
Abstract
Relapse remains the most common cause of treatment failure in patients receiving autologous stem cell transplantation (ASCT) for follicular lymphoma (FL). The aim of this study was to evaluate the effect of adding radioimmunotherapy or rituximab (R) to BEAM (carmustine, etoposide, ara-c, melphalan) high-dose therapy for ASCT in patients with relapsed FL. Using the European Society for Blood and Marrow Transplantation registry, we conducted a cohort comparison of BEAM (n=1973), Zevalin-BEAM (Z-BEAM) (n=207) and R-BEAM (n=179) and also a matched-cohort analysis of BEAM vs Z-BEAM including 282 and 154 patients, respectively. BEAM, Z-BEAM and R-BEAM groups were well balanced for age, time from diagnosis to ASCT and disease status at ASCT. The cumulative incidences of relapse (IR) at 2 years were 34, 34 and 32% for Z-BEAM, R-BEAM and BEAM, respectively. By multivariate analysis, there were no significant differences with Z-BEAM or R-BEAM compared with BEAM for IR, non-relapse mortality, event-free survival or overall survival. With the caveat that the limitations of registry analyses have to be taken into account, this study does not support adding radioimmunotherapy or R to BEAM in ASCT for relapsed FL. However, we cannot rule out the existence a particular subset of patients who could benefit from Z-BEAM conditioning that cannot be identified in our series, and this should be tested in a randomized trial.
Similar content being viewed by others

Introduction
High-dose therapy (HDT) followed by autologous stem cell transplantation (ASCT) is considered to be a standard treatment for eligible patients with relapsed chemosensitive follicular lymphoma (FL).1 However, disease recurrence remains the most common cause of treatment failure after ASCT. As FL is highly sensitive to radiotherapy, TBI has been traditionally used as part of high-dose regimens for ASCT and has been associated with lower relapse rates,2, 3 although this has been outweighed in some studies by a higher long-term toxicity.3, 4 Other strategies have been used to reduce relapse rates, including the use of post-transplant immunotherapy with rituximab (R).5
Radioimmunotherapy (RIT) has been explored as a means of harnessing the antitumour effects of radiation while potentially reducing toxicity compared with fractionated TBI. It combines the potency of radiotherapy with the targeting capability and immunological potency of cell-type-specific monoclonal antibodies. The use of targeted antibodies to deliver radiation directly to the tumour and its microenvironment is intended to spare critical organs, thereby allowing treatment of older and more heavily pretreated patients. Hence, there is a strong rationale for using RIT as part of the conditioning treatment for ASCT. Two different radiolabelled anti-CD20 antibodies have been used in this setting to treat B-cell lymphomas: iodine-131 (I131)-tositumomab (Bexxar)6, 7 and yttrium-90 (Y90)-ibritumomab tiuxetan (Zevalin).8
Augmenting the high-dose regimen for ASCT with RIT has been evaluated in patients with B-cell non-Hodgkin lymphoma (NHL) in several studies.9, 10, 11, 12 Although RIT is approved for treatment of FL, however, there are no studies analysing the role of RIT-ASCT specifically in patients with FL. Here we report a registry analysis of the effect of adding Y90-ibritumomab tiuxetan (Z) or R to BEAM (carmustine, etoposide, ara-c, melphalan) HDT for ASCT in patients with relapsed FL.
Patients and methods
Data source
The European Society for Blood and Marrow Transplantation (EBMT) is a voluntary organization consisting of >600 transplant centres mainly from Europe. Accreditation as a member centre requires submission of minimal essential data (MED-A form) from all consecutive patients to a central registry in which patients may be identified by the diagnosis of underlying disease and type of transplantation. MED-A data are updated annually. Informed consent for transplantation and data collection was obtained locally according to regulations applicable at the time of transplantation. Since 1 January 2003, all transplant centres have been required to obtain written informed consent before data registration with the EBMT following the Helsinki Declaration 1975.
Patient eligibility
Eligible for this registry study were patients with FL aged ⩾18 years who underwent a first ASCT after BEAM HDT with or without Z (Z-BEAM) or R (R-BEAM) from 2004 to 2012 and were registered with the EBMT with a full data set as required for this analysis. Patients who had received other drugs in addition to BEAM were not eligible. Patients with histological transformation, those undergoing a second transplant and patients in first CR or PR were excluded.
Disease status categorization
For the purposes of this analysis, any CR or PR were considered as sensitive disease, while primary refractory disease, chemoresistant and untreated relapse, stable disease and progressive disease were grouped together as active disease.
Outcome measures
Overall survival (OS) was defined as the time from ASCT to death from any cause, and surviving patients were censored at last follow-up. Event-free survival (EFS) was defined as time from ASCT to recurrence, progressive disease or death from any cause. Non-relapse mortality (NRM) was defined as death from any cause without progression. Incidence of relapse (IR) was defined as the time from ASCT to relapse or progression (taking into account NRM as competing risk).
Statistical analysis
Patient characteristics were compared with t-test for continuous variables and χ2 or Fisher’s exact test for categorical variables. The primary end point was IR and secondary end points included OS, EFS, NRM and time to engraftment. OS and EFS were determined using the Kaplan–Meier method, and curves were compared by log-rank test. IR and NRM were calculated by cumulative incidence curves to account for competing risks and compared by Gray's test. For analysing the effect of Z and R, respectively, as supplement to BEAM, multivariate comparisons adjusting for potential confounders were performed with the whole patient sample. Multivariate analyses of OS and EFS were carried out using Cox regression modelling stratified for variables not respecting the proportional hazard assumption. Multivariate analyses of IR and NRM were carried out using Fine and Gray regression models. Variables included in multivariate models were significant at the 0.2 level in univariate or unbalanced between the groups under study or known to have an impact on outcome studied.
In addition, a matched-cohort comparison of BEAM vs Z-BEAM (2:1 ratio) was performed. In situations where more than two BEAM patients were identified as potential matches for a Z-BEAM patient, the best-matched patients were selected. The variables used for matching were age, time from diagnosis to transplant, gender, performance status, year of transplant and disease status at ASCT. In the matched sample, outcome in BEAM vs Z-BEAM cohorts were compared using a Cox model stratified on matched pairs.
All P-values <0.05 were considered significant. All statistical analyses were carried out using R 2.15.3 (R Foundation for Statistical Computing, Vienna, Austria, http://www.R-project.org).
Results
BEAM vs Z-BEAM vs R-BEAM comparison
Altogether, 2359 patients who received either BEAM (n=1973), Z-BEAM (n=207) or R-BEAM (R-BEAM, n=179) were eligible, see Supplementary Table S1. Patient characteristics were well balanced among the three groups except that Z-BEAM patients tended to contain more male patients, a higher proportion of patients with a reduced performance score and to be preferentially transplanted between 2007 and 2009, Table 1.
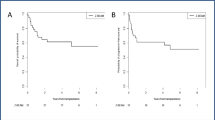
The cumulative IR at 2 years for the whole series was 32% with no differences according to high-dose regimen (P=NS, univariate with 32% for the BEAM group, 32% for the R-BEAM group and 34% for the Z-BEAM group). With similar 12-month NRM figures of 3% in each of the three groups, 2-year EFS and OS after BEAM vs Z-BEAM vs R-BEAM were 63% vs 62% vs 63% (P=0.978) and 82% vs 86% vs 88% (P=0.463), respectively (Figure 1). By multivariate analysis, there were no significant differences in NRM in the Z-BEAM group (hazard ratio (HR): 0.88 (95% confidence interval (CI): 0.4–1.94); P=0.74) and in the R-BEAM cohort (HR: 1.24 (95% CI: 0.57–2.72); P=0.59) compared with BEAM. The same accounted for IR, with an HR=1.02 ((95% CI: 0.78–1.33); P=0.89) for patients treated with Z-BEAM and HR=0.92 ((95% CI: 0.68–1.23); P=0.58) for patients who received R-BEAM. Similarly, no significant differences between the BEAM and the Z-BEAM or R-BEAM cohorts were found for OS (HR=0.93 (95% CI: 0.64–1.35); P=0.71 and HR=0.78 (95% CI: 0.51–1.2); P=0.26) and for EFS (HR=0.93 (95% CI: 0.71–1.23); P=0.63 and HR=1.1 (95% CI: 0.84–1.41); P=0.51). In contrast, a long interval between diagnosis and ASCT (⩾2 years) and sensitive disease status at ASCT predicted both favourable IR (HR=0.67 (95% CI: 0.57–0.79); P<0.0001 and HR=0.38 (95% CI: 0.31–0.48); P<0.0001) and OS (HR=0.76 (95% CI: 0.61–0.95); P=0.016 and HR=0.41 (95% CI: 0.31–0.55); P<0.0001) but had no significant impact on NRM (HR=1.1 (95% CI: 0.62–1.79); P=0.84 and HR=1.18 (95% CI: 0.47–2.95); P=0.73). In addition, the Eastern Cooperative Oncology Group performance status was an independent variable of OS (HR=0.4 (95% CI: 0.27–0.7); P=0.006).

Survival analysis in total cohort. (a) OS; (b) EFS.
Matched cohort comparison
Altogether, there were 154 Z-BEAM patients who could be matched with 2 (n=128) or 1 (n=26) BEAM recipients, resulting in a total sample size of 436 patients (282 patients treated with BEAM and 154 patients who received Z-BEAM). Their characteristics are described in Table 2.
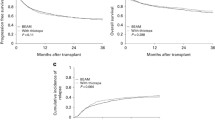
Ninety-seven percent and 98% of the BEAM and Z-BEAM patients respectively engrafted. The median time to engraftment was similar in both groups (11 days (range: 5–29) in patients treated with BEAM and 11 days (range: 7–47) in the Z-BEAM group). NRM in the BEAM and Z-BEAM cohorts was 2% and 0.7% on day +100, 2.4% and 0.7% at 1 year and 9% and 8% at 5 years, respectively (HR: 0.5 (95% CI: 0.13–1.93); P=0.3; Figure 2). Similarly, there were no significant differences in the risk of secondary malignancies for both groups, including AML/myelodysplastic syndrome (MDS), NHL and solid tumours. Seven patients (2.5%) in the BEAM group and 4 (2.5%) in the Z-BEAM group developed secondary malignancies.

Survival analysis in the matched cohorts. (a) NRM; (b) cumulative incidence of relapse; (c) EFS; (d) OS.
With a median follow-up of 19 months for survivors (range: 1–86), 25% of patients in the BEAM group relapsed, in comparison to 34% in the Z-BEAM cohort. This translated into an increased IR after Z-BEAM compared with BEAM that was, however, not statistically significant (HR=1.55 (95% CI: 0.96–2.51); P=0.07). Similarly, no significant differences between the BEAM and Z-BEAM groups were found in EFS (HR=1.34 (95% CI: 0.86–2.08); P=0.2) nor in OS (HR=0.77 (95% CI: 0.41–1.46); P=0.43) (Figure 2). We analysed the subgroup of patients who were in PR at the time of ASCT to assess whether Z-BEAM would result in a greater benefit in this subgroup. Patients who received BEAM had a significantly higher NRM (P=0.02), but there were no differences in any of the other outcomes (Figures 3 and 4).

Survival of patients in CR prior to ASCT in the matched cohort. (a) NRM; (b) cumulative incidence of relapse; (c) EFS; (d) OS. A full color version of this figure is available at the Bone Marrow Transplantation journal online.

Survival of patients in PR prior to ASCT in the matched cohort. (a) NRM; (b) cumulative incidence of relapse; (c) EFS; (d) OS. A full color version of this figure is available at the Bone Marrow Transplantation journal online.
Discussion
Despite the increasing efficacy of first-line treatment in FL and the advent of targeted drugs for the salvage setting, ASCT remains a standard treatment option for the relapse setting, in particular in patients with short-lived remissions.1, 13 Although a substantial proportion of patients might enjoy remissions lasting ⩾10 years after ASCT,2, 3, 4, 5 relapse represents the main cause of treatment failure. To this end, the radio-sensitivity of FL makes the use of RIT as part of the high-dose regimen for ASCT a very attractive option to increase disease control while avoiding the potential long-term complications of TBI. Apart from Zevalin, other RIT, such as 90Y-labelled anti-CD22 (epratuzumab) combined with a humanized antibody anti-CD20 (veltuzumab), could be used as a part of HDT.14 The feasibility of combining RIT with BEAM or other chemotherapy-based conditioning regimens has been explored in a number of phase I–II studies in patients with NHL, demonstrating its safety8, 15, 16, 17 and efficacy.16, 17 These studies, mostly in patients with aggressive lymphoma or with a mixture of different histological subtypes were limited by small patient numbers and lack of comparators.8, 15 A small randomized trial compared the outcomes of ASCT for relapsed/refractory aggressive B-cell lymphoma with or without Z as an adjunct to BEAM.18 However, there have been no randomized studies analysing the role of RIT-BEAM specifically in patients with relapsed FL. The present study is the largest study comparing BEAM vs RIT-BEAM and the first one specifically in FL.
The hypothesis that Z-BEAM would result in better disease control reducing the relapse rate was not confirmed. As R-based chemoimmunotherapy has represented the standard for first-line treatment for FL since the early 2000s19 and many of the patients in need for ASCT will have received R maintenance as well,20 one explanation for the lack of effect of CD20-based (radio-)immunotherapy as adjunct to HDT as observed here might be that patients with relapsed/refractory FL proceeding to ASCT are very likely to be heavily preexposed to CD20-directed treatment. Another explanation for the lack of efficacy could be the hypothetical use of standard doses of Zevalin instead of a dose escalation for the conditioning regimen. Unfortunately, we do not have the doses of Zevalin administered to confirm or refute this hypothesis. Notwithstanding the fact that even in R-naive patients in vivo purging with R prior to ASCT had no significant effect on disease control in a large randomized trial in relapsed FL.5
Similarly, no significant differences were found in NRM. The increased use of RIT in the management of patients with indolent lymphomas raised concerns about the risks associated with this therapy, including the risk of developing MDS/AML.21, 22 Z-BEAM has been demonstrated to be well tolerated in the initial phase I/II studies.11, 15 A randomized study in aggressive lymphoma confirmed the previously reported observations that the addition of Z to high-dose BEAM is safe and not associated with excess toxicity. Although there was a trend for more mucositis and more serious infections in the Z-BEAM arm, all the toxicities were reversible with no early deaths.18 Also, median engraftment times in the initial trials are similar to conventional high-dose regimens as it has been confirmed in our study. The risk of AML/MDS after RIT was reported to be low21 and no cytogenetic abnormalities after RIT and ASCT were reported.23 In our series, there were no differences in the risk of secondary malignancies (including AML/MDS, NHL and solid tumours), although the follow-up of the series is not long enough to draw any conclusions in this regard.
However, this study has some limitations that are inherent to a registry study. For instance, there are some missing data with potential prognostic importance, such as the number of treatment lines, the fraction of patients with R-refractory disease pre-ASCT or the indication for using RIT-BEAM by the treating physician. The number of treatment lines was not mandatory in the MED-A forms until recently so the time from diagnosis to transplant was used as a surrogate for the matched analysis. Whereas it is clear that they are not equivalent, the fact that patients in first response were excluded from the study suggests that a short time from diagnosis to transplant is a poor risk factor. Thus, with these caveats in mind, our study demonstrates that Z-BEAM is a safe regimen, but we have not been able to demonstrate that it is more efficacious than BEAM.
In conclusion, although it is not excluded that Z-BEAM might be superior to BEAM despite the results presented here, this study is clearly not an argument in favour of pursuing this approach. Instead, further improvement of ASCT outcome in FL may be achieved by CD20 antibody maintenance, as recently shown in a large randomized trial,5 or by other post-transplant interventions, which could also include RIT.
References
Montoto S, Corradini P, Dreyling M, Ghielmini M, Kimby E, López-Guillermo A et al. Indications for hematopoietic stem cell transplantation in patients with follicular lymphoma: a consensus project of the EBMT-Lymphoma Working Party. Haematologica 2013; 98: 1014–1021.
El-Najjar I, Boumendil A, Luan JJ, Bouabdallah R, Thomson K, Mohty M et al. The impact of total body irradiation on the outcome of patients with follicular lymphoma treated with autologous stem-cell transplantation in the modern era: a retrospective study of the EBMT Lymphoma Working Party. Ann Oncol 2014; 25: 2224–2229.
Montoto S, Canals C, Rohatiner AZS, Taghipour G, Sureda A, Schmitz N et al. Long-term follow-up of high-dose treatment with autologous haematopoietic progenitor cell support in 693 patients with follicular lymphoma: an EBMT registry study. Leukemia 2007; 21: 2324–2331.
Rohatiner AZS, Nadler L, Davies AJ, Apostolidis J, Neuberg D, Matthews J et al. Myeloablative therapy with autologous bone marrow transplantation for follicular lymphoma at the time of second or subsequent remission: long-term follow-up. J Clin Oncol 2007; 25: 2554–2559.
Pettengell R, Schmitz N, Gisselbrecht C, Smith G, Patton WN, Metzner B et al. Rituximab purging and/or maintenance in patients undergoing autologous transplantation for relapsed follicular lymphoma: a prospective randomized trial from the lymphoma working party of the European group for blood and marrow transplantation. J Clin Oncol 2013; 31: 1624–1630.
Vose JM, Carter S, Burns LJ, Ayala E, Press OW, Moskowitz CH et al. Phase III randomized study of rituximab/carmustine, etoposide, cytarabine, and melphalan (BEAM) compared with iodine-131 tositumomab/BEAM with autologous hematopoietic cell transplantation for relapsed diffuse large B-cell lymphoma: results from the BMT C. J Clin Oncol 2013; 31: 1662–1668.
Gopal AK, Gooley TA, Maloney DG, Petersdorf SH, Eary JF, Rajendran JG et al. High-dose radioimmunotherapy versus conventional high-dose therapy and autologous hematopoietic stem cell transplantation for relapsed follicular non-Hodgkin lymphoma: a multivariable cohort analysis. Blood 2003; 102: 2351–2357.
Winter JN, Inwards DJ, Spies S, Wiseman G, Patton D, Erwin W et al. Yttrium-90 ibritumomab tiuxetan doses calculated to deliver up to 15Gy to critical organs may be safely combined with high-dose BEAM and autologous transplantation in relapsed or refractory B-cell non-Hodgkin’s lymphoma. J Clin Oncol 2009; 27: 1653–1659.
Dreyling M, Trümper L, von Schilling C, Rummel M, Holtkamp U, Waldmann A et al. Results of a national consensus workshop: therapeutic algorithm in patients with follicular lymphoma—role of radioimmunotherapy. Ann Hematol 2007; 86: 81–87.
Witzig TE, Fishkin P, Gordon LI, Gregory SA, Jacobs S, Macklis R et al. Treatment recommendations for radioimmunotherapy in follicular lymphoma: a consensus conference report. Leuk Lymphoma 2011; 52: 1188–1199.
Decaudin D, Mounier N, Tilly H, Ribrag V, Ghesquières H, Bouabdallah K et al. (90)Y ibritumomab tiuxetan (Zevalin) combined with BEAM (Z -BEAM) conditioning regimen plus autologous stem cell transplantation in relapsed or refractory low-grade CD20-positive B-cell lymphoma. A GELA phase II prospective study. Clin Lymphoma Myeloma Leuk 2011; 11: 212–218.
Gisselbrecht C, Vose J, Nademanee A, Gianni AM, Nagler A . Radioimmunotherapy for stem cell transplantation in non-Hodgkin’s lymphoma: in pursuit of a complete response. Oncologist 2009; 14 (Suppl 2): 41–51.
Dreyling M, Ghielmini M, Rule S, Salles G, Vitolo U, Ladetto M et al. Newly diagnosed and relapsed follicular lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2016; 27: v83–v90.
Morschhauser F, Kraeber-Bodéré F, Wegener WA, Harousseau JL, Petillon MO, Huglo D et al. High rates of durable responses with anti-CD22 fractionated radioimmunotherapy: results of a multicenter phase I/II study in non-Hodgkin's lymphoma. J Clin Oncol 2010; 28: 3709–3716.
Krishnan A, Nademanee A, Fung HC, Raubitschek AA, Molina A, Yamauchi D et al. Phase II trial of a transplantation regimen of yttrium-90 ibritumomab tiuxetan and high-dose chemotherapy in patients with non-Hodgkin’s lymphoma. J Clin Oncol 2008; 26: 90–95.
Nademanee A, Forman S, Molina A, Fung H, Smith D, Dagis A et al. A phase 1/2 trial of high-dose yttrium-90-ibritumomab tiuxetan in combination with high-dose etoposide and cyclophosphamide followed by autologous stem cell transplantation in patients with poor-risk or relapsed non-Hodgkin lymphoma. Blood 2005; 106: 2896–2902.
Shimoni A, Zwas ST, Oksman Y, Hardan I, Shem-Tov N, Yerushalmi R et al. Yttrium-90-ibritumomab tiuxetan (Zevalin) combined with high-dose BEAM chemotherapy and autologous stem cell transplantation for chemo-refractory aggressive non-Hodgkin’s lymphoma. Exp Hematol 2007; 35: 534–540.
Shimoni A, Avivi I, Rowe JM, Yeshurun M, Levi I, Or R et al. A randomized study comparing yttrium-90 ibritumomab tiuxetan (Zevalin) and high-dose BEAM chemotherapy versus BEAM alone as the conditioning regimen before autologous stem cell transplantation in patients with aggressive lymphoma. Cancer 2012; 118: 4706–4714.
Ghielmini M, Vitolo U, Kimby E, Montoto S, Walewski J, Pfreundschuh M et al. ESMO Guidelines consensus conference on malignant lymphoma 2011 part 1: diffuse large B-cell lymphoma (DLBCL), follicular lymphoma (FL) and chronic lymphocytic leukemia (CLL). Ann Oncol 2013; 24: 561–576.
Salles G, Seymour JF, Offner F, López-Guillermo A, Belada D, Xerri L et al. Rituximab maintenance for 2 years in patients with high tumour burden follicular lymphoma responding to rituximab plus chemotherapy (PRIMA): a phase 3, randomised controlled trial. Lancet 2011; 377: 42–51.
Czuczman MS, Emmanouilides C, Darif M, Witzig TE, Gordon LI, Revell S et al. Treatment-related myelodysplastic syndrome and acute myelogenous leukemia in patients treated with ibritumomab tiuxetan radioimmunotherapy. J Clin Oncol 2007; 25: 4285–4292.
Bennett JM, Kaminski MS, Leonard JP, Vose JM, Zelenetz AD, Knox SJ et al. Assessment of treatment-related myelodysplastic syndromes and acute myeloid leukemia in patients with non-Hodgkin lymphoma treated with tositumomab and iodine I131 tositumomab. Blood 2005; 105: 4576–4582.
Devizzi L, Guidetti A, Tarella C, Magni M, Matteucci P, Seregni E et al. High-dose yttrium-90-ibritumomab tiuxetan with tandem stem-cell reinfusion: an outpatient preparative regimen for autologous hematopoietic cell transplantation. J Clin Oncol 2008; 26: 5175–5182.
Acknowledgements
This study was funded by an unrestricted grant from Sepropharm, Munich, Germany.
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Partially presented in abstract form at the 41st Annual Meeting of the European Society for Blood and Marrow Transplantation on the 23 March 2014 and as an oral presentation in 13th International Conference on Malignant Lymphoma on the 17 June 2015.
Supplementary Information accompanies this paper on Bone Marrow Transplantation website
Supplementary information
Rights and permissions
About this article

Cite this article
Bento, L., Boumendil, A., Finel, H. et al. Radioimmunotherapy-augmented BEAM chemotherapy vs BEAM alone as the high-dose regimen for autologous stem cell transplantation (ASCT) in relapsed follicular lymphoma (FL): a retrospective study of the EBMT Lymphoma Working Party. Bone Marrow Transplant 52, 1120–1125 (2017). https://doi.org/10.1038/bmt.2017.88
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bmt.2017.88
- Springer Nature Limited
This article is cited by
-
The role of stem cell transplantation in the management of relapsed follicular lymphoma in the era of targeted therapies
Bone Marrow Transplantation (2019)
-
Strategies to improve outcomes of autologous hematopoietic cell transplant in lymphoma
Bone Marrow Transplantation (2019)