
Abstract
The objective of this study was to investigate the impact of metabolic syndrome (MS) on carotid atherosclerosis in a Japanese population. A total of 1727 subjects (805 males and 922 females) were included. Intima-media thickness (IMT) was measured using ultrasonography. To evaluate the independent determinants of IMT, a stepwise multiple regression analysis was employed that included age, current smoking habit, LDL-C, HbA1c and the MS components (SBP, DBP, TG, HDL-C, FBG, and WC) as independent variables. Multivariate regression analyses were performed to determine the independent associations of the MS components with IMT. In males, age (β=0.383, P<0.001), SBP (β=0.237, P<0.001), LDL-C (β=0.188, P<0.001), current smoking habit (β=0.124, P=0.007) and HbA1c (β=0.110, P=0.014) were significantly associated with IMT. In females, age (β=0.474, P<0.001), SBP (β=0.130, P=0.003) and FBG (β=0.110, P=0.038) were significantly associated with IMT. The present study demonstrated that an elevated number of MS components, with or without central obesity, is associated with higher IMT. Among the analyzed components, hypertension has the strongest association with higher IMT.
Similar content being viewed by others


Introduction
It is well known that even though each of the arteriosclerotic risk factors alone is not serious, the risk becomes more ‘powerful’ when they are combined. According to this concept, metabolic syndrome (MS) has been highlighted as a cluster of risk factors for arteriosclerosis. Intima-media thickness (IMT) of the carotid arteries, as determined via non-invasive ultrasonography, is a useful measure for preclinical atherosclerosis1, 2, 3 and predicts an individual’s future risk of cerebrovascular and cardiovascular events.4, 5, 6, 7 Although several epidemiological studies have demonstrated a correlation between MS and carotid atherosclerosis, most of these studies used data from western populations8, 9, 10, 11, 12 or MS definitions that differ from Japanese definitions.13, 14, 15, 16 Hence, few studies have investigated the association between carotid IMT and MS based on the Japanese criteria definitions in a large Japanese population. In addition, it remains unclear whether each component of MS confers a similar risk for increasing IMT and which components of MS are more strongly associated with IMT.8, 9, 17, 18
The objective of this study was to investigate the impact of MS on carotid atherosclerosis in a community-based population in Japan.
Methods
Study population
The subjects in the present study were residents living in two communities in the western part of Japan (Minabe Town and Katsuragi Town) who participated in a specific health checkup conducted between July 2011 and July 2012. A total of 1727 subjects (805 males and 922 females) were enrolled in this study. All participants were informed about the aim of the study and provided informed consent before the examination. The study was approved by the ethical committee of Wakayama Medical University.
Evaluation of risk factors
Body height and weight were measured using a standard protocol and were then used to calculate body mass index (BMI). Waist circumference (WC) was measured by trained staff members at the umbilical level, with the subjects in a standing position. Resting systolic and diastolic blood pressures (SBP and DBP), respectively, were measured in the seated position using an automated sphygmomanometer (HEM-907; Omron, Kyoto, Japan). Blood samples were collected from an antecubital vein in the morning after an overnight fast. Serum total cholesterol (T-C), high-density lipoprotein cholesterol (HDL-C), triglycerides (TG) and fasting blood glucose (FBG) were measured using enzymatic methods. An automated ion-exchange chromatographic method was used to calculate hemoglobin A1c (HbA1c). Each patient’s low-density lipoprotein cholesterol (LDL-C) level was calculated using the Friedewald formula (T-C (mg dl−1)−HDL-C (mg dl−1)−0.2 × TG (mg dl−1)), and those patients with a TG level ⩾400 mg dl−1 were excluded from the study. A questionnaire was administered to evaluate smoking habits and the use of medications for hypertension, dyslipidemia and diabetes mellitus. Subjects with smoking habits were identified as current regular smokers.
Ultrasonography examination
Carotid atherosclerosis was determined using a B-mode ultrasound machine (GM-72P00A; Panasonic, Kanagawa, Japan) equipped with an 8.5-MHz linear scan type B-mode probe. The subjects were kept in the supine position with their heads slightly extended. We measured the thickness of the IMT on the far wall of the bilateral common carotid artery (CCA) at ~10 mm proximal to the bifurcation of the carotid artery because the image at that site is more clearly depicted than the site near the wall.5, 19 The mean value of the area was calculated for each side, and the mean value (mean IMT) was used for the further analyses. If carotid plaque was isolated, the carotid IMT was measured outside of that portion. The average values of both the right and left arteries from each segment were used for analyses (the software program gives the average thickness of the IMT complex on the left and right side of the CCA). The images were measured in an automated analyzing system composed of four automated settings (Auto ROI, Auto Trigger, Auto IMT, Auto Freeze) based on ultrasound echo signal processing.20 By using this method, we overcame some problems, such as the high time requirement of a more complicated procedure and insufficient reproducibility due to operator bias.
Definition of MS
MS was defined using the Japanese criteria that consist of central obesity and the presence of two or more of the following conditions: hypertension, dyslipidemia and hyperglycemia. Central obesity was defined as WC ⩾85 cm for males and ⩾90 cm for females. Hypertension was defined as SBP ⩾130 and/or DBP ⩾85 mm Hg or a history of treatment for hypertension. Dyslipidemia was defined as TG ⩾150 mg dl−1 and/or HDL-C <40 mg dl−1 or a history of treatment for dyslipidemia. Hyperglycemia was defined as FBG ⩾110 mg dl−1 or a history of treatment for diabetes mellitus.
Statistical analysis
The data are presented as the mean values±s.d., unless otherwise specified. Logarithmic transformation was performed before the analyses if the variables were normally distributed. Differences in the characteristics of the subjects with and without MS were analyzed by Student’s t-test for continuous variables and by the chi-square test for categorical variables. The effects of MS and the increasing number of MS components on IMT were investigated using the analysis of covariate (ANCOVA) after controlling for age as a covariate. To evaluate the independent determinants of IMT, a stepwise multiple regression analysis was employed that included age, current smoking habit, LDL-C, HbA1c and the MS components (SBP, DBP, TG, HDL-C, FBG and WC) as independent variables. The impact of the number of MS components on IMT was compared among subjects with and without central obesity using two-way analysis of variance (ANOVA; (those with central obesity vs. those without central obesity) × number of MS components). When appropriate, post hoc testing was performed using one-way ANOVA followed by the Bonferroni correction for multiple comparisons. Values <0.05 were considered significant in all analyses. Data analyses were performed using the SPSS statistical software package (SPSS Software; Chicago, IL, USA).
Results
The age range of the enrolled subjects was 34–75 years, and the mean age was 59.9±9.0 years (males, 59.7±10.2 years; females, 60.2±9.4 years).
Table 1 shows the clinical and biochemical characteristics of the study population according to the presence or absence of MS. In males and females, subjects with MS had significantly higher age, BMI, WC, SBP, DBP, TG, FBG and HbA1c and lower HDL-C than those without MS. Moreover, hypertension, dyslipidemia and hyperglycemia occurred significantly more frequent in subjects with MS than in those without MS. In addition, females with MS had significantly higher LDL-C compared with those without MS. According to Japanese criteria, MS was detected in 152 males (18.9%) and 51 females (5.6%). Hypertension (males, 54.8%; females, 49.1%) was the most frequent MS component, followed by dyslipidemia (males, 38.2%; females, 32.4%) and hyperglycemia (males, 20.0%; females, 9.8%) in both sexes.
The use of antihypertensive, antidyslipidemic and antihyperglycemic drugs were 499 (28.9%), 256 (14.8%) and 75 (4.3%), respectively.
Comparisons of IMT according to the presence or absence of MS and the number of MS components are shown in Table 2. In both sexes, IMT tended to be greater in subjects with MS than in those without MS. However, the difference did not reach statistical significance after adjustment for age by ANCOVA. A gradual increase in IMT was observed as the number of MS components increased in both sexes. In addition, the IMT of the male subjects who had more than one MS component was significantly greater than that of subjects without any MS components. Female subjects with one MS component had significantly higher IMT than those without any MS components.
The impact of the increasing number of MS components on IMT was compared among subjects with and without central obesity (Figure 1). Despite the presence or absence of central obesity, the associations between the number of MS components and IMT were similar in both sexes. Furthermore, the MS component effect was significant, but neither the group effect (central obesity) nor the group × MS component interaction was significant by two-way ANOVA.

IMT according to the number of MS components among subjects with and without central obesity. The circle plots represent the IMT values of the subjects with increasing number of MS components including hypertension, dyslipidemia and hyperglycemia. Closed circles indicate subjects with central obesity and open circles those without central obesity. Data are shown as the mean±s.d. MS components effect was significant (P<0.01) but central obesity effect was not significant in both genders by two-way ANOVA. **P<0.01 (vs. the subjects without any MS component by post hoc analysis using Bonferroni correction).
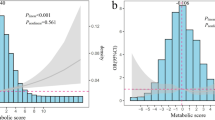
To identify which MS component had a more prominent impact on IMT, we selected subjects who had only one MS component. The effects of hypertension, dyslipidemia and hyperglycemia on IMT are shown in Figure 2. The same results were obtained in the subjects without anti-hypertensive, antidyslipidemic and antihyperglycemic drugs.

Effects of each MS component on IMT. Hypertension, subjects with hypertension and without any other MS components; dyslipidemia, subjects with dyslipidemia and without any other MS components; hyperglycemia, subjects with hyperglycemia and without any other MS components; none, subjects without any MS components. Data are shown as mean ±s.d. *P<0.05 vs. none group by ANCOVA adjusted for age and smoking habit.
The subjects with any MS components tended to have greater IMT than subjects without any MS components. However, a significant difference was found in only hypertension in both sexes. Multivariate regression analyses were performed to determine the independent associations of MS components with IMT (Table 3). In males, age (β=0.383, P<0.001), SBP (β=0.237, P<0.001), LDL-C (β=0.188, P<0.001), current smoking habit (β=0.124, P=0.007) and HbA1c (β=0.110, P=0.014) were significantly associated with IMT. In females, age (β=0.474, P<0.001), SBP (β=0.130, P=0.003) and FBG (β=0.110, P=0.038) were significantly associated with IMT.
Discussion
We analyzed the data from 1727 subjects (aged 34–75 years) in a general Japanese population and found that the clustering of MS components contributes to increased IMT. Among the MS components, hypertension had the greatest impact on IMT.
The impact of an increasing number of MS components on atherosclerosis was previously investigated in several epidemiological studies.8, 10, 11, 21 Similarly, we found that IMT increased as the number of MS components increased in both genders.
However, the association between IMT and MS did not reach statistical significance after adjusting for age and smoking. In this regard, we showed that IMT in subjects without central obesity was similar to that in subjects with central obesity when they had the same number of MS components (two-way ANOVA). Noda et al.22 found a higher prevalence of carotid atherosclerosis in subjects with a higher number of MS components, irrespective of central obesity. Moreover, Lee et al.23 reported that individuals in the central obesity/metabolic syndrome group and the no central obesity/metabolic syndrome group were at similar risk of ischemic heart disease. This finding suggests that central obesity is not an indicator of increased risk of ischemic heart disease.
Central obesity is a significant predictor of insulin resistance that causes impaired glucose tolerance, hypertension and dyslipidemia.24 Our findings suggest that central obesity may not directly cause arteriosclerosis but, instead, may cluster risk factors including hypertension, dyslipidemia and hyperglycemia. Yasuda et al.25 suggested that central obesity itself has a key role in the clustering of risk factors, which is positively associated with the development of atherosclerosis.
Our most important finding is that the risk of developing IMT was associated with the number of MS components but not with central obesity. We should not ignore subjects without central obesity who have a clustering of MS components because they are also at a risk of developing IMT.
It has been unclear whether each individual component of MS is equally associated with IMT and whether the presence of a particular component confers an increased risk. We investigated the impact of each MS component on increases in IMT and demonstrated that subjects with hypertension but not those with dyslipidemia and hyperglycemia had IMT values that were significantly higher than those of subjects without any MS components in both sexes. In addition, multivariate regression analyses revealed that among MS components, BP was most strongly associated with IMT in both sexes. These results suggest that not all MS components confer similar atherosclerotic risk and that hypertension might be the most important determinant in the development of increased IMT with investigation of only one MS component.
Hypertension has been recognized as a strong risk factor for atherosclerotic cardiovascular disease and stroke. Ishizaka et al.14 have shown that among the five MS components based on the cutoff points of ATP-III, hypertension had a greater odds ratio for carotid plaque independent of age, gender, T-C and smoking status. Su et al.26 also demonstrated that among risk factors including hypertension, hypercholesterolemia, hypertriglyceridemia and diabetes mellitus, hypertension was the most prominent risk factor for thicker IMT and the development of carotid stenosis.
In the present study, hypertension was the most common component of MS in both sexes. Therefore, hypertension is important to both the frequency and development of arteriosclerosis.
Several population-based studies have found associations between IMT and conventional atherosclerotic risk factors other than BP, including smoking, dyslipidemia and hyperglycemia.27, 28, 29 In our study, multivariate analysis results showed that LDL-C, smoking habit and HbA1c were associated with IMT in males and FBG was associated with IMT in females. Accordingly, although hypertension seems to be the most important risk factor for the development of IMT, we should not ignore subjects with risk factors other than BP.
We consider each MS component, including hypertension, dyslipidemia and hyperglycemia, as an equal risk factor for increased IMT. The contribution of MS components to the impact on IMT, however, may be unbalanced. The present study demonstrated that subjects with hypertension are likely to be at a higher risk for carotid atherosclerosis than subjects without hypertension, who have only one MS component. When hypertension is among an individual’s MS components, particular care might be required in their risk assessment and interventional approach.
This study has some advantages that are worth mentioning. First, we included a large study population, which enabled the assessment of gender differences. Second, we used an automated ultrasound analyzing system to measure the carotid IMT, which provided an accurate measure of atheroma development and enabled the study of the association between MS and atherosclerosis.
There are limitations in interpreting the present findings. First, the study population may not be representative of the Japanese population as a whole. We only included those subjects who were able to participate in annual medical health checks in the community; therefore, the present study has the potential for selection bias by including relatively healthier subjects. In our study, the subjects’ carotid atherosclerotic thicknesses were relatively thinner, and the prevalence of MS was less than those reported in previous studies in Japan.1 Thus, it is possible that the frequency of MS and the observed associations of MS with the carotid IMT were underestimated. Second, the present data, obtained by a cross-sectional study, cannot allow the temporal sequence of the observed association to be inferred. Longitudinal observations are required to evaluate longitudinal effects of MS in the progression of IMT.
Conclusion
The present study demonstrated that an increased number of MS components, in the presence or absence of central obesity, is associated with higher IMT. We also found that the risk of developing IMT differs among MS components; hypertension is the most important determinant in the development of IMT. Our finding strongly supports the idea that the simple diagnosis of MS is not sufficient to define a subject’s atherosclerotic risk factors and that it might be advisable to evaluate MS components both qualitatively and quantitatively.
References
Mannami T, Baba S, Ogata J . Strong and significant relationships between aggregation of major coronary risk factors and the acceleration of carotid atherosclerosis in the general population of a Japanese city: the Suita Study. Arch Intern Med 2000; 160: 2297–2303.
Raitakari O, Juonala M, Kähönen M, Taittonen L, Laitunen T, Mäki-Torkko N, Järvisalo MJ, Uhari M, Jokinen E, Rönnemaa T, Akerblom HK, Viikari JS . Cardiovascular risk factors in Childhood and carotid artery intima -media thickness in adulthood: the cardiovascular risk in young Finns study. JAMA 2003; 290: 2277–2283.
Bonithon-Kopp C, Jouven X, Taquet A, Touboul PJ, Guize L, Scarabin PY . Early carotid atherosclerosis in healthy middle-aged women A follow-up study. Stroke 1993; 24: 1837–1843.
O'Leary DH, Polak JF, Kronmal RA, Manolio TA, Burke GL, Wolfson SK Jr . Carotid-artery and media thickness as a risk factor for myocardial infarction and stroke in older adults. N Engl J Med 1999; 340: 14–22.
Salonen J, Salonen R . Ultrasonographically assessed carotid morphology and the risk of coronary heart disease. Arterioscler Thromb Vasc Biol 1991; 11: 1245–1249.
Bots ML, Hoes AW, Koudstaal PJ, Hofman A, Grobbee DE . Common carotid intima-media thickness and risk of stroke and myocardial infarction: the Rotterdam study. Circulation 1997; 96: 1432–1437.
Chambless LE, Heiss G, Folsom AR, Rosamond W, Szklo M, Sharrett AR, Clegg LX . Association of coronary heart disease incidence with carotid arterial wall thickness and major risk factors: the atherosclerosis risk in communities (ARIC) Study, 1987-1993. Am J Epidemiol 1997; 146: 483–494.
Pietri P, Vlachopoulos C, Vyssoulis G, Ioakeimidis N, Stefanadis C . Macro- and microvascular alterations in patients with metabolic syndrome: sugar makes the difference. Hypertens Res 2014; 37: 452–456.
Iglseder B, Cip P, Malaimare L, Ladurner G, Paulweber B . The metabolic syndrome is a stronger risk factor for early carotid atherosclerosis in women than in men. Stroke 2005; 36: 1212–1217.
Pollex RL, Al-Shali KZ, House AA, Spence JD, Fenster A, Mamakeesick M, Zinman B, Harris SB, Hanley AJ, Hegele RA . Relationship of the metabolic syndrome to carotid ultrasound traits. Cardiovasc Ultrasound 2006; 4: 28–35.
Koskinen J, Kähönen M, Viikari JS, Taittonen L, Laitinen T, Rönnemaa T, Lehtimäki T, Hutri-Kähönen N, Pietikäinen M, Jokinen E, Helenius H, Mattsson N, Raitakari OT, Juonala M . Conventional cardiovascular risk factors and metabolic syndrome in predicting carotid intima-media thickness progression in young adults: the cardiovascular risk in young Finns study. Circulation 2009; 120: 229–236.
Herder M, Arntzen KA, Johnsen SH, Mathiesen EB . The metabolic syndrome and progression of carotid atherosclerosis over 13 years. The Tromso study. Cardiovasc Diabetol 2012; 11: 77–90.
Lee YH, Shin MH, Kweon SS, Rhee JA, Ryu SY, Ahn HR, Choi JS . Metabolic syndrome and carotid artery parameter in Koreans aged 50 years and older. Cir J 2010; 74: 560–566.
Ishizaka N, Ishizaka Y, Toda E, Hashimoto H, Nagai R, Yamakado M . Hypertension is the most common component of metabolic syndrome and the greatest contributor to carotid arteriosclerosis in apparently healthy Japanese individuals. Hypertens Res 2005; 28: 27–34.
Matoba Y, Inoguchi T, Suzuki S, Nasu S, Hashimoto T, Yanase T, Nawata H, Takayanagi R . Impact of metabolic syndrome on the progression of Intima-Media thickening in Japanese a follow-up study. Diabetes Res Clin Pract 2009; 86: e50–e53.
Teramura M, Emoto M, Araki T, Yokoyama H, Motoyama K, Shinohara K, Mori K, Koyama H, Shoji T, Inaba M, Nishizawa Y . Clinical impact of metabolic syndrome by modified NCEP-ATPIII criteria on carotid atherosclerosis in Japanese adults. J Atheroscler Thromb 2007; 14: 172–178.
Kawamoto R, Tomita H, Oka Y, Kodama A, Kamitani A . Metabolic syndrome amplifies the LDL -cholesterol associated increases in carotid atherosclerosis. Intern Med 2005; 44: 1232–1238.
Prejbisz A, Florczak E, Pręgowska-Chwała B, Klisiewicz A, Kuśmierczyk-Droszcz B, Zieliński T, Makowiecka-Cieśla M, Kołodziejczyk-Kruk S, Śliwiński P, Januszewicz A . Relationship between obstructive sleep apnea and markers of cardiovascular alterations in never-treated hypertensive patients. Hypertens Res 2014; 37: 573–579.
Sidhu PS, Desai SR . A simple and reproducible method for assessing intimal-medial thickness of the common carotid artery. Br J Radiol 1997; 70: 85–89.
Kawabata A, Suzuki T, Urabe M . Automated IMT measurement for atherosclerosis screening. Panasonic Tech J 2011; 57: 10–15.
Ninomiya T, Kubo M, Doi Y, Yonemoto K, Tanizaki Y, Rahman M, Arima H, Tsuryuya K, Iida M, Kiyohara Y . Impact of metabolic syndrome on the development of cardiovascular disease in a general Japanese population: the Hisayama study. Stroke 2007; 38: 2063–2069.
Noda H, Iso H, Yamashita S, Ueno H, Yokode M, Yamada N, Ouchi Y, Defining Vascular Disease (DVD) Research Group. Risk stratification based on metabolic syndrome as well as non-metabolic risk factors in the assessment of carotid atherosclerosis. J Atheroscler Thromb. 2011; 18: 504–512.
Lee J, Ma S, Heng D, Tan CE, Chew SK, Hughes K, Tai ES . Should central obesity be an optional or essential component of the metabolic syndrome? Ischemic heart disease risk in the Singapore Cardiovascular Cohort Study. Diabetes Care 2007; 30: 343–347.
Matsuzawa Y, Funahashi T, Nakamura T . The concept of metabolic syndrome: contribution of visceral fat accumulation and its molecular mechanism. J Atheroscler Thromb 2011; 18: 629–639.
Yasuda T, Matsuhisa M, Fujiki N, Sakamoto F, Tsuji M, Fujisawa N, Kimura M, Ishibashi R, Kaneto H, Yamasaki Y, Watarai T, Imano E . Is central obesity a good predictor of carotid atherosclerosis in Japanese type 2 diabetes with metabolic syndrome? Endocrine J 2007; 54: 695–702.
Su TC, Jeng JS, Chien KL, Sung FC, Hsu HC, Lee YT . Hypertension status is the major determinant of carotid atherosclerosis: a community -based study in Taiwan. Stroke 2001; 32: 2265–2271.
Johnson HM, Douglas PS, Srinivasan SR, Bond MG, Tang R, Li S, Chen W, Berenson GS, Stein JH . Predictors of carotid intima-media thickness progression in young adults: the Bogalusa Heart Study. Stroke 2007; 38: 900–905.
Salonen R, Salonen J . Determinants of carotid intima-media thickness: a population-based ultrasonography study in eastern Finnish men. J Intern Med 1991; 229: 225–231.
Wagenknecht LE, Zaccaro D, Espeland MA, Karter AJ, O'Leary DH, Haffner SM . Diabetes and progression of carotid atherosclerosis: the insulin resistance atherosclerosis study. Arterioscler Thromb Vasc Biol 2003; 23: 1035–1041.
Acknowledgements
We thank the staff of the Division of Health and Welfare of Minabe and Katsuragi for their cooperation in this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Hirata, C., Miyai, N., Idoue, A. et al. Effect of metabolic syndrome components and their clustering on carotid atherosclerosis in a sample of the general Japanese population. Hypertens Res 39, 362–366 (2016). https://doi.org/10.1038/hr.2015.152
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2015.152
- Springer Nature Singapore Pte Ltd.
Keywords
This article is cited by
-
Reference values of one-point carotid stiffness parameters determined by carotid echo-tracking and brachial pulse pressure in a large population of healthy subjects
Hypertension Research (2017)
-
The ratio of monocyte frequency to HDL cholesterol level as a predictor of asymptomatic organ damage in patients with primary hypertension
Hypertension Research (2017)
-
The relationship between obesity and hypertension: an updated comprehensive overview on vicious twins
Hypertension Research (2017)
-
Preventive effect of Eucommia leaf extract on aortic media hypertrophy in Wistar-Kyoto rats fed a high-fat diet
Hypertension Research (2017)
-
Clinical significance of ‘cardiometabolic memory’: a systematic review of randomized controlled trials
Hypertension Research (2017)