
Abstract
The use of mathematical modeling to represent, analyze, make predictions or providing information on data obtained in drug research and development has made pharmacometrics an area of great prominence and importance. The main purpose of pharmacometrics is to provide information relevant to the search for efficacy and safety improvements in pharmacotherapy. Regulatory agencies have adopted pharmacometrics analysis to justify their regulatory decisions, making those decisions more efficient. Demand for specialists trained in the field is therefore growing. In this review, we describe the meaning, history, and development of pharmacometrics, analyzing the challenges faced in the training of professionals. Examples of applications in current use, perspectives for the future, and the importance of pharmacometrics for the development and growth of precision pharmacology are also presented.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Pharmacometrics has emerged as a tool important to the field of clinical pharmacology, allowing for the development and application of mathematical and statistical methods in understanding, characterizing, and predicting exposure and response to drugs. This branch of science aims to create models and simulations of biology, pharmacology, disease, and physiology that can describe and quantify interactions between xenobiotics and patients, human or not, considering beneficial and adverse effects [1,2,3,4,5,6,7].
The U.S. Food and Drug Administration (FDA) uses pharmacometrics to quantify substances, diseases, and test information with the aim of assisting in the development of new drugs and regulatory decision-making, making those processes more efficient. That is, drug developers and regulators recognize that pharmacometrics approaches are considered innovative and can improve the interpretation of significant amounts of data and predict large-scale processes. Those techniques, also known as data modeling and simulation (M&S), can be widely applied in drug research and development and in the translational validation of models through the more efficient use of collected clinical data, contributing to decision making about future studies and to the development of study designs with more assertive dose selection [8,9,10,11,12,13,14,15,16,17,18].
In recent years, the application of pharmacometrics has stood out in the FDA’s approval process, whether in dose adjustments for special populations (elderly individuals and children, for example) or in specific diseases such as diabetes and kidney disease [19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40] (Table 1).
By minimizing costs and time (which are considered obstacles in conventional clinical studies) and by maximizing the information generated from trials, pharmacometrics has become a powerful ally in drug research and development [41,42,43,44,45,46]. In addition, the multidisciplinary vision embodied by pharmacometrics constitutes an important resource to integrate knowledge and promote rational decision-making (Fig. 1).

Steps in the application of pharmacometrics. ADME absorption, distribution, metabolism, excretion, IV intravenous, PK pharmacokinetics, PD pharmacodynamics
History and Development of Pharmacometrics
Regulatory authorities such as the FDA and the European Medicines Agency (EMA) have sets of guidelines that describe the experiments needed to meet regulatory requirements in drug development requirements that include M&S. However, the use of pharmacometrics is recent: the first mentions appear in articles by Lee in 1971 and 1976 [1].
The first pharmacometrics group at the FDA’s Center for Drug Evaluation and Research (CDER) was established in 1991. Initially, that group changed the focus of drug development, shifting the emphasis from interpretation of dose–response information to analysis of exposure–response data [47].
In 1994, the FDA published guidelines in ICH E7—Studies in Support of Special Populations: Geriatrics, with recommendations that pharmacokinetic screening be performed to gather important information about the safety and efficacy of medications used in elderly individuals. In 1999, the agency issued guidelines on population analyses for the pharmaceutical industry and, in 2003, on exposure–response relationship analyses.
In general, those documents recommended the use of special methods for data collection and analysis, indicating the trend toward the use of Pharmacometrics analyses in the near future.
Challenges in Teaching Pharmacometrics
Because Pharmacometrics analyses are considered more efficient than those using conventional methods, the application of Pharmacometrics techniques and the demand for qualified professionals are both increasing exponentially.
On the other hand, obtaining specific training in the field of pharmacometrics led to certain problems being encountered, such as a lack of degree granting in the area and lack of standardization of a basic curriculum. Universities, pharmaceutical industry research centers, the FDA, and nonprofit associations offered only training fellowship programs. An example is the International Society of Pharmacometrics, which emerged in 2013 and which aims to promote and expand the science of pharmacometrics through the integration of multidisciplinary data and continuous innovation in methods and technologies, leading to impacts on discovery, research, development, and approval and use of new therapies. It also promotes scientific events, offers training materials, and maintains official journals that disseminate research and news. A community of student members who have organized themselves into special interest groups is dedicated to the study of specific subject areas (Fig. 2):
-
Clinical pharmacometrics: applying pharmacometrics to guide patient care
-
Mathematical and computational sciences: developing new theories, methods, and computational tools
-
Quantitative systems pharmacology: advancing the development and use of safe and effective drugs through the application of quantitative systems pharmacology
-
Statistics and pharmacometrics: promoting collaboration between pharmacists and biostatisticians to develop innovative approaches in modeling drug development

International Society of Pharmacometrics special interest groups
Bringing together various subject areas is clearly something intrinsic to pharmacometrics, which facilitates the translation of highly complex biologic processes into a quantitative language, therefore making the discipline an effective communications bridge. But integrating data, proposing model structures, interpreting raw data, extracting the most from publicly available data and information, and predicting the value of data and models are complex tasks. Consequently, the need to provide professionals who are competent in pharmacometrics is urgent.
Education in this area has to be standardized through the development of appropriate curricula (with M&S still being incorporated into the undergraduate course in Pharmacy), increasing the frequency and number of training courses so as to offer continuing education that meets the demands of a growing market.
Perspectives and Applications of Pharmacometrics
Given the complexity of integrating experimental observations with observations emerging from clinical medicine, M&S has been applied in the preclinical phase, to both in silico studies [48] and studies using animal models [49], and also in the clinical stage for patient follow-up [43, 50, 51]. For any drug, its pharmacokinetic profile (any one or a combination of absorption, distribution, metabolism, and excretion), concentration at the site of action, change in effect related to disease-specific changes, and many other variables make interpretation a real challenge when seeking to identify correlations that contribute to more effective pharmacotherapy.
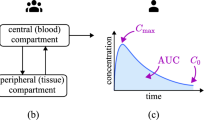
In this sense, modeling aims to develop a mathematical representation that relates the covariates of a process, disease, or system, and simulation seeks to solve mathematical equations so as to show the variables that can be considered relevant to the process in question. Pharmacometrics-based analyses include drug models (based on pharmacokinetics or PK), exposure–response models (pharmacokinetics–pharmacodynamics or PK-PD), physiology-based models (PBPK), and clinical trials models (Clinical Trial Simulation or CTS). The choice of approach depends on the pharmacokinetics and pharmacodynamics of the drug [52] and on the clinical objectives and questions to be answered.
For example, population pharmacokinetics models (popPK) can be useful if the aim is to find pharmacokinetic parameters and sources of variability in a given population [53]. It is also possible to associate popPK data with pharmacodynamics data to uncover the relationships between exposure and response to a drug, generating a more robust and accurate understanding of the pharmacologic action of a compound in the body [54]. Those models are considered empirical and describe clinical data based on the analysis of concentration as a function of time (“top down”). However, that approach limits the ability to predict pharmacokinetics for a similar drug or to extrapolate results to different physiologic conditions.
The PBPK models have a mechanistic approach (“bottom up”), compared against which the empirical models are noted to be simpler and more descriptive [55]. But the more complex PBPK models provide more robust prediction with respect to how changes in a pathophysiologic condition can affect specific system parameters leading to changes in pharmacologic effect [54]. Thus, PBPK models consider detailed data about an organism’s physiology (density of receptors, disease progression, homeostatic feedback, blood flow); the drug’s properties (site of action, affinity to target protein, lipophilicity, solubility); and the study design (dose administered, route and frequency of administration) [56] (Fig. 3). The most common use of PBPK in drug development is the study of drug interactions (60%), followed by studies for pediatric populations (16%) [57].

Schematic of a physiology-based pharmacokinetics (PBPK) model. The inset presents a detailed representation of the intestine. CLint intrinsic clearance. (Reprinted from Jones and Rowland-Yeo [56])
The growing interest of the pharmaceutical industry in the application of PBPK modeling has increased the number of platforms that integrate this modeling method, among them: Simcyp PBPK Simulator (Certara, Princeton, NJ, U.S.A.; https://www.certara.com/software/simcyp-pbpk/), GastroPlus (Simulations Plus, Lancaster, CA, U.S.A.; https://www.simulations-plus.com/software/gastroplus/), and PK-Sim (Bayer Technology Services, Leverkusen, Germany; http://www.systems-biology.com/products/pk-sim.html).
Finally, clinical trial simulation models represent a specialized area of quantitative pharmacology that generates pharmacokinetics or pharmacodynamics profiles (or both) in virtual participants [58] (Fig. 4), considering study design and execution, pathophysiologic changes in participants during the trial, and the pharmacokinetic and pharmacodynamic characteristics of the drug [59].

Information sources for a model used in clinical trial simulation. PK/PD pharmacokinetics/pharmacodynamics. (Reprinted from Kimko and Peck, [58])
Pharmacometrics can be used to achieve a variety of objectives, such as analyzing progression in diseases such as HIV-triggered immunodeficiency [60], osteoporosis [61], multiple sclerosis [62], rheumatoid arthritis [63, 64] and diabetes [65,66,67]. Studies that investigate certain disorders of the central nervous system such as depression, Alzheimer disease, and schizophrenia have increased the use of M&S strategies to assess the efficiency of drugs in preclinical and clinical studies [68].
M&S can also be applied in biomarker follow-up studies [69,70,71], in the analysis of drug–drug interactions [72,73,74,75,76,77], for dose adjustment in special populations such as pediatrics [78,79,80,81] and in studies focused on the veterinary market [82,83,84,85,86]. Examples are presented in the subsections that follow.
HIV-Triggered Immunodeficiency
Approximately 35 million people worldwide are infected with HIV. In drug research and development, pharmacometrics helps in the search for improvements in treatment that could overcome current limitations related to side effects and monitoring of disease progression.
In the 1990s, a model was developed being able to predict the HIV replication process in the plasma of infected individuals—a great achievement for the study of that disease [87]. The calculated value was approximately 12 billion viral particles per day. Subsequently, several studies using M&S proposed the inclusion of covariates that could be important to an understanding of the dynamics of the infection [88,89,90,91,92,93,94,95,96,97,98,99,100,101].
Given the high rate of viral replication observed, mutation and drug resistance must be considered during treatment, and therapy with multiple drugs is necessary. A PBPK model was proposed as a predictive tool for drug–drug interactions with tenofovir [102] (Fig. 5). The model was able to predict a 60% increase in plasma tenofovir exposure and a reduction in renal cell exposure by a factor of 3 after co-administration with 2 g probenecid. The expected increase in exposure, considering the observed clinical pharmacokinetics data, was 15%. The resulting PBPK model can be used to assess the safety and efficacy of drug–drug interactions involving the inhibition of OAT1 and OAT3.

Proposed drug–drug interactions (DDIs) in a physiology-based pharmacokinetics model workflow. PRO probenecid, TFV tenofovir, PBMC peripheral blood mononuclear cell. (Reprinted from Liu et al. [102])
Osteoporosis
Osteoporosis is a chronic disease characterized by low bone density and tissue deterioration. The result is increased bone fragility and, consequently, greater susceptibility to fractures. A higher incidence is seen in women during menopause. Reduction in estrogenic hormonal activity promotes an imbalance in bone remodeling favoring osteoclast-mediated resorption and less formation of new cells by osteoblasts. M&S has been used to evaluate therapies using various classes of drugs such as bisphosphonates, cathepsin K inhibitors, parathormone and its analogs, and others [103,104,105].
Bisphosphonates such as etidronate, clodronate, alendronate, and risedronate inhibit bone resorption. After administration, they accumulate rapidly on the bone mineral surface and are released slowly (having half-lives of months to years). The development of PK and PK-PD models for bisphosphonates has traditionally been a challenge because of a lack of assays sufficiently sensitive to quantify the drugs in serum, urine, and bone. This limitation makes it difficult to describe long-term pharmacokinetic parameters and the relationship of exposure with the anti-resorptive effect [106]. Consequently, models linking pathophysiology with clinical biomarkers have gained popularity [61, 107,108,109,110].
Such models can be established at various levels of complexity, ranging from descriptive to mechanistic approaches. A drug-trial model was developed for postmenopausal osteoporosis that used a mechanistic approach [111]. The resulting model was able to identify changes in clinically relevant biomarkers over time as a result of disease progression and to assess the response to therapeutic interventions. Models of this kind are of great importance for monitoring and follow-up of patients.
Another class of drugs with anti-resorptive action also had its studies guided by M&S. The inhibitory effects of cathepsin K were compared with those of bisphosphonates. Some cathepsin K inhibitors such as odanacatib are excreted in urine and bile and appear to undergo enterohepatic recirculation, which is reflected by a double peak after oral administration [112]. The pharmacokinetics have been described by several models, in most cases using simple 1-, 2-, or 3-compartment models [113, 114].
The relationship between the serum concentrations of 3 different cathepsin K inhibitors [odanacatib (MK-0822), MK-0674, and MK-1256] and the associated effects on bone resorption markers in various animals and in humans was explored [115]. A better relationship was observed between the unbound drug concentration and anti-resorptive action than between the total drug concentration and anti-resorptive action. The elucidation of such pharmacokinetic–pharmacodynamic relationships will be of great translational value for prediction among various species.
Diabetes Mellitus
Pharmacometrics is also being used in studies of metabolic diseases. Diabetes mellitus is a group of metabolic disorders characterized by hyperglycemia resulting from problems with insulin secretion (type 1, failure to produce insulin), insulin action (type 2, insulin resistance), or both.
Treatment of type 1 diabetes is limited to insulin injections, whereas in type 2 diabetes, patients can control blood glucose with diet and regular physical activity. Anti-hyperglycemic medications available on the market belong to various classes and can be prescribed as monotherapy or in combination.
Biomarkers are of great importance for monitoring the progression of the disease and also for evaluating the response to pharmacologic treatment. In type 2 diabetes, glycosylated hemoglobin A1 (HbA1c) provides information about medium- to long-term glycemic control; plasma glucose and serum insulin, both in fasting state, are the biomarkers most responsive to changes in glycemic control in the short term.
A study applied a population pharmacodynamics model of disease progression that integrated HbA1c, fasting plasma glucose, and fasting serum insulin data into a single comprehensive and physiologically significant structure [65]. The model provided accurate descriptions of the relationship of biomarkers to disease progression and allowed the long-term effects of various treatments using pioglitazone, metformin, and gliclazide on the loss of beta-cell function and insulin sensitivity to be identified. Expanding that model, Gaitond et al. considered the physiologically significant dynamics between the biomarkers fasting plasma glucose, fasting serum insulin, and HbA1c; the inter-individual differences in disease state for patients at baseline and during disease progression; and clinically significant covariate relationships [116].
The proposed model is of great importance for quantitative pharmacology because it can identify the relationships among patient characteristics, drug action, and disease peculiarities in a physiologically significant analysis.
Other studies of marketed hypoglycemic agents can also be performed using data available in the literature, providing information for evaluating drug dose–response relationships. Models developed based on data from the literature [117, 118] are similar to models developed using patient data, except that the variability estimates reflect the variability of each trial performed [117, 119, 120].
Multiple Sclerosis
Multiple sclerosis is a chronic debilitating disease characterized by repeated episodes of neurologic dysfunction separated by intermittent periods of partial or complete recovery [121].
The effectiveness of treatment is typically assessed using decline in the frequency of relapses and progression of the deficiency (“endpoints”). In an M&S study, pharmacodynamics models used data from 1319 patients who received placebo or cladribine (Trial 25643 [CLARITY, NCT00213135] and Trial 27820 [CLARITY EXT, NCT00641537]) to characterize the time course of the multiple sclerosis endpoints. Disability scale measures were then evaluated as predictors of efficacy outcomes. The resulting models showed a positive correlation between cladribine use and the endpoints, with a lower (or even nonexistent) relapse rate being observed [122]. Such specific and, above all, reliable models allow for comparisons between drugs already in use and those recently discovered, potentially guiding decisions about whether to continue the use of drugs available for commercialization.
A popPK–pharmacodynamics model was developed to establish the quantitative relationship between pharmacokinetics and the relapse rate in patients who used different peginterferon beta-1a therapeutic regimens [123]. Pharmacokinetics were well described by a 1-compartment model, with first-order absorption and linear elimination kinetics. The results, when compared with those from a placebo group and with the different regimens, demonstrated that administration every 2 weeks was sufficient for observation of benefit. The study was of great importance in safely proposing a dose adjustment to regulatory agencies.
Special Populations: Pediatrics
Current EMA and FDA guidelines recommend that dose selection for pediatric studies be based on all available prior information, starting with learnings from adult populations [124, 125]. However, incomplete understandings of the effects of growth and development (or maturation) on drug disposition (pharmacokinetics) and drug effects (pharmacodynamics) remain a significant challenge in defining appropriate doses for children [126].
Advances in quantitative pharmacology and in model-based drug research and development go hand in hand in pediatric research [127, 128]. Pharmacometrics studies for pediatric populations use data from drugs that are already available on the market, but for which information about safety and efficacy for young patients is lacking. The definition of “dose” must consider the clearance, volume of distribution, and dose–response relationship in addition to ontogenic and clinical factors.
Comparative analysis were presented of the various types of models that were used to approve the use of some drugs in pediatrics [129]. Dose selection for esomeprazole was based on pharmacokinetic correspondence with the adult dose, using a simulation based on pharmacokinetics/pharmacodynamics. Adalimumab has been recommended for the treatment of Crohn disease in children based on pharmacokinetic data, the pharmacokinetics/pharmacodynamics ratio, and efficacy and safety data. On the other hand, dose–response for vigabatrin was found to be similar for children and adults, allowing for application of the allometric scale to calculate the pediatric dose.
With PBPK models, a consideration of the effects of the child’s growth and development is possible. Aspects such as body size and composition, tissue blood flow, and biochemical characteristics (enzyme and transporter profiles) can therefore be included in the M&S. Table 2 shows some examples of the application of this physiology-based approach [130,131,132,133,134].
M&S in pediatric drug research and development can also be used to compare and optimize studies, understand the ontogeny and natural history of disease, and describe pharmacokinetics and pharmacodynamics profiles in clinical pharmacology quantification studies.
Applications in the Veterinary Market
The animal health industry is on a growth trajectory, fueled by an increase in the number of pets and also by an increased global population that seeks food products such as meat and dairy. In 2014, developers and manufacturers of drugs and vaccines for pets and farm animals achieved a sales record of US$24 billion, and projections through 2020 reached US$33 billion [135].
Some differences between the human and veterinary pharmaceutical market are evident. According to the FDA, the cost to develop a new veterinary drug is approximately $100 million over a period of 7–10 years; for humans, the cost reaches $1 billion over a period of 12 years. In another comparison, veterinary drug studies are carried out in models of the species of interest, which shortens the pre-clinical phase. Moreover, “animal patients” have a shorter life expectancy, which is also reflected in studies seeking data about efficacy and safety.
The regulatory agencies, the FDA and the EMA, maintain requirements for approved drugs that include proof of manufacturing quality, plus safety and effectiveness. They also require tests to ensure that the tissues and milk of treated animals are safe for human consumption. Given those requirements, pharmacometrics models are also incorporated into the professional routine for the veterinary market. A food safety analysis study used PBPK modeling to predict penicillin concentrations in milk. A high number of animals with residues above the limit was observed because of use of a higher than established drug dose. The model was able to quantify penicillin residues in tissue and milk based on a comparison with data from earlier pharmacokinetics studies [136]
Mavacoxib (a COX-2 inhibitor) is approved for the treatment of osteoarthritis in dogs. Simulations based on PopPK modeling in a comparative study using 1317 samples from 286 dogs that received 2 different mavacoxib doses (4 mg/kg and 2 mg/kg) indicated that most dogs (> 85%) treated with mavacoxib 2 mg⁄kg sustained concentrations above the efficacy level (0.4 µg/mL) throughout the entire dose interval [137]. That study helped to justify reducing the dose of mavacoxib to 2 mg/kg from 4 mg/kg, increasing its therapeutic index.
The use of monoclonal antibody therapies is relatively new in veterinary medicine. The first such antibody was lokivetmab (Cytopoint: Zoetis Services, Parsippany, NJ, U.S.A.), which was approved in 2016. It is indicated for the treatment of canine atopic dermatitis, with an anti–IL-31 mechanism of action. A pharmacokinetics/pharmacodynamics model was used to define the recommended dose of Cytopoint [138]. Other studies applying M&S to the use of monoclonal antibodies can be found [139, 140], reinforcing the importance of those techniques for precision pharmacology.
Starting from the initial stages of veterinary drug projects, pharmacometrics remains present through to the approval and post-marketing phases, where it assists in responding to regulatory issues. It therefore constitutes an important tool for the veterinary market during its current expansion.
The Already-Present Future of Precision Pharmacology
Clinical pharmacology is fundamental to the management of drug-related problems and an important instrument of precision medicine. Through its mathematical models (pharmacokinetics, pharmacokinetics/pharmacodynamics, and PBPK), pharmacometrics refines data extrapolation, lending additional confidence to quantitative prediction by integrating modern concepts of the pathophysiology and pharmacology of systems [141, 142].
Pharmacometrics approaches yield strategies for research and development of new drugs and add efficiency and rigor to regulatory processes. This is because the models developed allow us to understand and predict: the physiological phenomena, the action of the studied drug and the results of clinical trials. M&S also reduces costs and time for research and development as it contributes to the choice of a molecule, guides decisions on which way to go, optimizes pre-clinical and clinical planning, assists in dose selection as well as regulatory approvals. Thus, by exploring the variability and better understanding the molecules, pharmacometrics tools can further support decisions, increasing the probability of successful clinical development and, consequently, the efficacy and safety of new drugs [143].
Studies in Pharmacokinetics, including Pharmacometrics, are essential to understand all these important aspects in the development of new drugs and require a rational approach with a multidisciplinary scope. Only in this way will it be possible to propose innovative strategies in the search for effective and safe pharmacotherapy that will guarantee adherence to treatment and, above all, a positive impact on the patient's quality of life.
For those criteria to be met, furthering the training of professionals to work at the academic level and in the pharmaceutical industry in researching new drugs is essential into the future. In the absence of a specific and standardized curriculum, a constant search for partnerships with clinical research centers and the private sector is necessary to carry out new projects and collaborations, to disseminate expertise, and to deliver services. Only with such collaborations will it be possible to guarantee the already-present future of precision pharmacology.
References
Barrett JS, Fossler MJ, Cadieu KD, et al. Pharmacometrics: a multidisciplinary field to facilitate critical thinking in drug development and translational research settings. J Clin Pharmacol. 2008;48(5):632–49.
Chan PLS, Holford NHG. Drug treatment effects on disease progression. Annu Rev Pharmacol Toxicol. 2001;41:625–59.
Gobburu JV, Lesko LJ. Quantitative disease, drug, and trial models. Ann Rev Pharmacol Toxicol. 2008;49:291–301.
Eddy DM, Archimedes SL. A trial-validated model of diabetes. Diabetes Care. 2003;26:3093–101.
Bangs A. Predictive biosimulation and virtual patients in pharmaceutical R and D. Stud Health Technol Inform. 2005;111:37–42.
Landersdorfer CB, Jusko WJ. Pharmacokinetic/pharmacodynamic modelling in diabetes mellitus. Clin Pharmacokinet. 2008;47:417–48.
Danhof M, de Jongh J, De Lange EC, et al. Mechanism-based pharmacokinetic-pharmacodynamic modeling: biophase distribution, receptor theory, and dynamical systems analysis. Annu Rev Pharmacol Toxicol. 2007;47:357–400.
Sheiner LB. Learning versus confirming in clinical drug development. Clin Pharmacol Ther. 1997;61:275–91.
Breimer DD, Danhof M. Relevance of the application of pharmacokinetic pharmacodynamic modelling concepts in drug development. The ‘wooden shoe’ paradigm. Clin Pharmacokinet. 1997;32:259–67.
Minto C, Schnider T. Expanding clinical applications of population pharmacodynamic modelling. Br J Clin Pharmacol. 1998;46:321–33.
Derendorf H, Meibohm B. Modeling of pharmacokinetic/pharmacodynamic (PK/PD) relationships: concepts and perspectives. Pharm Res. 1999;16:176–85.
Balant LP, Gex FM. Modelling during drug development. Eur J Pharm Biopharm. 2000;50:13–26.
Holford NH, Kimko HC, Monteleone JP, et al. Simulation of clinical trials. Annu Ver Pharmacol Toxicol. 2000;40:209–34.
Bonate PL. Clinical trial simulation in drug development. Pharm Res. 2000;17:252–6.
Sheiner LB, Steimer JL. Pharmacokinetic/pharmacodynamic modeling in drug development. Annu Rev Pharmacol Toxicol. 2000;40:67–95.
Aarons L, Karlsson MO, Mentre F, et al. Role of modelling and simulation in phase I drugdevelopment. Eur J Pharm Sci. 2001;13(2):115–22.
Meibohm B, Derendorf H. Pharmacokinetic/pharmacodynamic studies in drug product development. J Pharm Sci. 2002;91:18–23.
Stanski DR, Rowland M, Sheiner LB. Getting the dose right: report from the tenth European Federation of Pharmaceutical Sciences (EUFEPS) conference on optimizing drug development. J Pharmacokinet Pharmacodyn. 2005;32:199–211.
Florian J, Jadhav PR, Amur S, et al. Boceprevir dosing for late responders and null responders: the role of bridging data between treatment-naïve and -experienced subjects. Hepatology. 2013. https://doi.org/10.1002/hep.25843.
Fourie Zirkelbach J, Jackson AJ, Wang Y, et al. Use of partial AUC (PAUC) to evaluate bioequivalence—a case study with complex absorption: methylphenidate. Pharm Res. 2013. https://doi.org/10.1007/s11095-012-0862-x.
Huang SM, Abernethy DR, Wang Y, et al. The utility of modeling and simulation in drug development and regulatory review. J Pharm Sci. 2013;102:2912.
Lee JY, Wang Y. Use of a biomarker in exposure-response analysis to support dose selection for fingolimod. CPT Pharmacometrics Syst Pharmacol. 2013;2:1.
Sun W, Laughren TP, Zhu H, et al. Development of a placebo effect model combined with a dropout model for bipolar disorder. J Pharmacokinet Pharmacodyn. 2013;40:359.
Yang J, Zhao H, Garnett C, et al. The combination of exposure-response and case-control analyses in regulatory decision making. J Clin Pharmacol. 2013;53:160.
Younis IR, Laughren TP, Wang Y, et al. An integrated approach for establishing dosing recommendations: paliperidone for the treatment of adolescent schizophrenia. J Clin Psychopharmacol. 2013;33:152.
Liu J, Chan-Tack KM, Jadhav P, et al. Why did the FDA approve efavirenz 800 mg when co-administered with rifampin? Int J Clin Pharmacol Ther. 2014;52:446.
Ma L, Zhao L, Xu Y, et al. Clinical endpoint sensitivity in rheumatoid arthritis: modeling and simulation. J Pharmacokinet Pharmacodyn. 2014;41:537.
Dykstra K, Mehrotra N, Tornøe CW, et al. Reporting guidelines for population pharmacokinetic analyses. J Clin Pharmacol. 2015;42:301.
Khurana M, Vaidyanathan J, Marathe A, et al. Canagliflozin use in patients with renal impairment-utility of quantitative clinical pharmacology analyses in dose optimization. J Clin Pharmacol. 2015;55:647.
Lon HK, DuBois DC, Earp JC, et al. Modeling effects of dexamethasone on disease progression of bone mineral density in collagen-induced arthritic rats. Pharmacol Res Perspect. 2015;3:e00169.
Zhou D, Li H, Wang Y, et al. Quantitative characterization of circadian rhythm of pulmonary function in asthmatic patients treated with inhaled corticosteroids. J Pharmacokinet Pharmacodyn. 2015;42:391.
Mulugeta Y, Barrett JS, Nelson R, et al. Exposure matching for extrapolation of efficacy in pediatric drug development. J Clin Pharmacol. 2016;56:1326.
Yu J, Chung S, Zadezensky I, et al. Utility of exposure-response analysis in regulatory decision on the selection of starting dose of pasireotide for cushing disease. J Clin Pharmacol. 2016;56:1035.
Zhuang L, He Y, Xia H, et al. Gentamicin dosing strategy in patients with end-stage renal disease receiving haemodialysis: evaluation using a semi-mechanistic pharmacokinetic/pharmacodynamic model. J Antimicrob Chemother. 2016;71:1012.
Earp JC, Mehrotra N, Peters KE, et al. Esomeprazole FDA approval in children with GERD: exposure-matching and exposure-response. J Pediatr Gastroenterol Nutr. 2017;65:272.
Li L, Wang Y, Uppoor RS, et al. Exposure-response analyses of blood pressure and heart rate changes for methylphenidate in healthy adults. J Pharmacokinet Pharmacodyn. 2017;44:245.
Li H, Yu J, Liu C, et al. Time dependent pharmacokinetics of pembrolizumab in patients with solid tumor and its correlation with best overall response. J Pharmacokinet Pharmacodyn. 2017;44:403.
Li L, Zhang Y, et al. Exposure-response modeling and power analysis of components of ACR response criteria in rheumatoid arthritis (part 1: binary model). J Clin Pharmacol. 2017;57:1097.
Liu C, Yu J, Li H, et al. Association of time-varying clearance of nivolumab with disease dynamics and its implications on exposure-response analysis. Clin Pharmacol Ther. 2017;101:657.
Paterniti MO, Bi Y, Rekić D, et al. Acute exacerbation and decline in forced vital capacity are associated with increased mortality in idiopathic pulmonary fibrosis. Ann Am Thorac Soc. 2017;14:1395.
Chaikin P, Rhodes GR, Bruno R, et al. Pharmacokinetics/pharmacodynamics in drug development: an industrial perspective. J Clin Pharmacol. 2000;40:1428–38.
Reigner BG, Williams PE, Patel IH, et al. An evaluation of the integration of pharmacokinetic and pharmacodynamic principles in clinical drug development. Experience within Hoffmann La Roche. Clin Pharmacokinet. 1997;33:142–52.
Gieschke R, Steimer JL. Pharmacometrics: modelling and simulation tools to improve decision making in clinical drug development. Eur J Drug Metab Pharmacokinet. 2000;25:49–58.
Olson SC, Bockbrader H, Boyd RA, et al. Impact of population pharmacokinetic pharmacodynamic analyses on the drug development process: experience at Parke Davis. Clin Pharmacokinet. 2000;38:449–59.
Blesch KS, Gieschke R, Tsukamoto Y, et al. Clinical pharmacokinetic/pharmacodynamic and physiologically based pharmacokinetic modeling in new drug development: the capecitabine experience. Invest New Drugs. 2003;21:195–223.
Lockwood P, Ewy W, Hermann D, et al. Application of clinical trial simulation to compare proof of concept study designs for drugs with a slow onset of effect; an example in Alzheimer’s disease. Pharm Res. 2006;23:2050–9.
Peck CC, Barr WH, Benet LZ, et al. Opportunities for integration of pharmacokinetics, pharmacodynamics, and toxicokinetics in rational drug development. Clin Pharmacol Ther. 1992;51:465–73.
Noble D, Levin J, Scott W. Biological simulations in drug discovery. Drug Discov Today. 1999;4:10–6.
Lesko LJ, Rowland M, Peck CC, et al. Optimizing the science of drug development: opportunities for better candidate selection and accelerated evaluation in humans. Pharm Res. 2000;17:1335–44.
Drusano GL, Louie A, Deziel M, et al. The crisis of resistance: identifying drug exposures to suppress amplification of resistant mutant subpopulations. Clin Infect Dis. 2006;42:525–32.
Hutmacher MM, Mukherjee D, Kowalski KG, et al. Collapsing mechanistic models: an application to dose selection for proof of concept of a selective irreversible antagonist. J Pharmacokinet Pharmacodyn. 2005;32:501–20.
Danhof M. Systems pharmacology—towards the modeling of network interactions. Eur J Pharm Sci. 2016;30(94):4–14.
Mould DR, Upton RN. Basic concepts in population modeling, simulation, and model-based drug development—part 2: introduction to pharmacokinetic modeling methods. CPT: Pharm Syst Pharmacol. 2013;2:1–16.
Mould DR, Upton RN. Basic concepts in population modeling, simulation, and model-based drug development—part 3: introduction to pharmacodynamic modeling methods. CPT: Pharm Syst Pharmacol. 2014;3:1–18.
Ait-Oudhia S, Mager DE, Straubinger RM. Application of pharmacokinetic and pharmacodynamic analysis to the development of liposomal formulations for oncology. Pharmaceutics. 2014;6(1):137–74.
Jones H, Rowland-Yeo K. Basic concepts in physiologically based pharmacokinetic modeling in drug discovery and development. CPT Pharmacometrics Syst Pharmacol. 2013;2(8):e63.
U.S. Food and Drug Administration. Application of physiologically-based pharmacokinetic modeling to support dosing recommendations—the US Food and Drug Administration experience. 2016. https://www.ema.europa.eu/documents/presentation/presentation-application-physiologicallybased-pharmacokinetic-modeling-support-dosing_en.pdf. Accessed 22 Sept 2021.
Kimko H, Peck C. Clinical trial simulations: applications and trends. Berlin: Springer; 2011.
Liu X, Ward RM. Pharmacometrics in pediatrics. Ther Innov Regul Sci. 2019;53(5):579–83.
Bortz DM, Nelson PW. Model selection and mixed-effects modeling of HIV infection dynamics. Bull Math Biol. 2006;68:2005–25.
Pillai G, Gieschke R, Goggin T, et al. A semimechanistic and mechanistic population PK-PD model for biomarker response to ibandronate, a new bisphosphonate for the treatment of osteoporosis. Br J Clin Pharmacol. 2004;58(6):618–31.
Mostafavi S, Baranzini S, Oksernberg J, et al. Predictive modeling of therapy response in multiple sclerosis using gene expression data. Conf Proc IEEE Eng Med Biol Soc. 2006;1:5519–22.
Van der Helm-van Mil AH, le Cessie S, van Dongen H, et al. A prediction rule for disease outcome in patients with recentonset undifferentiated arthritis: how to guide individual treatment decisions. Arthritis Rheum. 2007;56:433–40.
Barton P, Jobanputra P, Wilson J, et al. The use of modelling to evaluate new drugs for patients with a chronic condition: the case of antibodies against tumor necrosis factor in rheumatoid arthritis. Health Technol Assess. 2004;8:1–91.
Winter W, DeJongh J, Post T, et al. A mechanism-based disease progression model for comparison of long-term effects of pioglitazone, metformin and gliclazide on disease processes underlying Type 2 diabetes mellitus. J Pharmacokinet Pharmacodyn. 2006;33:313–43.
Gaitonde PG, Chien JY, Schmidt S. Drug-systems-disease model to predict treatment-outcome in type 2 diabetes mellitus. Clin Pharmacol Ther. 2015;97:S40–1.
Hurtado FKG, Garhyan P, Chien JY, et al. Development of a mechanism-based drug-disease modeling platform for type 2 diabetes mellitus. Clin Pharmacol Ther. 2016;99:S37.
Srinvas N, Maffuid K, Kashuba ADM. Clinical pharmacokinetics and pharmacodynamics of drugs in the central nervous system. Clin Pharmacokinet. 2018;54:1059–74.
Conrado DJ, Nicholas T, Tsai K, et al. Dopamine transporter neuroimaging as an enrichment biomarker in early Parkinson’s disease clinical trials: a disease progression modeling analysis. Clin Transl Sci. 2018;11:63–70.
Romero K, Conrado D, Burton J, et al. Molecular neuroimaging of the dopamine transporter as a patient enrichment biomarker for clinical trials for early Parkinson’s disease. Clin Transl Sci. 2019;12:240–6.
Stephenson D, Hill D, Cedarbaum MJ, et al. The qualification of an enrichment biomarker for clinical trials targeting early stages of Parkinson’s disease. J Park Dis. 2019;9:553–63.
Burger D, Agarwala S, Child M, et al.: Effect of rifampin on steadystate pharmacokinetics of atazanavir and ritonavir in healthy subjects. In: 12th Conference on Retroviruses and Opportunistic Infections, Boston, MA, 22–25 Feb 2005.
Zamek-Gliszczynski MJ, Chu X, Polli JW, et al. Understanding the transport properties of metabolites: case studies and considerations for drug development. Drug Metab Dispos. 2014;42(4):650–64.
Zanger Ulrich M, Matthias S. Cytochrome P450 enzymes in drug metabolism: regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol Ther. 2013;138(1):103–41.
Li M, Zhu L, Chen L, et al. Assessment of drug–drug interactions between voriconazole and glucocorticoids. J Chemother. 2018;30(5):296–303.
Back D, Marzolini C. The challenge of HIV treatment in an era of polypharmacy. J Int AIDS Soc. 2020;23(2):e25449.
Marzolini C, Rajoli R, Battegay M, et al. Physiologically based pharmacokinetic modeling to predict drug–drug interactions with efavirenz involving simultaneous inducing and inhibitory effects on cytochromes. Clin Pharmacokinet. 2017;56(4):409–20.
Dong M, Fukuda T, Selim S, et al. Clinical trial simulations and harmacometrics analysis in pediatrics: application to inhaled loxapine in children and adolescents. Clin Pharmacokinet. 2017;56:1207–17.
van Hasselt JG, van Eijkelenburg NK, Beijnen JH, et al. Design of a drug-drug interaction study of vincristine with azole antifungals in pediatric cancer patients using clinical trial simulation. Pediatr Blood Cancer. 2014;61:2223–9.
Wharton GT, Murphy MD, Avant D, et al. Impact of pediatric exclusivity on drug labeling and demonstrations of efficacy. Pediatrics. 2014;134:e512–8.
Ward RM, Drover DR, Hammer GB, et al. The pharmacokinetics of methadone and its metabolites in neonates, infants, and children. Pediatr Anaesth. 2014;24:591–601.
Li M, Gehring R, Riviere JE, et al. Probabilistic physiologically based pharmacokinetic model for penicillin G in milk from dairy cows following intramammary or intramuscular administrations. Toxicol Sci. 2018;164(1):85–100.
Buur J, Baynes R, Smith G, et al. Use of probabilistic modeling within a physiologically based pharmacokinetic model to predict sulfamethazine residue withdrawal times in edible tissues in swine. Antimicrob Agents Chemother. 2006;2006(50):2344–51.
DeWoskin RS, Sweeney LM, Teeguarden JG, et al. Comparison of PBTK model and biomarker based estimates of the internal dosimetry of acrylamide. Food Chem Toxicol. 2013;58:506–21.
Henri J, Carrez R, Meda B, et al. A physiologically based pharmacokinetic model for chickens exposed to feed supplemented with monensin during their lifetime. J Vet Pharmacol Ther. 2017;40:370–82.
Lin Z, Li M, Gehring R, et al. Development and application of a multiroute physiologically based pharmacokinetic model for oxytetracycline in dogs and humans. J Pharm Sci. 2015;104:233–43.
Ho DD, Neumann AU, Perelson AS, et al. Rapid turnover of plasma virions and CD4 lymphocytes in HIV-1 infection. Nature. 1995;1995(373):123–6.
Perelson AS, Neumann AU, Markowitz M, et al. HIV-1 dynamics in vivo: virion clearance rate, infected cell life-span, and viral generation time. Science. 1996;271:1582–6.
Nowak MA, Bonhoeffer S, Shaw GM, et al. Anti-viral drug treatment: dynamics of resistance in free virus and infected cell populations. J Theor Biol. 1997;184:203–17.
Murray JM, Kaufmann G, Kelleher AD, et al. A model of primary HIV-1 infection. Math Biosci. 1998;154:57–85.
Kramer I. Modeling the dynamical impact of HIV on the immune system: viral clearance, infection, and AIDS. Math Comput Model. 1999;29:95–112.
Perelson AS, Nelson PW. Mathematical analysis of HIV-1 dynamics in vivo. SIAM Rev. 1999;41:3–44.
Wodarz D, Lloyd AL, Jansen VAA, et al. Dynamics of macrophage and T cell infection by HIV. J Theor Biol. 1999;196:101–13.
Stafford MA, Corey L, Cao Y, et al. Modeling plasma virus concentration during primary HIV infection. J Theor Biol. 2000;203:285–301.
Callaway DS, Perelson AS. HIV-1 infection and low steady state viral loads. Bull Math Biol. 2002;64:29–64.
Herz AVM, Bonhoeffer S, Anderson RM, et al. Viral dynamics in vivo: limitations on estimates of intracellular delay and virus decay. Proc Natl Acad Sci USA. 1996;93:7247–51.
Grossman Z, Feinberg M, Kuznetsov V, et al. HIV infection: how effective is drug combination treatment? Immunol Today. 1998;19:528–32.
Mittler JE, Sulzer B, Neumann AU, et al. Influence of delayed viral production on viral dynamics in HIV-1 infected patients. Math Biosci. 1998;152:143–63.
Nelson PW, Murray JD, Perelson AS. A model of HIV-1 pathogenesis that includes an intracellular delay. Math Biosci. 2000;163:201–15.
Nelson PW, Perelson AS. Mathematical analysis of delay differential equation models of HIV-1 infection. Math Biosci. 2002;179:73–94.
Lloyd AL. The dependence of viral parameter estimates on the asumed viral load life cycle: Limitations of studies of viral load data. Proc R Soc Lond Ser B. 2001;268:847–54.
Liu Stephanie N, Desta Z, et al. Probenecid-Boosted Tenofovir: a physiologically-based pharmacokinetic model-informed strategy for on-demand HIV preexposure prophylaxis. CPT Pharmacometrics Syst Pharmacol. 2019. https://doi.org/10.1002/psp4.12481.
Riggs MM, Cremers S. Pharmacometrics and systems pharmacology for metabolic bone diseases. Br J Clin Pharmacol. 2019;85(6):1136–46.
Post TM, Schmidt S, Peletier LA, et al. Application of a mechanism-based disease systems model for osteoporosis to clinical data. J Pharmacokinet Pharmacodyn. 2013;40(2):143–56.
Ross DS, Mehta K, Cabal A. Mathematical model of bone remodeling captures the antiresorptive and anabolic actions of various therapies. Bull Math Biol. 2017;79(1):117–42.
Cremers SCLM, Pillai G, Papapoulos SE. Pharmacokinetics/pharmacodynamics of bisphosphonates: use for harmacometr of intermittent therapy for osteoporosis. Clin Pharmacokinet. 2005;44(6):551–70.
Peterson MC, Riggs MM. A physiologically based mathematical model of integrated calcium homeostasis and bone remodeling. Bone. 2010;46(1):49–63.
Pivonka P, Zimak J, Smith DW, et al. Model structure and control of bone remodeling: a theoretical study. Bone. 2008;43(2):249–63.
Post TM, Freijer JI, DeJongh J, et al. Disease system analysis: basic disease progression models in degenerative disease. Pharm Res. 2005;22(7):1038–49.
Riggs M M, Gillespie W R, Gastonguay M R, et al. Extension of a multiscale model of calcium homeostasis and bone remodeling to include the progressive effects of estrogen loss during menopause transition [Conference presentation]. In: National Institute of General Medical Sciences, Quantitative and System Pharmacology Workshop II, Bethesda, MD, 9 September 2010.
Lien YTK, Madrasi K, Samant S, et al. Establishment of a disease-drug trial model for postmenopausal osteoporosis: a zoledronic acid case study. J Clin Pharmacol. 2020;60(2):86–102.
Kassahun K, McIntosh I, Koeplinger K, et al. Disposition and metabolism of the cathepsin K inhibitor odanacatib in humans. Drug Metab Dispos. 2014;42(5):818–27.
Zajic S, Stone JA, Jaworowicz D. Semi-mechanistic PK/PD model of the effect of odanacatib, a cathepsin K inhibitor, on bone turnover to characterize lumbar spine and distal forearm bone mineral density in a phase IIb study of postmenopausal women. PAGE Abstr Annu Meet Popul Approach Gr Eur. 2011;20:2190.
Zajic S, Rossenu S, Hreniuk D, et al. The absolute bioavailability and effect of food on the pharmacokinetics of odanacatib: a stable-label i.v./oral study in healthy postmenopausal women. Drug Metab Dispos. 2016;44(9):1450–8.
Ma B, Luo B, Euler DH, et al. Applicability of in vitro-in vivo translation of cathepsin K inhibition from animal species to human with the use of free-drug hypothesis. Naunyn Schmiedebergs Arch Pharmacol. 2017;390(4):435–41.
Gaitonde P, Hurtado FK, Garhyan P, et al. Development and qualification of a drug-disease modeling platform to characterize clinically relevant endpoints in type 2 diabetes trials. Clin Pharmacol Ther. 2018;104(4):699–708.
Mandema JW, Cox E, Alderman J. Therapeutic benefit of Eletriptan compared to Suma triptan for the acute relief of migraine pain results of a model based meta analysis that accounts for encapsulation. Cephalalgia. 2005;25:715–25.
Samtani M. Simple pharmacometric tools for oral anti diabetic drug development: competitive landscape for oral non insulin therapies in type 2 diabetes. Biopharm Drug Dispos. 2010;31:162–77.
Normand SL. Meta analysis: formulating, evaluating, combining, and reporting. Stat Med. 1999;18:321–59.
Berry DA, Berry SM, McKellar J, et al. Comparison of the dose response relation ships of 2 lipid lowering agents: a Bayesian meta analysis. Am Heart J. 2003;145:1036–45.
Heard RN. The spectrum of multiple sclerosis. Curr Allergy Asthma Rep. 2007;7:280–4.
Novakovic AM, Thorsted A, Schindler E, et al. Pharmacometric analysis of the relationship between absolute lymphocyte count and expanded disability status scale and relapse rate, efficacy end points, in multiple sclerosis trials. J Clin Pharmacol. 2018;58(10):1284–94.
Hu X, Hang Y, Cui Y, et al. Population-based pharmacokinetic and exposure-efficacy analyses of peginterferon beta-1a in patients with relapsing multiple sclerosis. J Clin Pharmacol. 2017;57(8):1005–16.
U.S. Food and Drug Administration. General clinical pharmacology considerations for pediatric studies for drugs and biological products—draft guidance for industry. 2014.
European Medicines Agency (EMA). Concept paper on extrapolation of efficacy and safety in medicine development. EMA. 2013. Accessed from https://www.ema.europa.eu/en/documents/scientific-guideline/concept-paper-extrapolation-efficacy-safety-medicine-development_en.pdf
Kearns GL, Abdel-Rahman SM, Alander SW, et al. Developmental pharmacology—drug disposition, action, and therapy in infants and children. N Engl J Med. 2003;349:1157–67.
Stockmann C, Barrett JS, Roberts JK, et al. Use of modeling and simulation in the design and conduct of pediatric clinical trials and the optimization of individualized dosing regimens. CPT Pharmacometrics Syst Pharmacol. 2015;4:630–40.
Vinks AA, Emoto C, Fukuda T. Modeling and simulation in pediatric drug therapy: application of pharmacometrics to define the right dose for children. Clin Pharmacol Ther. 2015;98:298–308.
Mehrotra N, Bhattaram A, Earp JC, et al. Role of quantitative clinical pharmacology in pediatric approval and labeling. Drug Metab Dispos. 2016;44(7):924–33.
Ogungbenro K, Aarons L, CRESim. A physiologically based pharmacokinetic model for clobazam and stiripentol in adults and children. Pharm Res. 2015;32:144–57.
Ogungbenro K, Aarons L, CRESim. Physiologically based pharmacokinetic modelling of methotrexate and 6-mercaptopurine in adults and children. Part 1: methotrexate. J Pharmacokinet Pharmacodyn. 2014;41:159–71.
Maharaj AR, Barrett JS, Edginton AN. A workflow example of PBPK modeling to support pediatric research and development: case study with lorazepam. AAPS J. 2013;15:455–64.
Jiang XL, Zhao P, Barrett JS, et al. Application of physiologically based pharmacokinetic modeling to predict acetaminophen metabolism and pharmacokinetics in children. CPT Pharmacometrics Syst Pharmacol. 2013;2:e80.
Leong R, Vieira MLT, Zhao P, et al. Regulatory experience with physiologically based pharmacokinetic modeling for pediatric drug trials. Clin Pharmacol Ther. 2012;91:926–31.
Life Science Leader. 2021. https://www.lifescienceleader.com/doc/why-animal-health-is-the-next-big-growth-area-0001. Accessed 14 Oct 2021
Li M, Gehring R, Riviere JE, Lin Z. Probabilistic physiologically based pharmacokinetic model for penicillin G in milk from dairy cows following intramammary or intramuscular administrations. Toxicol Sci. 2018;164(1):85–100.
Cox SR, Liao S, Payne-Johnson M, et al. Population pharmacokinetics of mavacoxib in osteoarthritic dogs. J Vet Pharmacol Ther. 2011;34(1):1–11.
European Medicines Agency (EMA). CVMP assessment report for CYTOPOINT (EMEA/V/C/003939/0000). 2017. Accessed from https://www.ema.europa.eu/en/documents/assessment-report/cytopoint-epar-public-assessment-report_en.pdf.
Ridker PM, Tardif JC, Amarenco P, et al. Lipid-reduction variability and antidrug-antibody formation with bococizumab. N Engl J Med. 2017;376(16):1517–26.
Jones HM, Zhang Z, Jasper P, et al. A physiologically-based pharmacokinetic model for the prediction of monoclonal antibody pharmacokinetics from in vitro data. CPT Pharmacometrics Syst Pharmacol. 2019;8(10):738–47.
Sahota T, Danhof M, Della PO. The impact of composite AUC estimates on the prediction of systemic exposure in toxicology experiments. J Pharmacokinet Pharmacodyn. 2016;42:251–61.
Tan Y-M, Worley RR, Leonard JA, et al. Challenges associated with applying physiologically based pharmacokinetic modeling for public health decision-making. Toxicol Sci. 2018;162(2):341–8.
Bonate PL. PK-PD Modeling and Simulation, 2nd Ed Allerheiligen, SRB. Clin Pharmacol Ther. 2014;96(4):413–5.
Acknowledgements
The authors would like to thank Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) and Pró-reitoria de Pesquisa Pós-graduação (PROPPI/UFOP) for providing financial support.
Author information
Authors and Affiliations
Contributions
LCB: Conceptualization, Data curation, Writing—original draft, review and editing; LP Co-supervision, Writing—review and editing; CMC: Writing—review and editing, Supervision, Funding acquisition, Project administration, Resources.
Corresponding author
Ethics declarations
Conflict of interest
Authors state no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Bandeira, L.C., Pinto, L. & Carneiro, C.M. Pharmacometrics: The Already-Present Future of Precision Pharmacology. Ther Innov Regul Sci 57, 57–69 (2023). https://doi.org/10.1007/s43441-022-00439-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43441-022-00439-4