
Abstract
Background/Objectives:
The body mass index (BMI) of breakfast eaters is frequently reported to be lower compared with that of breakfast skippers. This is not explained by differences in energy intakes, indicating there may be other mechanisms serving to drive this paradoxical association between breakfast and BMI. This study aimed to investigate the effect of eating breakfast versus morning fasting on measures predominantly of metabolism in lean and overweight participants who habitually eat or skip breakfast.
Subjects/Methods:
Participants (n=37) were recruited into four groups on the basis of BMI (lean and overweight) and breakfast habit (breakfast eater and breakfast skipper). Participants were randomly assigned to a breakfast experimental condition, breakfast eating or no breakfast, for 7 days and then completed the alternative condition. At the end of each breakfast experimental condition, measurements were made before and after a high carbohydrate breakfast of 2274±777 kJ or a rest period. Resting metabolic rate, thermic effect of food (TEF), blood glucose, insulin and leptin levels were recorded. Hunger and ‘morningness’ were assessed and pedometers worn.
Results:
Lean participants had lower fasting insulin levels (P=0.045) and higher insulin concentrations following breakfast (P=0.001). BMI and breakfast habit did not interact with the experimental breakfast condition, with the exception of hunger ratings; breakfast eaters were hungrier in the mornings compared with breakfast skippers in the no breakfast condition (P=0.001).
Conclusions:
There is little evidence from this study for a metabolic-based mechanism to explain lower BMIs in breakfast eaters.
Similar content being viewed by others


Introduction
Body mass index (BMI) is frequently reported to be lower in adults who habitually eat breakfast than in people who typically skip breakfast.1, 2, 3, 4, 5 However, a mechanism explaining this possible difference has not been established.6 Contenders for a mechanism include differences in food intakes4, 7 and/or energy expenditure (EE).8 However, there is now evidence that eating breakfast may actually increase energy intakes,9 as also reported by the participants from this study who ate 671±1808 kJ/day more when eating breakfast compared with not eating breakfast.10 This makes the difference in BMI even more unexpected and emphasises the need to investigate other potential mechanisms. Skipping breakfast has been shown to elevate blood glucose levels and alter metabolism including the resting metabolic rate (RMR) and the thermic effect of food (TEF) of people with a range of BMIs,11 and this could also have a role in establishing metabolic differences between breakfast eaters and breakfast skippers as both contribute to EE. Furthermore, leptin, an important peripheral regulator of energy metabolism, has a role in maintaining energy balance and correlates with body fat mass and the BMI.12
Farschi et al.13, 14 described differences in post-prandial thermogenesis following regular and irregular meals in lean and obese women, reporting a lower TEF following irregular meal frequency that could contribute to weight gain in the long term, and impaired post-prandial insulin sensitivity in lean women after omitting breakfast.15 However, some research14, 16 did not report the participants’ breakfast habits, and this could be of relevance as differences in BMI between breakfast eaters and skippers are possibly associated with differing morning habits.17 Such habits may in turn be linked to a preference for early or late rising and being more active earlier or later in the day, respectively; these patterns have been considered by researchers by reference to the concept of ‘morningness’,18 and these time of day preferences may be linked to caffeine intakes. Several studies19, 20 have shown that people who prefer to be active in the evening consume more caffeine compared with those who are morning active. Caffeine not only increases alertness and wakefulness but may also increase daily EE and reduce appetite.21, 22
There is some evidence of greater weight loss in obese women who switch their usual morning routines from either eating breakfast to skipping breakfast or vice versa.23 However, a more recent randomised controlled trial where healthy adults were instructed to eat or skip breakfast found no noticeable effects of breakfast regime on weight loss.24
At present the available evidence is unable to clarify a mechanism that links BMI with the frequency of breakfast consumption; thus, studies aimed at explaining the underlying differences between breakfast eaters and breakfast skippers who are lean and overweight are required.6 Given the role of personal daily routines associated with morning eating, such a study should consider usual breakfast habits and morningness. Therefore, the present study investigated the effect of eating breakfast and morning fasting on measures of metabolism including post-prandial TEF, activity levels, glucose, insulin and leptin levels, along with morningness, caffeine intake and pedometer scores in lean and overweight healthy people who habitually eat or skip breakfast.
Materials and methods
Participants
The study set out to recruit participants who could be divided into the following four groups: (1) lean breakfast eaters, (2) lean breakfast skippers, (3) overweight breakfast eaters and (4) overweight breakfast skippers. The lean groups were defined by the participants having a BMI under 25 kg/m2 and the overweight groups a BMI over 25 kg/m2 (three participants in each of the overweight groups could be classified as obese). In terms of breakfast habit, an habitual ‘breakfast eater’ was defined as someone who considered themselves to eat breakfast regularly and had eaten breakfast ⩾5 days in the last week, which had consisted of >418 kJ.25 An habitual ‘breakfast skipper’ was someone who considered themselves not to be a regular breakfast eater and had eaten breakfast on 2 days or less in the past week.
A minimum total sample size of n=34 was determined on the basis of presumed and practically important differences in energy intake equivalent to a medium effect size of d=0.50, power of 80% and a two-tailed alpha of 0.05 using G*Power v3.1.15, 26 Thirty-seven healthy male and female participants (32.9±13.5 years) were recruited and completed the study (Table 1).
Exclusion criteria included dieting, diabetes, symptoms such as dizziness, fainting and blackouts, high blood pressure or cholesterol medication. Female participants with a hysterectomy or on hormone replacement therapy were excluded. In menstruating women, all measurements were made during the luteal phase of the menstrual cycle.
Design
The study employed a randomised cross-over design consisting of two 7-day experimental periods plus a minimum of a 1-week wash-out in between. Participants were randomly assigned to either the breakfast eating (BE) condition, where they consumed breakfast within an hour of waking in the morning, or the no breakfast (NB) condition, where they were asked to refrain from eating until midday; then following the wash-out period, participants took part in the alternate experimental condition. Participants attended the laboratory on the first morning of each breakfast condition and the morning after the final day of each test condition for assessment. Ethical clearance for the study was granted by the University of Roehampton Ethics Committee (Ref: LSC 11/ 010). All participants completed a health screen questionnaire and gave written informed consent before participating.
At a familiarisation session, participants answered questions related to breakfast habits, completed the composite morningness questionnaire18 and a questionnaire to measure caffeine intake (EL Gibson, unpublished, questionnaire analysis conducted using Food Standards Agency data).27 Anthropometric data are reported in Table 1.
Free-living procedures
Physical activity data
Participants were required to wear a pedometer (Yamax Digiwalker SW-200, Tokyo, Japan) for the duration of the study and report the total daily step count it recorded. Participants were requested to attach the pedometer to the waist band of their clothing as soon as they arose in the morning and remove it when they went to bed.
Laboratory procedures
Protocol of laboratory visits
Participants were asked to arrive at the laboratory at 0800 h for each testing session having fasted from 2200 h the evening before and avoided strenuous exercise for the previous 24 h. After at least 10 min rest in the supine position, baseline data recording commenced. RMR and whole blood glucose were measured and blood samples were taken to measure insulin and leptin levels. This was then followed by a 30-min intervention period during which participants either consumed breakfast or rested. Immediately after completion of the breakfast meal or rest period, participants underwent the first of a series of six repeated measurement sessions. During this time the participants remained in the laboratory under controlled conditions. For each measurement session, hunger, EE and whole blood glucose were measured. At the fifth of the six repeated test measurements (2 h post intervention), additional blood samples for insulin were taken.
Breakfast consumption
On the experimental test day at the end of the BE week, the meal was eaten in the food laboratory and consisted of some or all of cereal, toast, fruit juice, tea, coffee, fruit and yoghurt. Participants served themselves and were permitted to eat as much as they wanted of the foods provided within 30 min. The mean energy consumed during breakfast on the experimental test days was 2274±777 kJ. There was no evidence for differences in the amounts eaten at breakfast between groups. Participants in the NB condition rested in the physiology laboratory for the 30-min period.
Energy expenditure: RMR and TEF
Baseline RMR was measured using the Douglas Bag technique while the participants were lying supine. Post intervention (BE or NB) EE was also measured using the Douglas bag technique as part of the six repeated measurement sessions. RMR and EE were calculated using the Weir equation.28 The TEF was calculated as the area under the curve (AUC) using the trapezoid method as absolute EE above baseline RMR for 150 min after the breakfast intervention.29
Blood sampling and analysis
Blood samples obtained from finger pricks were collected into microvettes that contained heparin fluoride for glucose sampling and clot activator for insulin and leptin. Blood glucose was measured immediately using an YSI 2300 Stat Plus blood glucose analyser (Fleet, UK). For blood glucose, baseline concentrations were recorded and the AUC from 0 to 150 min was calculated for post-intervention readings, using the trapezoid method.30 Blood samples for insulin and leptin were left to clot at room temperature for 30 min before being centrifuged at 1000 g (2500 r.p.m.) for 5 min at 20 °C. The serum was extracted and stored at −20 °C. Insulin concentrations were later measured using a DRG Insulin ELISA kit (DRG Instruments, Marbury, Germany). Insulin concentrations at baseline and 2 h post intervention were reported, and insulin resistance was determined using the following formula.
Homeostasis model assessment for insulin resistance (HOMA-IR)=fasting serum insulin μIU/ml x fasting blood glucose (mmol/l)/22.5.31
Leptin concentrations were tested using a Quantikine Human Leptin Immunoassay (R&D Systems, Oxford, UK). Manufacturers specified an intra-assay coefficient of variation of 3.0–3.3% and an inter-assay coefficient of variation of 3.5–5.4%.
Hunger ratings
Subjective hunger ratings were assessed using the visual analogue scale, which consisted of a 100-mm line with words at each end to describe the two extreme hunger scenarios.32 The data were analysed as the baseline reading (taken on arrival at the lab) and the mean of the six post-breakfast intervention readings.
Statistical analysis
IBM SPSS Statistics 19 (IBM UK Ltd, Portsmouth, UK) and Microsoft Excel 2007 were used for statistical analysis. Normality of data was evaluated on the basis of Shapiro–Wilk’s test and histograms; equality of variances was assessed using Levene’s test. ANOVA models with two between-subject factors (BMI and breakfast habit) were generated to investigate the effects of the repeated measures test condition (breakfast versus no breakfast). 2 × 2 factorial ANOVAs were used to compare effects of BMI and breakfast habit on TEF, caffeine intake and morningness. Summary statistics are reported in tables as means±s.d.’s and in figures as means±one s.e., unless otherwise indicated. Treating the P-value as a continuous variable, analyses were deemed to provide good evidence for an effect when P<0.05, whereas P-values⩽0.10 were considered to provide some evidence of an effect.33, 34
Results
The analysis did not indicate any large effects of the experimental conditions, except for expected differences in hunger ratings, glucose and insulin levels, following the consumption of breakfast. The controlled confounds BMI and breakfast habit did not interact with the experimental test condition; with the exception of the hunger ratings, there was no evidence for an effect of any of the two-way interactions between experimental condition, BMI and breakfast habit.
Physical activity
Participating in the BE condition as opposed to the NB condition had no effect on pedometer scores as assessed by step count averaged over the 7 days spent in each breakfast condition (P=0.57); similarly, there was no evidence for interactions between experimental test condition and BMI (P=0.28), test condition and breakfast habit (P=0.99) and the 3-way interaction between all three variables and step count data (P=0.87). BMI or breakfast habit alone did not affect step count (P=0.83 and 0.39, respectively); however, there was good evidence for an interaction between BMI and breakfast habit on mean daily step count (P=0.005): overweight breakfast skippers had a mean daily step count of 10 465±3263 steps and lean skippers 7743±2969 steps. Lean habitual breakfast eaters had a mean step count of 9563±2012 steps and overweight habitual breakfast eaters 7209±2344 steps.
Energy expenditure: RMR and TEF
RMR was not affected by the experimental test condition (P=0.97), and there was no evidence that breakfast interacted with the intervention and BMI (all P -values⩾0.12) (Table 2).
Figure 1 shows TEF post breakfast consumption (0–150 min) for participants grouped by BMI and breakfast habit. There was some evidence that lean participants had a greater TEF (173.92±69.54 kJ) compared with overweight participants (131.36±75.65 kJ; P=0.086), but breakfast habit was unrelated to TEF (breakfast eaters 147.87±56.35 kJ had similar values to skippers 156.50±92.07 kJ; P=0.74).

Mean TEF post breakfast (0–150 min), measured as iAUC of absolute EE above the absolute resting metabolic rate. Error bars represent±one s.e.
Blood measures
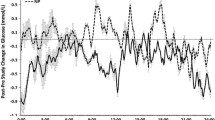
Figure 2 presents glucose concentrations at 30-min intervals post intervention and indicates, as expected, a post-intervention effect (P<0.001) on AUC glucose levels (150 min), with higher readings in the BE condition (BE: 860±99.8 mmol·min/L; NB: 680±56.7 mmol·min/L) (Table 2).

Response–time curves for glucose concentration at baseline (BL) and at 30-min intervals after the breakfast (a) and no breakfast (b) test conditions. Errors bars represent ± one s.e.
Insulin data were based on 35 participants, because of the insufficient volume of blood samples taken from two participants in one of the test conditions. There was good evidence that BMI was related to baseline insulin concentration (P=0.045); these were lower in lean compared with overweight participants. There was good evidence for an effect of breakfast condition on 2 h post meal insulin levels, with higher insulin concentrations reported for the BE than for the NB condition (P<0.001). No other interactions were reported for baseline or post breakfast insulin concentrations (P⩾0.22); (Table 2). BMI and insulin resistance were linked; HOMA-IR was higher for the overweight compared with the lean group (P=0.024). There was no evidence for an effect of test condition or breakfast habit on HOMA-IR values (P-values⩾0.49).
Leptin concentrations were available for 34 participants because of insufficient volumes of samples collected from 3 participants in one of the test conditions (Table 2). There was no evidence for an effect of test condition or breakfast habit on leptin concentration (P=0.18 and 0.30, respectively). There was good evidence for an association between BMI and leptin levels (P=0.026), with the overweight group having greater leptin concentrations compared with the lean group.
Hunger
Hunger rating curves were very different for the BE and the NB conditions (Figure 3); there was good evidence for an effect of test condition (P=0.042) and breakfast habit (P<0.001) on baseline hunger, whereby hunger scores were greater in the BE compared with NB condition, and habitual breakfast eaters were more hungry compared with habitual skippers. Also, there was good evidence for an interaction between BMI and breakfast habit (P=0.008). Overweight habitual eaters were slightly hungrier at the start of the experimental day compared with overweight habitual skippers, whereas lean habitual breakfast eaters were the hungriest and lean habitual skippers the least hungry.

Mean hunger rating curves at baseline (BL) and at 30-min intervals (a) post breakfast and (b) no breakfast intervention. Error bars represent±one s.e.
As anticipated, higher mean hunger ratings were observed in the NB compared with BE condition (P<0.001), and habitual breakfast skippers had lower mean hunger ratings compared with habitual breakfast eaters (P=0.004). There was also good evidence for an interaction between test condition and breakfast habit (P<0.001). In the BE test condition habitual breakfast eaters and skippers expressed similar mean levels of hunger, whereas habitual breakfast eaters were hungrier compared with habitual breakfast skippers in the NB condition.
Morningness
Morningness scores were similar across all groups (Figure 4). Breakfast consumption was not linked to morningess (P=0.15). Furthermore, BMI was not related to morningness (P=0.58).

Mean total caffeine intake (a) and morningness scores (b). Error bars represent±one s.e.
Caffeine
There was some evidence of an association between breakfast habit on caffeine intake (P=0.052), with breakfast skippers consuming 181.50±160.65 mg/day and breakfast eaters 95.49±82.72 mg/day. Caffeine intake was unrelated to BMI and the interaction between BMI and breakfast habit (P-values>0.65, see Figure 4).
Discussion
Many cross-sectional studies1, 5, 8 provide evidence that breakfast eaters are slimmer compared with breakfast skippers. Yet, it has also been shown that daily energy intakes may actually be higher when breakfast is consumed.9, 10 Furthermore, the present study offers no evidence that daily activity levels are associated with eating or not eating breakfast, supporting findings from a previous experiment.17 If indeed apparent differences in BMI between breakfast eaters and skippers are not a result of differences in energy intakes or activity levels, other mechanisms that influence energy balance must be at play. Although glucose, insulin and hunger levels were affected by the breakfast intervention, there was a lack of interactions between the breakfast intervention and the potential confounders BMI and breakfast habit. Therefore, evidence for a mechanism to explain why breakfast eaters tend to be leaner compared with breakfast skippers was not forthcoming from the present experiments. The non-significant findings support the recent criticism of positive reporting bias in the field of breakfast research6 and serve to refocus research towards alternative mechanistic explanations.
In the present study, there was no evidence for an association between the breakfast condition and activity levels, represented by pedometer scores. Overweight habitual breakfast skippers recorded the highest mean daily step count and, although unreported, it is remotely possible that this group was increasing their activity as well as skipping breakfast in an attempt to lose weight, although participants were screened out during recruitment if they reported to be dieting. There were no methodological reasons why the overweight groups would have higher pedometer scores.35 Future studies should consider using accelerometers to determine more accurate levels of physical activity as one study has shown that regular breakfasting may increase activities of light intensity during the morning in lean adults.36
Despite no differences in RMR between groups, there was some evidence for an association between BMI and TEF, with lean participants demonstrating higher TEF on average. However, there was no effect of breakfast habit on TEF. Other studies have shown that skipping breakfast and/or irregular meal patterns can result in blunted TEF,13 and blunted TEF could decrease overall EE, contribute to weight gain and increase insulin resistance.37, 38 Given that TEF is a key component of energy balance, and that energy balance may in some cases only be achieved over a period of weeks,39 it is conceivable that a study with a longer time frame is required.
Other than as a result of eating breakfast, there was no evidence for differences in blood glucose levels between groups. There was good evidence for an effect of BMI on insulin resistance; lean participants had lower baseline insulin levels and higher insulin concentrations following breakfast than did overweight participants. Overweight participants may have had some insulin resistance as a result of their body weight and location of body fat.40 Other studies have noted changes in insulin secretion following irregular meal patterns and have suggested that this could affect circadian secretions of insulin.14, 41 However, future studies should consider increasing the number of insulin measurements taken and investigating post-lunch effects. Leptin concentrations were higher in the overweight groups compared with the lean groups, similarly to the findings of other studies,42 but did not vary between the different test conditions in this study. There are studies that have reported that leptin levels are affected by sleep and meal timing;43 however, other research44 has suggested that this hormone may not be involved in short-term regulation of food intake but has a greater role when energy stores change, and thus a longer time frame would be required to investigate this.
Participants who were habitual breakfast eaters were hungrier in the mornings, and this was particularly pronounced in the lean breakfast eaters whose hunger ratings may reflect an habitual expectation to eat breakfast and the possibility of reduced food intake the night before.10 There was also some evidence for greater consumption of caffeine in breakfast skippers compared with breakfast eaters. Caffeine could suppress the appetite or hunger45 for breakfast, but equally this could be linked to personality type and associated with a degree of morningness as research has shown that evening types are more likely to consume greater amounts of caffeine19, 20 and are more likely to skip breakfast.46 Other studies have shown that routine breakfast eaters are more likely to be morning active, that is, report high levels of morningness,17, 47, 48 although our own data did not provide further evidence of this relationship.
Our data add to previous research indicating the lack of association between breakfasting behaviour and physical activity17 and lower self-reported energy intakes when breakfast is not consumed.9, 10, 49 Other potential mechanisms underlying a relationship between breakfasting frequency and BMI that are worth exploring include the role of molecular genetics and appetite hormones.50, 51 However, perhaps at present the most parsimonious explanation for observed cross-sectional associations between breakfast and BMI reported by other researchers 1, 2, 3 is that breakfast eaters are generally healthier and exhibit corresponding habits that include healthy eating. Thus, maybe eating breakfast is simply a marker for a healthy lifestyle,48, 52 and in turn psychosocial processes53 that can potentially help elucidate the link between breakfast and BMI may also warrant further exploration.
In summary, our study represents an experimental manipulation, with a protocol of high ecological validity, to compare the predominantly physiological effects of breakfasting versus morning fasting in lean and overweight habitual breakfast eaters and skippers. The data suggest that the measured physiological differences that arise between breakfasting and fasting are at best small. Further research is required to expand the search for the putative causal link between breakfast consumption and BMI.
References
Cho S, Dietrich M, Brown CJ, Clark CA, Block G . The effect of breakfast type on macronutrient intakes and body mass index (BMI) of Americans. J Am Coll Nutr 2003; 22: 296–302.
Barton BA, Eldridge AL, Thompson D, Affenito SG, Striegel-Moore RH, Franko DL et al. The relationship of breakfast and cereal consumption to nutrient intake and body mass index: the National Heart, Lung, and Blood Institute Growth and Health Study. J Am Diet Assoc 2005; 105: 1383–1389.
Keski-Rahkonen A, Kaprio J, Rissanen A, Virkkunen M, Rose RJ . Breakfast skipping and health-compromising behaviors in adolescents and adults. Eur J Clin Nutr 2003; 57: 842–853.
Casazza K, Fontaine KR, Astrup A, Birch L, Brown AW, Bohan Brown MM et al. Myths, presumptions, and facts about obesity. N Engl J Med 2003; 368: 446–454.
Song WO, Chun OK, Obayashi S, Cho S, Chung CE . Is consumption of breakfast associated with body mass index in US adults? J Am Diet Assoc 2005; 105: 1373–1382.
Brown AW, Bohan Brown MM, Allison DB . Belief beyond the evidence: using the proposed effect of breakfast on obesity to show 2 practices that distort scientific evidence. Am J Clin Nutr 2013; 98: 1298–1308.
Stanton JL, Keast DR . Serum cholesterol, fat intake and breakfast consumption in the United States population. J Am Coll Nutr 1989; 8: 567–572.
Timlin MT, Pereira MA . Breakfast frequency and quality in the etiology of adult obesity and chronic diseases. Nutr Rev 2007; 65: 268–281.
Levitsky DA, Pacanowski CR . Effects of skipping breakfast on subsequent energy intakes. Physiol Behav 2013; 11: 9–16.
Reeves S, Huber JW, Halsey LG, Horabady-Farahani Y, Ijadi M, Smith T . Experimental manipulation of breakfast in normal and overweight/obese participants is associated with changes to nutrient intake and energy consumption patterns. Phys Behav 2014; 133: 130–135.
Kobayashi F, Ogata H, Omi N, Nagasaka S, Yamaguchi S, Hibi M et al. Effect of breakfast skipping on diurnal variation of energy metabolism and blood glucose. Obes Res Clin Pract 2014; 8: e201–e298.
Bonifacio LA, Ikuno MR, HCCE Villar, Carvalho PE, Rubira CJ . Leptin for overweight and obesity (protocol). Cochrane Library 2010; 12.
Farshchi HR, Taylor MA, Macdonald IA . Decreased thermic effect of food after irregular compared with regular meal pattern in healthy lean women. Int J Obes 2004; 28: 653–660.
Farshchi HR, Taylor MA, Macdonald IA . Beneficial metabolic effects of regular meal frequency on dietary thermogenesis, insulin sensitivity and fasting lipid profiles in healthy obese women. Am J Clin Nutr 2005; 1: 16–24.
Farshchi HR, Taylor MA, Macdonald IA . Deleterious effects of omitting breakfast on insulin sensitivity and fasting lipid profiles in healthy lean women. Am J Clin Nutr 2005; 81: 88–396.
Farshchi HR, Farschi HR, Taylor MA, Macdonald IA . Regular meal frequency creates more appropriate insulin sensitivity and lipid profiles compared with irregular meal frequency in healthy lean women. Eur J Clin Nutr 2004; 58: 1071–1077.
Halsey L, Huber J, Low T, Ibeawuchi C, Woodruff P, Reeves S . Does breakfasting affect activity levels? An experiment into the effect of breakfast consumption on eating habits and energy expenditure. Public Health Nutr 2011; 15: 238–245.
Barton J, Costa G, Smith L, Spelten E, Totterdell P, Folkard S . The Standard Shift work Index: a battery of questionnaires for assessing shift work-related problems. Work Stress 1995; 9: 4–30.
Mitchell PJ, Redman JR . The relationship between morningness-eveningness, personality and habitual caffeine consumption. Person Indiv Diff 1993; 5: 105–108.
Penolazzi B, Natale V, Leone L, Russo PM . Individual differences affecting caffeine intake. Analysis of consumption behaviours for different times of day and caffeine sources. Appetite 2012; 58: 971–977.
Glade MJ . Caffeine – not just a stimulant. Nutrition 2010; 26: 932–938.
Belza A, Toubro S, Astrup A . The effect of caffeine, green tea and tyrosine on thermogenesis and energy intake. Eur J Clin Nutr 2009; 63: 57–64.
Schlundt DG, Hill JO, Sbrocco T, Pope-Cordle J, Sharp T . The role of breakfast in the treatment of obesity. Am J Clin Nutr 1992; 55: 645–651.
Dhurandhar E, Dawson J, Alcorn A, Larson LH, Thomas EA, Cardel M et al. The effectiveness of breakfast recommendations on weight loss: a randomized controlled trial. Am J Clin Nutr 2014; 100: 507–513.
Martin A, Normand S, Sothier M, Peyrat J, Louche-Pelissier C, Laville M . Is dietary advice for breakfast consumption justified? Results from a short-term dietary and metabolic experiment in young health men. Br J Nutr 2000; 84: 337–344.
Faul F, Erdfelder E, Buchner A, Lang A-G . Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav Res Method 2009; 4: 1149–1160.
Food Standards Agency Food Standards Agency Survey of Caffeine Levels in Hot Beverages. Information sheet 53/04, HMSO: London, 2004.
Weir JB . New methods for calculating metabolic rate with special references to protein metabolism. J Physiol 1949; 109: 1–9.
Reed GW, Hill JO . Measuring the thermic effect of food. Am J Clin Nutr 1996; 63: 164–169.
Allison DB, Paultre F, Maggio C, Mezzitis N, Pi-Sunyer FX . The use of areas under curves in diabetes research. Diabetes Care 1995; 18: 245–250.
Matthews D, Hosker J, Rudenski A, Naylor B, Treacher D, Turner R . Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985; 28: 412–419.
Stubbs RJ, Hughes DS, Johnston AM, Rowley E, Reid C, Elia M et al. The use of visual analogue scales to assess motivation to eat in human subjects: a review of their reliability and validity with an evaluation of new hand held computerised systems for temporal tracking of appetite ratings. Br J Nutr 2000; 84: 405–415.
Fisher RA . Statistical Methods for Research Workers. Oliver and Boyd Pub: London, UK, 1950.
Lew MJ . Bad statistical practice in pharmacology (and other basic biomedical disciplines): you probably don’t know P. Br J Pharmacol 2012; 166: 1559–1567.
Tudor-Locke C . A preliminary study to determine instrument responsiveness to change with a walking program: Physical activity logs versus pedometers. Res Q Exerc Sport 2001; 72: 288–292.
Betts JA, Richardson JD, Chowdhury EA, Holman GD, Tsintzas K, Thompson D . The causal role of breakfast in energy balance and health: a randomized controlled trial in lean adults. Am J Clin Nutr 2014; 100: 539–547.
Jequier E, Schutz Y . Long term measurements of energy expenditure in humans using a respiration chamber. Am J Clin Nutr 1983; 38: 989–998.
de Jonge L, Bray GA . The thermic effect of food and obesity: a critical review. Obes Res 1997; 5: 622–631.
Edholm OG, Fletcher JG, Widdowson EM, McCance RA . The energy expenditure and food intake of individual men. Br J Nutr 1955; 9: 286–300.
Carey DG, Jenkins AB, Campbell LV, Freund J, Chisholm DJ . Abdominal fat and insulin resistance in normal and overweight women: direct measurements reveal a strong relationship in subjects at both low and high risk of NIDDM. Diabetes 1996; 4: 633–638.
Haus E, Smolensky M . Biological clocks and shift work: circadian dysregulation and potential long term effects. Cancer Cause Control 2006; 17: 489–500.
Havel PJ, Kasim-Karakas S, Mueller W, Johnson PR, Gingerion RL, Stent JS . Relationship of plasma leptin to plasma insulin and adiposity in normal weight and overweight women: effects of dietary fat content and sustained weight loss. J Clin Endocrinol Metab 1996; 81: 4406–4413.
Schoeller DA, Cella LK, Sinha MK, Caro JF . Entrainment of the diurnal rhythm of plasma leptin to meal timing. J Clin Invest 1997; 100: 1882–1887.
Blom WAM, Stafleu A, de Graaf C, Kok FJ, Schaafsma G, Henriks HFJ . Ghrelin response to carbohydrate-enriched breakfast is related to Insulin. Am J Clin Nutr 2005; 1: 367–375.
Astrup A, Toubro S, Cannon S, Hein P, Madsen J . Thermogenic synergism between ephedrine and caffeine in healthy volunteers: a double-blind, placebo-controlled study. Metabolism 1991; 40: 323–329.
Kaneyoshi I, Miyasita A, Inugami M, Fukuda K, Yamazaki K, Yo M . Differences in the time or frequency of meals, alcohol and caffeine ingestion and smoking found between morning and evening types. Psych Rep 2014; 57: 391–396.
Boschloo A, Ouwehand C, Dekker S, Lee N, de Groot R, Krabbendam L, Jolles J . The relationship between breakfast skipping and school performance in adolescents. Mind Brain Educ 2012; 6: 81–88.
Reeves S, McMeel Y, Halsey L, Huber J . Breakfast habits, beliefs and measures of health and wellbeing in a nationally representative UK sample. Appetite 2013; 3: 51–57.
de la Hunty A, Ashwell M . Are people who regularly eat breakfast cereals slimmer than those who don’t? A systematic review of the evidence. Nutr Bull 2007; 32: 118–128.
Garaulet M, Gomez-Abellan P, Alburerque-Bejar JJ, Lee YC, Orddovas JM, Scheer FAJL . Timing of food intake predicts weight loss effectiveness. Int J Obes 2013; 37: 604–611.
Goldstone AP, Prechtl de Hernandez CG, Beaver JD, Muhammed K, Croese C, Bell G et al. Fasting biases brain reward systems towards high-calorie foods. Eur J Neurosci 2009; 30: 1625–1635.
Ruxton CHS, Kirk RT . Breakfast: a review of associations with measures of dietary intake, physiology and biochemistry. Br J Nutr 1997; 78: 199–213.
Jarvandi S, Yan Y, Schootman M . Income disparity and risk of death: the importance of health behaviours and other mediating factors. PLoS ONE 2012; 7: e49929.
Acknowledgements
This study was supported by Kellogg’s Company who funded the project and discussed initial ideas that helped inform the design. They were not involved in data collection, analysis or interpretation. We are grateful to Leigh Gibson who allowed us to use his caffeine questionnaire and all the volunteers who participated in this study. Trial registered with the ISRCTN, trial number ISRCTN89657927 (http://www.controlled-trials.com/ISRCTN89657927/). Ethical clearance for the study was granted by the University of Roehampton Ethics Committee (Ref: LSC 11/010).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Author Contributions
JH, LH and SR contributed to study design; LH, JH, SR and TS contributed to study coordination; TS, LH, JH, SR, MVM and JE contributed to data collection; TS contributed to supervision of data collection; TS and JH contributed to data analyses, SR contributed to drafting of manuscript; all authors contributed to input on data and manuscript.
Rights and permissions
About this article

Cite this article
Reeves, S., Huber, J., Halsey, L. et al. A cross-over experiment to investigate possible mechanisms for lower BMIs in people who habitually eat breakfast. Eur J Clin Nutr 69, 632–637 (2015). https://doi.org/10.1038/ejcn.2014.269
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejcn.2014.269
- Springer Nature Limited