
Abstract
The association between cadmium exposure and risk of lung cancer is still unclear. We quantitatively reviewed the observational studies that investigated the association between cadmium exposure and lung cancer risk in both general and occupational populations published through April 2015. The final data set is comprised of three cohort studies in the general population totaling 22,551 participants (354 events) with a mean follow-up of 15 years, five occupational cohort studies including 4205 individuals (180 events) with an average follow-up of 31 years, and three occupational case–control studies including 4740 cases and 6268 controls. Comparing the highest to the lowest category of cadmium exposure, the weighted relative risk and 95% confidence interval of lung cancer in the general population was 1.42 (95% CI (0.91, 2.23)); the weighted risk estimates (95% CIs) of lung cancer in three occupational cohort studies and three case–control studies were 0.68 (95% CI (0.33, 1.41)) and 1.61 (95% CI (0.94, 2.75)), respectively. No linear association was found. When comparing participants exposed to cadmium with non-exposed based on available data, the association became statistically significant. According to findings from this meta-analysis, the possibility that cadmium exposure may increase risk of lung cancer cannot be completely ruled out in either general or occupational population.
Similar content being viewed by others


Introduction
Lung cancer is the leading cause of cancer death in both genders worldwide.1 In the United States, more than 25% of all cancer deaths are attributed to lung cancer.2 Although tobacco smoking is the most important determinant of lung cancer, several other risk factors have been recognized or suspected to be involved in lung cancer etiology, including exposure to cadmium, arsenic, and radon.1 These factors may be in aggregate accounting for large numbers of lung cancer cases.3 As lung cancer is a multi-factorial disease, avoidance of one or more contributing factors may help reduce its incidence and mortality.
Cadmium is a widespread metal that has been confirmed as a highly toxic carcinogen.4 Cadmium can be released in the process of nonferrous metal mining and refining, manufacture and application of phosphate fertilizers, fossil fuel combustion, and waste incineration and disposal.5 The major routes of occupational exposure are inhalation of dust and fumes, and incidental ingestion of dust from contaminated hands, cigarettes, or foods.6 Thus, workers in a wide variety of occupations that involve cadmium use have high levels of cadmium exposure. In addition, the extensive usage of cadmium in industries may result in ubiquitous cadmium pollution in air, soil, and water; because of that, the major sources of cadmium exposure are diet and tobacco smoking in the general population.6
The International Agency for Research on Cancer (IARC) classified cadmium as a human carcinogen, especially a lung cancer carcinogen, mainly based on the results from the studies of American smelter workers.4 However, findings on the association between cadmium exposure and lung cancer risk from occupational studies are inconsistent,3, 7, 8, 9, 10, 11, 12, 13 though two systematic reviews14, 15 suggested that there was evidence of a potentially positive association. Little is known about the carcinogenicity of cadmium in the general population having low-to-moderate levels of exposure. One recent meta-analysis16 based on three environmentally exposed populations found a significantly positive association between cadmium exposure and risk of lung cancer. However, controversy still remains; other studies found the association being non-significant.17
Therefore, we conducted this study to quantitatively assess the overall association between cadmium exposure and risk of lung cancer in both general and occupational populations by accumulating evidence from the existing literature.
Methods
Study selection
The relevant observational studies published in English-language journals through April 2015, which investigated the association between cadmium exposure and risk of lung cancer, were identified by searching PubMed database using the expression ‘(‘cadmium’[MeSH Terms] OR ‘cadmium’[All Fields]) AND (‘lung neoplasms’[MeSH Terms] OR (‘lung’[All Fields] AND ‘neoplasms’[All Fields]) OR ‘lung neoplasms’[All Fields] OR (‘lung’[All Fields] AND ‘cancer’[All Fields]) OR ‘lung cancer’[All Fields])’. Additional information was retrieved by searching Google Scholar and the reference lists of relevant articles.
All relevant articles were independently reviewed by two co-authors (C.C. and P.X.). Disagreements were resolved by group discussion. The inclusion criteria are as follows: (a) cohort, case–control, or cross-sectional studies; and (b) reported hazard ratio (HR), relative risk (RR), or odds ratio (OR) with corresponding 95% confidence intervals (95% CIs) of lung cancer in relation to cadmium exposure, or such information could be derived from the published results. We also included unpublished de novo results provided by authors in one study.17
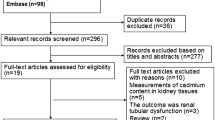
The detailed search process is shown in Figure 1. Of the 282 non-duplicated abstracts from PubMed and Google Scholar, 232 publications were excluded after reviewing titles and abstracts due to one of the following reasons: (a) laboratory studies (n=106); (b) non-original studies (reviews or letters-to-editors; n=81); (c) ecological studies, case reports, or methodological articles (n=18); or (d) not published in the English language (n=27). In addition, 39 articles were further excluded after reviewing full-texts because of the following reasons: (a) the exposure or outcome was not cadmium exposure or lung cancer (n=16); (b) the results have been updated in a later publication (n=10); or (c) the available data cannot be combined with other studies and requested de novo results were not obtained (n=13). In sum, 11 studies (three cohort studies in the general population, five cohort studies, and three case–control studies in occupational populations) met the criteria and were included in this meta-analysis (Figures 2, 3, 4).

Process of study selection.

Multivariable adjusted RR and 95% CI of lung cancer by cadmium exposure from three prospective cohort studies among general populations. The summary estimate was obtained using a random-effects model. The dots indicate the adjusted RRs by comparing the highest with the lowest level of cadmium exposure. The size of the shaded square is proportional to the percent weight of each study. The horizontal lines represent 95% CIs. The diamond data marker indicates the summary RR. CI, confidence interval; RR, relative risk.

Multivariable adjusted RR and 95% CI of lung cancer by cadmium exposure from five retrospective cohort studies among occupational populations. The summary estimates were obtained using a random-effects model. The dots indicate the adjusted RRs by one unit increment of exposure or comparing the highest with the lowest level of cadmium exposure. The size of the shaded square is proportional to the percent weight of each study. The horizontal lines represent 95% CIs. The diamond data markers indicate the summary RRs. CI, confidence interval; RR, relative risk.

Multivariable adjusted OR and 95% CI of lung cancer risk by cadmium exposure from three case–control studies. The summary estimate was obtained using a random-effects model. The dots indicate the adjusted ORs by comparing the highest with the lowest level of cadmium exposure or by comparing the exposed participants with the non-exposed individuals. The size of the shaded square is proportional to the percent weight of each study. The horizontal lines represent 95% CIs. The diamond data marker indicates the summary OR. CI, confidence interval; OR, odds ratio.
Data extraction
We collected data on the first author’s last name, year of publication, region of study, number of participants and events (or number of cases and controls), age of participants (mean or range), proportion of men, follow-up years (for cohort studies; mean, median years or person-years), exposure assessment method, categories of exposure, methods of outcome confirmation (or case confirmation), measurements of the association, and adjusted covariates in the final model. In particular, HR, RR, and OR with 95% CIs for all cadmium exposure categories versus the lowest exposure group (reference) were collected. In occupational case–controls studies, non-exposed individuals were used as the reference group in all primary studies. For testing the dose–response relationship, measurements with a continuous variable were extracted. HR, RR, and OR were transformed to their natural logarithms (ln) and the corresponding 95% CIs were used to calculate the SE. Two of the co-authors (C.C. and P.X.) independently assessed each study and extracted the relevant information. Discrepancies were resolved by group discussion.
Statistical analysis
The weighted RR and OR were used as the measurement of the overall association between cadmium exposure and lung cancer risk. HR was considered as RR in the analysis. We pooled data from cohort studies in the general population,17, 18, 19 occupational cohort studies,7, 8, 13 and occupational case–control studies,3, 10, 11 respectively, by comparing the highest to the lowest category of cadmium exposure (non-exposed group for occupational case–control studies). Random-effects models were used in the meta-analysis. Dose–response relationships of lung cancer in relation to one unit (mg/m3-years) increment in cadmium exposure in the three occupational cohort studies were estimated based on available categorical RRs7, 8, 13 using a meta-regression method.20 The overall dose–response relationship was examined by pooling continuous RRs in five occupational cohort studies.7, 8, 9, 12, 13 The weighted OR was also estimated by comparing participants exposed with cadmium with non-exposed individuals in the occupational case–control studies. In addition, we performed sensitivity analyses to detect the influence of any single study on the combined results. Heterogeneities among studies were evaluated by calculating the I2 statistic along with Cochran’s Q test. Finally, publication bias were assessed by using Egger’s regression asymmetry test. A two-sided P value ≤0.05 was considered statistically significant. All analyses were performed using STATA statistical software (Version 13.0, STATA Corporation LP, College Station, TX, USA).
Results
Study characteristics
Eleven studies,3, 7, 8, 9, 10, 11, 12, 13, 17, 18, 19 including three prospective cohort studies in the general population, five retrospective cohort studies, and three case–control studies in occupational populations, were identified in the meta-analysis. The three cohort studies in the general population consist of 22,551 participants and 354 cases with a mean follow-up of 15 years (Table 1). The five occupational cohort studies are composed of 4205 participants and 180 cases with an average follow-up of 31 years (Table 2). The three occupational case–control studies include 4740 cases and 6268 controls (Table 3).
Three cohort studies in the general population included both genders. Multivariate-adjusted HRs or RRs of lung cancer mortality were reported based on tertiles or quartiles of urinary cadmium concentrations. Five occupational cohort studies included only men. Cumulative cadmium exposures in occupational cohort and case–control studies were estimated using job histories. The multivariate-adjusted RRs of lung cancer mortality being related to cadmium exposure were determined by tertiles or quartiles of cadmium exposure in three studies,7, 8, 13 or by continuous cadmium exposure in two studies.9, 12 Among three occupational case–control studies, two studies3, 10 included only men and the other one11 included both genders. Multivariate-adjusted ORs of lung cancer risk were estimated by quartiles, quintiles or three exposure levels of cadmium exposure.3, 10, 11
Meta-analysis
The weighted RR of cohort studies in the general population suggested a non-significant association between cadmium exposure and lung cancer mortality (RR=1.42, 95% CI (0.91, 2.23)), comparing the highest to the lowest cadmium exposure group. The result was not materially affected by excluding any study each time in the sensitivity analysis. However, the heterogeneity among studies was significant (I2=88.90%, P<0.01). Egger’s test suggested no evidence of publication bias (P=0.11).
Among occupational cohort studies, the weighted RR of lung cancer mortality, by comparing the highest to the lowest cadmium exposure category, was not statistically significant (RR=0.68, 95% CI (0.33, 1.41)). No dose–response relationship was observed (RR=0.99, 95% CI (0.78, 1.26)). Omitting one study each time did not substantially change the pooled results. Significant heterogeneities were not observed in either categorical or linear analyses (I2=15.80%, P=0.31; I2=22.80%, P=0.27) Egger’s test suggested no evidence of publication bias in both analyses (P=0.70, P=0.83).
Similarly, the combined OR from occupational case–control studies indicated a non-significant association between cadmium exposure and risk of lung cancer (OR=1.61, 95% CI (0.94, 2.75)), when comparing the highest level of cadmium exposure to non-exposed. The association became statistically significant if omitting Mannetje et al. (cadmium dust) in the analysis. Of note, the association became statistically significant when comparing participants exposed to cadmium with non-exposed individuals (OR=1.21, 95% CI (1.01, 1.46)). Non-significant heterogeneities were observed across studies (I2=46.50%, P=0.11; I2=0.00%, P=0.93). Egger’s test suggested no evidence of publication bias in either analysis (P=0.76, P=0.23).
Discussion
Although this meta-analysis did not reveal a statistically significant association, the possibility that cadmium exposure may increase risk of lung cancer cannot be completely ruled out in either general or occupational population.
In 2003 and 2007, two systematic reviews14, 15 suggested a potentially positive association between cadmium exposure and risk of lung cancer. Recently, Nawrot et al.16 reported evidence supporting the positive association by using a meta-analytical approach with three cohort studies in the general population. Of note, all studies included in the two systematic reviews, except one,7 have been updated. The present meta-analysis included all available studies and the latest findings from literature, except the results from those studies cannot be combined with others (e.g., Kazantzis et al.21 did not report HR, RR or OR with corresponding 95% CI, and Nawrot et al.22 reported HR of lung cancer with a two-unit increment in log scale of cadmium, which is a different measure from that of other studies). Thus, the present meta-analysis provides the updated overall association between cadmium exposure and risk of lung cancer. In addition, the present study is the first meta-analysis that investigated the association between cadmium exposure and risk of lung cancer in both general and occupational populations. Also, all included cohort studies had long follow-up periods, especially for the studies conducted in occupational populations.
However, some limitations exist in this meta-analysis. First, included primary studies are not ideally abundant due to lack of large-scale cohort studies in both populations. Still, our study has combined the most comprehensive and updated findings in the literature. Second, significant heterogeneity was observed among the cohort studies. The reason might be that the range of cadmium exposure varies substantially across studies. Nevertheless, based on the existing literature,23 we can reasonably make a linear assumption and estimate the pooled RR of lung cancer risk in relation to cadmium exposure. Of note, when omitting one case–control study, the combined association became statistically significant. Presumably, this change was due to few case–control studies being included in the meta-analysis. Third, the possible impact of bias from the primary studies could not be ruled out. However, sensitivity analyses demonstrated the robustness of the findings, though stratified analyses or meta-regression could not be conducted due to the relatively small number of studies. Fourth, a potential publication bias resulting from the exclusion of articles published in a language other than English or any unpublished studies was not impossible, even though Egger’s regression asymmetry test did not suggest publication bias for this meta-analysis.
The observed association between cadmium exposure and risk of lung cancer in the present meta-analysis was highly likely to be underestimated due to a few possible reasons. First, the statistical power may not be sufficient because of the relatively small number of participants in the primary studies, especially those in the highest category of cadmium exposure. In fact, when we collapsed all exposed groups to compare participants exposed to cadmium with non-exposed individuals, the association became statistically significant. Second, not all occupational studies have adjusted for other heavy metals, which may confound the association, probably due to lack of information. Similarly, the null association observed in the general population might be confounded by potential protective factors of cancers, such as high vegetables and fruits consumption.24 Third, cadmium exposure measured based on job histories may not be as reliable as biomarkers, though it is the most common method used in occupational studies. However, air samples at different historical time points were collected in half of the studies to determine the cadmium concentrations at the workplaces, which might reduce this measurement error. Fourth, Healthy Worker Effect has been shown in several occupational studies8, 9, 13. This important survival bias might lead to underestimated risk estimates, which should be kept in mind when interpreting the results of occupational cohort studies.
In summary, although this updated meta-analysis did not provide solid evidence, a positive association between cadmium exposure and risk of lung cancer in either general or occupational population could not be ruled out based on findings from the present meta-analysis. Also, the absence of significant association in the present meta-analysis should not change ongoing public health and policy efforts to reduce cadmium exposure of industrial workers and cadmium contamination in the environment, which could still have potential detrimental influence on human health based on the existing literature, especially at high exposure levels.
References
Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D . Global cancer statistics. CA Cancer J Clin 2011; 61: 69–90.
Siegel R, Ma J, Zou Z, Jemal A . Cancer statistics, 2014. CA Cancer J Clin 2014; 64: 9–29.
Beveridge R, Pintos J, Parent MÉ, Asselin J, Siemiatycki J . Lung cancer risk associated with occupational exposure to nickel, chromium VI, and cadmium in two population-based case-control studies in Montreal. Am J Ind Med 2010; 53: 476–485.
International Agency for Research on Cancer, World Health Organization. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Beryllium, cadmium, mercury, and exposures in the glass manufacturing industry: IARC, 1993.
Agency for Toxic Substances and Disease Registry. Potential for human exposure. In: Toxicological Profile for Cadmium. 2011, 277–331.
U.S. Department of Health and Human Services. Cadmium and Cadmium Compounds. 2011.
Sorahan T, Lister A, Gilthorpe MS, Harrington JM . Mortality of copper cadmium alloy workers with special reference to lung cancer and non-malignant diseases of the respiratory system, 1946-92. Occup Environ Med 1995; 52: 804–812.
Sorahan T, Esmen N . Lung cancer mortality in UK nickel-cadmium battery workers, 1947–2000. Occup Environ Med 2004; 61: 108–116.
Park RM, Stayner LT, Petersen MR, Finley-Couch M, Hornung R, Rice C . Cadmium and lung cancer mortality accounting for simultaneous arsenic exposure. Occup Environ Med 2012; 69: 303–309.
Martin J-C, Imbernon E, Goldberg M, Chevalier A, Bonenfant S . Occupational risk factors for lung cancer in the French electricity and gas industry a case-control survey nested in a cohort of active employees. Am J Epidemiol 2000; 151: 902–912.
Mannetje A, Bencko V, Brennan P, Zaridze D, Szeszenia-Dabrowska N, Rudnai P et al. Occupational exposure to metal compounds and lung cancer. Results from a multi-center case–control study in Central/Eastern Europe and UK. Cancer Causes Control 2011; 22: 1669–1680.
Jones S, Atkin P, Holroyd C, Lutman E, Batlle JV, Wakeford R et al. Lung cancer mortality at a UK tin smelter. Occup Med 2007; 57: 238–245.
Järup L, Bellander T, Hogstedt C, Spång G . Mortality and cancer incidence in Swedish battery workers exposed to cadmium and nickel. Occup Environ Med 1998; 55: 755–759.
Silvera SAN, Rohan TE . Trace elements and cancer risk: a review of the epidemiologic evidence. Cancer Causes Control 2007; 18: 7–27.
Verougstraete V, Lison D, Hotz P . Cadmium, lung and prostate cancer: a systematic review of recent epidemiological data. J Toxicol Environ Health Part B Crit Rev 2003; 6: 227–256.
Nawrot TS, Martens DS, Hara A, Plusquin M, Vangronsveld J, Roels HA et al. Association of total cancer and lung cancer with environmental exposure to cadmium: the meta-analytical evidence. Cancer Causes Control 2015; 26: 1281–1288.
Qian L, Nishijo M, Nakagawa H, Morikawa Y, Sakurai M, Nakamura K et al. Relationship between urinary cadmium and mortality in habitants of a cadmium-polluted area: a 22-year follow-up study in Japan. Chin Med J 2011; 124: 3504–3509.
García-Esquinas E, Pollan M, Tellez-Plaza M, Francesconi KA, Goessler W, Guallar E et al. Cadmium exposure and cancer mortality in a prospective cohort: the Strong Heart Study. Environ Health Perspect 2014; 122: 363.
Adams SV, Passarelli MN, Newcomb PA . Cadmium exposure and cancer mortality in the Third National Health and Nutrition Examination Survey cohort. Occup Environ Med 2012; 69: 153–156.
Borenstein M, Hedges LV, Higgins J, Rothstein HR . Meta-regression. In: Introduction to Meta-analysis 2009, 187–203.
Kazantzis G, Lam T-H, Sullivan KR . Mortality of cadmium-exposed workers: a five-year update. Scand J Work Environ Health 1988; 14: 220–223.
Nawrot T, Plusquin M, Hogervorst J, Roels HA, Celis H, Thijs L et al. Environmental exposure to cadmium and risk of cancer: a prospective population-based study. Lancet Oncol 2006; 7: 119–126.
Stayner L, Steenland K, Dosemeci M, Hertz-Picciotto I . Attenuation of exposure-response curves in occupational cohort studies at high exposure levels. Scand J Work Environ Health 2003; 29: 317–324.
Soerjomataram I, Oomen D, Lemmens V, Oenema A, Benetou V, Trichopoulou A et al. Increased consumption of fruit and vegetables and future cancer incidence in selected European countries. Eur J Cancer 2010; 46: 2563–2580.
Acknowledgements
Source of funding: Drs. Xun and He were partially supported by grants from the NIH (R01HL081572, R01ES021735 and R03CA139261). The funding sources had no involvement in the study design; the collection, analysis and interpretation of data; the writing of the report; and the decision to submit the article for publication.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Chen, C., Xun, P., Nishijo, M. et al. Cadmium exposure and risk of lung cancer: a meta-analysis of cohort and case–control studies among general and occupational populations. J Expo Sci Environ Epidemiol 26, 437–444 (2016). https://doi.org/10.1038/jes.2016.6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jes.2016.6
- Springer Nature America, Inc.
Keywords
This article is cited by
-
Estimation of health risks associated with dietary cadmium exposure
Archives of Toxicology (2023)
-
Risk mapping of lung cancer: a comprehensive appraisal of published meta-analyses incorporating Mendelian randomization studies
Journal of Cancer Research and Clinical Oncology (2023)
-
Identification and Characterization of Cadmium-Related Genes in Liver Carcinoma
Biological Trace Element Research (2018)