
Abstract
Purpose
The purpose of this study was to examine peak torque (PT), mean power (MP), electromyographic (EMG) amplitude, mechanomyographic (MMG) amplitude, and neuromuscular efficiency from EMG and MMG amplitude (NMEEMG and NMEMMG, respectively) across the velocity spectrum in children versus adolescents.
Methods
Seventeen children (n = 8 males, n = 9 females) and 22 adolescents (n = 11 males, n = 11 females) participated. Participants completed maximal concentric isokinetic leg extensions at 60, 120, 180, 240 and 300°/s. PT, MP, EMG amplitude, and MMG amplitude were quantified during all muscle actions. NMEEMG and NMEMMG were quantified by expressing PT relative to EMG and MMG amplitude, respectively, for each muscle action.
Results
PT, MP, NMEEMG, and NMEMMG were greater for the adolescents than the children collapsed across sex and velocity (P ≤ 0.021). There were no significant differences for EMG amplitude (P ≥ 0.051), while MMG amplitude increased significantly from 60 to 240°/s (P < 0.001) then decreased significantly from 240 to 300°/s (P < 0.001) for all groups.
Conclusion
Overall, regardless of velocity, the expression of PT relative to EMG and MMG amplitude (NMEEMG and NMEMMG, respectively), in conjunction with measurements of torque and power production, may provide practitioners a unique method of examining growth and development-related augmentations in neuromuscular function during dynamic movements.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Many previous studies examining growth and development-related changes in muscle strength and power have utilized assessments of maximal and/or submaximal isometric strength [6, 7, 19, 24, 34, 39] or power production using vertical jump tests [21, 22, 32, 45]. However, several studies have suggested that the examination of muscle strength and power across a range of isokinetic velocities may provide unique insight regarding growth-mediated changes in muscle function [23, 27, 38, 42, 43]. In children and adolescents, previous studies have suggested that the ability to maintain high torque and power output across increases in isokinetic velocity may be reflective of muscular hypertrophy [38] or augmentations in neuromuscular function [23, 27, 38, 42, 43]. Most recently, Gillen et al. [23] reported that maximal isometric strength, but not muscle size, was able to fully account for the differences in isokinetic leg extension torque and power production between children and adolescents, concluding that augmentations in neuromuscular function may account for a large proportion of the differences in isokinetic strength and power between children and adolescents. However, we are aware of only two studies to noninvasively assess neuromuscular function during isokinetic muscle actions in healthy children and adolescents [42, 43].
Seger and Thorstensson [42, 43] assessed neuromuscular function in children during isokinetic muscle actions via surface electromyographic (EMG) recordings. Surface EMG represents the linear sum of the muscle fiber action potentials passing within the recording areas of the electrodes and represents the electrical component of neuromuscular control [20]. Seger and Thorstensson [42, 43] reported increases in EMG amplitude across velocity for pre-pubertal children, and greater absolute EMG amplitude for adults and post-pubertal adolescents compared to pre-pubertal children. Based on these findings [42, 43], muscle activation may increase with velocity in children, while adults have greater muscle activation capabilities than children regardless of velocity.
In addition to surface EMG, previous studies in adults [10,11,12,13, 17, 18], have suggested that examination of mechanomyographic (MMG) recordings, which records the low-frequency, lateral oscillations of the active skeletal muscle fibers representing the mechanical component of neuromuscular control [2, 40, 44], in conjunction with EMG recordings, may provide complimentary information regarding changes in neuromuscular function during isokinetic muscle actions. In adults, previous studies [11,12,13] have demonstrated velocity-related dissociations between MMG amplitude and peak torque (PT), but close relationships between MMG amplitude and mean power (MP) during isokinetic muscle actions, concluding that measurements of isokinetic PT and MP across the velocity spectrum may provide simple, practical assessments of neuromuscular function during isokinetic muscle actions. However, we are unaware of any previous studies to concurrently examine PT, MP, EMG amplitude, and MMG amplitude during isokinetic muscle actions in children and adolescents, which may provide clarifying information regarding the growth-mediated adaptations leading to increases in muscle strength and power during dynamic movements.
In addition to quantification of EMG and MMG amplitude, previous studies [16, 24, 31, 35] have suggested that unique information regarding the growth-mediated augmentations in neuromuscular function may be gained by calculating neuromuscular efficiency (NME), which reflects muscle strength relative to the activation of that muscle [15]. Several previous studies have utilized isometric muscle actions to provide growth-related comparisons of NME in children and adolescents [24, 25, 31], demonstrating growth and development-related increases in isometric NME. However, we are unaware of any previous studies to examine NME, from EMG or MMG amplitude, during isokinetic muscle actions in children and adolescents. Therefore, the purpose of this study was to concurrently examine PT, MP, EMG amplitude, MMG amplitude, and NME from EMG and MMG amplitude (NMEEMG and NMEMMG, respectively) across the isokinetic velocity spectrum in children versus adolescents.
Methods
Participants
Nineteen boys and 20 girls between the ages of 9–17-years-old volunteered for this study. Participants were categorized as either children if they were < 12-years-old or adolescent if they were ≥ 12-years-old [9, 23]. Participant demographics and categorizations are presented in Table 1. All participants reported participating in one or more sports for one to five hours per week during the year prior to this study. Sports included baseball, basketball, cheerleading, cross-country, football, gymnastics, lacrosse, rugby, soccer, softball, speed/power/agility training, swimming/diving, tennis, track and field, trap shooting, volleyball, weightlifting, and wrestling. Both the participant and their parent or legal guardian completed the PAR-Q+ 2015 [47] and were included in this study if questions 1–7 were answered “no” or all of the follow-up questions of the PAR-Q+ 2015 were answered “no.” This study was approved by the University of Nebraska-Lincoln Institutional Review Board for the protection of human subjects (IRB # 20171017495EP, title: Changes in noninvasive, applied physiological laboratory measurements and field measurements of athletic performance in children and youth: Influences of growth and development). Each subject signed the approved assent form if they were 7–18-years-old, while 5- and 6-year-olds verbally assented after being read an age-appropriate assent script, while one parent or legal guardian signed the approved consent form.
Research Design
Participants visited the laboratory twice, once for familiarization and once for the experimental trial. Familiarization and experimental trials were separated by 2–7 days and performed at approximately the same time of day (± 2 h). During each visit, participants performed two maximal voluntary isometric contractions (MVICs) at a leg flexion angle of 60° below the horizontal plane and three maximal voluntary concentric isokinetic muscle actions of the leg extensors at 60, 120, 180, 240 and 300°/s in random order. These velocities were chosen as previous studies have used this range of velocities to examine muscle function across varying velocities [10,11,12, 23]. Only data from the experimental trial are reported herein. Variables calculated during all isokinetic leg extensions included PT, MP, EMG amplitude, MMG amplitude, and NME from EMG and MMG amplitude (NMEEMG and NMEMMG, respectively).
Anthropometrics and Body Composition
Height (cm), seated height (cm), and body mass (kg) were measured using a digital scale and stadiometer (Seca 769, Hamburg, Germany). These variables were used to estimate maturity offset from peak height velocity [36]. Percent body fat was calculated from skinfold measurements taken with a Lange caliper (Model 68,902, Cambridge Scientific Industries, Inc., Cambridge, MD, USA). All skinfolds were taken on the right side of the body at the subscapular (diagonal fold immediately inferior to the interior angle of the scapula), triceps (vertical fold in the middle of the arm, midway between the acromion and olecranon process), and suprailiac (diagonal fold immediately superior to the anterior superior iliac spine) sites and were recorded to the nearest 0.5 mm [30]. Equations established by Housh et al. [29] and Brozek et al. [5] were used to estimate body density and percent body fat, respectively. Fat-free mass (FFM) was calculated as the difference between body mass and fat mass as determined by percent body fat.
Leg Extension Muscle Actions
All leg extension muscle actions were completed on a calibrated isokinetic dynamometer (Biodex System 3, Biodex Medical Systems, Inc., Shirley, NY, USA) that was custom fitted with a load cell (Omegadyne, model LCHD-500, 0–500 lbs, Stamford, CT, USA) located between the shin pad and the lever arm. Recorded force (N) was multiplied by the lever arm length (m) to calculate torque (N·m). Participants were seated with restraining straps over the pelvis, trunk, and contralateral thigh. The lateral epicondyle of the femur was aligned with the axis of rotation of the dynamometer head. All MVIC measurements were performed at a leg flexion angle of 60° below the horizontal plane. Each participant completed two, 4-s MVICs, with 1-min of rest between attempts. Participants were instructed to push against the lever arm as hard and fast as possible, while strong verbal encouragement was provided. Following the MVICs, the range of motion for the isokinetic muscle actions was set from 0° to 90°, with 0° representing full leg extension. Participants completed three repetitions of maximal voluntary isokinetic leg extension muscle actions at 60, 120, 180, 240 and 300°/s in random order, with 1-min of rest between each angular velocity. Each participant was instructed to extend their leg as hard and fast as possible, while strong verbal encouragement was provided. The order of the angular velocities was randomized separately for the familiarization and experimental trials.
Electromyography
Surface EMG signals were recorded from the vastus lateralis with pre-amplified, active electrodes (TSD150B, Biopac Systems, Inc., Santa Barbara, CA, USA) with a center-to-center interelectrode distance of 20 mm, gain of 330 (nominal), input impedance of 100 MΩ, common mode rejection ration of 95 dB (nominal), and bandwidth of 12–500 Hz. The electrode was placed at 66% of the distance between the anterior superior iliac spine and lateral border of the patella [28]. The longitudinal axis of the electrode was arranged parallel to the angle of pennation of the muscle fibers (20°) [24]. A reference electrode (EL503, Biopac Systems Inc., Santa Barbara, CA, USA) was placed over the tibial tuberosity. Placement sites for the EMG and MMG sensors were shaved and cleaned with isopropyl alcohol prior to application.
Mechanomyography
Surface MMG signals were detected from the vastus lateralis with an active miniature accelerometer (EGAS-S704-10_Rev C, Measurement Specialties, Inc., Hampton, VA; frequency response = 0–200 Hz, sensitivity = 655.1 mV/g, range = ± 10 g). Placement for the accelerometer was 50% of the distance between the anterior superior iliac spine and lateral border of the patella. The accelerometer was fixed to the skin using 3 M double-sided tape.
Signal Processing
During all isokinetic leg extension muscle actions, the position (°) and velocity (°/s) signals were sampled from the isokinetic dynamometer, while torque (N·m), EMG (μV), and MMG (m/s2) were sampled at 1 kHz with a Biopac data acquisition system (MP150, Biopac Systems, Inc., Santa Barbara, CA, USA). All signals were stored on a personal computer and processed off-line with custom written software (LabVIEW v. 17.0, National Instruments, Austin, TX). The torque-time signal was multiplied by the velocity–time signal to calculate the power-time signal. MMG signals were digitally filtered with a bandpass of 5–100 Hz. All subsequent analyses were performed on the filtered signals.
Isometric PT was taken as the highest 0.5-s average torque value during the plateau of the 4-s MVIC. Isokinetic PT was taken as the highest torque value during the selected epoch of each angular velocity. To determine the selected epoch, the load range was automatically determined during all isokinetic muscle actions from the onset to the end of the constant-velocity phase [4]. The onset of the isokinetic load range was automatically detected as the joint angle (°) at which the velocity signal had reached the pre-determined angular velocity. The end of the isokinetic load range was the joint angle (°) at which the velocity signal dropped below the pre-determined angular velocity. These start and end positions were used as the ranges of motion during which PT was taken during all angular velocities. During the automatic detections of each subject’s isokinetic load range, the investigator visually inspected the velocity- and position-time signals to ensure that an onset had not been falsely triggered and that the range of motion for all angular velocities was within the load range. The same epoch was taken from the power-velocity signal during each isokinetic muscle action to calculate MP, expressed as the average power during the selected epoch, while EMG amplitude and MMG amplitude were taken during the same epoch and expressed as root mean square. Normalized EMG and MMG amplitude during all isokinetic leg extensions were expressed relative the EMG and MMG amplitude, respectively, from the MVIC. To examine NME, PT was expressed relative to absolute EMG and MMG amplitude (NMEEMG and NMEMMG, respectively) as described previously [16, 24, 35, 37].
Statistical Analyses
Means and 95% confidence intervals of all participant demographics (Table 1) were calculated. Two-way factorial analyses of variance (ANOVAs) [sex (male vs. female) × group (children vs. adolescent)] were used to analyze age, maturity offset, height, body mass, and FFM. Three-way mixed factorial ANOVAS (sex [male vs. female] × group [ children vs. adolescent] x velocity [60°/s vs. 120°/s vs. 180°/s vs. 240°/s vs. 300°/s]) were used to analyze isokinetic PT and MP, normalized and absolute EMG amplitude, normalized and absolute MMG amplitude, NMEEMG, and NMEMMG. When appropriate, follow-up analyses included low-order ANOVAs and dependent samples t-tests with Bonferronni corrections.
Results
Age, height, body mass, FFM, and MVIC PT were greater in the adolescents than children (P ≤ 0.003, Table 1). The female children had a greater maturity offset than the male children (P < 0.001), while the male adolescents had a greater maturity offset than the children (P < 0.001), and the female adolescents had a greater maturity offset than all groups (P < 0.001).
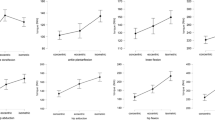
Isokinetic PT and MP were greater for the adolescents than the children across velocity (P ≤ 0.011, Fig. 1, Table 2). For the adolescents, PT decreased systematically across velocity (P ≤ 0.002, Fig. 1A, Table 2). For the children, PT decreased from 60–240°/s (P ≤ 0.041) then plateaued to 300°/s (P = 0.148, Fig. 1A, Table 2). For the adolescents, MP increased from 60–240°/s (P < 0.001) then plateaued to 300°/s (P = 0.054, Fig. 1B, Table 2). For the children, MP increased from 60 to 180°/s (P ≤ 0.007), plateaued from 180–240°/s (P ≥ 0.158), then decreased from 240 to 300°/s (P ≤ 0.007, Fig. 1B, Table 2).

Means ± 95% confidence intervals for A isokinetic peak torque across velocity, and B isokinetic mean power across velocity. *Indicates adolescents > children. For the adolescents, # indicates different than 60°/s, ## indicates different than 60 and 120°/s, ### indicates different than 60, 120, and 180°/s, and #### indicates different than 60, 120, 180, and 240°/s. For the children, $ indicates different than 60°/s, $$ indicates different than 60 and 120°/s, and $$$ indicates different than 60, 120, and 180°/s
There were no group-, sex-, or velocity-related differences for normalized or absolute EMG amplitude (P ≥ 0.051, Fig. 2A, Table 3), while normalized and absolute MMG amplitude increased from 60 to 240°/s (P < 0.001) then decreased from 240 to 300°/s (P ≤ 0.009, Fig. 2B, Table 3) collapsed across group and sex, while absolute MMG amplitude was greater for the adolescents than children at each velocity (P < 0.001, Table 3). Within the children, there were no sex-related differences for absolute MMG amplitude (P = 0.980, Table 3), while within the adolescents, absolute MMG amplitude was greater for the males compared to the females across velocity (P = 0.002, Table 3). NMEEMG and NMEMMG were greater for the adolescents than the children across sex and velocity (P ≤ 0.021, Fig. 2C and D, Table 3). NMEEMG decreased from 60–180°/s (P ≤ 0.014), then plateaued from 180 to 300°/s (P ≥ 0.245, Fig. 2C, Table 3), while NMEMMG decreased from 60 to 240°/s (P < 0.001) then plateaued to 300°/s (P = 0.949, Fig. 2D, Table 3) collapsed across group and sex.

Means ± 95% confidence intervals for A percent maximal voluntary isometric contraction (% MVIC) for electromyographic (EMG) amplitude across velocity, B % MVIC for mechanomyographic (MMG) amplitude across velocity, C neuromuscular efficiency (NME) from EMG amplitude across velocity, and D NME from MMG amplitude across velocity. *Indicates adolescents > children. + Indicates different from 60°/s, ++ indicates different from 60 and 120°/s, +++indicates different from 60, 120 and 180°/s, and ++++ indicates different from 60, 120, 180 and 300°/s
Discussion
To our knowledge, this is the first study to collectively compare PT, MP, EMG amplitude, MMG amplitude, NMEEMG, and NMEMMG during isokinetic muscle actions between children and adolescents. The main findings of this study demonstrated greater isokinetic PT, MP, NMEEMG, and NMEMMG for adolescents than children across velocity (Figs. 1 and 2, Tables 2 and 3). Furthermore, the velocity-related patterns for EMG and MMG amplitude were similar for children and adolescents (Figs. 2A and 2B, Table 3). However, when PT was expressed relative to EMG and MMG amplitude (NMEEMG and NMEMMG, respectively), differences between children and adolescents emerged (Figs. 2C and 2D, Table 3). Interestingly, as demonstrated previously [11, 13], 2004), velocity-related changes in MMG amplitude, NMEEMG, and NMEMMG seemed to closely track changes in MP across velocity (Figs. 1 and 2, Tables 2 and 3). In fact, a post hoc Pearson product moment correlation test revealed high significant relationships MP and these measures of neuromuscular function across all velocities (r = 0.353–0.843, P ≤ 0.028). Collectively, these findings demonstrate that augmentations in neuromuscular function may be influential on torque and power production across velocity during growth and development, and that isokinetic torque and power production may provide indirect assessments of neuromuscular function.
To our knowledge, only two studies have compared EMG amplitude during isokinetic muscle actions in children and adolescents [42, 43]. Seger and Thorstensson [42, 43] reported increases in EMG amplitude with increases in velocity using angular velocities ranging from 45 to 180°/s for pre-and post-pubertal males and females, suggesting this may reflect submaximal muscle activation due to central nervous system inhibition during low velocity, high tension conditions [42, 43]. In adults, previous studies have reported increases [10, 13, 42], decreases [1, 12], or no change [41] in EMG amplitude across a range of velocities from 30 to 480°/s. Additionally, in contrast to the present study, Seger and Thorstensson [42, 43] reported greater EMG amplitude in adults and post-pubertal children compared to pre-pubertal children. This discrepancy previous results and the present study may be due to methodological differences as Seger and Thorstensson [42, 43] quantified absolute EMG amplitude, while the present study quantified normalized EMG amplitude per previous recommendations [33]. Interestingly, in the present study there were no sex, group, or velocity-related differences in absolute EMG amplitudes, which emphasizes the importance of the normalization procedure to provide consistency across studies in reporting these data. The inconsistent results between the present study and previous studies in adults and children [1, 10, 12, 13, 41,42,43] may reflect differences among the muscle or muscle group involved, different ranges of motion, and/or the range of isokinetic velocities used. Although several previous studies have examined the muscles of the quadriceps femoris, differences in the velocities chosen, muscle action performed (concentric vs. eccentric), or range of motion used may alter the neuromuscular responses. Therefore, future studies should determine the optimal methodology to examine velocity-related responses of the EMG signal to provide greater consistency in the methods used.
In the present study, there were no differences for MMG amplitude between groups (Fig. 2B). Furthermore, MMG amplitude increased from 60 to 240°/s for both groups (Fig. 2B), which closely resembled the velocity-related responses for MP. Previous studies in adults [10,11,12,13, 17, 18], have reported similar findings, with MMG amplitude and MP increasing to approximately 240°/s, and plateauing or decreasing with further increases in angular velocity. It is possible that the velocity-related increases in MMG amplitude may reflect changes in low- versus high-threshold motor unit contributions to torque production, subsequently decreasing muscle stiffness [10,11,12,13, 17, 18]. Theoretically, when velocity increases there is a shift in the contribution of torque production from low- plus high-threshold motor units at low velocities to primarily high-threshold motor units at higher velocities. Thus, at higher velocities, the unloading of low-threshold motor units results in less torque production and reduced muscle stiffness, which increases muscle fiber oscillations and, subsequently, MMG amplitude. Therefore, it is possible that the velocity-related patterns for MMG amplitude may reflect decreases in muscle stiffness across increasing velocity for children and adolescents due to changes in motor unit contributions.
Although there were no apparent group-related differences for EMG and MMG amplitude, previous studies have suggested that comparisons of PT relative to absolute EMG or MMG amplitude (NMEEMG and NMEMMG, respectively) provides unique information regarding the potential neural contributions to differences in muscle strength. DeVries [16] suggested that increases in NME with concurrent increases in muscle strength may reflect muscle fibers becoming more effective at producing tension or the same motor units being activated at a lower stimulation threshold. Additionally, Milner-Brown et al. [35] suggested that NME quantifies excitation–contraction coupling, indicating that increases in NME reflect decreases in the action potential threshold necessary to result in force production. Few studies have quantified NMEEMG in children and adolescents [25, 31], and only one study we are aware of has quantified NMEMMG in this population [24]. Grosset et al. [25] and Lambertz et al. [31] reported age-related increases in NMEEMG ranging from 69 to 207% across 7–11-year-old children. Furthermore, in comparing preadolescent and adolescent males and females Gillen et al. [24] reported 74%–81% greater NMEEMG for adolescents and 31%–139% greater NMEMMG for adolescents. However, none of these studies examined NME during dynamic, isokinetic muscle actions. In the present study, the adolescents achieved 78%–138% greater NMEEMG and 12%–46% greater NMEMMG than the children across velocity (Fig. 2C and D). Thus, in conjunction with previous studies [16, 25, 31, 35], it is possible that the adolescents may have a lower action potential threshold necessary to result in torque production during maximal isokinetic muscle actions.
Furthermore, the velocity-related patterns for NMEEMG and NMEMMG tracked closely to the velocity-related patterns for MP and MMG amplitude. Previous studies in adults have demonstrated similar velocity-related responses for MP and MMG amplitude [10,11,12,13, 17, 18]. To describe the close relationship between MMG amplitude and MP, Bodor [3] used the analogy of playing a violin such that the amplitude of the violin string can be increased either by increasing the force applied to the bow, increasing the bowing velocity, or both. Thus, a change in the power applied to the violin strings results in an increase in the amplitude or sound volume generated by the violin, demonstrating the proportional relationship between power and amplitude. Although this has been demonstrated previously in adults for the relationship between MP and MMG amplitude [10,11,12,13, 17, 18], we are unaware of any previous studies in adults, adolescents, or children, that demonstrated this same, yet inverse, relationship between NME, whether from EMG or MMG amplitude, and MP during isokinetic muscle actions. Collectively, the responses of NMEEMG and NMEMMG may similarly reflect the offloading of low-threshold motor units during higher-velocity muscle actions, which necessarily would require greater energy contribution from high-threshold motor units. Specifically, high-threshold motor units tend to have lower motor unit firing frequencies than low-threshold motor units [8, 14, 46], which is thought to optimize the relationship between force production and the duration of motor unit activity [14, 46], termed the “Onion-Skin scheme.” One of the guiding principles of the “Onion-Skin Scheme” is the minimization of energy expenditure through reliance on low-threshold motor units, which are less fatigable [14, 46]. In the present study, at the fastest velocities (240°/s and 300°/s), where NME was the lowest, isokinetic PT only reflected 43%–53% of PT during the MVIC. Previous studies [8, 14, 46] have demonstrated that, during isometric contractions (zero velocity), low-threshold motor units tend to contribute more to force production between 40% and 50% of MVIC. Thus, perhaps due to the offloading of low-threshold motor units during fast-velocity, lower intensity dynamic muscle actions [12, 26, 27], high-threshold motor units must disproportionately contribute to energy production to maintain torque and power production at faster velocities with fewer motor units, leading to decreases in the efficiency of neuromuscular recruitment.
In conclusion, the main findings of this study demonstrated greater PT, MP, NMEEMG, and NMEMMG for adolescents than children regardless of velocity. In conjunction with the findings of previous studies [24, 25, 31], the group-related differences in NME, whether from EMG or MMG amplitude, provide evidence that changes in muscle strength and power during dynamic muscle actions from childhood to adolescence may be at least partially mediated by the underlying neuromuscular adaptations that occur during growth and development. Overall, regardless of velocity, the expression of PT relative to EMG and MMG amplitude (NMEEMG and NMEMMG, respectively), in conjunction with measurements of isokinetic torque and power production, may provide practitioners a unique method of examining growth and development-related augmentations in neuromuscular function. Therefore, further examination of muscle strength, power, and neuromuscular efficiency during dynamic muscle actions may provide a greater understanding of the underlying mechanisms leading to increases in muscle strength and power across growth and development.
Availability of Data and Materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Code Availability
The custom-written software of this study is available from the corresponding author upon reasonable request.
References
Barnes WS. The relationship of motor-unit activation to isokinetic muscular contraction at different contractile velocities. Phys Ther. 1980;60(9):1152–8. https://doi.org/10.1093/ptj/60.9.1152.
Barry D, Cole N. Muscle sounds are emitted at the resonant frequencies of skeletal muscle. IEEE Trans Biomed Eng. 1990;37(5):525–31.
Bodor M. Mechanomyographic and electromyographic muscle responses are related to power. Muscle Nerve. 1999;22(5):649–50. https://doi.org/10.1002/(sici)1097-4598(199905)22:5%3c649::aid-mus18%3e3.0.co;2-f.
Brown L, Whitehurst M, Findley B. Reliability of rate of velocity development and phase measures on an isokinetic device. J Strength Cond Res. 2005;19(1):189–92. https://doi.org/10.1519/R-15004.1.
Brozek J, Grande F, Anderson J, Keys A. Densiometric analysis of body composition: revision of some quantitative assumptions. Ann N Y Acad Sci. 1963;110:113–40.
Chalchat E, Piponnier E, Bontemps B, Julian V, Bocock O, Duclos M, Ratel S, Martin V. Characteristics of motor unit recruitment in boys and men at maximal and submaximal force levels. Exp Brain Res. 2019;237(5):1289–302.
Cohen R, Klentrou P, Gabriel D, Gabriel D, Klentrou P, Falk B. Do neuromuscular adaptations occur in endurance-trained boys and men? Appl Phys Nutr Metab. 2010;35(4):471–9. https://doi.org/10.1139/H10-031.
Contessa P, De Luca CJ. Neural control of muscle force: indications from a simulation model. J Neurophysiol. 2013;109(6):1548–70. https://doi.org/10.1152/jn.00237.2012.
Centers for Disease Control and Prevention. CDC Learn About Child Development. 2019. https://www.cdc.gov/ncbddd/childdevelopment/index.html. Accessed 23 Oct 2019.
Cramer JT, Housh TJ, Johnson GO, Ebersole KT, Perry SR, Bull AJ. Mechanomyographic and electromyographic responses of the superficial muscles of the quadriceps femoris during maximal, concentric isokinetic muscle actions. Isokinet Exerc Sci. 2000;8(2):109–17. https://doi.org/10.3233/IES-2000-0041.
Cramer JT, Housh TJ, Johnson GO, Ebersole KT, Perry SR, Bull AJ. Mechanomyographic amplitude and mean power output during maximal, concentric, isokinetic muscle actions. Muscle Nerve. 2000;23(12):1826–31. https://doi.org/10.1002/1097-4598(200012)23:12%3c1826::AID-MUS5%3e3.0.CO;2-7.
Cramer JT, Housh TJ, Weir JP, Johnson GO, Berning JM, Perry SR, Bull AJ. Gender, muscle, and velocity comparisons of mechanomyographic and electromyographic responses during isokinetic muscle actions. Scand J Med Sci Sports. 2004;14(2):116–27. https://doi.org/10.1111/j.1600-0838.2003.00317.x.
Cramer JT, Housh TJ, Weir JP, Johnson GO, Ebersole KT, Perry SR, Bull AJ. Power output, mechanomyographic, and electromyographic responses to maximal, concentric, isokinetic muscle actions in men and women. J Strength Cond Res. 2002;16(3):399–408. https://doi.org/10.1519/00124278-200208000-00010.
De Luca CJ, Contessa P. Biomechanical benefits of the onion-skin motor unit control scheme. J Biomech. 2015;48(2):195–203. https://doi.org/10.1016/j.jbiomech.2014.12.003.
Deschenes MR, Giles JA, McCoy RW, Volek JS. Neural factors account for strength decrements observed after short-term muscle unloading. Am J Physiol Regul Integr Comp Physiol. 2002;282(2):578–83. https://doi.org/10.1152/ajpregu.00386.2001.
DeVries HA. “Efficiency of electrical activity” as a physiological measure of the functional state of muscle tissue. Am J Phys Med. 1968;47(1):11–22.
Ebersole KT, Housh TJ, Weir JP, Johnson GO, Evetovich TK, Smith DB. The effects of leg angular velocity on mean power frequency and amplitude of the mechanomyographic signal. Electromyogr Clin Neurophysiol. 2000;40(1):49–55.
Evetovich TK, Housh TJ, Johnson GO, Smith DB, Ebersole KT, Perry SR. Gender comparisons of the mechanomyographic responses to maximal concentric and eccentric isokinetic muscle actions. Med Sci Sports Exerc. 1998;30(12):1697–702. https://doi.org/10.1097/00005768-199812000-00007.
Falk B, Usselman C, Dotan R, Brunton L, Klentrou P, Shaw J, Gabriel D. Child-adult differences in muscle strength and activation pattern during isometric elbow flexion and extension. Appl Physiol Nutr Metab. 2009;34(4):609–15. https://doi.org/10.1139/H09-020.
Farina D, Merletti R, Enoka RM. The extraction of neural strategies from the surface EMG. J Appl Physiol. 2004;96(4):1486–95. https://doi.org/10.1152/japplphysiol.01070.2003.
Gillen ZM, Jahn LE, Shoemaker ME, McKay BD, Mendez AI, Bohannon NA, Cramer JT. Effects of eccentric preloading on concentric vertical jump performance in youth athletes. J Appl Biomech. 2019;35(5):327–35. https://doi.org/10.1123/jab.2018-0340.
Gillen ZM, Shoemaker ME, Bohannon NA, Gibson SM, Cramer JT. Effects of eccentric pre-loading on concentric vertical jump performance in young female athletes. J Sci Sport Exerc. 2021;3(1):98–106. https://doi.org/10.1007/s42978-020-00098-7.
Gillen ZM, Shoemaker ME, Bohannon NA, Gibson SM, Cramer JT. Comparing the torque- and power-velocity relationships between children and adolescents during isokinetic leg extension muscle actions. Hum Mov Sci. 2020;74:102678. https://doi.org/10.1016/j.humov.2020.102678.
Gillen ZM, Shoemaker ME, McKay BD, Bohannon NA, Gibson SM, Cramer JT. Muscle strength, size, and neuromuscular function before and during adolescence. Eur J Appl Physiol. 2019;119(7):1619–32. https://doi.org/10.1007/s00421-019-04151-4.
Grosset JF, Mora I, Lambertz D, Pérot C. Voluntary activation of the triceps surae in prepubertal children. J Electromyogr Kinesiol. 2008;18(3):455–65. https://doi.org/10.1016/j.jelekin.2006.11.002.
Gür H, Gransberg L, vanDyke D, Knutsson E, Larsson L. Relationship between in vivo muscle force at different speeds of isokinetic movements and myosin isoform expression in men and women. Eur J Appl Physiol. 2003;88(6):487–96. https://doi.org/10.1007/s00421-002-0760-8.
Herda TJ, Ryan ED, Kohlmeier M, Trevino MA, Gerstner GR, Roelofs EJ. Examination of muscle morphology and neuromuscular function in normal weight and overfat children aged 7–10 years. Scand J Med Sci Sports. 2018;28(11):2310–21. https://doi.org/10.1111/sms.13256.
Hermens HJ. SENIAM 8: European recommendations for surface electromyography. 2nd ed. Enschede: Roessingh Research and Development; 1999.
Housh TJ, Johnson GO, Housh DJ, Stout JR, Eckerson JM. Estimation of body density in young wrestlers. J Strength Cond Res. 2000;14(4):477–82.
Jackson AS, Pollock ML. Practical assessment of body composition. Phys Sportsmed. 1985;13(5):76–90. https://doi.org/10.1080/00913847.1985.11708790.
Lambertz D, Mora I, Grosset J-F, Pérot C. Evaluation of musculotendinous stiffness in prepubertal children and adults, taking into account muscle activity. J Appl Physiol. 2003;95(1):64–72. https://doi.org/10.1152/japplphysiol.00885.2002.
Lloyd RS, Oliver JL, Hughes MG, Williams CA. Age-related differences in the neural regulation of stretch–shortening cycle activities in male youths during maximal and sub-maximal hopping. J Electromyogr Kinesiol. 2012;22(1):37–43. https://doi.org/10.1016/j.jelekin.2011.09.008.
Merletti R. Standards for reporting EMG data. J Electromyogr Kinesiol. 2014;24(2):I–II. https://doi.org/10.1016/S1050-6411(14)00042-X.
Miller JD, Sterczala AJ, Trevino MA, Wray ME, Dimmick HL, Herda TJ. Motor unit action potential amplitudes and firing rates during repetitive muscle actions of the first dorsal interosseous in children and adults. Eur J Appl Physiol. 2019;119(4):1007–18. https://doi.org/10.1007/s00421-019-04090-0.
Milner-Brown HS, Mellenthin M, Miller RG. Quantifying human muscle strength, endurance and fatigue. Arch Phys Med Rehabil. 1986;67(8):530–5.
Mirwald RL, Baxter-Jones ADG, Bailey DA, Beunen GP. An assessment of maturity from anthropometric measurements. Med Sci Sports Exerc. 2002;34(4):689–94. https://doi.org/10.1097/00005768-200204000-00020.
Moritani T, DeVries HA. Neural factors versus hypertrophy in the time course of muscle strength gain. Am J Phys Med. 1979;58(3):115–30.
O’Brien TD, Reeves ND, Baltzopoulos V, Jones DA, Maganaris CN. Strong relationships exist between muscle volume, joint power and whole-body external mechanical power in adults and children. Exp Physiol. 2009;94(6):731–8. https://doi.org/10.1113/expphysiol.2008.045062.
O’Brien TD, Reeves ND, Baltzopoulos V, Jones DA. In vivo measurements of muscle specific tension in adults and children. Exp Physiol. 2010;95(1):202–10. https://doi.org/10.1113/expphysiol.2009.048967.
Orizio C. Muscle sound: bases for the introduction of a mechanomyographic signal in muscle studies. Crit Rev Biomed Eng. 1993;21(3):201–43.
Rothstein JM, Delitto A, Sinacore DR, Rose SJ. Electromyographic, peak torque, and power relationships during isokinetic movement. Phys Ther. 1983;63(6):926–33. https://doi.org/10.1093/ptj/63.6.926.
Seger JY, Thorstensson A. Muscle strength and myoelectric activity in prepubertal and adult males and females. Eur J Appl Physiol Occup Physiol. 1994;69(1):81–7. https://doi.org/10.1007/BF00867932.
Seger JY, Thorstensson A. Muscle strength and electromyogram in boys and girls followed through puberty. Eur Appl Physiol Occup Physiol. 2000;81(1–2):54–61. https://doi.org/10.1007/PL00013797.
Stokes MJ, Dalton PA. Acoustic myography: applications and considerations in measuring muscle performance. Isokinet Exerc Sci. 1993;3(1):4–15. https://doi.org/10.3233/IES-1993-3101.
Suchomel TJ, Sands WA, McNeal JR. Comparison of static, countermovement, and drop jumps of the upper and lower extremities in U.S. junior national team male gymnasts. Sci Gymnast J. 2016;8(1):15–30.
Trevino MA, Herda TJ, Fry AC, Gallagher PM, Vardiman JP, Mosier EM, Miller JD. Influence of the contractile properties of muscle on motor unit firing rates during a moderate-intensity contraction in vivo. J Neurophysiol. 2016;116(2):552–62. https://doi.org/10.1152/jn.01021.2015.
Warburton DER, Jamnik V, Bredin SSD, Shephard RJ. The 2015 physical activity readiness questionnaire for everyone (PAR-Q+) and electronic physical activity readiness medical examination (ePARmed-X+). Health Fit J Can. 2015;8:53–6. https://doi.org/10.14288/hfjc.v8i1.194.
Acknowledgements
Efforts for this study were funded, in part, by the University of Nebraska Agriculture Research Division with funds provided by the Hatch Act (Agency: U.S. Department of Agriculture, National Institute of Food and Agriculture; Accession No: 1000080; Project No: NEB-36-078) and a grant from Abbott Nutrition, Columbus, OH.
Funding
Efforts for this study were funded, in part, by the University of Nebraska Agriculture Research Division with funds provided by the Hatch Act (Agency: U.S. Department of Agriculture, National Institute of Food and Agriculture; Accession No: 1000080; Project No: NEB-36–078) and a grant from Abbott Nutrition, Columbus, OH.
Author information
Authors and Affiliations
Contributions
ZMG was a substantial contributor to the study concept and design, carried out data acquisition, analysis, and interpretation, and wrote the manuscript. MES contributed to data acquisition and manuscript revision. JTC was the primary manuscript reviser and a substantial contributor to the study concept, design, and interpretation. All authors provided critical feedback and approved the final version of the manuscript. All persons designated as authors qualify for authorship, and all those who qualify for authorship are listed. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflict of interests
The authors have no relevant financial or non-financial interests to disclose.
Ethical Approval
This study was approved by the University of Nebraska-Lincoln’s Institutional Review Board (IRB) for the protection of human subjects (IRB # 20171017495EP, title: Changes in noninvasive, applied physiological laboratory measurements and field measurements of athletic performance in children and youth: Influences of growth and development).
Consent to Participate
Before any data collection, each subject signed the approved assent form if they were 7–18-years-old, while 5- and 6-year-olds verbally assented after being read an age-appropriate assent script, while one parent or legal guardian signed the approved consent form. Each subject, with the assistance from their parent or legal guardian, completed the PAR-Q+ 2015 and was included in this study if questions 1–7 were answered “no” or all of the follow-up questions of the PAR-Q+ 2015 were answered “no.”
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Gillen, Z.M., Shoemaker, M.E. & Cramer, J.T. Electromyographic and Mechanomyographic Responses During Isokinetic Leg Extensions in Children Versus Adolescents. J. of SCI. IN SPORT AND EXERCISE 5, 226–235 (2023). https://doi.org/10.1007/s42978-022-00193-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42978-022-00193-x