
Abstract
Background
To analyze and evaluate the clinical outcomes of using high-viscosity bone cement compared to low-viscosity bone cement in percutaneous vertebroplasty (PVP) for treatment of Kummell’s disease.
Methods
From July 2017 to July 2019, 68 Kummell’s disease patients who underwent PVP were chosen and separated into 2 groups: H group (n = 34), were treated with high-viscosity bone cement and L group (n = 34), treated with low-viscosity bone cement during treatment. The operation time, number of fluoroscopy tests done, and amount of bone cement perfusion were recorded for both groups. Clinical outcomes were compared, by measuring their Visual Analog Scale (VAS), Oswestry Disability Index (ODI), Kyphosis Cobb’s angle, vertebral height compression rate, and other complications.
Results
High-viscosity group showed less operation time and reduced number of fluoroscopy tests than the low-viscosity group (P < 0.05). When compared to preoperative period, both groups’ VAS and ODI scores were significantly reduced at 1 day and 1 year postoperatively (P < 0.05). The vertebral height compression rate and Cobb’s angle were significantly lower (P < 0.05) in both groups after surgery compared with those before surgery (P < 0.05). The cement leakage rate in group H was 26.5%, which was significantly lower than that in group L, which was 61.8% (P < 0.05).
Conclusions
High-viscosity and low-viscosity bone cement in PVP have similar clinical efficacy in reducing pain in patients during the treatment, but in contrast, high-viscosity bone cement shortens the operative time, reduces number of fluoroscopy views and vertebral cement leakage and improves surgical safety.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Osteoporotic vertebral compression fractures are the most common type of fragility fracture. Most patients experience gradual symptomatic relief after several weeks of conservative treatment, however, about one-third of patients still experience persistent pain and discomfort, and about 10% of patients may develop delayed post-traumatic vertebral collapse [1]. The disease was originally described by the German surgeon Kummell in 1895 and it is, therefore, known as Kummell’s disease [2]. Kummell’s disease is characterized by asymptomatic or mild symptoms after minor trauma to the vertebral body, delayed compression fractures over time, progressive pain and kyphosis. The main pathogenesis includes avascular osteonecrosis and pseudo articulation [3,4,5]. The most typical imaging manifestation of Kummell’s disease is intravertebral vacuum cleft (IVC) [3, 6]. In the later stages, vertebral collapse, vertebral pseudo joint formation and kyphosis often cause severe intractable back pain, and some patients even develop spinal cord compression, which affects the well-being of aged patients [7]. Conservative treatment of Kummell’s disease is often ineffective and treatment often needed is surgery [1, 7].
Percutaneous vertebroplasty (PVP) has been widely used in the treatment of osteoporotic vertebral compression fractures due to its rapid pain relief, fracture stabilization, partial recovery of vertebral height and other advantages after its birth and has achieved remarkable clinical results [8]. PVP has also been gradually applied to treat Kummell’s disease, as it is a special type of osteoporotic vertebral compression fracture [9]. However, because there are often significant fissures in the vertebral body of Kummell disease [6], bone cement is prone to leakage along the fractures to the surrounding area during the treatment of bone cement injection. Ha et al. [10] noted in a comparative study that up to 75% leakage of bone cement can occur after vertebroplasty in patients with vertebral vacuum fissure sign. Although a small amount of bone cement leakage does not normally cause clinical symptoms, it can cause serious complications such as thermal injury, nerve root and vessel compression, and pulmonary embolism if it leaks into nerve roots and/or large blood vessels.
Hence, to effectively avoid or reduce the leakage, bone cement has become a challenging in the field of research. In recent years, viscosity has been the key focus to pursue better clinical outcomes and fewer complications in PVP/PKP. Some scholars have reported that the use of high-viscosity bone cement in PVP can reduce leakage with satisfactory clinical efficacy [11,12,13,14]. However, to our knowledge, there are no comparative studies on the efficacy of using different viscosity bone cement during PVP for Kummell’s disease, and therefore, the clinical effectiveness of using high-viscosity bone cement is yet to be studied. For this reason, we conducted a retrospective study to compare the clinical efficacy and complication rates of using high-viscosity and low-viscosity bone cement for the treatment of Kummell’s disease during PVP.
Materials and Methods
2.1. Patient Details
This retrospective study was approved by the Institutional Review Board at The Third Hospital of Hebei Medical University, China. During the period from July 2017 to July 2019, a total of 68 patients with Kummell’s disease type I and II, adopting PVP treatment were included in the present study and were divided into H group (n = 34) and L group (n = 34). The H group was given high-viscosity bone cement in the PVP operation, while the L group was given low-viscosity bone cement in the PVP. Written consent to participate in the study was obtained from each patient.
Inclusion Criteria were (a) Medical history > 3 months, with persistent chest and lower back pain; (b) Age ≥ 60 years; (c) X-ray and CT suggests vertebral compression and fracture, MRI suggests low signal at T1, high signal or mixed signal at T2; (d) Dual-energy X-ray bone densitometry T-score < − 2.5; (e) Patients with a single vertebral lesion; (f) Complete clinical data and follow-up information. Exclusion criteria were (a) Kummell’s disease with neurological symptoms; (b) Vertebral compression fractures due to other causes such as infection, tumor, etc.; (c) Multiple vertebral lesions or a history of previous spinal surgery; (d) Severe comorbidities that preclude surgical treatment; (e) Incomplete follow-up information.
Among them, 25 were male and 43 were female, aged 62–87. Fracture sites: T7 1, T8 2, T9 2, T10 4, T11 13, T12 27, L1 8, L2 4, L3 3, L4 2, L5 2. Kummell’s disease is mostly located in the thoracolumbar segment, with the highest incidence in the T12 vertebra (Fig. 1).

Distribution of vertebral segments and cases of Kummell’s disease
There was no obvious history of trauma in 20 cases and a history of minor sprains or falls in the remaining 46 cases. There were no statistical differences in age, sex, body mass index (BMI), bone mineral density (BMD) and vertebral fracture section between the two groups (Table 1).
Surgical Procedures
The surgery is performed by the same surgeon. Group H was treated by unilateral PVP with high-viscosity bone cement perfusion. High-viscosity bone cement consists of polymethyl methacrylate (87.6%), benzoyl peroxide (2.4%), barium sulfate (10.0%) powder, methyl methacrylate (84.4%), butyl methacrylate (13.2%), N,N-dimethyl P-toluidine (2.4%), hydroquinone (20 ppm) liquid composition; There is no liquid phase after the completion of the concoction, the mixture immediately became the high viscosity, jelly-like, dough period from the curing period to maintain a long time, with low polymerization temperature. The manufacturers of PVP needle and bone cement high-pressure perfusion instruments used are procured from the Domestic Beijing Bonovo Company, and high-viscosity bone cement is manufactured by Heraeus Medical GmbH, Germany. Treatment procedure starts by placing the patient in a prone position with both hands fixed on either side of the head. C-arm X-ray machine fluoroscopy was used to locate the lesioned vertebral body and mark the body surface, and the puncture needle was inserted after routine disinfection and satisfactory local anesthesia. The tip of the puncture needle is placed in the anterior middle 1/3 of the diseased vertebral body by fluoroscopic adjustment on a C-arm X-ray machine. The high-viscosity bone cement was immediately mixed into a doughy shape and then slowly injected into the diseased vertebra with a hydraulic high-pressure infusion instrument under fluoroscopy. Group L was treated with unilateral PVP with low-viscosity bone cement, and the surgical instruments and bone cement were produced by Tecres SPA, Italy. The traditionally used low viscosity bone cement is polymethyl methacrylate bone cement (PMMA), which consists of methyl acrylate—methyl methacrylate polymer 40.58%, zirconia (33.0%), benzoyl peroxide (0.28%) powder and liquid methyl methacrylate (25.98%), N,N-dimethyl P-toluidine (0. 56%) composition after the preparation of low viscosity, dough phase or toothpaste like semi fluidity, dough period from curing time is short, there are exothermic polymerization, monomer toxicity. Preoperative positioning, disinfection and anesthesia were performed initially, and a unilateral arch-root approach was performed under the fluoroscopic guidance of a C-arm X-ray machine. When the puncture needle reaches the posterior edge of the vertebral body, the needle core is removed to place the guide needle. The expansion cannula and fine drill are placed in the anterior collapsed part of the vertebral body in turn, and the bone cement is administered after the position is satisfactory. When the bone cement transitions from a fluid shape to a ductile state, it is injected into the diseased vertebra, and the injection is removed when the bone cement has been adequately filled or has spread till the edge of the vertebra or has spilled outside of the vertebra. All patients were kept in the supine position for the time period of 8–12 h after surgery and were given conventional antibiotic therapy and continued anti-osteoporosis treatment. All patients were clinically and radiologically assessed at 1 day and 1 year postoperatively.
Evaluation Methods
(1) General conditions during operation: operation time, number of X-ray machine fluoroscopy, and amount of bone cement perfusion. (2) Assessment of pain and quality of life: Visual analogue scale (VAS) was used to assess pain and Oswestry and Disability Index (ODI) was used to assess the health of patient before surgery, 1 day, and 1 year after surgery, respectively. (3) Imaging evaluation: The vertebral height compression rate of the injured vertebral body was measured by X-ray lateral radiographs before surgery, 1 day and 1 year after surgery using Eq. (1)
where H1, H2, and H3 are the anterior heights of the fractured vertebra, the vertebra above the fractured vertebra, and the vertebra below the fractured vertebra, respectively. Kyphosis Cobb’s angle was assessed by measuring the kyphotic angle from the superior endplate of the fractured vertebral body to the inferior endplate of the vertebral body before surgery, 1 day and 1 year after surgery (4) Cement leakage: CT examination was performed 1st day after the operation to determine the leakage situation and leakage type of the two bone cements used. In addition, the location of leakage was recorded and classified as follows [15] (1) disc space, (2) epidural space, (3) paravertebral areas, and (4) peripheral veins. All radiological assessments were reviewed by two radiologists who had no involvement in their treatment.
Statistical Analysis
Statistical analysis was performed using SPSS22.0 statistical software (SPSS, Chicago, IL). Data were presented as the Mean ± Standard deviation. For baseline data (Table 1), differences between the two groups were compared by the Student’s t test for continuous data and X2 test or Fisher exact for count data. The VAS score, ODI score, vertebral height compression rate and Kyphosis Cobb’s angle were compared between the two groups preoperatively and postoperatively using the Student’s paired t test. Cement leakage rates in two groups were compared by X2 or Fisher exact test. P < 0.05 was considered to be a statistically significant difference.
Results
All surgeries were performed successfully. The operating time in the H group was 43.35 ± 3.93 min, and 48.88 ± 4.04 min in the L group. The differences were statistically significant, suggesting that PVP using high-viscosity had shortened operation time (P < 0.05, Table 2). The number of intraoperative fluoroscopic views was 18.29 ± 2.96 and 20.50 ± 3.20 in the H group and in the L group, respectively. Statistically significant difference was observed between the two groups (P < 0.05, Table 2).
All 68 patients were successfully followed up, with a mean follow-up time of 14.5 months (range 12–18 months). The preoperative VAS score was 7.97 ± 1.21 in the H group and 7.56 ± 1.23 points in the L group. After surgery, the score was 2.47 ± 0.71 and 2.26 ± 0.45 among the two groups, respectively, with significant differences observed between them (P < 0.05, Table 3). ODI score in the two groups was significantly improved after surgery compared with before surgery, and the differences were statistically significant (P < 0.05, Table 3). However, there was no significant difference in VAS score and ODI score between the two groups before surgery, at 1 day and 1 year after surgery (P > 0.05, Table 3).
Preoperatively, vertebral height compression rate was 40.53 ± 9.67 and 41.41 ± 10.14% in the H and L groups, respectively, and these were significantly decreased in the two groups after Surgery (P < 0.05, Table 4). In both the groups, the kyphosis Cobb Angle was significantly lower at 1 day and 1 year following surgery (P < 0.05, Table 4). But prior to surgery, 1 day after surgery, and 1 year after surgery, there was no discernible difference among the two groups in vertebral height compression ratio and kyphosis Cobb Angle (P > 0.05, Table 4).
Intraoperative bone cement perfusion for (5.89 ± 0.44) ml in the H group and (6.04 ± 0.42) ml in the L group was performed, and there was no statistically significant difference between the two groups (P > 0.05, Table 2). Bone cement leakage occurred in 30 (44.1%) out of 68 patients, but no clinical symptoms were seen in them. In group H, there were nine cases of bone cement leakage, four cases of intervertebral leakage, one case of epidural leakage, three cases of paravertebral leakage, and one case of venous leakage, with a cement leakage rate of 26.5% (9/34). In group L, there were 21 cases of cement leakage, 8 cases of intervertebral leakage, 3 cases of epidural leakage, 6 cases of paravertebral leakage, and 4 cases of venous leakage, with a cement leakage rate of 61.8% (21/34). The leakage rate of the high-viscosity bone cement group was significantly lower than that of the low-viscosity bone cement, and the difference was statistically significant (P < 0.05, Table 5). There was no statistically significant difference in the leakage site of bone cement between the two groups (P > 0.05, Table 5).
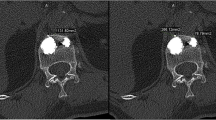
All the bone cement leaks were clinically asymptomatic, and there was no nerve compression or pulmonary embolism occurrence. There were three cases of new adjacent vertebral compression fracture (AVCF) in group H and two cases in group L within 1 year postoperatively. The symptoms improved after receiving an additional VP. There was no significant difference in the rate of AVCF occurrence within 1 year between the two groups (P = 0.64) (Table 5). Pre- and post-operative images of a typical patient in group H treated with PVP using high-viscosity bone cement are shown in Figs. 2, 3 and 4. Pre- and post-operative images of a typical patient in group L treated with PVP using low-viscosity bone cement are shown in Figs. 5, 6 and 7. Postoperative CT scan revealed paravertebral cement leakage [marked by the red arrow, Fig. 7)]. Fortunately, the patient did not have any clinical symptoms.

A 78-year-old female with a compression fracture at the L1 Vertebral body in group H was treated with PVP using high-viscosity bone cement. Anteroposterior X-ray film a and lateral X-ray film b revealed a compression fracture of the L1 vertebral body

Coronal CT scan (c), sagittal CT scan (d) and Transverse CT scan (e) confirmed intraosseous vacuum phenomenon. MRI suggests low signal at T1 (f), high signal at T2 (g)

Coronal CT scan (h), sagittal CT scan (i) and Transverse CT scan (j) obtained postoperatively showing satisfactory vertebral height and bone cement filling without bone cement leakage

A 84-year-old female with a compression fracture at the T8 Vertebral body in group L was treated with PVP using low-viscosity bone cement. Anteroposterior X-ray film (k) and lateral X-ray film (l) revealed a compression fracture of the T8 vertebral body

Coronal CT scan (m), sagittal CT scan (n) and Transverse CT scan (o) confirmed intraosseous vacuum phenomenon. MRI suggests low signal at T1 (p), high signal at T2 (q)

Coronal CT scan (r), sagittal CT scan (s) and Transverse CT scan (t) obtained postoperatively showing satisfactory vertebral height and bone cement filling accompanied by paravertebral cement leakage
Discussion
Kummell’s disease is a kind of delayed post-traumatic vertebral collapse, which is common in elderly patients with osteoporosis and is a special type of osteoporotic fracture [4, 16]. Li et al. 2007 [17] divided Kummell’s disease into three stages: stage I, with < 20% reduction in vertebral body height and no adjacent degenerative disc disease; stage II, with > 20% reduction in vertebral body height, usually accompanied with adjacent degenerative disc disease; stage III, with posterior cortical rupture of the vertebral body combined with spinal cord compression, with the main symptom being low back pain with or without symptoms of spinal cord injury. Kummell’s disease stage III with severe kyphosis and neurological symptoms should be treated with open surgery [18]. Patients with stage I and II Kummell disease usually have no neurological symptoms, and the main goal of surgery is to eliminate micromovement of the fractured vertebrae and rebuild spinal stability. Minimally invasive surgery such as PVP or PKP is preferred for treatment, which can obtain satisfactory clinical efficacy [19, 20].
In this study, the VAS score and ODI score of Kummell’s disease type I and II patients were significantly improved after surgery compared with that of before surgery, but there were no significant differences in VAS score and ODI score of Kummell’s disease patients at the same time point after surgery, suggesting that both bone cement have definite and pain-relieving clinical effects. The reason is that the chemical toxicity of bone cement and the heat released during the polymerization process can damage nerve endings, block nerve conduction and achieve analgesic effect. The injection of bone cement can fill in the fracture space, stabilizing the local fracture and rebuilding the mechanical conduction. Imaging comparison showed that postoperative kyphosis Cobb’s Angle and vertebral height compression rate of the injured vertebrae in the two groups decreased significantly compared with that of before surgery, but there was no difference in postoperative Cobb Angle and vertebral height compression rate of the injured vertebrae in the two groups at the same time point after surgery. The results showed that there was no significant difference in the recovery of vertebral height and the correction of kyphosis Angle between the two groups when the spine was hyperextended and prone during the operation. We considered that the degree of vertebral compression and recovery of kyphosis Angle may be related to the intraoperative position reduction and that the position reduction helps restore vertebral height and improve kyphosis, regardless of the type of bone cement used.
Bone cement leakage is a common complication of PVP treatment for osteoporotic vertebral compression fractures, with an incidence of 22–82% [21, 22]. Nieuwenhuijse et al. [23] believed that the vacuum crack pattern was an unfavorable factor for the leakage of PMMA bone cement. Peh et al. [24] reported that the bone cement leakage rate in PVP treatment of Kummell’s disease was as high as 79% and believed that bone cement leakage was related to vertebral rupture. Generally, when PVP is performed, if bone cement with low viscosity is used, the surgeon must start to inject bone cement when the bone cement enters the ductile state from fluid shape, at which time the bone cement is relatively thin, which may lead to cement leakage. Some studies have suggested that early injection of bone cement with low viscosity increases the incidence of postoperative leakage [25]. However, if low-viscosity cement is injected too late, the cement may not disperse well enough to fill the vertebra completely. It has been reported [26] that when performing PVP surgery, bone cement should be filled as much as possible in the vertebral body so as to produce the best vertebral stiffness and to achieve good therapeutic effect. Some studies [27] believe that high-viscosity bone cement has obvious advantages over low-viscosity bone cement in PVP surgery. High-viscosity bone cement immediately forms a doughy shape without the stage of wire drawing after the preparation. In addition, the dough period is long from the fully formed period, allowing full operation time. Theoretically, the use of high-viscosity bone cement for PVP has certain advantages for the treatment of this disease.
In this study, when there was no statistically significant difference in the amount of bone cement injected between the two groups, the bone cement leakage rate in the PVP group with high viscosity was 26.5%, lower than that in the low viscosity group (61.8%). It suggests that high-viscosity bone cement has an advantage in safety, and the difference is statistically significant, which is consistent with literature reports [28]. This is related to the physical and chemical properties of high-viscosity bone cement, which has a short liquid period, low fluidity and instantaneous high viscosity. In this study, there were 12 cases of intervertebral disc leakage, 9 cases of paravertebral leakage, 5 cases of vein leakage, and 4 cases of epidural leakage. Bone cement leakage was mainly caused by intervertebral disc and paravertebral leakage. Because vertebral body fissures are generally connected to the intervertebral disc and paravertebral area, bone cement leakage in patients with vertebral body fissure sign is more likely to occur in the intervertebral disc and paravertebral area, which is consistent with the study reported by Tanigawa et al. [29]. High-viscosity bone cement has the characteristics of short liquefaction period, which can reduce leakage in the treatment of Kummell’s disease. Meanwhile, the operation time and fluoroscopy time of the high-viscosity bone cement group were significantly less than those of the low-viscosity bone cement group, and the differences were statistically significant. The reduction of fluoroscopy has very important clinical significance. First of all, the surgical time can be minimized, and for elderly patients in prone position, the shorter the surgical time, the better. What is more, in vertebroplasty, even though the surgeon wears lead clothing and the patient wears protective gear, the radiation is still harmful to the human body. Minimizing the number of fluoroscopy during surgery can protect the health of doctors and patients to the greatest extent.
In terms of the adjacent vertebral compression fracture, we did not observe any significant differences between both groups in this study. Studies conducted by Lee et al. [30] revealed that the risk factors for AVCF after VP include BMD, preoperative compression ratio, preoperative sagittal index, intradiscal cement leakage, and large cement volume-to-vertebral body ratio as per the univariate analysis. Significant risk factors for multifactorial analysis were bone mineral density and intradiscal cement leakage. There was no significant difference in the proportion of AVCF, probably due to the absence of such differences in bone density and the proportion of cement leakage within the disc between the two groups. Therefore, PVP with high-viscosity bone cement does not increase the risk of adjacent vertebral re-fracture in single-level Kummel’s disease.
The major limitations of this study were the small sample size and limited follow-up period. Moreover, comparison between kyphoplasty and vertebroplasty with high-viscosity bone cement was not performed. Future studies with larger sample sizes and long-term follow-up periods will be necessary to evaluate the safety and efficacy of high-viscosity bone cement in kyphoplasty and vertebroplasty.
Conclusions
The results of this study confirmed that high-viscosity bone cement and low-viscosity bone cement in PVP have similar clinical efficacy in improving the health status and quality of life and relieving the pain for patients suffering from Kummell’s disease. Based on the study outcomes reported here, high-viscosity cement PVP had comparable effects in restoring vertebral body height and correcting kyphotic deformities, with lower cement leakage rate, less operative time and fluoroscopy views compared to low-viscosity cement. High-viscosity cement was recommended to be used in PVP for the treatment of Kummell’s disease. However, additional studies involving large sample size is warranted to have concrete results corroborating with our study.
Data Availability
All information included in this review is documented by relevant references.
References
Pappou, I. P., Papadopoulos, E. C., Swanson, A. N., Cammisa, F. P., Jr., & Girardi, F. P. (2008). Osteoporotic vertebral fractures and collapse with intravertebral vacuum sign (Kümmel’s disease). Orthopedics, 31(1), 61–66.
Kümmell, H. (1895). Die rarefizierende ostitis der Wirbelkorper. Deutsche Med, 21(1), 180–181.
Lim, J., Choi, S. W., Youm, J. Y., Kwon, H. J., Kim, S. H., & Koh, H. S. (2018). Posttraumatic delayed vertebral collapse: Kummell’s disease. Journal of Korean Neurosurgical Association, 61(1), 1–9.
Formica, M., Basso, M., Cavagnaro, L., Formica, C., Zanirato, A., & Felli, L. (2016). Kümmell disease: Illustrative case for definition criteria. The Spine Journal, 16(10), e707–e708.
Xia, Y. H., Chen, F., Zhang, L., Li, G., Tang, Z. Y., Feng, B., et al. (2018). Percutaneous kyphoplasty treatment evaluation for patients with Kümmell disease based on a two-year follow-up. Experimental and Therapeutic Medicine, 16(4), 3617–3622.
Wang, W., Liu, Q., Liu, W. J., Li, Q. B., Cai, L., & Wang, Z. K. (2020). Different performance of intravertebral vacuum clefts in Kümmell’s disease and relevant treatment strategies. Orthopaedic Surgery, 12(1), 199–209.
Wu, A. M., Chi, Y. L., & Ni, W. F. (2013). Vertebral compression fracture with intravertebral vacuum cleft sign: Pathogenesis, image, and surgical intervention. Asian Spine Journal, 7(2), 148–155.
Siemionow, K., & Lieberman, I. H. (2007). Vertebral augmentation in osteoporosis and bone metastasis. Current Opinion in Supportive and Palliative Care, 1(4), 323–327.
Park, J. W., Park, J. H., Jeon, H. J., Lee, J. Y., Cho, B. M., & Park, S. H. (2017). Kümmell’s disease treated with percutaneous vertebroplasty: Minimum 1 year follow-up. Korean Journal of Neurotrauma, 13(2), 119–123.
Ha, K. Y., Lee, J. S., Kim, K. W., & Chon, J. S. (2006). Percutaneous vertebroplasty for vertebral compression fractures with and without intravertebral clefts. Journal of Bone and Joint Surgery, British Volume, 88(5), 629–633.
Baroud, G., Crookshank, M., & Bohner, M. (2006). High-viscosity cement significantly enhances uniformity of cement filling in vertebroplasty: An experimental model and study on cement leakage. Spine (Phila Pa 1976), 31(22), 2562–2568.
Luo, A. J., Liao, J. C., Chen, L. H., & Lai, P. L. (2022). High viscosity bone cement vertebroplasty versus low viscosity bone cement vertebroplasty in the treatment of mid-high thoracic vertebral compression fractures. The Spine Journal, 22(4), 524–534.
Wang, Q., Sun, C., Zhang, L., Wang, L., Ji, Q., Min, N., & Yin, Z. (2022). High- versus low-viscosity cement vertebroplasty and kyphoplasty for osteoporotic vertebral compression fracture: A meta-analysis. European Spine Journal, 31(5), 1122–1130.
Wang, W., Liu, H., Wu, Z., Teng, Y., Huang, Y., Liu, T., & Yang, H. (2022). A comparison of percutaneous kyphoplasty with high-viscosity and low-viscosity bone cement for treatment of osteoporotic vertebral compression fractures: A retrospective study. Geriatr Orthop Surg Rehabil, 13, 21514593221119624.
Georgy, B. A. (2013). Comparison between radiofrequency targeted vertebral augmentation and balloon kyphoplasty in the treatment of vertebral compression fractures: Addressing factors that affect cement extravasation and distribution. Pain Physician, 16(5), E513–E518.
Swartz, K., & Fee, D. (2008). Kümmell’s disease: A case report and literature review. Spine (Phila Pa 1976), 33(5), E152–E155.
Li, K. C., Li, A. F., Hsieh, C. H., Liao, T. H., & Chen, C. H. (2007). Another option to treat Kümmell’s disease with cord compression. European Spine Journal, 16(9), 1479–1487.
Liu, F., Chen, Z., Lou, C., Yu, W., Zheng, L., He, D., et al. (2018). Anterior reconstruction versus posterior osteotomy in treating Kümmell’s disease with neurological deficits: A systematic review. Acta Orthopaedica et Traumatologica Turcica, 52(4), 283–288.
Huang, Y., Peng, M., He, S., Tang, X., Dai, M., & Tang, C. (2016). Clinical efficacy of percutaneous kyphoplasty at the hyperextension position for the treatment of osteoporotic Kümmell disease. Clinical Spine Surgery, 29(4), 161–166.
Zhang, G. Q., Gao, Y. Z., Chen, S. L., Ding, S., Gao, K., & Wang, H. Q. (2015). Comparison of percutaneous vertebroplasty and percutaneous kyphoplasty for the management of Kümmell’s disease: A retrospective study. Indian Journal of Orthopaedics, 49(6), 577–582.
Elnoamany, H. (2015). Percutaneous vertebroplasty: A first line treatment in traumatic non-osteoporotic vertebral compression fractures. Asian Spine Journal, 9(2), 178–184.
Ploeg, W. T., Veldhuizen, A. G., The, B., & Sietsma, M. S. (2006). Percutaneous vertebroplasty as a treatment for osteoporotic vertebral compression fractures: A systematic review. European Spine Journal, 15(12), 1749–1758.
Nieuwenhuijse, M. J., Van Erkel, A. R., & Dijkstra, P. D. (2011). Cement leakage in percutaneous vertebroplasty for osteoporotic vertebral compression fractures: Identification of risk factors. The Spine Journal, 11(9), 839–848.
Peh, W. C., Gelbart, M. S., Gilula, L. A., & Peck, D. D. (2003). Percutaneous vertebroplasty: Treatment of painful vertebral compression fractures with intraosseous vacuum phenomena. AJR, American Journal of Roentgenology, 180(5), 1411–1417.
Ding, J., Zhang, Q., Zhu, J., Tao, W., Wu, Q., Chen, L., et al. (2016). Risk factors for predicting cement leakage following percutaneous vertebroplasty for osteoporotic vertebral compression fractures. European Spine Journal, 25(11), 3411–3417.
Chen, B., Li, Y., Xie, D., Yang, X., & Zheng, Z. (2011). Comparison of unipedicular and bipedicular kyphoplasty on the stiffness and biomechanical balance of compression fractured vertebrae. European Spine Journal, 20(8), 1272–1280.
Tang, S., Fu, W., Zhang, H., Zhang, H., & Liang, B. (2019). efficacy and safety of high-viscosity bone cement vertebroplasty in treatment of osteoporotic vertebral compression fractures with intravertebral cleft. World Neurosurg, 132, e739–e745.
Zhang, Z. F., Huang, H., Chen, S., Liu, D. H., Feng, Y. H., Xie, C. L., et al. (2018). Comparison of high- and low-viscosity cement in the treatment of vertebral compression fractures: A systematic review and meta-analysis. Medicine (Baltimore), 97(12), e0184.
Tanigawa, N., Kariya, S., Komemushi, A., Tokuda, T., Nakatani, M., Yagi, R., et al. (2009). Cement leakage in percutaneous vertebroplasty for osteoporotic compression fractures with or without intravertebral clefts. AJR, American Journal of Roentgenology, 193(5), W442–W445.
Lee, H. J., Park, J., Lee, I. W., Yi, J. S., & Kim, T. (2019). Clinical, radiographic, and morphometric risk factors for adjacent and remote vertebral compression fractures over a minimum follow-up of 4 years after percutaneous vertebroplasty for osteoporotic vertebral compression fractures: Novel three-dimensional voxel-based morphometric analysis. World Neurosurgery, 125, e146–e157.
Funding
This research received no external funding.
Author information
Authors and Affiliations
Contributions
Conceptualization, D-JK; Methodology, D-PH; Software, D-PH; Formal analysis, J-HW and L-FW; Investigation, J-HW; Resources, L-FW; Writing—original draft, D-JK; Writing—review and editing, YS; Supervision, YS.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflict of interest.
Ethical Standard Statement
This article does not contain any studies with human or animal subjects performed by the any of the authors.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Affiliated Hospital of Hebei University of Engineering (2022[K]038 and 2022-6-16).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kan, DJ., Han, DP., Wang, JH. et al. Efficacy and Safety of High-Viscosity Bone Cement in Percutaneous Vertebroplasty for Kummell’s Disease. JOIO 58, 575–586 (2024). https://doi.org/10.1007/s43465-024-01133-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43465-024-01133-3