
Abstract
Aim
To analyze the functional outcomes between limb salvage and amputation patients who had multiple open injuries in the same lower limb.
Materials and Methods
This observational study analyzed 21 patients who were admitted with multiple open injuries in the same lower limb between January 2012 and December 2015 in our unit. Twelve patients underwent limb salvage and nine patients underwent amputation. The total number of surgeries, duration of hospital stays, ICU admission, complications, time to return to work and costs of inpatient treatment were analyzed. The functional outcome was assessed by using the lower extremity functional scale (LEFS) in both groups, SF-12 score was done for both groups and amputation specific scoring was done by using locomotors capabilities index (LCI).
Results
The LEFS was lower in salvage group than amputation group. The SF-12 score was close to normal population in the amputation group and was higher than salvage group. The duration of hospital stays, total number of surgeries and the costs of inpatient admission were higher in salvage group. The time to return to work was earlier in amputation group. Sixty-seven percentage of patients in the salvage group developed complications.
Conclusion
The functional outcome and SF-12 score was better in amputation group. Patients who had amputation returned to work earlier, had smaller number of secondary hospitalization and has less complications and incurred less expenditure for treatment. The treatment decision should be periodically reviewed when an initial choice of salvage is made. Amputation must be looked at as a treatment for early rehabilitation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The incidence of open lower limb injuries in India is higher than that in other countries due to factors such as larger number of motorcycles, absence of stringent traffic rule implementation, and public negligence [1,2,3]. The ideal treatment choice between amputation and salvage for patients with severe open lower limb injuries is debatable. Most of the literature pertaining to this problem is from developed countries [4,5,6,7].
The Indian scenario is vastly different from that in developed countries due to overcrowded and underfunded public hospitals. Although private healthcare is also available, it is expensive, and the cost of treatment must be borne by the patients.
Additionally, patients who have two major open injuries to the same lower limb constitute another group. The therapeutic choice between limb salvage and amputation becomes more difficult when such patients are confronted in emergency services. Moreover, amputation is unacceptable among Indian population due to various cultural and social reasons.
If it is technically feasible, some surgeons advocate reconstruction despite the cost, resulting in situations where a patient must continuously undergo multiple reconstructive surgeries for 3 years. The psychological trauma, and costs to the patient, society, and healthcare system in terms of time and finances are substantial.
The present observational study was thus conducted to compare the differences in outcome and morbidity between limb salvage and amputation in patients who have multiple open injuries in the same lower limb.
We attempted to answer the following questions.
-
i.
Does amputation lead to better functional outcomes?
-
ii.
Does amputation reduce the total number of surgeries, duration of hospital stays, cost, and complications?
-
iii.
Does amputation lead to an increased rate of return to work?
Materials and Methods
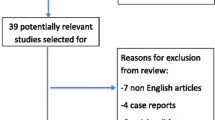
After institutional ethics clearance (IRB 11453), the present observational study was conducted in 21 consecutive patients with at least two open injuries to the same lower limb who were admitted to our unit in this tertiary care center between January 2012 and December 2015. Initially, 29 patients were selected for the study. Of these, eight patients had severe crush injury where reconstruction was not possible. These patients underwent amputation and were excluded from the study. The remaining 21 patients had two major high-energy open injuries in the same lower limb, where at least one of the fractures was a Gustilo–Anderson IIIB injury, and the other fracture was a Gustilo–Anderson IIIA or IIIB injury or a major soft tissue injury which required a flap cover. Among these 21 patients, 18 patients had two open fractures in the same lower limb, whereas the other three had one open fracture and a major soft tissue injury at an additional site in the same lower limb. The soft tissue injury was considered major if it was around a joint and warranted soft tissue cover, or a degloving injury to the foot with heel pad avulsion. The mangled extremity severity score (MESS) and Ganga Hospital Score was calculated for the leg fractures.
All the patients were evaluated by a multidisciplinary team on arrival, and resuscitation was initiated as per standard protocols. Of the 21 patients, 11 presented with a systolic blood pressure of less than 90 mmHg. After a thorough systemic secondary survey, the treatment plan was decided by the orthopedic consultant. A second opinion was also obtained from another orthopedic surgeon confirming the decision.
Patients underwent surgery on an emergency basis, followed by intensive care unit (ICU) admission, if required. Out of 21 patients, 12 had a limb salvage surgery, and nine underwent amputation as decided by the surgical team.
All patients who underwent limb salvage received wound wash, sterile dressings, and intravenous antibiotics, and their limbs were splinted in the emergency department. All fractures were classified using the AO Foundation/Orthopedic Trauma Association (AO/OTA) classification, whereas the grade of open injuries was classified using the Gustilo–Anderson classification. The skeletal stabilization was performed using an external fixator or internal fixation based on the contamination and severity of soft tissue injury decided by the operating surgeon. Further surgical procedures included soft tissue procedures such as re-debridement; skin graft; local flap cover; and bony procedures such as internal fixation, additional plating, and bone grafting, which were performed either during the same hospitalization or in subsequent admissions.
A total of three patients who underwent limb salvage initially had to be taken for a subsequent amputation within 4 days. In one patient, who was referred after initial resuscitation elsewhere and presented late (34 h with a vascular injury) with a type 2 limb ischemia (Rutherford classification), limb salvage was attempted initially but later underwent above-knee amputation later due to persisting sepsis. In the second patient, who had an open femur and foot injury associated with compartment syndrome of leg, limb salvage was initially attempted but he later underwent above-knee amputation as a lifesaving measure in view of sepsis and subsequently expired due to multiorgan dysfunction. In a third patient, who had a crush injury of the foot with an open leg fracture, despite an initial attempt at limb salvage with debridement and external fixator application a below knee amputation was subsequently required in view of infection and an insensate foot.
All the 12 patients in the salvage group required further surgeries during the same hospital stay, ranging from 2 to 4 surgeries (Table 1). All patients underwent periodic clinical and radiological assessment, and standard rehabilitation procedures. In this group, ten patients required subsequent admission and surgeries later (Table 1).
For the purpose of analysis, the limb salvage and amputation group were studied separately. The three patients who underwent an initial attempt at salvage and later required amputation were included in the amputation group for analysis. The total number of surgeries, duration of hospital stays, ICU admission, complications, return to pre-injury work and inpatient treatment costs were analyzed.
The functional outcome was assessed using the lower extremity functional scale (LEFS). The physical and mental health composite scoring SF 12 was calculated in both groups. Amputation functional scoring was assessed by locomotors capabilities index (LCI).
Results
The study group consisted of 18 males and three females. The modes of injury are presented in Table 2.
The average age of the study group was 37.5 years (range: 17–71 years). The average age of patients in the salvage group was 40 years (range: 17–71 years) and in the amputation group was 38 years (range 24–52 years). The average time of presentation post-injury to the emergency services was 8 h (range: 1–48 h). The average time of presentation post-injury in the salvage group was 5 h, whereas it was 9 h in the amputation group. Except one patient who was a diabetic, no other patients in the study group had any systemic illness. The average injury severity score was 20 (range: 18–37). The various combinations of injuries are illustrated in Tables 3 and 4. The LEFS and LCI of amputation patients are exhibited in Table 5.
The LEFS was 25% in four patients, 25–50% in six patients, and more than 50% in one patient in the salvage group. The LEFS was more than 50% in five patients and 25–50% in one patient in amputation group. The LCI was best in five out of six patients and good in one. The average SF-12 physical score was 44 (range: 36.18–47.49) in the amputation group, whereas it was 30 (range: 24.94–33.78) in the salvage group. The average mental score in the amputation group was 50.37 (range: 46.51–54.53), whereas it was 44.45 (range: 38.82–52.14) in the salvage group. The average number of surgeries was 3 (range: 1–6) in the salvage group and 2 (range: 1–3) in the amputation group. The average hospital stay was 38 days (range: 26–72 days) in the salvage group and 15 days (range: 5–29 days) in the amputation group.
The average cost of treatment excluding the pharmacy bill in the salvage group was three times higher than that in the amputation group. Only one patient in the amputation group, who required long-term ICU care due to sepsis exhibited a higher bill. ICU admission was required in 66% of patients in the amputation group and 46% of patients in the salvage group. The average total duration of treatment was 18.5 months (range: 6–48 months) in the salvage group and 3 months (range: 2–6 months) in the amputation group. The complications rate in the salvage group was 67%, with four patients developing knee stiffness, three developing infections, one developing osteomyelitis, two patients presenting with nonunion of femur fracture, one patient developing deep venous thrombosis and one patient with a stiff knee presenting much later with a supracondylar fracture of femur. Sixty-two percentage required further staged surgeries for these complications. No complications were observed in the amputation group.
Five of the six patients who were followed up in the amputation group returned to work early within 1 year of surgery, and only two patients of the six long-term follow-up patients in the salvage group returned to work within 1 year. A total of eight patients in the amputation group had three injuries to the same lower limb, whereas only three patients in the salvage group had a similar type of injury with less than 25% of LEFS. The average MESS was 9 (range: 6–11) in the amputation group and 5.5 (range: 4–7) in the salvage group. The average Ganga hospital score was 14.6 (range: 12–17) in the amputation group. Vascular injuries were observed in five patients in the amputation group and in only one patient in the salvage group.
Discussion
The orthopedic surgeon in the developing countries is faced with an increasing number of patients with multiple complex open injuries to the same lower limb [1, 3]. No guidelines or scores are currently available to prognosticate these injuries and to decide whether amputation or salvage is the best option in this scenario. In single open injury to the lower limb, multiple validated scores are available to assist in the decision on limb salvage or amputation [8,9,10,11,12,13]. Not much information is available regarding the morbidity, cost, duration of treatment, and functional outcome of these injuries. In the absence of this information, it is difficult for the treating surgeon and the patient to decide on the appropriate course of treatment.
In the present study, the functional outcome, time of return to work, duration of treatment, and other factors were assessed in patients with multiple open injuries in the same lower limb.
We used LEFS to assess functional outcome in both the amputation and the salvage group. In the amputation group, five out of six patients had scores more than 50%. Only one patient who had a IIIB patella fracture, proximal shaft of tibia fracture foot crush injury and intertrochanteric fracture and was managed with a through ankle amputation scored 43%. However, 11 out of 12 (91%) patients in the salvage group had less than 50% on the LEFS score after prolonged treatment and multiple surgeries. The time of return to work was 12 months in the amputation group, and three out of six patients returned to their pre-injury occupation. Among the six long-term follow-up patients in the salvage group, only two returned to their pre-injury occupation. This clear difference suggests that amputation may be a better choice in these patients. This hypothesis was further confirmed by the fact that the amputation-specific LCI score was consistently excellent (average 88.5%) in the amputation group, indicating excellent functional recovery in this group. Furthermore, the amputation group exhibited an SF-12 score close to that of the normal population. Among the salvage patients, SF-12 could be calculated only for four patients, which on an average, was less than the patients in the amputation group. All these facts can be used to judiciously decide between salvage and amputation for patients on an individual basis.
In our study, all salvage patients required additional surgeries during the same admission and nine out of 12 patients required rehospitalization for further procedures. The length of hospital stay was higher in salvage patients than in amputation patients during the primary admission. Considering only the inpatient admission bills, the cost of treatment in the amputation group was lower compared with the salvage patients. In our study, 67% of patients in the salvage group developed complications, whereas no complications were observed in the amputation group.
Not much literature evidence is available on similar case series to compare with our study. However, there are studies which compared amputation vs limb salvage in leg-threatening severe lower limb injuries [5, 7, 14]. In contrast with our study, all these studies included patients with only one severe injury in the lower limb.
Busse et al. concluded in their meta-analysis involving severe open tibial fractures (leg-threatening injuries) that the functional outcome was similar in both amputation and salvage groups [5]. However, in our study, the functional outcome was lower in the salvage group. This might be because there were multiple injuries to the same lower limb in our study. They further concluded that the time of return to work was similar in both the groups. This was contrary to our findings, where we observed that the time to return to work was earlier in the amputation patients than in the limb salvage patients. The length of hospital stay was shorter in the amputation group compared with the salvage group. However, Busse et al. reported similar length of hospital stays between the two groups. The length of rehabilitation, total costs, additional procedures, rehospitalization, and complications in their study were higher for limb salvage patients, which was mirrored in our study.
The lower extremity assessment project (LEAP) of patients who had single severe open injury to the lower limbs exhibited similar functional outcomes between the salvage and amputation groups at the end of 2 years [14]. In our study, the amputation group had better functional outcomes than the limb salvage group at the end of 4 years. The patients who underwent reconstruction in this study were more likely to have a secondary hospitalization for major complications than those who underwent amputation. This finding was similar in our study group.
Currently, there are no scores which can help to decide between limb salvage and amputation in patients who have multiple open injuries to the same lower limb. For open leg injuries, scores such as MESS and Ganga hospital score have been used. Ganga hospital score has been validated to demonstrate 98% sensitivity and 100% specificity [15]. Further studies will be required to assess the possibility to develop a score to aid decision-making in this complex setting and the efficacy of the Ganga hospital score and MESS in decision-making. However, these scores were developed only for leg injuries.
Based on our study, we are unable to reach a definitive conclusion regarding poor prognostic factors in these injuries. However, in patients with three open injuries in the same lower limb, simultaneous open IIIB injuries in two areas of the same limb, other skeletal injuries, and vascular injury, the functional outcome was likely to be poor.
The limitations of this study are due to its retrospective nature. However, in this condition prospective randomized trials may not be ethical. In addition, the incidence of these injuries is not high. Hence retrospective studies are helpful. The patient follow-up in salvage group could have been better. All efforts were made to contact the patients including visits to the address provided by the patient by one of the authors.
Conclusion
The following differences were observed between the amputation and salvage group in patients with multiple open injuries to the same lower limb:
-
1.
The functional outcome was better in the amputation group.
-
2.
The SF-12 scores were better in the amputation group.
-
3.
Patients who had amputation returned to work earlier, had a smaller number of secondary hospitalization and surgeries, exhibited fewer complications, and incurred less expenditure for treatment.
The choice between limb salvage and amputation is difficult in patients with single severe leg-threatening injuries. When patients have multiple open injuries to the same lower limb, the decision-making about salvage or amputation is much more complex. No clinical scores are available to help in this regard. Hence, a thorough evaluation of the patient considering all the injuries, decision-making by a team of orthopedic surgeons, and an individualized decision-making for each patient is necessary in managing these patients. The treatment decision should be periodically reviewed when an initial choice of salvage is made. Amputation should not be considered as a failure. Rather, it must be looked at as a treatment for early rehabilitation.
References
Gopinathan, N. R., Santhanam, S. S., Saibaba, B., & Dhillon, M. S. (2019). Epidemiology of lower limb musculoskeletal trauma with associated vascular injuries in a tertiary care institute in India. Indian Journal of Orthopaedics. http://www.ijoonline.com/article.asp?issn=0019-5413;year=2017;volume=51;issue=2;spage=199;epage=204;aulast=Gopinathan. Accessed 27 May 2019.
Road accidents in India 2017. http://www.indiaenvironmentportal.org.in/files/file/road%20accidents%20in%20India%202017.pdf. Accessed 6 June 2019.
Shakti, G., Neel, B., Harnish, M., et al. (2019). Epidemiology and patterns of lower limb injuries at a tertiary care hospital in Ahmedabad. https://www.researchgate.net/publication/278847952_Epidemiology_and_patterns_of_lower_limb_injuries_at_a_tertiary_care_hospital_in_Ahmedabad. Accessed 27 May 2019.
Bosse, M. J., MacKenzie, E. J., Kellam, J. F., Burgess, A. R., Webb, L. X., Swiontkowski, M. F., et al. (2002). An analysis of outcomes of reconstruction or amputation after leg-threatening injuries. The New England Journal of Medicine, 347(24), 1924–1931.
Busse, J. W., Jacobs, C. L., Swiontkowski, M. F., Bosse, M. J., & Bhandari, M. (2007). Evidence-based orthopaedic trauma working group. Complex limb salvage or early amputation for severe lower-limb injury: a meta-analysis of observational studies. Journal of Orthopaedic Trauma, 21(1), 70–76.
Dagum, A. B., Best, A. K., Schemitsch, E. H., Mahoney, J. L., Mahomed, M. N., & Blight, K. R. (1999). Salvage after severe lower-extremity trauma: are the outcomes worth the means? Plastic and Reconstructive Surgery, 103(4), 1212–1220.
MacKenzie, E. J., Bosse, M. J., Kellam, J. F., Burgess, A. R., Webb, L. X., Swiontkowski, M. F., et al. (2002). Factors influencing the decision to amputate or reconstruct after high-energy lower extremity trauma. The Journal of Trauma, 52(4), 641–649.
Durham, R. M., Mistry, B. M., Mazuski, J. E., Shapiro, M., & Jacobs, D. (1996). Outcome and utility of scoring systems in the management of the mangled extremity. American Journal of Surgery, 172(5), 569–573. (Discussion 573–574).
Fodor, L., Sobec, R., Sita-Alb, L., Fodor, M., & Ciuce, C. (2012). Mangled lower extremity: can we trust the amputation scores? International Journal of Burns and Trauma, 2(1), 51–58.
Helfet, D. L., Howey, T., Sanders, R., & Johansen, K. (1990). Limb salvage versus amputation. Preliminary results of the Mangled Extremity Severity Score. Clinical Orthopaedics and Related Research, 256, 80–86.
Kumar, M. K., Badole, C., & Patond, K. (2007). Salvage versus amputation: utility of mangled extremity severity score in severely injured lower limbs. Indian Journal of Orthopaedics, 41(3), 183–187.
Ly, T. V., Travison, T. G., Castillo, R. C., Bosse, M. J., & MacKenzie, E. J. (2008). LEAP Study Group. Ability of lower-extremity injury severity scores to predict functional outcome after limb salvage. The Journal of Bone and Joint Surgery American, 90(8), 1738–1743.
Rajasekaran, S., Sabapathy, S. R., Dheenadhayalan, J., Sundararajan, S. R., Venkatramani, H., Devendra, A., et al. (2015). Ganga hospital open injury score in management of open injuries. European Journal of Trauma and Emergency Surgery, 41(1), 3–15.
Higgins, T. F., Klatt, J. B., & Beals, T. C. (2010). Lower Extremity Assessment Project (LEAP)–the best available evidence on limb-threatening lower extremity trauma. The Orthopedic Clinics of North America, 41(2), 233–239.
Rajasekaran, S., Naresh Babu, J., Dheenadhayalan, J., Shetty, A. P., Sundararajan, S. R., Kumar, M., et al. (2006). A score for predicting salvage and outcome in Gustilo type-IIIA and type-IIIB open tibial fractures. The Journal of Bone and Joint Surgery British, 88(10), 1351–1360.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Ethical Standard Statement
This article does not contain any studies with human or animal subjects performed by the any of the authors.
Informed Consent
For this type of study informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Govindaraju, S.K., Inja, D.B., Albert, S. et al. Multiple High-Energy Open Injuries in the Same Limb: Comparison of Outcomes Between Salvage and Amputation Groups. JOIO 55, 734–740 (2021). https://doi.org/10.1007/s43465-020-00311-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43465-020-00311-3