer risk calculators in conjunction with mpMRI in initial risk assessment before prostate biopsy at a tertiary prostate cancer center
BMC Urology (2024)
-
Prostate cancer detection and complications of MRI-targeted prostate biopsy using cognitive registration, software-assisted image fusion or in-bore guidance: a systematic review and meta-analysis of comparative studies
Prostate Cancer and Prostatic Diseases (2024)