
Abstact
Background
Studies comparing C-RARP and RS-RARP have reported different results and the choice between the two operation methods remains controversia.
Methods
We present the meta-analysis on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. The meta-analysis was carried out using Review Manager 5.3 (Cochrane Collaboration, Oxford, United Kingdom) and Stata SE 14.0. The mean difference (MD) with 95% confidence intervals (CI) were used to describe the results of continuous data; odds ratio (OR) with 95% CI were used to describe dichotomous data. Statistical significance was set at P < 0.05.
Results
The meta-analysis revealed that RS-RARP had a statistically significant advantage in terms of continence recovery immediately after operation (OR: 0.40, 95% CI: 0.20–0.77; P = 0.007) (Fig. 2a), after 1 month (OR: 0.17, 95% CI: 0.10–0.29; P < 0.00001) (Fig. 2b), after 3 months (OR: 0.18, 95% CI: 0.09–0.36; P < 0.00001) (Fig. 2c), after 6 months (OR: 0.26, 95% CI: 0.15–0.46; P < 0.00001) (Fig. 2d) and after 12 months (OR: 0.50, 95% CI: 0.28–0.89; P = 0.02) (Fig. 2e).
Conclusions
This meta-analysis found that RS-RARP had better postoperative continence recovery than C-RARP, while sexual function recovery rates were not significantly different. There were also no significant differences in operation time, intraoperative blood loss, length of stay, positive margin rate and complications.
Similar content being viewed by others


Introduction
According to the latest data from the latest World Health Organization and the American Cancer Society in 2021, the incidence and mortality of prostate cancer rank first among the tumours of the urinary system [1, 2]. Hence, the early treatment of prostate cancer has become particularly important. The first robot-assisted radical prostatectomy (RARP) was introduced in 2001, and it is often used to treat prostate cancer [3]. In 2010, Galfano et al. reported a new surgical method for RARP via the Retzius-sparing (RS) or posterior approach [4].
Several studies reported favourable results for Retzius-sparing robot-assisted radical prostatectomy (RS-RARP), in terms of continence, compared with conventional robot-assisted radical prostatectomy (C-RARP) [4,5,6]. Previous meta-analyses have shown that RS-RARP had improved early incontinence with C-RARP, but with little long-term difference. The recovery of sexual function was also unclear [7,8,9,10]. On the basis of the current literature, we hypothesised that RS-RARP had better postoperative sexual function recovery and long-term continence recovery for patients than those of C-RARP.
This study aimed to review the current literature and evaluate the continence and sexual function between two different kinds of RARP for prostate cancer patients.
Method
This study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (number: CRD42021253732). We present this meta-analysis according to the PRISMA Guideline [11].
Search strategy
We conducted a meta-analysis under the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Two reviewers independently searched Pubmed, Embase and Web of Science up to May 6, 2021. All English published articles were searched by using the search formula: (“robot-assisted radical prostatectomy”[Title/Abstract] OR “RARP”[Title/Abstract] OR “robot-assisted laparoscopic radical prostatectomy”[Title/Abstract]) AND (“Retzius”[Title/Abstract] OR “posterior”[Title/Abstract]). The reference lists from identified publications and included studies from previous meta-analyses were also searched.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) articles that compared C-RARP with RS-RARP for the treatment of prostate cancer and (2) English language articles. The exclusion criteria were as follows: (1) conference abstract, (2) case series, (3) incomplete data and (4) duplicated data.
Data extraction
The data of the included studies were selected and extracted independently by two reviewers (Zhang and Liu). Negotiations with a third reviewer resolved any disagreements about data extraction. All records were selected in the Endnote software. All data were extracted from the included articles and placed in an Excel spreadsheet. Baseline characteristics and other data that must be analysed were directly determined from included articles. The missing data were directly retrieved from the articles’ authors via e-mail. If the data could still not be found despite these efforts, the article was excluded.
Quality assessment
The Jadad scale [12] and Newcastle-Ottawa Scale (NOS) [13] were used to evaluate the quality of randomised controlled trials (RCTs) and non-RCT studies, respectively. The NOS included eight items with a maximum of nine stars, whereas the Jadad scale ranged from 0 to 5. For both scales, higher scores are associated with higher quality. The assessment included studies and outcome levels. The Oxford Centre evaluated the level of evidence for included articles for Evidence-Based Medicine: Levels of Evidence (March 2009) [14]. Two reviewers evaluated the quality of studies independently and any disagreements were resolved by negotiation with a third reviewer.
Outcomes of interest
The main outcomes included continence and sexual function. The additional outcomes included length of stay, complications, operation time, blood loss, positive margin rate.
Statistical analysis
The meta-analysis was conducted using Review Manager 5.3 (Cochrane Collaboration, Oxford, UK) and Stata SE 14.0. Continuous data were described using the mean difference (MD) with 95% confidence intervals (CI), whereas dichotomous data were described using odds ratio (OR) with 95% CI. Statistical significance was set at P < 0.05. In addition, heterogeneity among studies was assessed using I2 and χ2 tests and was considered acceptable if P > 0.10 or I2 < 50, using a fixed-effects model. Conversely, a random-effects model was used.
Result
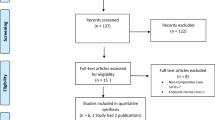
We identified 1002 records from three electronic databases (Pubmed, Embase and Web of Science). Among these, 11 studies and 12 articles [6, 15,16,17,18,19,20,21,22,23,24,25] were included for our meta-analysis after repeated screening (Fig. 1). Table 1 summarises the baseline characteristics and quality of the included studies. All included studies were published within the past 5 years, except for one published in 2014. Five of these were published within 1 year. In total, 2705 patients were included in our meta-analysis, with 1338 and 1367 in the C-RARP and RS-RARP groups, respectively.

Flow diagram of the selection process of relevant studies.
Continence recovery
RS-RARP had a statistically significant advantage in terms of continence recovery immediately after operation (OR: 0.40, 95% CI: 0.20–0.77; P = 0.007) (Fig. 2a), after 1 month (OR: 0.17, 95% CI: 0.10–0.29; P < 0.00001) (Fig. 2b), after 3 months (OR: 0.18, 95% CI: 0.09–0.36; P < 0.00001) (Fig. 2c), after 6 months (OR: 0.26, 95% CI: 0.15–0.46; P < 0.00001) (Fig. 2d) and after 12 months (OR: 0.50, 95% CI: 0.28–0.89; P = 0.02) (Fig. 2e).

Continence recovery immediately after surgery (0 month) (a), 1 month (b), 3 months (c), 6 months (d) and 12 months (e).
Sexual function recovery
Two studies [6, 22] reported sexual function recovery after RARP, but no statistically significant difference was found between RS-RARP and C-RARP after 3, 6 and 12 months (Fig. 3).

Sexual function recovery after surgery 3 months (A), 6 months (B) and 12 months (C).
Secondary outcomes
The secondary outcomes included operation time, intraoperative blood loss, length of stay, positive margin rate and complications. No statistical difference was found between RS-RARP and C-RARP regarding operation time (OR: 8.54, 95% CI: − 11.15–28.53; P = 0.40) (Fig. 4A), intraoperative blood loss (OR: − 0.27, 95% CI: − 46.18–45.64; P = 0.99) (Fig. 4B), length of stay (OR: 0.42, 95% CI: − 0.13–0.97; P = 0.14) (Fig. 4C), positive margin rate (OR: 0.92, 95% CI: 0.76–1.12; P = 0.40) (Fig. 4D) and complications (OR: 1.06, 95% CI: 0.72–1.55; P = 0.76) (Fig. 4E).

Operation time (A), intraoperative blood loss (B), length of stay (C), positive margin rate (D) and complications (E).
Publication bias and sensitivity analysis
We conducted a funnel plot (Fig. 5a) and sensitivity analysis (Fig. 5b) of continence recovery at 1 month after surgery. The funnel plot was symmetrical, indicating a lower probability of publication bias in the included studies. Sensitivity analysis was performed by removing the studies one by one; the pooled effect size remained statistically significant and the forest plot direction was consistent before and after removal.

Funnel plot (a) and sensitivity analysis (b) of continence recovery at 1 month after surgery.
Discussion
Urinary incontinence is a common complication of radical prostatectomy, and surgeons are committed to improving this problem [26]. RS-RARP is performed through the Douglas space to avoid destroying the pelvic fascia and the prostate’s anatomical structures [4]. Because of the difficulty of this operation, we compared it with the traditional method in the hopes of discovering a better way to treat patients with prostate cancer.
Continence was assessed immediately after catheter removal and at 1, 3, 6 and 12 months postoperatively. In the RS-RARP group, these recovery rates were 65.92%, 52.84%, 87.19%, 90.70% and 91.24%, respectively. In the C-RARP group, these values were 43.00%, 18.92%, 52.78%, 75% and 83.89%, respectively. Compared with C-RARP, RS-RARP had significantly better postoperative continence recovery. In both groups, the continence recovery rates were higher immediately after catheter removal compared with that 1 month postoperatively, which may be attributable to the differences among the included studies. However, there were no significant differences in sexual function recovery rates at 3, 6 and 12 months postoperatively between both groups. Furthermore, there were no significant differences in operation time, intraoperative blood loss, length of stay, positive margin rate and complications between both groups.
The previous meta-analyses conducted by Jiang et al. [7], Phukan et al. [8], Checcucci et al. [9], and Dirie et al. [10] reported improved early incontinence with RS-RARP but with little long-term difference. In our meta-analysis, which included more patients from more published studies in the last year, we found that RS-RARP had a significant difference in both early follow-up and long-term follow-up. Sexual function recovery was not significant different. The positive margin rates were 20.42% and 21.39%, whereas the complication rates were 4.65% and 4.37% in the C-RARP and RS-RARP groups, respectively. Compared with the C-RARP group, the RS-RARP group had better postoperative continence recovery. However, the differences in complication rates and positive margin rates were not statistically significant. This implies that RS-RARP might be a better choice for such patients.
Checcucci et al. reported that RS-RARP is a safe and feasible alternative to C-RARP. However, RS-RARP was found to have a higher risk of positive margin rates, which can be considered a disadvantage of this procedure [9]. Lee et al. also showed that RS-RARP had a higher positive margin rate, but similar to our study, it was not statistically significant [27]. This means that the positive margin rate remains an important problem.
Menon et al. reported that 69.2% and 86.5% of patients could achieve an erection 1 year postoperatively after C-RARP and RS-RARP, respectively (P = 0.5) [6]. The first large series of RS-RARP by Galfano et al. had a 40% rate of sexual function recovery after 1 month [5]. Unfortunately, there are not enough data to confirm this.
Kowalczyk et al. [28] and Madi et al. [29] reported that RS-RARP provided an opportunity for patients who failed primary radiation or ablation therapy. Compared with C-RARP, RS-RARP is a feasible salvage option for urinary function and quality of life outcomes. It is hard to compare the quality of life outcomes between RS-RARP and radiation because of a lack of related studies.
Our study had several limitations. First, there were not enough RCTs in our included studies. Second, most RARP surgeons are more familiar with C-RARP. Thus, the learning curve effects are likely more emphasised in the RS-RARP group. Third, different surgeons performing the RARP may have caused heterogeneity among studies.
Conclusion
This meta-analysis found that RS-RARP had better postoperative continence recovery than C-RARP, whereas sexual function recovery rates were not significantly different between the two procedures. There were also no significant differences in operation time, intraoperative blood loss, length of stay, positive margin rate and complications. The learning curve of RS-RARP likely influences its effectiveness and applicability.
References
Siegel RL, Miller KD, Fuchs HF, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021;71:7–33.
China Source: Globocan 2020. The Global Cancer Observatory, All Rights Reserved-March, 2021. Available at: https://gco.iarc.fr/today/data/factsheets/populations/160-china-fact-sheets.pdf.
Checcucci E, Amparore D, De Luca S, Autorino R, Fiori C, Porpigliaet F. Precision prostate cancer surgery: an overview of new technologies and techniques. Minerva Urol Nefrol. 2019;71:487–501.
Galfano A, Ascione A, Grimaldi S, Petralia G, Strada E, Bocciardiet AM. A new anatomic approach for robot-assisted laparoscopic prostatectomy: a feasibility study for completely intrafascial surgery. Eur Urol. 2010;58:457–61.
Galfano A, Di Trapani D, Sozzi F, Strada E, Petralia G, Bramerio M, et al. Beyond the learning curve of the Retzius-sparing approach for robot-assisted laparoscopic radical prostatectomy: oncologic and functional results of the first 200 patients with ≥ 1 year of follow-up. Eur Urol. 2013;64:974–80.
Menon M, Dalela D, Jamil M, Diaz M, Tallman C, Abdollah F, et al. Functional recovery, oncologic outcomes and postoperative complications after robot-assisted radical prostatectomy: an evidence-based analysis comparing the Retzius sparing and standard approaches. J Urol. 2018;199:1210–7.
Jiang YL, Zheng GF, Jiang ZP, Li Z, Zhou XL, Zhou J, et al. Comparison of Retzius-sparing robot-assisted laparoscopic radical prostatectomy vs standard robot-assisted radical prostatectomy: a meta-analysis. BMC Urol. 2020;20:114.
Phukan C, Mclean A, Nambiar A, Mukherjee A, Somani B, Krishnamoorthy R, et al. Retzius sparing robotic assisted radical prostatectomy vs. conventional robotic assisted radical prostatectomy: a systematic review and meta-analysis. World J Urol. 2020;38:1123–34.
Checcucci E, Veccia A, Fiori C, Amparore D, Manfredi M, Dio MD, et al. Retzius-sparing robot-assisted radical prostatectomy vs the standard approach: a systematic review and analysis of comparative outcomes. BJU Int. 2020;125:8–16.
Dirie NI, Pokhrel G, Guan W, Mumin MA, Yang J, Masau JF, et al. Is Retzius-sparing robot-assisted radical prostatectomy associated with better functional and oncological outcomes? Literature review and meta-analysis. Asian J Urol. 2019;6:174–82.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1.
Clark HD, Wells GA, Hu€et C, McAlister FA, Salmi LR, Fergusson D, et al. Assessing the quality of randomized trials: reliability of the Jadad scale. Control Clin Trials. 1999;20:448–52.
Stang A. Critical evaluation of the Newcastle-Ottawa Scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25:603–5.
Centre for Evidence-based Medicine Oxford University: Levels of Evidence (March 2009). Updated by Jeremy Howick March 2009. Available at: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009.
Abu-Ghanem Y, Dotan Z, Ramon J, Zilberman DE. Retzius space reconstruction following transperitoneal laparoscopic robot-assisted radical prostatectomy: does it have any added value? J Robot Surg. 2018;12:475–9.
Lim SK, Kim KH, Shin TY, Han WK, Chung BH, Hong SJ, et al. Retzius-sparing robot-assisted laparoscopic radical prostatectomy: combining the best of retropubic and perineal approaches. BJU Int. 2014;114:236–44.
Eden CG, Moschonas D, Soares R. Urinary continence four weeks following Retzius-sparing robotic radical prostatectomy: The UK experience. J Clin Urol. 2017;11:15–20.
Asimakopoulos AD, Topazio L, De Angelis M, Agrò EF, Pastore AL, Fuschi A, et al. Retzius-sparing versus standard robot-assisted radical prostatectomy: a prospective randomized comparison on immediate continence rates. Surg Endosc. 2019;33:2187–96.
Sayyid R, Simpson WG, Lu C, Terris MK, Klaassen Z, Madi R. Retzius-sparing robotic-assisted laparoscopic radical prostatectomy: a safe surgical technique with superior continence outcomes. J Endourol. 2017;31:1244–50.
Dalela D, Jeong W, Prasad MA, Sood A, Abdollah F, Diaz M, et al. A pragmatic randomized controlled trial examining the impact of the retzius-sparing approach on early urinary continence recovery after robot-assisted radical prostatectomy. Eur Urol. 2017;72:677–85.
Liao PC, Hung SC, Hu JC, Chiu KY. Retzius-sparing robotic-assisted radical prostatectomy facilitates early continence regardless of neurovascular bundle sparing. Anticancer Res. 2020;40:4075–80.
Egan J, Marhamati S, Carvalho FLF, Davis M, O’Neill J, Lee H, et al. Retzius-sparing robot-assisted radical prostatectomy leads to durable improvement in urinary function and quality of life versus standard robot-assisted radical prostatectomy without compromise on oncologic efficacy: single-surgeon series and step-by-step guide. Eur Urol. 2021;79:839–57. Epub 2020 Jun 11
Ota Y, Hamamoto S, Matsuyama N, Hamakawa T, Iwatsuki S, Etani T, et al. Pelvic anatomical features after Retzius-sparing robot-assisted radical prostatectomy intended for early recovery of urinary symptoms. J Endourol. 2021;35:296–304.
Lee J, Kim HY, Goh HJ, Heo JE, Almujalhem A, Alqahtani AA, et al. Retzius sparing robot-assisted radical prostatectomy conveys early regain of continence over conventional robot-assisted radical prostatectomy: a propensity score matched analysis of 1,863 patients. J Urol. 2020;203:137–44.
Umari P, Eden C, Cahill D, Rizzo M, Eden D, Sooriakumaran P. Retzius-sparing versus standard robot-assisted radical prostatectomy: a comparative prospective study of nearly 500 patients. J Urol. 2021;205:780–90.
Freire MP, Weinberg AC, Lei Y, Soukup JR, Lipsitz SR, Prasad SM, et al. Anatomic bladder neck preservation during robot-assisted laparoscopic radical prostatectomy: description of technique and outcomes. Eur Urol. 2009;56:972–80.
Lee S, Kim KB, Jo JK, Ho JN, Oh JJ, Jeong SJ, et al. Prognostic value of focal positive surgical margins after radical prostatectomy. Clin Genitourin Cancer. 2016;14:e313–9.
Kowalczyk KJ, Madi RH, Eden CG, Sooriakumaran P, Fransis K, Raskin Y, et al. Comparative outcomes of salvage Retzius-sparing versus standard robotic prostatectomy: an international, multi-surgeon series. J Urol. 2021;206:1184–91.
Madi R, Sayyid RK, Hiffa A, Thomas E, Terris MK, Klaassen Z. Early experience with salvage Retzius-sparing robotic-assisted radical prostatectomy: oncologic and functional outcomes. Urology. 2021;149:117–21.
Acknowledgements
This work was supported by grants from the Natural Science Foundation of Chongqing (cstc2019jcyj-msxmX0732), and Chongqing Science and Technology Commission (cstc2017shms-zdyf0319).
Author information
Authors and Affiliations
Contributions
JYL, JDZ and DLW contributed to the conception and design this study. ZKY, QYL, WYZ and ZZQ were responsible for the development of the methology and data interpretation. JYL, JDZ and ZKY analyzed and interpreted the data. YWX and JDZ wrote the paper. JYL, JDZ, and DLW revised the paper. JYL and JDZ contributed equally and should share first authorship. All authors read and approved the final paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Liu, J., Zhang, J., Yang, Z. et al. Comparison of Retzius-sparing and conventional robot-assisted laparoscopic radical prostatectomy regarding continence and sexual function: an updated meta-analysis. Prostate Cancer Prostatic Dis 25, 47–54 (2022). https://doi.org/10.1038/s41391-021-00459-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41391-021-00459-5
- Springer Nature Limited
This article is cited by
-
Comparison of sexual function after robot-assisted radical prostatectomy and carbon-ion radiotherapy for Japanese prostate cancer patients using propensity score matching
BMC Cancer (2024)
-
Comparison of senhance and da vinci robotic radical prostatectomy: short-term outcomes, learning curve, and cost analysis
Prostate Cancer and Prostatic Diseases (2024)
-
Single port robot-assisted radical and simple prostatectomy: a systematic review and meta-analysis
Prostate Cancer and Prostatic Diseases (2024)
-
Preliminary comparison of the modified extraperitoneal free-PORT single incision technique and transabdominal multi-incision robot-assisted laparoscopic radical prostatectomy
Scientific Reports (2023)
-
Retzius-sparing vs. standard robot-assisted radical prostatectomy for clinically localised prostate cancer: a comparative study
Prostate Cancer and Prostatic Diseases (2023)