
Abstract
Background
There is no consensus regarding the definition of pediatric metabolic syndrome (MetS). This study assessed the impact of alternative definitions on the prevalence, children identified, and association with socioeconomic status (SES).
Methods
Data were from the prospective multigenerational Dutch Lifelines Cohort Study. At baseline, 9754 children participated, and 5085 (52.1%) with average follow-up of 3.0 (SD = 0.75) years were included in the longitudinal analyses; median ages were 12 (IQR = 10–14) and 14 years (IQR = 12–15), respectively. We computed MetS prevalence according to five published definitions and measured the observed proportion of positive agreement. We used logistic regression to assess the SES–MetS association, adjusted for age and sex. Longitudinal models were also adjusted for baseline MetS.
Results
MetS prevalence and positive agreement varied between definitions, from 0.7 to 3.0% and from 0.34 (95% CI: 0.28; 0.41) to 0.66 (95% CI: 0.58; 0.75) at baseline, respectively. We consistently found a socioeconomic gradient; in the longitudinal analyses, each additional year of parental education reduced the odds of having MetS by 8% (95% CI: 1%; 14%) to 19% (95% CI: 7%; 30%).
Conclusions
Alternative MetS definitions had differing prevalence estimates and agreed on 50% of the average number of cases. Additionally, regardless of the definition, low SES was a risk factor for MetS.
Impact
-
Little is known about the impact of using different definitions of pediatric metabolic syndrome on study results.
-
Our study showed that the choice of pediatric metabolic syndrome definition produces very different prevalence estimates.
-
We also showed that the choice of definition influences the socioeconomic gradient. However, low socioeconomic status was consistently a risk factor for having pediatric metabolic syndrome.
-
In conclusion, studies using different definitions of metabolic syndrome could be reasonably compared when investigating the association with socioeconomic status but not always validly when comparing prevalence studies.
Similar content being viewed by others


Introduction
Metabolic syndrome (MetS) is defined as a clustering of cardiometabolic risk factors (i.e., central obesity, dyslipidemia, hyperglycemia, and hypertension), which is associated with increased cardiometabolic risk.1 In children, there is still very little consensus on how to define and measure MetS. Notwithstanding the uncertainties surrounding a pediatric MetS definition, it is considered a useful construct. Due to its high specificity and negative predictive value, pediatric MetS can be used to identify children who will have lower cardiometabolic risk as adults.2,3 There is also evidence to indicate that children with MetS are at increased cardiometabolic risk later in life, and such risk is highly related to non-communicable diseases like type 2 diabetes and cardiovascular diseases (CVDs).4,5 One study found that children with MetS were two to three times more likely to develop type 2 diabetes as adults compared to children without MetS.6 This makes childhood MetS an important target for potential interventions to reduce the burden of cardiometabolic diseases, which are among the leading causes of disease burden.7
The lack of agreement on the definition of pediatric MetS is reflected by the existence of various definitions,8 which are operationalized to either detect the presence or absence of MetS (dichotomous definition) or act as a continuous scale that allows for varying degrees of MetS (continuous definition). A comparative study yielded weak agreement across four dichotomous MetS definitions,1 and the choice of different definitions can result in considerably differing prevalence estimates.9 Associated with this, the choice of definition may also influence other findings, such as the strength of associations with both risk factors and health outcomes, but evidence on this topic is scarce. One study showed that the association between insulin sensitivity and pediatric MetS according to four of the most common definitions were quite similar.10 However, in this study less stringent versions of these MetS definitions were used, and the level of agreement between the different definitions was not investigated.10 The heterogeneity seen among MetS definitions influences the comparability of research, as the various definitions may regard rather different children. This is important to consider, as it hampers a synthesis of the evidence to guide researchers, clinicians, policy makers, and other healthcare professionals.
A wealth of evidence indicates that socioeconomic status (SES) is a fundamental determinant of health,11 including non-communicable diseases like type 2 diabetes and CVD, but little is known about its association with pediatric MetS. Given the evidence on a socioeconomic gradient whereby lower SES is associated with worse health outcomes,12 such as obesity13 and future cardiometabolic diseases, we believe SES is an important risk factor for pediatric MetS.14,15 However, this association has been understudied. There is some cross-sectional evidence, which supports an inverse association between SES and MetS in childhood,16,17 but as these studies use different definitions of MetS, it is not clear whether their findings can be compared. More evidence is needed, especially from longitudinal studies, to determine the relationship between SES and pediatric MetS and whether its strength differs across definitions of MetS.
Our study aims to fill the aforementioned gaps by assessing the impact of using different definitions of pediatric MetS on (a) its prevalence and the extent to which definitions identify the same children and (b) its association with SES, cross-sectionally and longitudinally.
Methods
Setting and population
Data were used from the prospective multigenerational Dutch Lifelines Cohort Study.18,19 Briefly, Dutch speaking individuals aged 25–49 were asked to participate by their physicians. Those who accepted were subsequently asked to invite their family members. Individuals could also self-register through the Lifelines website. Ultimately, 167,729 individuals participated in the baseline assessments, during which participants filled out questionnaires and, if aged ≥8 years, underwent physical exams. For the purpose of this paper, Lifelines provided the data of 15,042 children aged 0–17 years at baseline along with the relevant parental data. Children aged <8 years at baseline (n = 5288) were excluded, as the components of MetS were not assessed in this age group. This resulted in 9754 participants eligible for inclusion during the baseline assessment. Written informed consent was obtained for each participant prior to participating in the cohort. The Lifelines Cohort study is conducted according to the conventions set forth in the Declaration of Helsinki, and it has received approval from the Medical Ethics Committee of the University Medical Center Groningen (METc approval number: 2007/152). A detailed description of the recruitment strategy and data collection can be found elsewhere.18
Procedures and measures
Participants completed questionnaires and underwent physical exams and venous blood draws during both the baseline (2007–2014 and 2010–2014 in adults and children, respectively) and second assessment (2014–2018). Questionnaire data were self-reported and covered various topics, including demographics. Physical exams and venous blood draws were conducted by trained research nurses using a standardized protocol.
MetS was defined using four of the most commonly used dichotomous definitions (Cook,20 de Ferranti,21 IDEFICS,1 and IDF22) and a continuous MetS score (cMetS).23 Operationalizing the definitions required the use of anthropometric measurements and blood pressure recorded during the physical exams and fasting glucose, triglyceride, and high-density lipoprotein levels assessed using venous blood samples. Age- and sex-specific percentiles for these risk components were also used. These percentiles were taken from a study with a sample of 1976 French children, excluding children with obesity or thinness (of at least grade 2), resulting in a healthier range of body mass index values.24 The exact operationalization of the dichotomous MetS definitions is shown in Table 1.
The cMetS score was dichotomized to allow for comparison with the other MetS definitions. To construct the cMetS score, we standardized and summed the residuals for the MetS components; mean arterial pressure was used instead of both systolic and diastolic blood pressure.23 This approach allowed for systolic and diastolic blood pressure to be counted as one risk factor so that blood pressure could be given the same weighting as in the dichotomous definitions of MetS.23 We selected a cutoff point to dichotomize the continuous score that would result in a baseline prevalence equivalent to the mean prevalence of the existing dichotomous definitions at baseline.
SES was measured using either the child’s mother’s or father’s highest level of education, whichever was higher. If only one parent was registered in Lifelines at baseline, then data from that parent was used. Education was defined as the minimal years of education needed to achieve their highest education level. This was assessed by asking parents about the highest educational level they attained, with eight potential response categories ranging from “no education” to university. In an approach similar to De Graaf et al.,25 these categories were recoded into years of education using the number of years it would take to complete each category by the fastest route possible, though “no education” was recoded as 5 years of education. Parental education was used as a measure of SES, as it has been theorized that education may be the strongest predictor of cardiovascular health due to its influence in shaping an individual’s values, health behaviors, and problem-solving abilities.26 To verify this, we conducted sensitivity analyses using equivalized household income (income) and occupation, measured using Treiman’s Standard International Occupational Prestige Scale.27
Statistical analysis
We first described the demographic and clinical characteristics of the sample during both assessments. Additionally, we compared the baseline characteristics of those included and excluded from the second assessment. Second, we assessed the extent to which the different MetS definitions identify the same children. We did so by measuring the agreement between pairs of dichotomous MetS definitions at both assessments, by using the observed proportion of positive agreement,28 which indicated either excellent agreement (>0.75), fair to good agreement (0.4–0.75), or moderate to poor agreement (<0.4).29 Lastly, we assessed the associations between parental education and MetS status at both assessments using logistic regression models to assess the impact of using different MetS definitions. Sensitivity analyses were also conducted using income and occupation as different proxies of SES. We estimated the logistic regression models using a data set in which we imputed missing values for independent and dependent variables. As all missing variables were numeric, we used the predictive mean matching (20 imputations) method from mice (v3.7.0)30; low-density lipoprotein, total cholesterol, glycated hemoglobin, weight, height, hip circumference, body mass index, mean arterial pressure, age, and sex were included as predictors of the missing variables. All models were adjusted for age and sex; longitudinal models were also adjusted for baseline MetS. Analyses were conducted using the R statistical software version 3.5.2.31
Results
Sample characteristics
The cross-sectional sample consisted of 9754 children. From this sample, 5085 (52.1%) children were included in the longitudinal analyses, as 3524 (36.1%) children were lost to follow-up and 1145 (11.8%) children became 18 years old during follow-up; children who turned 18 years old were excluded because at adulthood (after age 18 years) other MetS definitions are applied. Table 2 provides a summary of the demographic and clinical characteristics of the children included at each assessment. On average, the length of follow-up for our sample was 3 years (standard deviation (SD): 0.75). The children excluded from the second assessment were older, had a higher prevalence of MetS, and came from slightly lower SES backgrounds than the children included in the analyses (Table 3).
Prevalence and agreement of definitions
For most definitions, the prevalence of MetS increased between the baseline and second assessment. Additionally, each definition produced different prevalence estimates, with a more than fourfold difference between the lowest and highest estimates (Table 2). There was generally fair to good agreement between MetS definitions. The level of agreement ranged from 0.34 (95% confidence interval (CI): 0.28; 0.41) to 0.66 (95% CI: 0.58; 0.75) at baseline and from 0.32 (95% CI: 0.25; 0.39) to 0.74 (95% CI: 0.68; 0.80) at the second assessment, showing general improvement of agreement during the second assessment (Table 4). The agreement between the de Ferranti and IDF definitions was moderate to poor at both assessments and between the de Ferranti and cMetS definitions moderate to poor at the second assessment (Table 4).
Association between SES and MetS: cross-sectional and longitudinal
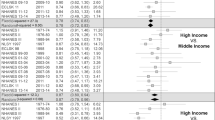
In the cross-sectional analyses, all MetS definitions showed an inverse association with parental education, with additional years of education protecting against MetS (Table 5). The strengths of these associations varied across the definitions, but the CIs of the odds ratios did overlap and differed little between the unadjusted and adjusted analyses (Table 5). In the adjusted analyses, for each additional year of parental education, the odds of having MetS compared to not having MetS ranged from a decrease of 15% (95% CI: 10%; 19%) to a decrease of 23% (95% CI: 13%; 31%) (Table 5), depending on the definition used. The sensitivity analyses yielded similar findings (Table 5).
In the longitudinal analyses, all MetS definitions maintained an inverse association between parental education and MetS over time (Table 5). In the adjusted longitudinal models, each additional year of parental education reduced the odds of having MetS compared to not having MetS by 8% (95% CI: 1%; 14%) to 19% (95% CI: 7%; 30%) (Table 5), depending on the definition used. Similar results were also seen when using occupation to measure SES; however, when using income, there was no longer any association with MetS (Table 5). Generally, the cross-sectional and longitudinal associations were similar, with overlap between the CIs (Table 5).
Discussion
Across the definitions, the average agreement was about 0.50 (i.e., the pairs of definitions agreed on 50% of the average number of cases). While this level of agreement between definitions is considered fair to good from a statistical point of view, the choice of definitions did influence the prevalence estimates, leading to a more than fourfold difference between the highest and lowest estimates. Additionally, the choice of definition influenced the estimated strength of the association between SES and MetS, resulting in an average of a 9.5 percentage point difference between the highest and lowest estimates. However, regardless of which definition was used, the results showed a socioeconomic gradient, whereby children from low SES backgrounds were more likely to have MetS than children from higher SES backgrounds. For example, if we use the most conservative estimate from the longitudinal analyses, children whose parents completed university education would have an additional 28.4% reduction in the odds of having MetS compared to children whose parents only completed secondary school.
The different definitions produced varying prevalence estimates, confirming previous findings.9 However, we generally found fair to good agreement between definitions, whereas a previous study using kappa indices to measure agreement found poor agreement between the Cook,20 IDEFICS,1 and IDF22 definitions.1 This could be partly explained by differences in the age of the cohorts, with the cohort in this previous study being much younger (aged 2–9 years at baseline) than our cohort.1 This hypothesis is in line with our finding that the level of agreement of MetS definitions increased at the second assessment, which may be explained by the increased prevalence of MetS as children age and accumulate more risk factors. It is important to note that the prevalence of pediatric MetS is relatively low. A global review estimated that the median prevalence was 3.3%.9 The cohort in the aforementioned study also reported a rather low prevalence (0.4–5.5%).1 Low prevalence estimates are known to unduly influence agreement when measured using kappa.1,32 We therefore chose not to use kappa and instead used the observed proportion of positive agreement, which indicates the proportion of agreement across the average number of MetS cases and is not dependent on prevalence.
We found that the more stringent definitions of MetS, such as the IDF definition in which increased waist circumference is a prerequisite,22 typically led to stronger associations with SES. However, all definitions consistently showed a socioeconomic gradient whereby children from low SES backgrounds were more likely to develop MetS than children from higher SES backgrounds. However, we did not find an association between income and MetS during the second assessment. Our findings are generally consistent with previous research into the association between SES and MetS.16,17 Furthermore, our finding that the choice of MetS definition did not overly influence the overall findings of our study is also consistent with previous research, which looked at the association between MetS and insulin sensitivity.10 Therefore, we feel that future research into the socioeconomic gradient of MetS among children can safely apply any of the MetS definitions used in this paper.
Strengths and limitations
The strengths of this study lie in its large sample size, its community-based nature, and the high-quality data derived from Lifelines.16 The standardized protocol for performing physical exams and collecting blood samples resulted in accurate measures of the various components of MetS. This, in addition to the large sample size, allowed us to more fully implement various MetS definitions compared to a previous study.10
It is important to point out some limitations of this study as well. First, the children lost to follow-up come from slightly lower SES backgrounds and have a higher prevalence of MetS, so not accounting for them could introduce selection bias into the study (Table 3). Additionally, the prevalence of MetS according to the IDF22 definition may have been underestimated due to a lack of medication information.22 This likely led to non-differential misclassification of the outcome, which would result in an underestimation of the strength of the association; however, dyslipidemia and hypertension in children are primarily treated through lifestyle interventions,33,34 so there was likely minimal misclassification present. It should also be noted that we could not account for pubertal status, which is known to influence cardiometabolic risk factors.35 For example, puberty influences insulin resistance, which is why some believe that it plays a role in the development of adverse metabolic health.36 Lastly, we could not account for ethnic difference due to our cohort consisting mainly of Caucasians, which is representative of this region of the Netherlands.37 This definitely deserves further study.
Implications
Our study added empirical evidence to understand the comparability of findings using different definitions of MetS. Given the lack of a universal definition of pediatric MetS, this is highly relevant for the interpretation of studies investigating the prevalence and socioeconomic gradient of MetS. Although the classification of the agreement between the definitions can be considered fair to good, it may not be wise to compare prevalence studies that use different definitions of MetS because they may differentially classify which children do or do not have MetS. However, when comparing results of studies looking at the association between SES and MetS that use different definitions, it is probably a reasonable assumption that the studies captured similar enough groups of children. Further research is needed to ensure that this holds true for other associations as well.
The difficulty in comparing prevalence studies highlights the need for a unifying definition of pediatric MetS. While most definitions agree on which risk factors comprise MetS, there is still some disagreement about whether or not certain risk factors are prerequisite (e.g., waist circumference in the IDF definition). Additionally, the various definitions tend to use different cutoffs for these risk factors. As shown in our results, these differences have implications for the identification of cases. To create a unifying MetS definition, it may be helpful to first gain a more in-depth understanding of the biological pathways involved in MetS. This would allow for further discussion as to what are the key components of MetS, whether certain components are a precondition, and which cutoffs should be implemented.
Given the stability of the results, when studying the association between SES and MetS one could choose to employ the MetS definition that is most easy to apply given the available data or given the resources available to collect data. This is especially beneficial for researchers using data from routine healthcare services that may not have all available data recorded. Furthermore, it is unclear whether using these pediatric definitions as prognostic or predictive indicators of future cardiometabolic health would lead to different results. For this reason, we need further studies to compare which definitions of pediatric MetS are most predictive of future cardiometabolic risk.
In addition, our findings support previous advice that special attention should be given to the prevention of MetS in children from low SES backgrounds, as they are particularly at risk of developing MetS. As previously stated, it is important to note that these findings may not be applicable to other ethnic groups. However, we feel that our findings are relevant to other Caucasian populations.
Conclusion
The existing definitions of MetS generally agreed on 50% of the average number of cases of MetS and consistently show that low SES is an important risk factor of having MetS. This stresses the importance of devoting more resources to reducing MetS among people with low SES; reducing this socioeconomic gradient would benefit the well-being and growth of both individuals and society.38
References
Ahrens, W. et al. Metabolic syndrome in young children: definitions and results of the IDEFICS study. Int. J. Obes. 38(Suppl 2), S4–S14 (2014).
Schubert, C. M., Sun, S. S., Burns, T. L., Morrison, J. A. & Huang, T. T. Predictive ability of childhood metabolic components for adult metabolic syndrome and type 2 diabetes. J. Pediatr. 155, S6 e1–S6 e7 (2009).
Huang, T. T., Nansel, T. R., Belsheim, A. R. & Morrison, J. A. Sensitivity, specificity, and predictive values of pediatric metabolic syndrome components in relation to adult metabolic syndrome: the Princeton LRC follow-up study. J. Pediatr. 152, 185–190 (2008).
Magnussen, C. G. et al. Continuous and dichotomous metabolic syndrome definitions in youth predict adult type 2 diabetes and carotid artery intima media thickness: the Cardiovascular Risk in Young Finns Study. J. Pediatr. 171, 97–103 (2016).
Puolakka, E. et al. Childhood socioeconomic status in predicting metabolic syndrome and glucose abnormalities in adulthood: the Cardiovascular Risk in Young Finns Study. Diabetes Care 39, 2311–2317 (2016).
Magnussen, C. G. et al. Pediatric metabolic syndrome predicts adulthood metabolic syndrome, subclinical atherosclerosis, and type 2 diabetes mellitus but is no better than body mass index alone: the Bogalusa Heart Study and the Cardiovascular Risk in Young Finns Study. Circulation 122, 1604–1611 (2010).
IHME. GBD Compare Data Visualization (University of Washington, Seattle, WA, 2020).
Magge, S. N. et al. The metabolic syndrome in children and adolescents: shifting the focus to cardiometabolic risk factor clustering. Pediatrics 140, e20171603 (2017).
Friend, A., Craig, L. & Turner, S. The prevalence of metabolic syndrome in children: a systematic review of the literature. Metab. Syndr. Relat. Disord. 11, 71–80 (2013).
Henderson, M., Van Hulst, A., von Oettingen, J. E., Benedetti, A. & Paradis, G. Normal weight metabolically unhealthy phenotype in youth: do definitions matter? Pediatr. Diabetes 20, 143–151 (2019).
Braveman, P. & Gottlieb, L. The social determinants of health: it’s time to consider the causes of the causes. Public Health Rep. 129(Suppl 2), 19–31 (2014).
Marmot, M. & Bell, R. Fair society, healthy lives. Public Health 126 Suppl 1, S4–S10 (2012).
Gebremariam, M. K., Lien, N., Nianogo, R. A. & Arah, O. A. Mediators of socioeconomic differences in adiposity among youth: a systematic review. Obes. Rev. 18, 880–898 (2017).
Maty, S. C., Lynch, J. W., Raghunathan, T. E. & Kaplan, G. A. Childhood socioeconomic position, gender, adult body mass index, and incidence of type 2 diabetes mellitus over 34 years in the Alameda County Study. Am. J. Public Health 98, 1486–1494 (2008).
Pollitt, R. A., Rose, K. M. & Kaufman, J. S. Evaluating the evidence for models of life course socioeconomic factors and cardiovascular outcomes: a systematic review. BMC Public Health 5, 7 (2005).
Iguacel, I. et al. Prospective associations between socioeconomically disadvantaged groups and metabolic syndrome risk in European children. Results from the IDEFICS study. Int. J. Cardiol. 272, 333–340 (2018).
MacPherson, M., de Groh, M., Loukine, L., Prud’homme, D. & Dubois, L. Prevalence of metabolic syndrome and its risk factors in Canadian children and adolescents: Canadian Health Measures Survey Cycle 1 (2007-2009) and Cycle 2 (2009-2011). Health Promot. Chronic Dis. Prev. Can. 36, 32–40 (2016).
Scholtens, S. et al. Cohort profile: LifeLines, a three-generation cohort study and biobank. Int. J. Epidemiol. 44, 1172–1180 (2015).
Stolk, R. P. et al. Universal risk factors for multifactorial diseases: LifeLines: a three-generation population-based study. Eur. J. Epidemiol. 23, 67–74 (2008).
Cook, S., Weitzman, M., Auinger, P., Nguyen, M. & Dietz, W. H. Prevalence of a metabolic syndrome phenotype in adolescents: findings from the third National Health and Nutrition Examination Survey, 1988-1994. Arch. Pediatr. Adolesc. Med. 157, 821–827 (2003).
de Ferranti, S. D. et al. Prevalence of the metabolic syndrome in American adolescents: findings from the Third National Health and Nutrition Examination Survey. Circulation 110, 2494–2497 (2004).
Zimmet, P. et al. The metabolic syndrome in children and adolescents - an IDF consensus report. Pediatr. Diabetes 8, 299–306 (2007).
Eisenmann, J. C., Laurson, K. R., DuBose, K. D., Smith, B. K. & Donnelly, J. E. Construct validity of a continuous metabolic syndrome score in children. Diabetol. Metab. Syndr. 2, 8 (2010).
Mellerio, H. et al. Novel modeling of reference values of cardiovascular risk factors in children aged 7 to 20 years. Pediatrics 129, e1020–e1029 (2012).
De Graaf, N. D., De Graaf, P. M. & Kraaykamp, G. Parental cultural capital and educational attainment in the Netherlands: a refinement of the cultural capital perspective. Sociol. Educ. 73, 92–111 (2000).
Winkleby, M. A., Jatulis, D. E., Frank, E. & Fortmann, S. P. Socioeconomic status and health: how education, income, and occupation contribute to risk factors for cardiovascular disease. Am. J. Public Health 82, 816–820 (1992).
Treiman, D. J. Occupational Prestige in Comparative Perspective (Academic Press, 1977).
Cicchetti, D. V. & Feinstein, A. R. High agreement but low kappa: II. Resolving the paradoxes. J. Clin. Epidemiol. 43, 551–558 (1990).
Kirkwood, B. R. & Sterne, J. A. C. In Essential Medical Statistics Ch. 36 (Blackwell Science, Malden, MA, 2003).
van Buuren, S. & Groothuis-Oudshoorn, K. mice: Multivariate imputation by chained equations in R. J. Stat. Softw. 45, 67 (2011).
R Core Team. R: A Language and Environment for Statistical Computing (R Foundation for Statistical Computing, Vienna, 2018).
Byrt, T., Bishop, J. & Carlin, J. B. Bias, prevalence and kappa. J. Clin. Epidemiol. 46, 423–429 (1993).
Grundy, S. M. et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 139, e1082–e1143 (2019).
Flynn, J. T. et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics 140, e20171904 (2017).
Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: summary report. Pediatrics 128(Suppl 5), S213–S256 (2011).
DeBoer, M. D. Assessing and managing the metabolic syndrome in children and adolescents. Nutrients 11, 1788 (2019).
Klijs, B. et al. Representativeness of the LifeLines Cohort Study. PLoS ONE 10, e0137203 (2015).
WHO. Healthy, Prosperous Lives for All: The European Health Equity Status Report (WHO Regional Office for Europe, Copenhagen, 2019).
Acknowledgements
The authors are grateful to Josué Almansa, PhD (Department of Health Sciences, University Medical Center Groningen, University of Groningen) who provided valuable methodological guidance when discussing how to impute data and measure agreement. This study is part of the TRANSSES project which is funded by ZonMw (Grant 531003011).
Author information
Authors and Affiliations
Contributions
A.L. conceptualized and designed this study, carried out the analyses, drafted the initial manuscript, and reviewed and revised the manuscript. M.L.A.d.K. and S.A.R. conceptualized, designed, and supervised this study; reviewed and revised the manuscript; conceived the project; and obtained the grant for the project TRANSSES. A.F.d.W. conceptualized, designed, and supervised this study and reviewed and revised the manuscript. All authors read and approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Consent statement
This study uses data from the Lifelines Cohort study, which obtained written informed consent for each participant prior to participating in the cohort.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lepe, A., de Kroon, M.L.A., de Winter, A.F. et al. Alternative pediatric metabolic syndrome definitions impact prevalence estimates and socioeconomic gradients. Pediatr Res 90, 694–700 (2021). https://doi.org/10.1038/s41390-020-01331-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-020-01331-3
- Springer Nature America, Inc.
This article is cited by
-
Educational inequalities in metabolic syndrome prevalence, timing, and duration amongst adults over the life course: a microsimulation analysis based on the lifelines cohort study
International Journal of Behavioral Nutrition and Physical Activity (2023)
-
Comparison of the ability of HOMA-IR, VAI, and TyG indexes to predict metabolic syndrome in children with obesity: a cross-sectional study
BMC Pediatrics (2023)