
Abstract
Background
While recent evidence suggests that the overall prevalence of overweight in young children in Bangladesh is low, little is known about variation in trends by sex, socioeconomic status, urbanicity, and region. We investigated the trends in overweight among children aged 24–59 months by these factors, using nationally representative samples from Bangladesh Demographic and Health Surveys (BDHS) between 2004 and 2014.
Methods
Data from four BDHS surveys conducted between 2004 and 2014, with valid height and weight measurements of children, were included in this study (n = 15,648). BMI was calculated and the prevalence of overweight (including obesity) was reported using the International Obesity Taskforce (IOTF) classification system. To explore the association between socioeconomic status and childhood overweight, we used multivariable logistic regression.
Results
The overall prevalence of overweight among children aged 24–59 months increased from 1.60% (95% CI: 1.20–2.05%) in 2004 to 2.33% (95% CI: 1.82–2.76%) in 2014. Among girls, the overweight trend increased significantly (adjusted odds ratio (OR) comparing 2014 vs. 2004: 2.02 95% CI: 1.52–2.68), whereas among boys the trend remained steady. When compared with households with the poorest wealth index, households with richest wealth index had higher odds of childhood overweight among both boys (OR 2.39, 95% CI: 1.76–3.25) and girls (OR 1.86, 95% CI: 1.35–2.55). Higher household education level was also associated with childhood overweight. Subgroup analyses showed that relative inequalities by these factors increased between 2004 and 2014 when adjusted for potential confounders.
Conclusions
There is a rising trend in overweight prevalence exclusively among girls aged 24–59 months in Bangladesh. Childhood overweight is associated with higher household education and wealth index, and the relative disparity by these factors appears to be increasing over time. These unmet inequalities should be considered while developing national public health programs and strategies.
Similar content being viewed by others

Introduction
The burden of overweight and obesity among children has risen significantly in recent decades and is now considered one of the biggest global health problems of the 21st century, owing to established links with various adulthood morbidities and premature mortality [1,2,3]. Recent global estimates suggest that nearly one in every five children in high-income countries is overweight [4]. Although the prevalence of childhood obesity and overweight in low- and middle-income countries (LMICs) appears quantitatively lower when compared with that of high-income countries, the determinants and burden of childhood obesity and overweight in these non-Western settings may vary importantly by population contexts like demographic and socioeconomic characteristics [5, 6].
According to a recent landmark global study, published by the Global Burden of Disease obesity collaborators, in 2015, Bangladesh (a dense and populous LMIC in South Asia) had the lowest overall prevalence of childhood obesity (1.2%) and 6th lowest overall prevalence for adult obesity (male 2.3%, female 3.7%) of the 195 countries studied [1]. Despite the lowest overall prevalence estimates, between 1990 and 2015, the greatest percent increases in age-standardized body mass index-related deaths and disability-adjusted life-years globally were also recorded in Bangladesh, with relative increases of 133.6% and 139.4%, respectively [1].
This discrepancy deserves warrants further study, to disentangle national obesity and overweight estimates by key drivers of inequality such as age group, sex, socioeconomic status, urbanicity, and changes over time. To date, however, studies on childhood overweight and obesity in Bangladesh have been limited by: insufficient power or detail (e.g., absence of data separately on urban and rural settings or time trends), use of suboptimal data sources (e.g., surveys based on non-representative population subsets), and methodological constraints (e.g., not employing well-established thresholds to define childhood overweight and obesity which precludes cross-comparison of estimates) [7,8,9,10,11].
To characterize childhood overweight and obesity in greater detail and address scientific uncertainties, we have conducted a large, comprehensive study, using nationally-representative data collected between 2004 and 2014 from >15,000 randomly-chosen children, including information on a wide range of demographic and socioeconomic factors. The key objectives of this study were: (i) to estimate prevalence of overweight and obesity in Bangladeshi children by factors like age at survey, sex, socioeconomic status, urbanicity, and region; (ii) to describe the relative disparities in childhood overweight and obesity burden by these factors over time; and (iii) to quantify the associations of these characteristics with childhood overweight and obesity.
Methods
Data sources and study design
This is a cross-sectional study based on Bangladesh Demographic and Health Surveys (BDHS).
BDHS surveys are nationally-representative surveys conducted every 3–5 years by the National Institute for Population Research and Training (NIPORT) of the Ministry of Health and Family Welfare, Government of Bangladesh with technical assistance from the ICF International, located in Calverton, Maryland, USA [12]. General details of the survey methodology have been published elsewhere [13,14,15,16]. Briefly, these surveys are based on two-staged stratified sampling of households nationwide. In the first stage, census enumeration areas are selected using probability proportional to size (PPS) sampling technique through statistics provided by the Bangladesh Bureau of Statistics (BBS). In the second stage, households are selected through systematic random sampling from the complete listing of households within a selected enumeration area.
Ethical approval for BDHS surveys has been received from the ICF International Institutional Review Board. Informed consent was provided by the mothers of children from whom data were collected before commencement of the survey. Additional consent was provided before the taking of anthropometric measurements. All data were de-identified at the cluster level and anonymized for protection of privacy, anonymity, and confidentiality. The data files are freely available from the MEASURE Demographic and Health Surveys (DHS) website (www.dhsprogram.com). We received authorization from the DHS program for using the relevant datasets for this analysis.
The current study is based on four consecutive BDHS surveys, using standardized protocol and instruments, conducted between 2004 and 2014. The response rates for these surveys were high (between 97 and 98.6%). The detailed methods and questionnaire of these Bangladeshi surveys are available in the final reports of BDHS [13,14,15,16]. We used children's record (coded as “KR” in DHS program) datasets which contained information about children born in the last 5 years prior to the survey (aged 0–59 months). The present analysis is based on children aged 24–59 months who had valid measurement of their weight and height. We excluded children aged less than 24 months because there is no available classification system for defining overweight at this age. A flowchart of sample selection from each BDHS survey for the present analysis is shown in Supplementary Figure S1.
Anthropometric measurement and defining childhood overweight
In the included BDHS surveys, height and weight of the children were measured by trained personnel using standardized instruments and procedures. Lightweight SECA scales (Hamburg, Germany) with digital screen, designed and manufactured by the United Nations Children’s Fund (UNICEF), were used to measure weight. The height/length was measured by boards, produced by Shorr Productions (Maryland, USA). In children with height less than 85 centimeters, recumbent length was measured, whereas standing height was measured for those taller than this. Body mass index (BMI) was calculated by dividing body weight (kg) by squared height (m2) [13,14,15,16].
We used the age and sex-specific BMI cut-offs from the International Obesity Task Force (IOTF) [10, 11] for defining childhood overweight. In IOTF classification, a child aged 2–18 years is classified as overweight if their BMI is larger than the age and sex-specific BMI cut-off corresponding to an adult BMI of >25 kg/m2 [10, 11].
Demographic and socioeconomic characteristics
BDHS surveys collected information about the characteristics of selected households and their respondents using face-to-face interview administered standardized questionnaires, conducted by trained personnel. Child’s place of residence was dichotomized into urban and rural based on country-specific definitions. BBS constructed a country-specific wealth index using principal components analysis from data on household assets including durable goods (i.e., bicycles, televisions, etc.) and dwelling characteristics (i.e., sanitation, source of drinking water and construction material of house, etc.) [13,14,15,16]. This is then categorized into five groups (i.e., poorest, poorer, middle, richer, and richest) based on the quintile distribution of the sample. Household’s highest education level was categorized as no education, primary, secondary and higher categories.
Statistical analysis
The distributions of sociodemographic characteristics of included children are described as proportions for categorical variables and as mean ± standard deviation (SD) for continuous variables, for each BDHS survey.
Following the instructions in the DHS guide on analysis of their datasets [17], we used sampling weights to calculate the prevalence of overweight to ensure that the estimates are representative of the Bangladeshi population. We calculated the overall prevalence of overweight and obesity (referred to hereafter as “overweight”) among children aged 24–59 months and 95% confidence intervals (CIs) for these were calculated using a logit transform of the estimate. All overweight prevalence estimates in our analysis included children with obesity as well. We calculated overweight prevalence in subgroups of children by sex, age, urbanicity, division, and socioeconomic status to examine trends of childhood overweight by these factors.
To assess the relative disparities in childhood overweight over time by these factors, we used multivariable logistic regressions with survey year as the explanatory variable and other factors (age of the child, area of residence, and division), when appropriate, as adjustment variables. This approach estimated the odds ratios (ORs) of childhood overweight over time with reference to a baseline year (e.g., 2004) in subgroups of children by socio-demographic factors studied.
We studied associations of socioeconomic status (i.e., household wealth index and highest education level) with childhood overweight in the total sample from four surveys. Then, to see whether these associations vary from survey to survey, we did the analyses separately for each survey. We employed a forward stepwise approach to build multivariable logistic regression models and conducted likelihood ratio tests, examining Chi-square statistics, to ascertain whether adding a variable improved the model fit.
When more than two categories were compared, group-specific confidence intervals (gs-CIs) were estimated using the variance of the log risk for each group. This allows comparisons to be made between two exposure groups, even if neither is the reference group [18]. Conventional CIs are provided in case of two categories being compared. All analyses were performed using Stata v14.2 (StataCorp, College Station, TX, USA).
Results
General characteristics of the study participants
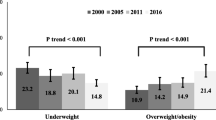
A total of 15 648 children aged 24–59 months from four BDHS surveys conducted between 2004 and 2014 were included in this study. The general characteristics of the study participants in these surveys have been summarized in Table 1. Briefly, the age and sex distributions of the children sampled in each survey were largely similar. Two-thirds or more of the sampled children were from rural areas, with higher proportions of children included from Dhaka and Chittagong divisions, compared to the other five divisions. The percentage of households with no education reduced from 39 to 17%, while the percentage of households with higher education almost doubled (from 5.3 to 9.8%) between 2004 and 2014 (Table 1).
Prevalence of childhood overweight over time, by factors studied
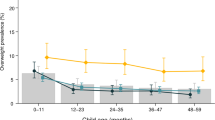
Figure 1 showed the prevalence of thinness, normal weight, overweight and obesity among children aged 24–59 months in Bangladesh between 2004 and 2014. The prevalence of overweight increased from 1.1% in 2004 to 1.7% in 2014 and less than 1% children had obesity in these years. The prevalence of overweight and obesity among children increased from 1.6% (95% CI: 1.2–2.1%) in 2004 to 2.3% (95% CI: 1.8–2.8%) in 2014. Among girls, the overweight prevalence increased almost two-folds during this period (1.4–2.8%) whereas the prevalence among boys remained steady (Fig. 1).

Sampling weight provided by the Demographic and Health Survey (DHS) [12] was used to estimate country-representative prevalence. 95% confidence intervals (CIs) for prevalence estimates were calculated using a logit transform of the estimate.
We estimated overweight prevalence in subgroups of boys and girls, by age, area of residence, division, household’s highest education, and wealth index in each survey (Fig. 2). For boys, a higher prevalence of overweight was found in urban areas than rural areas in all surveys. This urban-rural difference was not replicated among girls, except for the most recent survey in 2014. We observed no specific pattern in overweight prevalence among boys and girls according to division. Both boys and girls in households with higher educational qualification or in the richest wealth index had higher prevalence of overweight when compared with households with lower education level or poorer wealth index. There were also increasing trends of overweight among boys and girls in households with higher education or richest wealth index from 2004 to 2014 (Fig. 2).

Sampling weights provided by the Demographic and Health Survey (DHS) [12] was used to estimate the country-representative prevalence.
Relative disparities in childhood overweight over time
To explore the relative disparities in childhood overweight burden over time in subgroups of boys and girls by various factors, we calculated ORs for overweight by survey year with reference to the 2004 survey (Table 2). The overall trend of overweight among boys was not significant (OR comparing 2014 vs. 2004: 0.98, 95% CI: 0.72–1.32) whereas girls had a significant increase in the trend of overweight (OR comparing 2014 vs. 2004: 2.02, 95% CI: 1.52–2.68). In subgroup analysis among boys by the levels of area, education and wealth index, the trend of overweight was not significant except for households with higher education level (OR comparing 2014 vs. 2004: 1.84, 95% CI: 1.12–3.04) (Table 2). Among girls, the prevalence of overweight in urban area increased 3.60 times between 2004 and 2014 (OR 3.60, 95% CI: 2.42–5.36). There was significant increase in overweight prevalence over the study period among girls from households in the richer or richest wealth index and those in secondary or higher education (Table 2).
Association of socioeconomic status with childhood overweight
In the combined analysis of all survey data, we found that households in the richest wealth quintile had higher odds ratio of having childhood overweight among both boys (OR 2.39; 95% CI: 1.76–3.25) and girls (OR 1.86; 95% CI: 1.35–2.55). Households with a higher education level also had increased odds of childhood overweight (Boys OR 4.33, 95% CI: 3.12–6.01; Girls OR 2.14, 95% CI: 1.38–3.31), compared with households with no education (Fig. 3). Supplementary Tables S2 and S3 show the effects of adjustment by various factors on the associations of household’s highest education level and wealth index with childhood overweight. As confirmatory data, we looked at the associations of socioeconomic status and obesity only, and found similar results (Supplementary Table S4). When we studied the association of household’s socioeconomic status with childhood overweight separately for each survey year, we observed that the relative difference in overweight burden between households with higher and lower socioeconomic status widened over the survey years. Among boys, the OR for richest vs. poorest household wealth index were 1.28 (95% CI 0.59–2.76) and 3.48 (95% CI 2.01–6.05) in 2004 and 2014, respectively. Among girls, there was no appreciable change for ORs comparing richest vs. poorest between 2004 and 2014 because the corresponding 95% CIs overlapped (Table 3). For ORs comparing households with higher education vs. no education, there was an increase between 2004 and 2014 among both boys and girls, reflecting that the socioeconomic disparity for childhood overweight has increased over time.

Odds ratio with 95% floating confidence interval were calculated from logistic regression and models were adjusted for child’s age, area of residence, division, and survey year. 95% FCIs were estimated for an explanatory variable with more than two categories to allow comparisons between any two categories, even if neither is the reference group [18].
Discussion
The present study highlights that in Bangladesh while overall prevalence estimates for overweight among community-dwelling children aged 24–59 months appear low, there was an increasing trend in estimates between 2004 and 2014 exclusively among girls. There was also a substantial increase in the overweight burden amongst urban populations and in households with higher socioeconomic status among both boys and girls. Additionally, childhood overweight in Bangladesh was associated significantly with higher household education and wealth index, and the relative disparity by these factors continued to increase over time.
In our study, the prevalence of overweight among children aged under-five years was generally found to be low in each survey. The low prevalence rates were in line with earlier studies conducted at similar time points [1, 19, 20]. However, earlier studies had relatively smaller samples based on various specific populations which did not allow them to estimate a nationally-representative estimate for childhood overweight. We were able to reliably estimate the country-representative prevalence of childhood overweight in our study, which is also based on internationally-comparable cut-offs. Despite the relatively low prevalence of overweight and static trend, this translates to a large number of individuals with overweight and obesity due to the large population in this age group within Bangladesh and other South Asian countries [21]. This is likely to result in a double burden of childhood malnutrition in these countries due to the already high prevalence of childhood stunting and underweight within them [22, 23].
There was large variability in rates of overweight in subgroups of children by age, sex, urbanicity, regions, and socioeconomic status. We also observed increasing trends in overweight prevalence amongst urban populations and in households with higher socioeconomic status for both boys and girls. These findings show that reporting only national prevalence may hide variations in overweight burden by these factors and public health approaches should consider these variations, especially as countries continue to develop economically and environmentally.
The observed urban-rural gap in the childhood overweight-obesity prevalence in our study is similar to previous findings in the LMIC context [4, 7, 8, 19, 21, 23,24,25]. Das et al. reported an increasing trend in overweight and obesity in urban population in Bangladesh, both for children under 5 years (from 0.64% in 1993 to 5.15% in 2011) and children aged 5–19 years (from 0.80% in 1993 to 6.70% in 2011) [8]. Additionally, an urban-rural comparison of overweight trend in the last two decades in Bangladesh showed a higher net increase in overweight prevalence in urban children than in rural children (net increases of 2.0% and 1.4%, respectively) [7]. Rapid urbanization in LMICs is playing a major role in the increase of overweight-obesity prevalence both among children and adults [4, 21]. For example, in Bangladesh, rapid and unplanned urbanization reduced the number of playgrounds which may have led to more sedentary lifestyles and less physical activity amongst children [8]. A recent case-control study in Bangladesh reported that having an overweight parent and sedentary activities for more than four hours a day (including watching television and playing games on the computer) were associated with overweight-obesity in urban school children [26]. In addition, the higher availability of fast-food chains serving high calorie and processed foods in urban locations contributes significantly to the growing burden of childhood obesity [27].
Contrary to the usual inverse relationship between socio-economic gradient and childhood overweight observed in developed countries [28,29,30], we found higher socioeconomic status was positively associated with higher overweight prevalence. Moreover, the socioeconomic disparity in childhood overweight prevalence increased between 2004 and 2014. It is hypothesized that socioeconomic groups which have the easier access to energy-dense diets suffers more from overweight and obesity. In developed countries, children from less affluent households usually have more access to fast-foods and suffer from overweight and obesity disproportionately in comparison to their counterparts [28]. A recent study on Bangladeshi urban populations found that compared to households with low socioeconomic status, children from households with higher socioeconomic status had two-fold risk [OR 1.99; 95% CI: 1.02, 3.82] of being overweight [8]. A recent systematic review on childhood overweight and obesity in India also suggested that overweight and obesity rates in children are increasing in higher socio-economic groups [31]. Factors like increased purchasing power parity (PPP), changing social norms i.e. preferring to dine out or eat processed food to home cooking and a lack of an environment promoting physical activity, are thought to be contributing to the overweight and obesity burden in the urban affluent society.
There has been a considerable decline in the trend of underweight children under the age of 5 years in Bangladesh over the last two decades [7]. Reports from the DHS surveys showed that the prevalence of underweight children in this age group was 48% in 1999 and 33% in 2014 [13,14,15,16, 32]. Economic growth, higher maternal literacy, improved feeding practices for infants and young children and better immunization coverage contributed to this [4, 7, 22]. However, there has been simultaneous urbanization and industrialization, an adoption of Westernized lifestyles and a lack of physical activity, resulting in an increased prevalence of overweight and obesity, particularly amongst children in the higher socio-economic classes [20]. Therefore, we often see a contrasting scenario—undernutrition in the poorer section and over-nutrition in the richer section of the society, resulting in a double burden of malnutrition overall.
The strengths of our study include the use of nationally representative samples and objectively measured height and weight, obtained by trained health field researchers using calibrated equipment. We used the IOTF classification system to estimate the prevalence of overweight among children, which will make the observed estimates internationally comparable. However, the study lacks information regarding dietary and lifestyle factors, meaning we were unable to explain changes in the prevalence of overweight amongst the population. There were ~3000 children from all four surveys who did not have BMI information available. However, from BDHS reports, it is evident that children with and without BMI information did not vary in terms of sociodemographic characteristics. Childhood is a period of dynamic growth and development and composite indicator like BMI may capture only one aspect of childhood adiposity. We did not have other measures of adiposity and body size which could represent other aspects of childhood adiposity.
Our study provides evidence for inequalities in childhood overweight by factors like sex, region, urbanicity, and socioeconomic status. Public health interventions and policies must target children who are at risk of developing overweight. This is particularly important for countries in which the prevalence of both overweight and underweight is a problem and interventions that counter both must be developed and implemented. It is also crucial that surveillance data continues to be collected that allow trends to be monitored at a subnational level.
In summary, our study involving four nationally-representative samples found a rising trend in overweight and obesity prevalence exclusively among girls aged 24–59 months. There are also significant and specific increases of these outcomes among children who are based in urban setting or belonged to households with high socioeconomic level and the relative disparity by these factors appear to be increasing over time in Bangladesh. The present study, therefore, highlights that in resource-poor settings, where the aggregate burden of childhood overweight and obesity appear low, important unmet inequalities exist and these should be considered while developing national public health programs and strategies.
References
Afshin A, Forouzanfar MH, Reitsma MB, Sur P, Estep K, Lee A, et al. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377:13–27.
Park MH, Falconer C, Viner RM, Kinra S. The impact of childhood obesity on morbidity and mortality in adulthood: a systematic review. Obes Rev. 2012;13:985–1000.
Simmonds M, Burch J, Llewellyn A, Griffiths C, Yang H, Owen C et al. The use of measures of obesity in childhood for predicting obesity and the development of obesity-related diseases in adulthood: a systematic review and meta-analysis. Health Technol Assess (Rockv) 2015; https://doi.org/10.3310/hta19430.
Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766–81.
Rudolf MC, Sahota P, Barth JH, Walker J. Increasing prevalence of obesity in primary school children: cohort study. BMJ. 2001;322:1094–5.
Gupta N, Misra A, Goel K, Shah P. Childhood obesity in developing countries: epidemiology, determinants, and prevention. Endocr Rev. 2012;33:48–70.
Das SK, Chisti MJ, Malek MA, Das J, Salam MA, Ahmed T, et al. Changing childhood malnutrition in Bangladesh: trends over the last two decades in urban-rural differentials (1993–2012). Public Health Nutr. 2015;18:1718–27.
Das SK, Chisti MJ, Huq S, Malek MA, Vanderlee L, Salam MA, et al. Changing trend of overweight and obesity and their associated factors in an urban population of Bangladesh. Food Nutr Sci. 2013;4:678–89.
Jesmin A, Yamamoto SS, Malik AA, Haque MA. Prevalence and determinants of chronic malnutrition among preschool children: a cross-sectional study in Dhaka City, Bangladesh. J Health Popul Nutr. 2011;29:494–9.
Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320:1240–3.
Cole TJ, Lobstein T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes. 2012;7:284–94.
National Institute of Population Research and Training (NIPORT), Mitra and Associates, and ICF International. Bangladesh Demographic and Health Survey 2014. Dhaka, Bangladesh, and Rockville, Maryland, USA, 2016.
National Institute of Population Research and Training (NIPORT), Mitra and Associates and MI. Bangladesh Demographic and Health Survey 2007. Dhaka, Bangladesh and Calverton, Maryland, USA, 2009.
National Institute of Population Research and Training (NIPORT), Mitra and Associates and I, International. Bangladesh Demographic and Health Survey 2011. Dhaka, Bangladesh and Calverton, Maryland, USA, 2013.
National Institute of Population Research and Training (NIPORT), Mitra and Associates, and ICF International. Bangladesh Demographic and Health Survey 2014. Dhaka, Bangladesh, 2016.
National Institute of Population Research and Training (NIPORT), Mitra and Associates and II. Bangladesh Demographic and Health Survey 2004. Dhaka, Bangladesh and Calverton, Maryland, USA, 2005, http://measuredhs.com/pubs/pdf/FR165/FR-BD04[FR165].pdf.
DHS Program. Using datasets for analysis. https://dhsprogram.com/data/Using-Datasets-for-Analysis.cfm (accessed 14 Nov 2017).
Plummer M. Improved estimates of floating absolute risk. Stat Med. 2004;23:93–104.
Biswas T, Islam A, Pervin S. Overweight and obesity among children and adolescents in Bangladesh: a systematic review and meta-analysis. Public Health. 2017;142:94–101.
Rahman S, Islam MT, Alam DS. Obesity and overweight in Bangladeshi children and adolescents: a scoping review. BMC Public Health. 2014;14:70.
de Onis M, Blössner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr. 2010;92:1257–64.
Monteiro CA, Conde WL, Popkin BM. The burden of disease from undernutrition and overnutrition in countries undergoing rapid nutrition transition: a view from Brazil. Am J Public Health. 2004;94:433–4.
Hoque ME, Doi SAR, Mannan M, Long K, Niessen LW, Mamun AA. Prevalence of overweight and obesity among children and adolescents of the indian subcontinent: A meta-analysis. Nutr Rev. 2014;72:541–50.
Tchoubi S, Sobngwi-Tambekou J, Noubiap JJN, Asangbeh SL, Nkoum BA, Sobngwi E. Prevalence and risk factors of overweight and obesity among children aged 6–59 months in cameroon: a multistage, stratified cluster sampling nationwide survey. PLoS ONE 2015;10:e0143215.
de Onis M, Blössner M. Prevalence and trends of overweight among preschool children in developing countries. Am J Clin Nutr. 2000;72:1032–9.
Bhuiyan MU, Zaman S, Ahmed T. Risk factors associated with overweight and obesity among urban school children and adolescents in Bangladesh: a case-control study. BMC Pediatr. 2013;13:72.
Braithwaite I, Stewart AW, Hancox RJ, Beasley R, Murphy R, Mitchell EA. Fast-food consumption and body mass index in children and adolescents: an international cross-sectional study. BMJ Open. 2014;4:e005813.
Wang Y, Lim H, Program N. The global childhood obesity epidemic and the association between socio-economic status and childhood obesity. Int Rev Psychiatry. 2012;24:176–88.
Ogden CL, Lamb MM, Carroll MD, Flegal KM. Obesity and socioeconomic status in children and adolescents: United States, 2005–2008. NCHS Data Brief 2010;51:1–8.
Cecil JE, Watt P, Murrie ISL, Wrieden W, Wallis DJ, Hetherington MM, et al. Childhood obesity and socioeconomic status: a novel role for height growth limitation. Int J Obes (Lond). 2005;29:1199–203.
Ranjani H, Mehreen TS, Pradeepa R, Anjana RM, Garg R, Anand K, et al. Epidemiology of childhood overweight & obesity in India: a systematic review. Indian J Med Res. 2016;143:160–74.
National Institute of Population Research and Training (NIPORT), Mitra and Associates (MA) and OM (ORCM). Bangladesh Demographic and Health Survey 1999–2000. Dhaka, Bangladesh and Calverton, Maryland, USA, 2001.
Acknowledgements
The authors thank the participants of Bangladesh Demographic and Health Surveys used in this study. We would also like to thank the DHS Program to authorize us to use the data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Shawon, M.S.R., Hossain, F.B., Thomson, B. et al. Trends in the prevalence of overweight among Bangladeshi children aged 24–59 months (2004–2014) by sex and socioeconomic status. Int J Obes 44, 664–674 (2020). https://doi.org/10.1038/s41366-019-0507-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-019-0507-9
- Springer Nature Limited