
Abstract
Purpose
Waiting is a common experience for patients during an emergency department (ED) visit. While high acuity patients are seen with little delay, low acuity patients may experience dissatisfaction from prolonged wait times. One strategy to improve patient experience involves changing the perception of the wait by providing realistic expectations of wait times using public-facing wait time displays. The primary objective of this study is to quantify the number of Canadian EDs with online wait time displays and describe the features and type of information provided.
Methods
A systematic online search of all Canadian EDs was completed to identify EDs with public-facing wait time displays. A scoping review was then performed to assess their message characteristics, translations offered, availability of multi-site information, and accessibility features. Data were summarized using descriptive statistics.
Results
Sixty (9.3%) of the 647 Canadian EDs identified provide public-facing real-time wait time displays. Thirteen of these (21.7%) were associated with a single proprietary system. Distribution of wait time displays differs across Canada, with a range of zero to 100% of EDs within each province utilizing this communication tool. Common characteristics include “average” wait time (95%), graphical trend data (32%), number of patients waiting (33%), longest wait time (12%), and expected length of stay (10%). Sixty-two percent of wait time displays provide a combination of these methods to inform wait times. Important accessibility features include language translation, compliance with Canadian National Institute for the Blind (CNIB) accessibility guidelines and availability on a mobile application.
Conclusion
Currently, there is emerging use of wait time displays in Canada with considerable variability in the information communicated through these tools. Effectiveness of these displays and their content needs to be determined.
Résumé
Objectif
L'attente est une expérience courante pour les patients lors d'une visite au service des urgences (SU). Alors que les patients avec un niveau d'acuité élevé sont vus dans les plus brefs délais, les patients à faible degré d'acuité peuvent éprouver de l’insatisfaction à cause des temps d’attente prolongés. Une stratégie visant à améliorer l'expérience des patients consiste à modifier la perception de l'attente en fournissant des attentes réalistes en matière de temps d'attente au moyen d'affichages de temps d'attente destinés au public. L'objectif principal de la présente étude est de quantifier le nombre de services d'urgence canadiens qui affichent les temps d'attente en ligne et de décrire les caractéristiques et le type d'information fournie.
Méthodes
Une recherche systématique en ligne de tous les services d'urgence canadiens a été effectuée afin d'identifier les services d'urgence qui affichent les temps d'attente à l'intention du public. Un examen de la portée a ensuite été effectué pour évaluer les caractéristiques de leurs messages, les traductions offertes, la disponibilité d'informations multisites et les caractéristiques d'accessibilité. Les données ont été résumées à l'aide de statistiques descriptives.
Résultats
Soixante (9,3 %) des 647 urgences canadiennes recensées offrent au public un affichage en temps réel des temps d'attente. Treize d'entre eux (21,7 %) étaient associés à un seul système propriétaire. La répartition des affichages sur les temps d’attente varie d’un bout à l’autre du Canada, avec une fourchette de zéro à 100 % des services d'urgence dans chaque province utilisant cet outil de communication. Les caractéristiques communes comprennent le temps d'attente « moyen » (95 %), les données de tendance graphique (32 %), le nombre de patients en attente (33 %), le temps d'attente le plus long (12 %) et la durée prévue du séjour (10 %). Soixante-deux pour cent des affichages des temps d'attente fournissent une combinaison de ces méthodes pour informer les temps d'attente. Les fonctionnalités d'accessibilité importantes incluent la traduction linguistique, la conformité aux directives d'accessibilité de l'Institut national canadien pour les aveugles (INCA) et la disponibilité sur une application mobile.
Conclusion
À l’heure actuelle, l’utilisation des présentoirs sur les temps d’attente au Canada est de plus en plus répandue, et l’information communiquée au moyen de ces outils varie considérablement. L'efficacité de ces affichages et de leur contenu doit être déterminée.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
What is known about the topic? |
Emergency departments are informing patients about queues using online public-facing wait time as wait time is associated with patient satisfaction. |
What did this study ask? |
We sought to determine the current state of the use of public-facing wait time display tools across Canadian emergency departments. |
What did this study find? |
9.3% of emergency departments in Canada provide wait time information to patients via wait time display tools with variable features. |
Why does this study matter to clinicians? |
Effective implementation of wait time display tools could improve patient perception and satisfaction with waiting for emergency department services. |
Introduction
Waiting is a common experience for patients seeking care in the emergency department (ED). While high acuity patients are seen with little delay, low acuity patients may experience prolonged wait times. Patients who are “fed up with waiting” are more likely to leave without being seen [1], with resultant potential for adverse outcomes and delays in treatment.
Patient satisfaction and experience improves if the actual wait time can be reduced, however when resource constraints prohibit this, an alternate strategy involves changing the perceptions and expectations of the wait. The Satisfied Patients Exiting the Emergency Department (SPEED) study conducted by Hedges et al. [2], indicated that improvements of patients’ satisfaction in the ED should focus on patients’ perceptions of the wait rather than reducing the absolute time spent waiting. Wait time displays are public-facing communication tools providing estimated wait time information to patients prior to entering the ED to access medical care. The scope of the utility, quality, and effectiveness of wait time displays have not previously been determined.
We performed a scoping review to quantify the number of Canadian EDs with public-facing online wait time displays and describe the features and type of information they provide.
Methods
Study design
A scoping review (Appendix A) was conducted using an established five-stage framework [3]. EDs were defined as any centre providing acute medical care 24 h/day, 7 days/week. Urgent care centres providing acute care but not available 24/7 were excluded. Wait time displays were collected from all provinces across Canada between June, 2020 and August, 2020.
Data collection
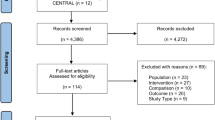
We conducted a web-based search of provincial health directories using the Google search engine to identify all EDs in each province. A manual search of each hospital for an existing wait time display was done by searching “[hospital name] wait time” to simulate how the general population would search for information about wait times at their nearby ED. If no wait time displays were identified, the search was broadened using “[hospital name] emergency department wait time”, and “[hospital name] emergency department”. Any relevant web page, with any basic information on the ED, was then screened for wait time information.
Wait time information needs to be regularly updated to qualify as real time. EDs were categorized into four categories; “no ED webpage”, “ED webpage with no information on wait times”, “ED webpage with static information concerning wait times”, or “ED webpage with real-time wait time information”. The last category equates to the identified wait time displays for this review and is the primary focus for analysis.
Data extraction and analysis
Identified public-facing wait time displays were reviewed. Wait time displays were characterized based on the type of information provided, and accessibility features as per the Canadian National Institute for the Blind’s (CNIB) Clear Print Accessibility Guidelines [4]. Information extracted was recorded on a standardized data form (Table 1). Data were summarized using descriptive statistics.
Results
Across Canada, 647 EDs were identified, of which 60 were found to have wait time displays. Six provinces employed wait time displays (PEI (100%), Ontario (12.7%), Alberta (20.8%), Saskatchewan (8%), Manitoba (7.4%) and British Columbia (7.6%). Four provinces did not have any ED wait time displays (Quebec, New Brunswick, Nova Scotia, and Newfoundland). None of the territories had wait time displays. There is a disproportionate number (71.7%) of wait time displays deployed in large urban centres (populations > 100 000).
Information characteristics
Of the 60 wait time displays identified, the majority (95%) provided an “average” wait time, while 32% provided a graphical illustration of expected wait times in the next few hours. Twenty-seven percent of wait time displays reported the number of registered patients waiting and the number of patients currently being assessed. Longest wait time (12%) and expected length of stay (10%) were also seen on wait time displays. Sixty-two percent of wait time displays provided a combination of the aforementioned data. A proprietary system is currently being used in 13 of Ontario EDs and communicates wait times using average wait time, patients waiting/being treated, and trend data for the next 6 h. Eighty-five percent of wait time displays were provided through regional sites, reporting the wait times of several local emergency departments on a single webpage.
Accessibility features
Translation services were offered by 57% of the ED wait time tools. English (n = 60), French (n = 34), and other languages (n = 21) were most commonly offered. Some sites offered in-webpage Google Translate services providing translation to 109 languages. Two centres provided translated wait times based on frequently requested languages. In Alberta, wait time tools offered translation to 14 commonly requested languages, while Hamilton translated three.
Most wait time displays (51.6%) in Canada refresh their information every 2 min or less. At the longer end of refresh rates, 20% of wait time displays update their information every 15 min.
Eight-five percent of wait time displays were accessible through mobile device. Thirty-five percent of wait time displays had a functional mobile-specific application, while another 11.7% of wait time displays had poor mobile/smartphone interfaces due inability for the website to open on the mobile device, or inability to read text.
CNIB clear print accessibility guidelines describe optimal font style and size for accessibility purposes. The font style deployed in 100% of wait time displays fit within the guidelines. Four (6.3%) wait time displays were not compliant with the optimal 12–18 size font.
Discussion
Interpretation
This study highlights the features of wait time displays across Canada and suggests that there is variability in how information is provided. To our knowledge, this is the first characterization and quantification of the use of real-time wait time displays tools across Canada.
Lengthy wait times in Canadian EDs remain an obstacle for both physicians and patients. Actual reduction in wait times requires additional staff, resources, and infrastructure. Alternative methods to improve the wait time experience provides a more amenable solution. Managing wait time perceptions and expectations has been shown to improve the patient experience and a web-based wait time displays was the preferred modality to notify patients about wait times prior to arriving in the ED [5]. Conversely, wait time displays can potentially discourage low acuity presentations to the ED when waits are long. This could have the secondary effect of encouraging patients to more appropriately seek care from their primary care provider.
A key component of this study was to assess accessibility features in wait time display tools. EDs are utilized by a diverse population, therefore information and tools need to be accessible. A scoping review identified language as the most common barrier to healthcare for immigrant populations in Canada [6]. Prioritizing languages commonly spoken in the community or making available universal language translation tools facilitates provision of wait time information to the community at large is key to removing barriers to access. Mobile applications are the second most preferred modality for accessing wait time information [5]. As highlighted in this study, only a small proportion of wait time displays are optimized for mobile use, so there is opportunity for improvement in digital access. Finally, presentation of wait time information needs to follow the CNIB clear print guidelines. Wait time display compatibility with voiceover software and accessibility for persons with other types of disability should be explored.
Previous studies
Wait time displays in Canada have a variety of different features. Although they all communicate wait time information, the presentation of this information is not standardized. To date, what information is important and how public-facing wait time displays should convey this information is unknown.
There have been concerns about the use of wait time displays. The first concern speaks to the accuracy of estimated wait time information. Published wait times may not represent the actual time spent in the waiting room due to flow confounders in larger volume EDs (5000 patients per month) [7]. Another concern suggests that wait time displays may encourage patients to self-triage or not seek timely care [8] resulting in increasing morbidity. While a study at two academic EDs highlighted that 44% of survey participants would choose the ED with a shorter wait time, there was no indication that wait time information would deter patients from presenting to the ED [9]. The use of wait time displays may also be important in addressing “fed up” patients who left the ED without being seen (LWBS). Tools such as wait time displays may help reduce the proportion of patients who LWBS; however, this is yet to be investigated [10].
Strengths and limitations
This study does not assess the effectiveness of wait time displays, nor the local needs for a wait time display. This may be relevant to smaller communities where wait times may not be a significant issue and where options for care are limited. Additionally, the method of our search omits discovery of any wait time displays only accessible inside the ED, which may also have an impact on improving patient experience in waiting rooms.
Implications
Optimizing use of wait time displays for ED care has the potential to divert low acuity presentations, minimize LWBS, and improve the patient experience. Potential development may include third party proprietary vendors that EDs could contract for wait time displays. Further studies to examine the benefits and weaknesses of online wait time displays should engage patients as end users to optimize the application of these digital tools.
Conclusion
There is substantial variability across Canada in the use of wait time displays, the information provided, and accessibility features such as mobile compatibility and translation services. Better application of these digital tools can improve the patient experience when seeking care in the ED.
Availability of data and materials
Requests for access to other data should be addressed to senior author: Kevin Cheung kcheung@cheo.on.ca. All requests will need to specify how the data will be used and will require approval by co-investigators.
Code availability
Not applicable.
References
Rowe BH, Channan P, Bullard M, Blitz S, Saunders LD, Rosychuk RJ, Lari H, Craig WR, Holroyd BR. Characteristics of patients who leave emergency departments without being seen. Acad Emerg Med. 2006;13(8):848–52. https://doi.org/10.1197/j.aem.2006.01.028 (Epub 2006 May 2 PMID: 16670258).
Hedges JR, Trout A, Magnusson AR. Satisfied patients exiting the emergency department (SPEED) study. Acad Emerg Med. 2002;9(1):15–21. https://doi.org/10.1111/j.1553-2712.2002.tb01161.x (PMID: 11772664).
Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010. https://doi.org/10.1186/1748-5908-5-69.
Clear Print Accessibility Guidelines. Canadian National Institute for the Blind (CNIB). 1. https://www.cnib.ca/sites/default/files/2020-08/Clear%20Print%20Guidelines%202020.pdf. Accessed 10 June 2020.
Calder-Sprackman S, Kwok ES, Bradley R, Landreville J, Perry JJ, Calder LA. Availability of emergency department wait times information: a patient-centered needs assessment. Emerg Med Int. 2021;22:2021. https://doi.org/10.1155/2021/8883933.
Kalich A, Heinemann L, Ghahari S. A scoping review of immigrant experience of health care access barriers in Canada. J Immigr Minor Health. 2016;18(3):697–709.
Jouriles N, Simon EL, Griffin P, Williams CJ, Haller NA. Posted emergency department wait times are not always accurate. Acad Emerg Med. 2013;20(4):421–3.
Weiner SG. Advertising emergency department wait times. West J Emerg Med. 2013;14(2):77.
Yip A, McLeod S, McRae A, Xie B. Influence of publicly available online wait time data on emergency department choice in patients with noncritical complaints. Can J Emerg Med. 2012;14(4):237–46.
Monzon J, Friedman S, Clarke C, Arenovich T. Patients who leave the emergency department without being seen by a physician: a control-matched study. Can J Emerg Med. 2005;7(2):107–13. https://doi.org/10.1017/S1481803500013063.
Funding
The work was supported by a summer student research grant from the Children’s Hospital of Eastern Ontario Research Institute.
Author information
Authors and Affiliations
Contributions
Concept and design of the study; RR, KC, and ALC. Acquisition, analysis, and interpretation of data; RR and IB. Manuscript drafting; RR. Critical revision of the manuscript for important intellectual content; ALC, ST, and KC.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Rathagirishnan, R., Birchall, I., Latimer-Cheung, A. et al. About time! A scoping review of public-facing emergency department wait time displays in Canada. Can J Emerg Med 24, 503–508 (2022). https://doi.org/10.1007/s43678-022-00301-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43678-022-00301-4