
Abstract
Background/Objectives
Overweight and obesity (OWOB) is a global epidemic. Adults and adolescents from low-income households are at higher risk to be OWOB. This study examined the relationship between income and OWOB prevalence in children and adolescents (518 years) in the United States (US) within and across race/ethnicities, and changes in this relationship from 1971 to 2014.
Subjects/Methods
A meta-analysis of a nationally representative sample (N = 73,891) of US children and adolescents drawn from three datasets (i.e., National Health and Nutrition Examination Survey, National Longitudinal Survey of Youth, & the Early Childhood Longitudinal Program) which included 14 cross-sectional waves spanning 1971–2014 was conducted. The exposure was household income-to-poverty ratio (low income = 0.00–1.00, middle income = 1.01–4.00, high income >4.00) with prevalence of overweight or obesity (body mass index ≥ 85th percentile) as the outcome.
Results
Children and adolescents from middle-income and high-income households were 0.78 (95% CI = 0.72, 0.83) and 0.68 (95% CI = 0.59, 0.77) times as likely to be OWOB compared to children and adolescents in low-income households. Separate analyses restricted to each racial/ethnic group showed children and adolescents from middle- and high-income households were less likely to be OWOB compared to their low-income peers within the White, Hispanic, and Other race/ethnic groups. Children and adolescents from low-income households who were Black were not more likely to be OWOB than their high- and middle-income counterparts. Analyses within each income stratum indicated that race/ethnicity was not related to the prevalence of OWOB in low-income households. However, racial/ethnic differences in OWOB were evident for children and adolescents in middle- and high-income households. Disparities in the prevalence of OWOB between low-income children and adolescents and their middle- and high-income counterparts have increased from 1971 to 2014.
Conclusions
Income and OWOB are related in US children and adolescents. Racial/ethnic differences in the prevalence of OWOB emerge in middle- and high-income households. Disparities in OWOB prevalence are growing.
Similar content being viewed by others
Introduction
The growing prevalence of children and adolescents (5–18 years) who are overweight or obese is global epidemic. Similarly in the United States (US) rates of OWOB in children and adolescents has nearly doubled over the last three decades [1]. This is troubling because OWOB is linked to a variety of non-communicable diseases, including cardiovascular disease, type 2 diabetes, hypertension, sleep apnea, and asthma [2,3,4,5,6]. Research from around the world has consistently shown that individuals from low-income families in highly developed countries are at increased risk for being OWOB [7, 8]. Similarly, adolescents [9, 10] and adults [11, 12] in the US from low-income families are at a higher risk of being OWOB than their higher income counterparts. Further, children in low-income families are more likely to become OWOB by the age of 5 than their high-income counterparts [13].
Evidence suggests the relationship between income and OWOB in the US may vary by individuals’ racial ethnic backgrounds [13,14,15,16]. While studies have established the relationship between income and prevalence of OWOB, we are aware of only three studies of US children and adolescents that have explored the interaction between race/ethnicity, income, and OWOB. All three of these studies have used data from the National Health and Nutrition Examination Survey (NHANES) [15, 17, 18]. The first study showed that from 1971 to 2002 the relationship between income and OWOB was inconsistent between race groups. Further, the study concluded that the relationship was weakening over time [17]. The second study included two more years of data (i.e., 2003–2004) and again concluded that relationships between income and OWOB varied by racial ethnic group. However, the study found that the strength of the relationship between income and the prevalence of OWOB was growing over time for children who are Hispanic. The final study is the only one that has examined data on this relationship between 2003 and 2014 [19]. This study found that lower income levels were associated with rates of OWOB in non-Hispanic White and Hispanic children but not in non-Hispanic Black or Asian children and concluded that disparities in OWOB may be growing over time. Thus, there is conflicting evidence in the literature on the relationship between income, race, and OWOB in children and adolescents.
The purpose of this paper is to examine the relationship between income, race, and obesity in US children and adolescents using three nationally representative datasets which include data from 1971 to 2014. We will accomplish this by examining the following research questions:
-
(1)
Does the prevalence of OWOB in children and adolescents differ by household income level?
-
(2)
Within individual racial/ethnic groups, does the prevalence of OWOB in children and adolescents differ by household income level?
-
(3)
Within household income levels, does the prevalence of OWOB in children and adolescents differ by racial/ethnic groups?
Materials/subjects and methods
Samples
The data presented herein are from three nationally representative datasets in the US [20,21,22]. Across all three datasets the sample for the analyses was restricted to children and adolescents (5–18 years) and included the following racial/ethnic categories: White, Black, Hispanic, and Other. The first dataset, NHANES, is designed to provide a nationally representative cross-sectional snapshot of the US population’s health [22]. Data collection is conducted at successive time points using surveys and examinations. The current study used NHANES I (1971–1974), NHANES II (1976–1980), NHANES III (1988–1994), and the NHANES samples collected every two years from 1999 to 2014 (e.g., 1999–2000, 2001–2002, etc.). The second dataset, the Early Childhood Longitudinal Study Kindergarten Cohort (ECLSK), is a longitudinal study designed to examine the early school experiences, school readiness, and development of US children [20]. This study includes both the 1998 and the 2011 cohort. Data from the first available measurement wave, where household income and height and weight were recorded, were included for each cohort (fall 1998 ECLSK-1998 and spring 2011 ECLSK-2011). The final dataset is the National Longitudinal Survey of Youth 1997 Cohort, a longitudinal study that follows US children born from 1980 to 1984. The cohort was first interviewed in 1997 [21]. Baseline data from the National Longitudinal Survey of Youth 1997 are included in this study. These datasets were chosen for two reasons. Their selection maximized the coverage of data across years. Apart from 10 years (i.e., 1975, 1981–1987, and 1995–1996) data were collected each year from 1971 to 2014. Second, because the number of minorities in each dataset is relatively small and becomes smaller when examining minorities across income groups, it was necessary to combine the three datasets to increase the sample size within each racial/ethnic and income group. Demographics of the children and adolescents included from all three datasets and data collection waves are presented in Table 1. Because all data were freely available online, and deidentified, this study was exempt from IRB review at the lead authors institution.
Income-to-poverty ratio
This study used income-to-poverty ratio as a measure of income status. The income-to-poverty ratio is a ratio calculated using total household income and represents the ratio of household income to poverty. Based upon the US Department of Health and Human Services’ poverty guidelines [23], the index is calculated by dividing total household income by the poverty guideline. For example, an income-to-poverty ratio of 0.5 indicates that a household is earning 50% the amount of income as the federally established poverty level, while an income-to-poverty ratio of 1.5 indicates that a household is earning 150% of the poverty level. The income-to-poverty ratio was included in every NHANES dataset and the National Longitudinal Survey of Youth dataset. For both the ECLSK-1998 and ECLSK-2011 datasets, the income-to-poverty ratio was calculated for this analysis by dividing total household income by the poverty guideline [23] for the year that the anthropometric data were collected. Consistent with previous research [15], each child across all datasets was assigned to the low-, middle-, or high-income group based on their family’s income-to-poverty ratio score. Children and adolescents in households with an income-to-poverty ratio of 0.00–1.00 were assigned to the low-income group. Likewise, children and adolescents living in a household with an income-to-poverty ratio of 1.01–4.00 were assigned to the middle-income group and children and adolescents living in households above 4.00 were classified to the high-income group.
Anthropometry
In each dataset, height and weight were measured using standardized techniques and calibrated equipment. Body mass index (BMI) was calculated using the standard formula (i.e., \({\mathrm{BMI}}=\frac{{\mathrm {kilograms}}}{({\mathrm {meter}})^2}\)). Children and adolescents were categorized as either OWOB using the sex-specific CDC growth chart percentiles for age [24].
Race/Ethnicity
Race/ethnicity of children and adolescents was collected in each of the datasets via self-report by the parent guardian of the participant. In order to align with previous work using the ECLS and NHANES datasets [12, 25], we employed a stepwise process for designating children and adolescents into racial/ethnic categories. First, children and adolescents who were reported as Hispanic were categorized as Hispanic regardless of race. Next, children and adolescents who were reported as Black were assigned to the Black category. Next, children and adolescents who were reported as White and had not been assigned to another category were assigned to the White category. Finally, children and adolescents who were not assigned to any of the previous categories were assigned to the Other racial/ethnic category.
Statistical analyses
All analyses were complete in 2017. The relationship between race/ethnicity, income and OWOB status was examined in a multi-step analysis. In the first step separate logistic regression models estimated the relationship between race/ethnicity and income-level. The models included in step one are separated by research question and described below.
Research question #1: Does the prevalence of OWOB in children and adolescents differ by household income level?
Logit models, with income-to-poverty ratio (i.e., low income, middle income, high income) as the independent variable, and OWOB status (i.e., dichotomous OWOB or not OWOB) as the dependent variable were conducted for each dataset and data collection wave. These models included race/ethnicity as a covariate and all possible race/ethnicity-by-income level interaction terms. The main effect of the association between income-to-poverty ratio and OWOB status was extracted for inclusion in step two in order to examine the relationship between household income and OWOB status. Henceforth, this approach is referred to as the “full model.” All models included age and sex as covariates.
Research question #2: Within individual racial/ethnic groups does the prevalence of OWOB in children and adolescents differ by household income level?
Separate logistic regression models for each racial/ethnic group were estimated for each dataset and data collection wave. Income-to-poverty ratio (i.e., low income, middle income, high income) and OWOB status were the independent and dependent variables, respectively. All models included age and sex as covariates. The main effect of the association between income-to-poverty ratio and OWOB status was extracted for inclusion in step two in order to examine the relationship between household income and OWOB status within each racial/ethnic group separately.
Research question #3: Within household income levels does the prevalence of OWOB in children and adolescents differ by racial/ethnic groups?
Separate logistic regression models for each income category (i.e., low, middle, high) with race/ethnicity and OWOB status as the independent and dependent variables, respectively, were completed for each dataset and data collection wave. All models included age and sex as covariates. The main effect of the association between race/ethnicity and OWOB status was extracted for inclusion in step two in order to examine the relationship between race/ethnicity and OWOB status within each income level separately.
Step two consisted of estimating summary odds ratios (OR) using the extracted main effects from the logistic regression models conducted across datasets and data collection waves in step one. This meta-analytic approach was completed in Comprehensive Meta-Analysis (v.3.3 Englewood, NJ) using both fixed and random effects. The summary ORs were interpreted to determine (1) the relationship between household income and OWOB, (2) the relationship between household income and OWOB within individual race/ethnic groups, and (3) the relationship of race/ethnicity with OWOB within each household income level. I-squared statistics were calculated to estimate the heterogeneity of effects across datasets and data collection waves.
Step three consisted of conducting a sensitivity analysis to examine the impact of individual datasets on the pooled meta-analytic ORs. We used a “one study removed” approach where the summary OR is recalculated multiple times [26]. In each recalculation one dataset is removed to detect if the removed dataset is unduly influencing the summary OR estimate. This analysis was completed using Comprehensive Meta-Analysis.
Finally, step four consisted of conducting a meta-regression analysis to determine the impact of data collection decade on the relationship between income, race/ethnicity, and OWOB status. Separate meta-regression models were estimated for each of the analytic approaches identified in steps one and two using Comprehensive Meta-Analysis with study decade as the independent variable and odds of being OWOB as the dependent variable.
Results
The results from each of the analyses are presented below. For simplicity and because the fixed and random effects ORs did not vary meaningfully, we only discuss the random effects OR estimates below. However, fixed and random effects estimates are presented in all relevant figures.
Odds ratios of OWOB
Research question #1: Does the prevalence of OWOB in children and adolescents differ by household income level?
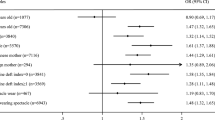
Figure 1 illustrates the results from the full model. After controlling for race and race × income interactions, there was a significant main effect for income level, with children and adolescents in the middle-income group 0.78 (95% CI = 0.72–0.83) times as likely as children and adolescents in the low-income group to be classified as OWOB. Children and adolescents in households classified as high income were 0.87 (95% CI = 0.79–0.96) and 0.68 (95% CI = 0.59–0.77) times as likely to be OWOB as children and adolescents living in households classified as middle or low income, respectively.

Forest plot of the odds of overweight or obese by income level when controlling for race/ethnicity, age, and sex
Research question #2: Within individual racial/ethnic groups does the prevalence of OWOB in children and adolescents differ by household income level?
Figure 2 depicts the results from the meta-analysis exploring the relationship between income and OWOB status by each racial/ethnic category. Children and adolescents who were classified as White and living in middle-income households were 0.90 (95% CI = 0.83–0.99) times as likely to be OWOB as their low-income counterparts, while White children and adolescents living in high-income households were 0.78 (95% CI = 0.72–0.84) and 0.69 (95% CI = 0.60–0.79) times as likely to be OWOB as their middle- and low-income counterparts. Similarly, high-income children and adolescents who were classified as Hispanic were statistically significantly less likely to be OWOB than children and adolescents who were Hispanic and living in low (OR = 0.68, 95% CI = 0.61–0.76) or middle (OR = 0.63, 95% CI = 0.56–0.71) income households. Finally, children and adolescents classified as having an Other racial/ethnic background and living in middle-income households were 0.77 (95% CI = 0.60–0.98) times as likely to be OWOB as their low-income counterparts, while children and adolescents classified as Other and living in high-income households were 0.73 (95% CI = 0.54–1.00) and 0.55 (95% CI = 0.44–0.69) times as likely to be OWOB as their middle- and low-income counterparts. Contrary to the other race/ethnic groups, children and adolescents who were classified as Black and living in middle-income households were 1.13 (95% CI = 1.04–1.22) times as likely to be OWOB as their counterparts living in low-income households, while children and adolescents who were Black and living in high-income households were 1.00 (95% CI = 0.86–1.16) and 1.14 (95% CI = 1.00–1.30) times as likely to be OWOB as children and adolescents in middle- and low-income households, respectively.

Forest plot of the odds of overwight or obese by income level by each race/ethnicity when controlling for age and sex
Research question #3: Within household income levels does the prevalence of OWOB in children and adolescents differ by racial/ethnic groups?
Figure 3 presents the results of the meta-analyses examining relationship between OWOB status and race/ethnicity by income level. For children and adolescents living in low-income households, those who were classified as Hispanic were 1.39 (95% CI = 1.24–1.56) and 1.26 (95% CI = 1.09–1.51) times as likely to be OWOB as children and adolescents classified as White and Other, respectively. Further, children and adolescents classified as Black were 0.75 (95% CI = 0.68–0.83) times as likely to be OWOB as children and adolescents classified as Hispanic. For children and adolescents living in middle-income households, those who were classified as Black were 0.87 (95% CI = 0.79–0.97), 1.36 (95% CI = 1.21–1.53), and 1.30 (95% CI = 1.16–1.44) times as likely to be OWOB as their Hispanic, White, and Other counterparts. Children and adolescents classified as Hispanic were 1.64 (95% CI = 1.44–1.87) and 1.52 (95% CI = 1.36–1.70) times as likely to be OWOB as their Other and White counterparts, respectively. For children and adolescents in high-income households, those who were classified as Black were 1.27 (95% CI = 1.09–1.47), 1.93 (95% CI = 1.52–2.45), and 1.74 (95% CI = 1.55–1.95) times as likely to be OWOB as their Hispanic, Other, and White counterparts, respectively. Children and adolescents who were classified as Hispanic were 1.47 (95% CI = 1.27–1.70) and 1.37 (95% CI = 1.23–1.53) times as likely to be OWOB as their Other and White counterparts, respectively. All other differences across income categories in the odds of children and adolescents being classified as OWOB were not statistically significant.

Forest plot of the odds of overwight or obese by each race/ethnicity when controlling for age and sex
Sensitivity analysis
Our primary findings were robust in terms of the direction and magnitude of effects throughout the “one study removed” sensitivity analysis. In three instances the “one study removed” analysis indicated the pooled OR lost statistical significance when one dataset was removed from the meta-analysis. Specifically, this was true for the meta-analysis comparing children and adolescents classified as Other in high-income households to children and adolescents classified as Other in middle-income households, the meta-analysis comparing children and adolescents classified as Other in middle-income households to children and adolescents classified as Other in low-income households, and the comparison between children and adolescents classified as White in middle-income households to children and adolescents classified as Other in low-income households. In all instances the magnitude and direction of the pooled OR remained constant. This gives us confidence that our findings are not unduly influenced by a single dataset.
Meta-regression analysis
Results from the meta-regression examining the influence of study decade on odds of being OWOB from the full model are presented in Fig. 4 (results from all models presented in Table 2). The full model indicated that for all comparisons (i.e., middle vs. low, high vs. middle, and high vs. low income), disparities in OWOB prevalence were becoming larger over time, with the higher income level becoming less likely to be OWOB every decade from 1971 until 2014 in comparison to lower income group. This difference was statistically significant for the middle vs. low income (OR = 0.93, 95% CI = 0.86–0.99) and high vs. low income (OR = 0.95, 95% CI = 0.89–1.00) comparisons, but not for the high vs. middle income (OR = 0.96, 95% CI = 0.91–1.01) comparison. These findings indicate that disparities between low-income and middle-income children and adolescents grew by 7% each decade from the 1970s until 2014. Similarly, the gap in the odds of being OWOB between low-income and high-income children and adolescents widened by 5% each decade over the same time period.

Odds of overwight or obese between income groups by decade of data collection
Discussion
Findings from this study indicate that household income is independently related to US children and adolescents’ OWOB status. Furthermore, there was a clear stair-stepping pattern of increased risk of OWOB from children and adolescents in low-income to high-income households. This finding was consistent within analyses restricted to racial/ethnic groups, except for children and adolescents who were Black. Findings also indicate that these disparities are widening over time. Finally, this meta-analysis indicates that race/ethnicity is not related to differences in prevalence of OWOB for children and adolescents who live in poverty, except for children and adolescents who are Hispanic. Differences in OWOB prevalence by racial/ethnic groups do emerge for children and adolescents living in middle- and high-income households.
Three previous studies have explored the relationship between race/ethnicity, income, and OWOB in US children and adolescents [15, 17, 19]. The findings of the current study extend the finding of the previous studies through 2014 and includes two additional nationally representative datasets. The current study is consistent with the previous studies which found low-income children and adolescents in the US who were White or Hispanic were more likely to be OWOB, but found that this relationship did not hold for children and adolescents who were Black. Further, the current study indicates that the strength of the relationship between income and the prevalence of OWOB grew over time while the previous studies found that this relationship did not exist [17], or was inconsistent across racial/ethnic groups [15, 16].
The finding that, in the US, children and adolescents in low-income families are at increased risk of becoming OWOB is consistent with a broader literature base showing children, adolescents, and adults in low-income families around the world are at elevated risk for a variety of negative health outcomes [9, 27,28,29]. Thus, understanding the mechanisms that are driving these disparities is critical. While the pathway to OWOB involves a complex web of social, environmental, and genetic determinates, several possible explanations that may illuminate strategies to address disparate rates of childhood OWOB have been identified. For instance, there is recent experimental evidence that low social status may increase calorie consumption [30]. This preliminary experimental evidence is supported by cross-sectional and longitudinal studies showing that OWOB status is associated with social status in minority children and adolescents [31, 32]. In addition to the psychobiological impact of low social status on low-income children and adolescents’ OWOB status, the “insurance hypothesis” suggests that food insecurity (i.e., access to adequate food is limited because of lack of money or other resources [33]) may actually trigger the body to store more fat [34]. Since children and adolescents from low-income households are more likely to be food insecure [33] their bodies may also be storing more fat, increasing their likelihood to be OWOB. However, empirical evidence of the relationship between food insecurity and OWOB is limited to adult women in high-income countries [34]. Further, a increased risk for low-income children and adolescents to be OWOB may be due to the environments in which they live. Studies have shown that low-income families are more likely to live in “obesogenic” environments [35]. Obesogenic environments are characterized by social and structural factors in one’s community that lead to higher rates of OWOB. Research has shown that low-income neighborhoods are less likely to have supermarkets [36], limiting access to healthy foods. A recent study also demonstrated that schools in low-income neighborhoods had more fast food restaurants and convenience stores close by than high-income neighborhoods [37]. Not surprisingly low socio-economic status has been related to reduced access to healthy foods like fruits and vegetables [38, 39]. There is also increasing evidence that features of physical environments influence levels of physical activity, and perceived neighborhood safety may be an important factor in low-income children and adolescents’ activity levels [40, 41]. Further, low-income neighborhoods are less likely to have parks and facilities in which children and adolescents can be physically active [42]. Thus, it appears that social context is a crucially important aspect that must be considered when attempting to address disparate rates of OWOB between low- and middle-to-high-income children and adolescents.
Several efforts to address childhood OWOB in low-income communities in the US have been undertaken [43,44,45,46,47,48,49]. However, these efforts have produced mixed and limited results [50,51,52,53]. This may be because these interventions are largely disconnected from the risk factors for overweight and obesity identified above (i.e., disparate access to healthy foods and infrastructure for physical activity, and failure to target the direct impacts of low social status on higher caloric intake). Instead these interventions primarily rely upon individual behavior change and health education strategies like intensive behavioral counseling [50, 51, 53, 54], health education and goal setting classes [53, 55, 56], placing health promoting brochures and posters in physicians’ offices [50, 55], and providing families with small plates to “nudge” them to eat smaller portion sizes [56]. New approaches that identify and target the underlying causes of childhood obesity for children and adolescents in low-income households are needed.
Results from this study indicate that US children and adolescents who are Hispanic, regardless of income level, are more likely to be OWOB. Despite this finding, high-income Hispanic children and adolescents were at a reduced risk for being OWOB compared to their low- and middle-income counterparts. Further, this study indicates that Black children and adolescents from middle and high-income households were more likely to be OWOB when compared to Black children and adolescents living in poverty. This finding is consistent with previous studies [13, 15]. There are several reasons why this may be the case. First, BMI is a relatively poor indicator of non-Hispanic Black children and adolescents’ adiposity when compared to children from other racial/ethnic backgrounds [16, 57,58,59,60]. Studies have suggested that BMI misclassifies between 30% and 60% of non-Hispanic Black children as OWOB [57]. This misclassification may be due to higher lean mass rather than increased fat mass in non-Hispanic Black children. Thus, further studies examining the relationship between income and non-Hispanic Black children and adolescents’ body composition with alternative measures such as dual-energy X-ray absorptiometry and bioelectrical impedance are warranted. Second, other studies have postulated that individuals who are non-Hispanic Black may not move to higher income, and consequently less obesogenic, neighborhoods because they may not feel welcome in those neighborhoods due to racial segregation [61, 62]. Finally, other studies have noted that racism and discrimination against individuals who are non-Hispanic Black persist, even when income is elevated, and chronic stress induced by persistent racism and discrimination offsets the health benefits of elevated socio-economic status due to increased income [63, 64]. Work to identify the reason children and adolescents who are middle- and high-income Black are more likely to be OWOB than their low-income counterparts is needed.
The finding that disparities in OWOB prevalence between the lowest and highest income groups are growing over time appears to be tracking larger trends of income disparities in the US, which have grown dramatically since the late 1970s [65]. Thus, it appears that growing income disparities are reflected in growing health disparities. Policies to close the gap between the lowest and highest income families may also mitigate growing health disparities between children and adolescents from low- and high-income families.
The study’s cross-sectional nature is both a strength and a limitation. It provides powerful and generalizable information for prediction of current obesity rates and for targeting obesity efforts in the US. However, it cannot shed light on causation or mechanisms. This would require a longitudinal design to establish temporal precedence and the inclusion of additional environmental, behavioral, and biological measures. However, other studies have identified longitudinal trends in children and adolescents’ OWOB status and the relationship to income from birth to preschool and from childhood to adulthood [13, 66]. This study is also limited by the use of a single indicator of social disparity (i.e., family income). There are a variety of measures of social status including net worth, educational attainment, parental occupation, family disadvantage, neighborhood disadvantage, etc. All indicators have advantages and disadvantages. For instance, the place (i.e., neighborhood) that one lives may be more important than other indicators of social status. Future work should consider all indicators of social status when exploring and attempting to address disparate rates of OWOB in children and adolescents. Also, while this study included nearly 74,000 children and adolescents, relatively few of the participants were from high-income households and were Black (10.9%) or Hispanic (12.5%). Future studies seeking to explore the relationship between race/ethnicity, income, and OWOB should consider oversampling minority children and adolescents from high-income households.
It appears that US children and adolescents living in poverty are at increased risk of being OWOB. However, racial ethnic differences in the prevalence of OWOB become more pronounced in middle- and high-income households. Finally, these disparities in the prevalence of OWOB between low- and middle/high-income households appear to be growing over time in the US.
References
Ogden CL, Carroll MD, Lawman HG, Fryar CD, Kruszon-Moran D, Kit BK, et al. Trends in obesity prevalence among children and adolescents in the United States, 1988-1994 through 2013-2014. JAMA. 2016;315:2292–9.
Cote AT, Harris KC, Panagiotopoulos C, Sandor GG, Devlin AM. Childhood obesity and cardiovascular dysfunction. J Am Coll Cardiol. 2013;62:1309–19.
Bacha F, Gidding SS. Cardiac abnormalities in youth with obesity and type 2 diabetes. Curr Diab Rep. 2016;16:1–9.
Mohanan S, Tapp H, McWilliams A, Dulin M. Obesity and asthma: pathophysiology and implications for diagnosis and management in primary care. Exp Biol Med. 2014;239:1531–40.
Narang I, Mathew JL. Childhood obesity and obstructive sleep apnea. J Nutr Metab 2012; 2012:1–8.
Pollock NK. Childhood obesity, bone development, and cardiometabolic risk factors. Mol Cell Endocrinol. 2015;410:52–63.
Bammann K, Gwozdz W, Pischke C, Eiben G, Fernandez-Alvira JM, De Henauw S, et al. The impact of familial, behavioural and psychosocial factors on the SES gradient for childhood overweight in Europe. A longitudinal study. Int J Obes. 2017;41:54.
Shrewsbury V, Wardle J. Socioeconomic status and adiposity in childhood: a systematic review of cross‐sectional studies 1990–2005. Obesity. 2008;16:275–84.
Barriuso L, Miqueleiz E, Albaladejo R, Villanueva R, Santos JM, Regidor E. Socioeconomic position and childhood-adolescent weight status in rich countries: a systematic review, 1990–2013. BMC Pediatr. 2015;15:129.
Miech RA, Kumanyika SK, Stettler N, Link BG, Phelan JC, Chang VW. Trends in the association of poverty with overweight among US adolescents, 1971-2004. JAMA. 2006;295:2385–93.
Bonney A, Mayne DJ, Jones BD, Bott L, Andersen SE, Caputi P, et al. Area-level socioeconomic gradients in overweight and obesity in a community-derived cohort of health service users—a cross-sectional study. PLoS ONE. 2015;10:e0137261.
Chang VW, Lauderdale DS. Income disparities in body mass index and obesity in the United States, 1971-2002. Arch Intern Med. 2005;165:2122–8.
Jones-Smith JC, Dieckmann MG, Gottlieb L, Chow J, Fernald LCH. Socioeconomic status and trajectory of overweight from birth to mid-childhood: the early childhood longitudinal study-birth cohort. PLoS ONE. 2014;9:e100181.
Sobal J, Stunkard AJ. Socioeconomic status and obesity: a review of the literature. Psychol Bull. 1989;105:260.
Freedman DS, Ogden CL, Flegal KM, Kettel Khan L, Serdula MK, Dietz WH. Childhood overweight and family income. MedGenMed. 2007;9:26–26.
Freedman DS, Wang J, Thornton JC, Mei Z, Pierson RN, Dietz WH, et al. Racial/ethnic differences in body fatness among children and adolescents. Obesity. 2008;16:1105–11.
Wang Y, Zhang Q. Are American children and adolescents of low socioeconomic status at increased risk of obesity? Changes in the association between overweight and family income between 1971 and 2002. Am J Clin Nutr. 2006;84:707–16.
Ogden CL, Carroll MD, McDowell MA, Flegal KM. Obesity among adults in the United States—no statistically significant change since 2003-2004. NCHS Data Breif, 2007. p. 1–8.
Ogden CL. Prevalence of obesity among youths by household income and education level of head of household—United States 2011–2014. MMWR Morbid Mortality Weekly Rep. 2018;67:186–89.
National Center for Education Statistics. Early Childhood Longitudinal Program (ECLS). 2017 [cited 3 Jan 2018]. https://nces.ed.gov/ecls/.
Bureau of Labor Statistics. National Longitudinal Surveys. 2017 [cited 3 Jan 2018]. https://www.bls.gov/nls/.
Centers for Disease Control and Prevention (CDC) and National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey Questionnaire. 2014 [cited 2 Oct 2014]. http://www.cdc.gov/nchs/nhanes.htm.
Department of Health and Human Services. Department of Health and Human Services Poverty Guidelines for 2017. 2017 [cited 10 Nov 2017]. https://aspe.hhs.gov/poverty-guidelines.
Kuczmarski R, Ogden C, Guo S, Grummer-Strawn L, Flegal K, Mei Z, et al. CDC growth charts for the US: methods and development. Vital Health Stat. 2002;11:1–190.
Anderson SE, Whitaker RC. Prevalence of obesity among us preschool children in different racial and ethnic groups. Arch Pediatr Adolesc Med. 2009;163:344–8.
Sutton, AJ, KR Abrams, DR Jones, DR Jones, TA Sheldon, F Song. Methods for meta-analysis in medical research. (Wiley, Hoboken, NJ 2000).
Braveman PA, Cubbin C, Egerter S, Williams DR, Pamuk E. Socioeconomic disparities in health in the United States: what the patterns tell us. Am J Public Health. 2010;100(S1):S186–S196.
Cameron AJ, Spence AC, Laws R, Hesketh KD, Lioret S, Campbell KJ. A review of the relationship between socioeconomic position and the early-life predictors of obesity. Curr Obes Rep. 2015;4:350–62.
Adler NE, Boyce T, Chesney MA, Cohen S, Folkman S, Kahn RL, et al. Socioeconomic status and health: the challenge of the gradient. Am Psychol. 1994;49:15.
Cardel M, Johnson S, Beck J, Dhurandhar E, Keita A, Tomczik A, et al. The effects of experimentally manipulated social status on acute eating behavior: a randomized, crossover pilot study. Physiol Behav. 2016;162:93–101.
Goodman E, Maxwell S, Malspeis S, Adler N. Developmental trajectories of subjective social status. Pediatrics 2015:136:1–10.
Goodman E, Adler NE, Kawachi I, Frazier AL, Huang B, Colditz GA. Adolescents 9 perceptions of social status: development and evaluation of a new indicator. Pediatrics. 2001;108:e31.
Coleman-Jensen A, Gregory C, Singh A. Household food security in the United States in 2013. 2014.
Nettle D, Andrews C, Bateson M. Food insecurity as a driver of obesity in humans: the insurance hypothesis. Behav Brain Sci. 2017;40:1–53.
Swinburn B, Egger G, Raza F. Dissecting obesogenic environments: the development and application of a framework for identifying and prioritizing environmental interventions for obesity. Prev Med. 1999;29:563–70.
Morland K, Wing S, Roux AD, Poole C. Neighborhood characteristics associated with the location of food stores and food service places. Am J Prev Med. 2002;22:23–29.
Walker RE, Block J, Kawachi I. The spatial accessibility of fast food estaurants and convenience stores in relation to neighborhood schools. Appl Spat Anal Policy. 2014;7:169–82.
Janssen I, Boyce WF, Simpson K, Pickett W. Influence of individual-and area-level measures of socioeconomic status on obesity, unhealthy eating, and physical inactivity in Canadian adolescents. Am J Clin Nutr. 2006;83:139–45.
Drewnowski A. Obesity and the food environment: dietary energy density and diet costs. Am J Prev Med. 2004;27:154–62.
Sallis JF, Nader PR, Broyles SL, Berry CC, Elder JP, McKenzie TL, et al. Correlates of physical activity at home in Mexican-American and Anglo-American preschool children. Health Psychol. 1993;12:390.
Sallis JF, Johnson MF, Calfas KJ, Caparosa S, Nichols JF. Assessing perceived physical environmental variables that may influence physical activity. Res Q Exerc Sport. 1997;68:345–51.
Powell LM, Slater S, Chaloupka FJ, Harper D. Availability of physical activity–related facilities and neighborhood demographic and socioeconomic characteristics: a national study. Am J Public Health. 2006;96:1676–80.
Pratt CA, Boyington J, Esposito L, Pemberton VL, Bonds D, Kelley M, et al. Childhood Obesity Prevention and Treatment Research (COPTR): interventions addressing multiple influences in childhood and adolescent obesity. Contemp Clin Trials. 2013;36:406–13.
Dooyema CA, Belay B, Foltz JL, Williams N, Blanck HM. The childhood obesity research demonstration project: a comprehensive community approach to reduce childhood obesity. Child Obes. 2013;9:454–9.
Baranowski T, Baranowski JC, Cullen KW, Thompson DI, Nicklas T, Zakeri IF, et al. The fun, food, and fitness project (FFFP): The Baylor GEMS pilot study. Ethn Dis. 2003;13(Supp/1):S1–30.
Klesges RC, Obarzanek E, Kumanyika S, Murray DM, Klesges LM, Relyea GE, et al. The Memphis Girls’ Health Enrichment Multi-site Studies (GEMS): an evaluation of the efficacy of a 2-year obesity prevention program in African American girls. Arch Pediatr Adolesc Med. 2010;164:1007–14.
Robinson TN, Matheson DM, Kraemer HC, Wilson DM, Obarzanek E, Thompson NS et al. A randomized controlled trial of culturally tailored dance and reducing screen time to prevent weight gain in low-income African American girls: Stanford GEMS. Arch Pediatr Adolesc Med 2010;164:995–1004.
Luepker RV, Perry CL, McKinlay SM, Nader PR, Parcel GS, Stone EJ, et al. Outcomes of a field trial to improve children’s dietary patterns and physical activity. JAMA. 1996;275:768–76a
Economos CD, Hyatt RR, Must A, Goldberg JP, Kuder J, Naumova EN, et al. Shape Up Somerville two-year results: a community-based environmental change intervention sustains weight reduction in children. Prev Med. 2013;57:322–7.
Taveras EM, Perkins M, Anand S, Woo Baidal JA, Nelson CC, Kamdar N, et al. Clinical effectiveness of the massachusetts childhood obesity research demonstration initiative among low‐income children. Obesity. 2017;25:1159–66.
Butte NF, Hoelscher DM, Barlow SE, Pont S, Durand C, Vandewater EA, et al. Efficacy of a community‐versus primary care–centered program for childhood obesity: TX CORD RCT. Obesity. 2017;25:1584–93.
Anchondo IM, Satter E, Danaher C, Estes PR. MA-CORD: Stop ineffective childhood obesity inverventions. Child Obes. 2015;11:731–2.
Barkin SL, Heerman WJ, Sommer EC, Martin NC, Buchowski MS, Schlundt D, et al. Effect of a behavioral intervention for underserved preschool-age children on change in body mass index: a randomized clinical trial. JAMA. 2018;320:450–60.
Moore SM, Borawski EA, Cuttler L, Ievers-Landis CE, Love TE. IMPACT: a multi-level family and school intervention targeting obesity in urban youth. Contemp Clin Trials. 2013;36:574–86.
Sherwood NE, French SA, Veblen-Mortenson S, Crain AL, Berge J, Kunin-Batson A, et al. NET-Works: linking families, communities and primary care to prevent obesity in preschool-age children. Contemp Clin Trials. 2013;36:544–54.
Robinson TN, Matheson D, Desai M, Wilson DM, Weintraub DL, Haskell WL, et al. Family, community and clinic collaboration to treat overweight and obese children: Stanford GOALS—a randomized controlled trial of a three-year, multi-component, multi-level, multi-setting intervention. Contemp Clin Trials. 2013;36:421–35.
Flegal KM, Ogden CL, Yanovski JA, Freedman DS, Shepherd JA, Graubard BI, et al. High adiposity and high body mass index–for-age in US children and adolescents overall and by race-ethnic group. Am J Clin Nutr. 2010;91:1020–6.
Nelson DA, Barondess DA. Whole body bone, fat and lean mass in children: comparison of three ethnic groups. Am J Phys Anthropol. 1997;103:157–62.
Ellis KJ, Abrams SA, Wong WW. Monitoring childhood obesity: assessment of the weight/height2 index. Am J Epidemiol. 1999;150:939–46.
Daniels SR, Khoury PR, Morrison JA. The utility of body mass index as a measure of body fatness in children and adolescents: differences by race and gender. Pediatrics. 1997;99:804–7.
Chang VW. Racial residential segregation and weight status among US adults. Soc Sci Med. 2006;63:1289–303.
LaVeist T, Pollack K, Thorpe R Jr, Fesahazion R, Gaskin D. Place, not race: disparities dissipate in southwest Baltimore when blacks and whites live under similar conditions. Health Aff. 2011;30:1880–7.
Hajat A, Kaufman JS, Rose KM, Siddiqi A, Thomas JC. Long-term effects of wealth on mortality and self-rated health status. Am J Epidemiol. 2010;173:192–200.
Williams DR. Race, socioeconomic status, and health the added effects of racism and discrimination. Ann N Y Acad Sci. 1999;896:173–88.
Saez E, Zucman G. Wealth inequality in the United States since 1913: Evidence from capitalized income tax data. Q J Econ. 2016;131:519–78.
Hernandez DC, Pressler E. Accumulation of childhood poverty on young adult overweight or obese status: race/ethnicity and gender disparities. J Epidemiol Community Health 2014;68:478–84.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

{kind=link}
Cite this article
Weaver, R.G., Brazendale, K., Hunt, E. et al. Disparities in childhood overweight and obesity by income in the United States: an epidemiological examination using three nationally representative datasets. Int J Obes 43, 1210–1222 (2019). https://doi.org/10.1038/s41366-019-0331-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-019-0331-2
- Springer Nature Limited
This article is cited by
-
Ethnicity/race, parent educational attainment, and obesity associated with prediabetes in children
Nutrition & Diabetes (2023)
-
Translating the Recommended Multicomponent Intervention for Childhood Overweight and Obesity into Practice: Implementation Challenges
Journal of Contemporary Psychotherapy (2023)