
Abstract
Youth may be particularly responsive to motor learning training strategies that support injury-resistant movement mechanics in youth for prevention programs that reduce injury risk, injury rehabilitation, exercise performance, and play more generally (Optimizing Performance Through Intrinsic Motivation and Attention for Learning Prevention Rehabilitation Exercise Play; OPTIMAL PREP) One purpose of the present manuscript was to provide clinical applications and tangible examples of how to implement the proposed techniques derived from OPTIMAL theory into PREP strategies for youth. A secondary purpose was to review recent advances in technology that support the clinical application of OPTIMAL PREP strategies without extensive resources/programming knowledge to promote evidence-driven tools that will support practitioner feedback delivery. The majority of examples provided are within the context of anterior cruciate ligament (ACL) injury rehabilitation, but we emphasize the potential for OPTIMAL PREP strategies to be applied to a range of populations and training scenarios that will promote injury resistance and keep youth active and healthy.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Participating in sports at an early age is attributed to numerous physical and psychosocial benefits that support long-term neuromotor development [30, 36, 54, 57, 59, 88], with youth being a particularly ideal time period to implement exercise-based interventions [9, 55,56,57,58, 60,61,62, 65, 72, 78]. The OPTIMAL theory of motor learning (Optimizing Performance Through Intrinsic Motivation and Attention for Learning) [123] proposes three "pillars"—two motivational (enhanced expectancies, autonomy support) and one attentional (external focus of attention)—that may support youth injury prevention strategies (reduction of injury risk), injury rehabilitation, exercise performance, and play more generally (Prevention, Rehabilitation, Exercise, Play; PREP) [24, 25]. Implementation of OPTIMAL PREP training strategies is further theorized to promote the long-term retention of injury-resistant motor control by capitalizing youth’s heightened central nervous system (CNS) plasticity and potential for neuro-mechanistically-targeted treatments to promote positive neuromotor adaptations [24, 25].
To facilitate the translation of theory to clinical practice, one purpose of the present manuscript is to provide clinical applications and tangible examples of how to implement the proposed OPTIMAL PREP strategies for youth. Historically, these principles have been delivered via verbal augmented feedback or "instruction-based" methods with or without the inclusion of simple visual feedback. An example of this is a cone being placed in front of a patient to focus on and jump towards in an effort to promote an external focus of attention. Prior approaches to feedback delivery has, in part, been due to technological constraints associated with the automated delivery of more complex, augmented biofeedback, as these methods have been limited to expensive laboratory environments and necessitated high levels of expertise, such as visual displays of computer-generated geometric shapes that respond in real-time to patients’ movement mechanics (deemed "technology-based" herein). Thus, a secondary purpose of the present manuscript is to review recent advances in technology that support the clinical application of OPTIMAL PREP strategies without extensive resources or programming knowledge to reduce the burden of clinicians providing the most appropriate instruction-based verbal feedback. Throughout the manuscript a brief summary of behavioral literature supporting the application of OPTIMAL theory is provided, but we direct the reader to a more thorough review of the extant literature and definitions of potentially unfamiliar terminology [25]. Of note, we provide most examples within the context of patients following ACL reconstruction (ACLR) and undergoing rehabilitation, but emphasize that OPTIMAL PREP strategies can be applied across the spectrum of youth ages—in both males and females—ranging from pre-adolescence (~ 6 years of age) to early adulthood (~ 25 years of age) [24, 25]. Importantly, we emphasize OPTIMAL PREP strategies could also be beneficial for youth with and without musculoskeletal-related conditions and are applicable to a wide range of training scenarios including injury prevention programs for further reduced risk, injury rehabilitation, and exercise performance/general play more broadly [24, 25].
Enhanced Expectancies and Clinical Applications Using Instruction-Based Feedback
Enhancing expectancies refers to boosting an individual’s sense of confidence and "expectations to succeed in the future", which, in turn, can better prepare the performer for action. Enhancing patient expectancies can be achieved by using positive/social-comparative feedback, which enhances conceptions of personal ability and reduces perceived task difficulty [123]. In turn, improved patient self-efficacy, confidence/motivation, and expectation for success can contribute to enhanced motor behavior. Furthermore, enhanced expectancies can even facilitate movement efficency [104]; this is particularly relevant to ACL injury, as maladaptive (or less efficient) neuromuscular function has been observed [17, 111] and deemed a precursor to secondary injury risk [46, 83]. ACL injury can also lead to fear of (re)injury—the most commonly cited reason among athletes who do not return to play [76]—potentially leading to increased muscular tension, fatigue, decreased coordination, and as a result, higher vulnerability to future injury [3]. As these psychological factors regarding perceived ability are critical for an athlete’s successful return to sport [66, 86], it is noteworthy that enhancing expectancies can improve self-efficacy [7, 8] and could potentially reduce fear of (re)injury.
Practitioners, used herein to be inclusive of researchers, clinicians, coaches, instructors, physical therapists, athletic trainers, certified strength and conditioning specialists, teammates, etc., can enhance expectancies within OPTIMAL PREP training applications to promote injury-resistant movement. Specifically, positive feedback can seamlessly be provided following good repetitions or the patient’s most effective repetitions (e.g. following the back squat: “Your knee alignment has significantly improved from last week’s session”). Likewise, social-comparative feedback is also easily implementable and favorably juxtaposes the patient’s current performance with normative performances of others performing the same task. However, this feedback should not be framed in a manner that would allow immediate peers and teammates to become aware of such negative social comparisons, or at least used with caution and with consideration of how it may influence the mindset of a given athlete [24] (e.g., “Your performance on this task is well above average”). Self-modeling can also be achieved using videos where a clinician displays to the patient their previous success, such as a pre-injury video of the patient performing a successful movement during rehabilitation. Self-modeling can also be achieved by providing videos of models who identify to the patient, such as an athlete from the same sport who experienced an injury describing their personal barriers and achievements during pre- and post-operative recovery. For example, self-modeling has been used to promote a current patient’s self-efficacy while also reducing pain [63] and can reduce biomechanics associated with ACL injury risk [87].
Lastly, participants’ confidence can even be raised by reducing perceptions of task difficulty and/or providing fake positive feedback. However, fake positive feedback must be "purposeful", such that it does not induce a level of confidence that exceeds an individuals’ physical capability, potentially exposing them to greater injury risk [24]. For instance, during a single leg hop a clinician could safely place a cone at a distance perceived as "easy" to reach by the patient to enhance self-efficacy before increasing the perceived distance the patient strives to jump to. As an illustrative example with respect to youth play, instructors could even adopt the "Ebbinghaus Illusion" that can enhance self-efficacy and motor behavior by making targets appear larger than they actually are [7, 8, 19, 82]. For instance, this principle could be used in youth by creating "perceptually larger targets" an athlete must kick a soccer ball towards; small objects could surround a goal target to make it appear larger. Notably, many sports performance examples likely will not induce injury risk, but careful consideration of purposeful expectancies are necessary in many medical scenarios and patient safety should be considered as to not induce a false sense of ability that could increase injury-risk behavior [24]. We provide a few more specific examples within the context of ACL injury rehabilitation in Table 1.
Autonomy Support and Clinical Applications Using Instruction-Based Feedback
Autonomy support refers to providing learners a degree of self-control which can positively influence self-efficacy/motivation to enhance motor performance and learning [20, 49, 52, 99, 116]. Autonomy support can be provided through numerous means, including control over individual practice conditions, instructional feedback that bolsters feelings of self-control, and allowing patients numerous opportunities for choices, with even just one choice potentially being beneficial. Like enhanced expectancies, conditions that support one’s need for autonomy can also target neuromuscular activity [47, 48] and potentially serve as an adjunctive therapy for restoration of neuromuscular deficits associated with ACLR [84, 109]. For instance, two studies demonstrated that participants who were allowed to choose when to receive feedback following a series of drop landing tasks exhibited biomechanics associated with reduced ACL injury risk during retention and transfer tests [11, 112].
Practitioners can easily provide individuals with opportunities for control during OPTIMAL PREP scenarios without compromising daily goals and/or prescribed clinical care. For instance, simply asking individuals the order in which they want to do exercises (e.g., “Do you want to perform the double leg squat or leg extension exercise first?”), allowing them to choose when they receive feedback (e.g., “Please let me know when you would like to receive feedback on your squatting technique”), or providing them opportunities to choose when they rest and/or for how long they rest are all easily implementable methods of providing autonomy support. Practitioners can provide motivation-boosting, autonomy-supportive language rather than negatively perceived controlling statements (e.g., “What exercise would you like to work on next week?” vs. “Your exercise next week will be…”). Likewise, when feedback about mechanics is required to ensure safety during particularly high-risk, dynamic exercises such as unanticipated cutting [69,70,71, 73], a practitioner can be empathetic with the individual and provide clear, supportive, and detailed feedback with solutions to problems. For instance, “I am continuously impressed by your progress. I understand how challenging these tasks are and would like you to consider practicing a few trials at a slower speed so we can optimize your technique to achieve faster progression,” in contrast to “Let’s try these tasks again.” Lastly, the opportunity for choice can be purposefully provided "incidentally" to not alter the designed care to be provided that day. For instance, a practitioner could ask an individual to select the background music, ask if they would like the temperature of the room changed, or even if there is a color of hand towel they prefer to use while exercising. Such "trivial" or "task-irrelevant" choices may seem like they would not affect motor function, but have been supported by recent literatures [45, 53, 118, 121] and may be particularly beneficial to youth. Trivial and task-irrelevant choices may also be the preferred manipulation for psychologically immature and relatively younger athletes; specifically, for those in controlling environments accustomed and reliant on others for critical decision-making (a 6- vs. 19-year-old athlete) [24]. Perceiving that an athlete made an "incorrect" task-related decision could be distressing for those with less psychological maturity, whereas incidental/trivial choices may be perceived as less important thereby alleviating worry during or after the decision-making process. Relatively younger athletes may also have limited experience/expertise in OPTIMAL PREP training modalities, warranting individual consideration when determining what type of autonomy support is provided for a given task or exercise. Specifically, autonomy support should only be provided if it purposefully implemented and appropriately reflects the youth athlete’s psychological maturity, experience, technical competency, task-mastery, etc.[24]. Additional autonomy-supportive examples are detailed in Table 2 using ACL injury rehabilitation as an example.
External Focus and Clinical Applications Using Instruction-Based Feedback
The attentional factor of OPTIMAL theory emphasizes the importance of directing an individual’s attention externally toward an intended movement effect (i.e., an external focus of attention) compared to body movements (i.e., an internal focus of attention) [122, 123]. The beneficial effects of an external focus on motor behavior have been reported for numerous tasks, skill levels, and populations [117]. Like the motivational pillars, an external focus can also enhance neuromuscular efficiency [110, 120, 125], but relative to the motivational pillars, has far more empirical support for a range of factors important for OPTIMAL PREP strategies, including balance control [26, 27, 50, 85, 96, 124], performance and movement accuracy [92, 95, 125], jump/hop distance [89, 91, 93, 115], and injury-resistant biomechanics [10, 11, 14, 15, 23, 34, 40, 94, 112, 113].
As discussed previously [24], within the context of ACL injury literature, an external focus has been used interchangeably with whether the augmented feedback is provided verbally or visually [6]. Augmented feedback studies have generally shown improved performance and/or biomechanics associated with ACL injury risk when an external focus is provided, whether feedback is delivered verbally/instruction- or visually/technology-based [10, 11, 14, 15, 23, 34, 38, 40, 94, 112, 113, 120]. With respect to verbal instruction, if a practitioner’s goal is to enhance performance of a hop or jump (i.e., elicit a further, higher, or quicker jump), instruction could be modified to direct an individual’s attention to performance- or mechanic-specific outcomes [77, 94]. For instance, if the goal is to specifically enhance drop vertical jump height, a cue could be provided to “…focus on getting as close to the ceiling as possible [77].” However, when the goal is to enhance movement mechanics, a practitioner could adhere a piece of tape on the patella and direct the individual to "push the tape" in a direction associated with safer landing mechanics [94]. As another example, while performing a supine "quad set" for the purpose of re-educating the quadriceps and increasing terminal knee extension, the simple instruction “focus on pressing into the table” is likely adequate to create an external focus. Whether practitioners aim to improve performance or injury-resistant biomechanics, they should be mindful that athletes exhibit specific responses to cues given [77, 94], with better performance not always reducing injury risk and vice versa. Thus, judiciously targeting the appropriate movement is critical. To aid practitioners in the implementation of "instruction-based" external focus strategies into OPTIMAL PREP training scenarios, examples using common knee exercises for ACL injury rehabilitation are provided in Table 3.
Furthermore, an external focus can be additively combined with enhanced expectancies and autonomy support for potentially more robust motor learning. We direct the reader to recent literature for more detail [24], but we are simply referring to the utilization of all three pillars during a single training session. A few instruction-based additive examples are presented in Table 4 for how this could be implemented as part of ACL injury rehabilitation.
Technologies of the Future to Integrate OPTIMAL PREP Strategies
While traditional "instruction-based" techniques are supported with empirical evidence to enhance motor performance and learning, recent advances in consumer-grade technologies have provided unique opportunities for integrating OPTIMAL PREP strategies for various training scenarios. Though these technology-based modalities have demonstrated high effectiveness for promoting injury-resistant biomechanics and are often theorized to engage an external focus of attention, they have historically been constrained to expensive biomechanics laboratories and necessitate the user to have expertise of several different tools and systems (e.g., motion capture systems, augmented reality, computer programming, etc.) [13,14,15, 31, 32, 35]. However, and of high relevance for OPTIMAL PREP training applications, rapidly evolving improvements in motion capture and display equipment have drastically reduced costs, increased availability, and enhanced user experiences in terms of quality (e.g., higher screen resolution, faster frame rates, immersive renderings and do not necessitate high levels of expertise. Thus, integrating OPTIMAL PREP strategies with such technology may be particularly useful to practitioners who may feel overwhelmed trying to adhere to the proposed modifications to instructional feedback such that they can let the technology assist with feedback delivery. As clinicians and researchers may be unfamiliar with some of the technology-related terms we use below, a brief reference guide with descriptions is provided in Table 5.
Augmented and Virtual Reality
With the increased availability of augmented and virtual reality technology to consumers, a wide range of software and hardware tools have become available to researchers and clinicians. Many of these tools often have freeware or open-source versions available for researchers and nonprofits. For example, the Unity game engine (Unity Technologies; CA, USA) is a popular and easy-to-use software environment for creating augmented and virtual reality content. Additionally, for inexperienced users, there are many free tutorials available online for Unity and other game development platforms (e.g., Unreal Engine; Epic Games, Inc.; NC, USA). Unity Free, available at no cost during the time of this article’s publication, can be used to create interactive 3D environments with complete experimental control that is not often possible in traditional laboratory and ‘real-world’ settings. In terms of research, augmented and virtual realities offer advantages over traditional sports medicine experiments conducted in pristine laboratory settings. For example, stimuli—such as a non-player character that a participant must avoid contact with—can be presented with precise timing to ensure exactly the same experience across participants; alternatively, achieving this without enhanced realities would be momentously difficult due to the ever present variability in human motor behavior/learning [21, 97].
For rehabilitation and research applications, audio-visual stimuli—developed in programs like Unity—can be presented using a range of different head mounted displays to produce controlled experiences, which both mimic and extend real sports scenarios. For example, youth athletes’ lower extremity biomechanics were evaluated using a virtual soccer environment that provided a realistic, but controlled, jump-landing task that evoked context-specific movement patterns that were specific to soccer, while allowing for comprehensive motion analysis that would not have been possible on the field [22, 40]. For this type of application, when a fully immersive environment is desirable, virtual reality head-mounted displays such as the HTC Vive Pro Eye (HTC Corporation; TW, China), which also offers a built in and affordable eye tracking capabilities, may be appropriate. The Vive and similar head-mounted displays will remove the external visual field and thereby allow the subject to focus fully on the virtual task at hand.
Alternatively, a specific application may require seamless integration of the task with real-world objects or individuals. In this case, the use of a head-mounted augmented reality device, such as the Microsoft HoloLens (Microsoft Corporation; WA, USA), may be desirable. The HoloLens allows for 3D objects to be displayed in holographic form while also providing built in tracking of the user’s hands and eyes. Due to the holographic presentation, the HoloLens allows for a participant to maintain awareness of their surroundings, which can be essential if the task at hand cannot be performed in isolation from other individuals or real-world obstacles. While augmented reality has not been used extensively in sports medicine, one recent study demonstrates that its potential use in clinical settings is promising. A HoloLens was used to create an augmented reality-based task that simulated the movement patterns of game-specific spike jump in volleyball, which effectively elicited similar biomechanics to that of a competitive environment [2]. Importantly, using a wireless augmented reality device in this case allowed training to be performed in a crowded gym environment as participants are able to maintain awareness of their surrounding while receiving feedback relative to virtual reality. In fact a HoloLens is also being utilized as part of an ongoing clinical trial (clinicaltrials.gov; NCT# 02933008) to institute a program of neuromuscular training, driven by augmented reality feedback to modify youth athletes’ biomechanics associated with ACL injury risk [13,14,15]. In general, both augmented and virtual reality technologies can be used to great effect when combined with other emerging technologies. For example, the addition of markerless motion capture technologies and other tracking devices, described below, can easily allow for virtual representations of subjects (i.e. avatars) to be displayed and manipulated. Avatars add immersion to virtual scenarios and provide visual grounding for subjects to produce natural movement [102].
Despite the limitless potential for augmented and virtual realities, we carefully point out that, for the foreseeable future, these technologies may be limited to one-on-one utilization in the clinic, with limitations for the simultaneous application to groups of players during team-based practices or competitions. Current augmented realities designed to reduce ACL injury risk require kinematic and kinetic data to stream in near "real-time" to support an interactive visual stimulus (i.e., a geometric rectangle) that distorts as a function of an athlete’s injury-risk and injury-resistant biomechanics elicited during exercises [13,14,15, 23, 40]. However, current marker-based motion capture systems limit the real time joint biomechanical analysis to a single subject, precluding the accommodation of multiple athletes in a training session simultaneously.
Markerless Motion Capture
Current clinical and research applications often leverage multi-camera optical motion capture systems that provide high precision in biomechanical assessment, but these systems may cost a considerable amount, can be difficult to re-configure, and require visible markers to be placed on the subject. Consequently, these systems may not fit within the budget or the available space and expertise of some smaller organizations. They may also be less than ideal for applications that require motion capture to be performed in a mobile setting, for example, at the home of a patient or participant. Recently, markerless motion capture solutions have emerged that capitalize on the significant advancements in machine learning and computing hardware [44, 106]. Two promising examples are the Microsoft Azure Kinect (Microsoft Corporation; WA, USA) and the Apple iPad Pro (Apple Inc.; CA, USA). The Azure Kinect is the newest in a line of small, camera-based devices that can enable motion capture when paired with a high-end desktop computer or laptop. Microsoft also provides multiple software development kits that enable developers to leverage their graphics processing unit-based machine learning tool for 3D joint center estimation. Joint center data derived in this way can then easily be analyzed or used to drive a real-time training or rehabilitation program, such as one of the augmented and virtual reality applications described above. The iPad Pro offers an interesting mix of motion capture and display technology. Recently, a light detection and ranging sensor was added to the newest iPad model, which enables high-precision 3D motion capture and environment mapping. Although it has not been tested for clinical applications, this could offer a very streamlined method of both collecting and displaying motion capture data.
Lastly, the Vive tracker (HTC Corporation; TW, China) is another piece of motion capture equipment that has shown promise in measuring joint rotations and positions with research-grade accuracy and low latency (near real time; ~ 5 ms) [18, 103]. The Vive tracker is part of a larger Vive system that includes up to four infrared-emitting base stations, two handheld controllers, a head-mounted display, and a small tracker “puck.” With concurrent use of the system’s tracking and display equipment, realistic feedback about a user’s movements can be reflected in real time in the virtual environment. While precise full body kinematic motion capture—as provided by systems like the Kinect—is not possible without using one Vive tracker for each tracked body segment, a small number of Vive trackers can be used in conjunction with machine learning to approximate full-body tracking. One example of such implementation would be using the Vive trackers in concert with the Vive Pro head-mounted display and two Vive controllers to approximate full-body tracking. In this scenario, Vive trackers would be placed on the feet and waist, the controllers would track hand positions, and the head-mounted display would provide head tracking. Additionally, software based inverse kinematic solvers can be utilized to transform the tracking data from such a setup into a realistic full-body avatar. Again, this may not be appropriate when highly detailed motion capture recordings are required, but will provide the most frictionless path to full-body motion tracking and avatar presentation.
Eye Tracking
In addition to the potential uses of the Vive head-mounted display and trackers, eye tracking is also possible with the use of a Vive Pro Eye (HTC Corporation; TW, China). Specifically, eye tracking via the Vive Pro Eye can be used as a supplementary tool to investigate how participants visually explore virtual environments. From a research perspective, this tool could even help elucidate the potential role of vision with respect to the attentional focus pillar – where there is an ongoing debate whether an external focus necessitates a person "looking" at the appropriate stimuli [1, 67, 90]. Eye tracking may also be particularly useful to investigate the visual-spatial processing deficits associated with musculoskeletal injury [5, 28, 37, 39, 41, 42, 75, 105, 114]. Based on fMRI data of knee flexion and extension movements [41, 42], researchers have theorized a framework whereby patients rely more heavily on visual-spatial information for knee motor control following ACLR [39] and prospective data indicate reduced visual memory and processing ability also increased primary ACL injury risk [105]. As such, eye tracking could be used to quantify the visual-spatial search strategies patients utilize during ACL injury rehabilitation or for youth with a wide range of musculoskeletal-disorders potentially influenced by altered sensorimotor control strategies. Further, even in the absence of augmented or virtual reality technologies, eye tracking could be used to supplement novel, neurocognitive-based return-to-play paradigms that have been designed to supplement traditional testing in light of neuroplasticity, such as neurocognitive challenges added to traditional hop testing [101]. Eye tracking could simply be used to quantify adherence to manipulations that direct vision, or as an exploratory variable that may be mediating/modulating the effects of a manipulation or intervention across the spectrum of youth populations.
Opportunities to Integrate Instruction-Based Feedback with Emergent Technologies for Optimized Motor Learning: The Future of Exercise Performance
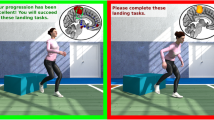
While the technology and research applications just described are not directly related to the OPTIMAL theory of motor learning, a salubrious opportunity exists to combine with enhanced expectancies, autonomy support, and an external focus of attention. Recently developed technological innovations have the potential to create highly effective PREP methods for near limitless training applications. One opportunity for creating new training programs exist by specifically directing a patient’s attention externally towards augmented or virtual reality stimuli. However, in place of verbal instruction that must be continuously provided by a practitioner and thus increases staffing resources, a computer program could instruct an individual to keep a horizontal virtual line—displayed within a head mounted-display using two Vive trackers—to elicit an external focus of attention (see Fig. 1). This provides several advantages as individuals can easily focus their attention towards the display (and concurrently their own performance) without looking down at their feet (BOSU® ball in this example), which detracts from proper form and execution on the task [68]. Additionally, performance can be easily quantified through the recorded positional data of the Vive trackers. This data may be used to quantify individual training session performance or potentially progression throughout rehabilitation. While this is only one specific example of how external focus and technology can be combined, there are numerous opportunities—from rehabilitation after a spinal cord injury [81] to baseball pitch training [108]—for integrating technological advancements with OPTIMAL PREP strategies.

Image demonstrates an approach to integrate all three pillars of OPTIMAL theory during a training session. Specifically, this individual is being provided feedback through a virtual reality headset while performing squats on a BOSU® ball. Importantly, the participant is provided with four choices of exercises to promote autonomy support (BOSU® ball exercise colored yellow; other three exercises shaded blue indicating they were not chosen). A blue colored bar provides biofeedback via a level indicator streamed in near real-time by the black sensors attached to the BOSU ball that an individual can attend to for promoting an external focus. The blue feedback bar can also be positively biased with largely green and yellow colors indicating good performance to enhance purposeful expectancies (the program could restrict the bar moving into the "red" as a function of individual physical capability while maintaining their safety)
The ability to quantify performance across individual training sessions provides excellent opportunities for further integrating enhanced expectancies and autonomy support into any technology-based training program. For instance, a practitioner could easily modify the stimulus to only provide purposeful feedback to enhance expectancies of individuals, safely (colored green in Fig. 1). For instance, positive feedback could be provided that challenges the individual without extending past their physical capability. As such, the practitioner is not required to provide the purposeful feedback, rather the technology would do this automatically and could be systematically programmed to not exceed an individual’s constraints. Furthermore, autonomy support—specifically allowing participants choice in training programs—can easily be achieved by providing a "gamification" of the individual session via technology. Gamification is the process of incorporating game features like social interaction, rules and goals, and control into traditionally nongame settings, such as classrooms, in order to increase the outcomes and effectiveness of training programs [33, 51, 126]. While practically all sports related activities inherently possess at least one gaming element, current rehabilitation and injury prevention/risk reduction strategies are specific areas that could benefit from increased gamification integrated into current practice. Gamification may be particularly beneficial in youth injury rehabilitation programs following the cessation of sport participation as motivation, autonomy, and numerous other psychological factors are impaired during recovery [107]. Moreover, there is a substantial body of literature that indicates gamification can increase motivation levels and engagement with learning programs while improving learning outcomes [33, 126]. However, gamification may be more appealing to relatively younger or psychologically immature athletes who require additional stimuli to maintain cognitive engagement. In contrast, some relatively older youth may have more exposure to video/computer games, cell phone games, etc., thus gamification may be particularly beneficial for these athletes. Though future research is needed, age and psychological maturity should be carefully considered before gamification is employed. Likewise, age and psychological-related factors should always be considered before any of the other aforementioned technologies or strategies are implemented with OPTIMAL PREP.
Despite the lack of empirical support for gamification of rehabilitation and injury prevention programs within sports medicine, there are opportunities to incorporate features of games to similarly increase motor learning and training outcomes. For instance, and as seen in Fig. 1, the individual chose the BOSU® Ball exercise (highlighted yellow), with other exercises that were not selected still displayed, but shaded blue/gray (indicating the individual did not choose those). Likewise, the "gamification" of feedback provided to users—provided either before, during, and/or after an exercise—can be systematically programmed in light of scientific findings (or manipulated/tailored to individual progression). The timing of feedback is a key component of OPTIMAL theory and successful motor learning in general [64]. Thus, the technological opportunities to not only program what feedback is provided, but when feedback is delivered via PREP strategies can further mitigate practitioner burden. While the timing (prior to, real-time or after exercise) of feedback is important, strategic implementation of OPTIMAL PREP should consider a number of factors such as the desired outcome, the task itself, and individual/environmental constraints, warranting future research. A general consensus is that a trainee should not become "dependent" on feedback—whether that feedback is provided prior to, during, or after a movement and how much is actually delivered—the specific nuances of when to provide feedback and exactly how much is outside the scope of this commentary. However we direct the reader to existing literature on this topic that can provide guidance on this topic [4, 43, 80, 98, 100, 119], and is a promising avenue for future OPTIMAL PREP research. Lastly, the advantages of integrating technology with OPTIMAL PREP strategies extend beyond the benefits provided to the user. With the lower cost of these potential systems and continued expansion of telehealth [29], it is reasonable to expect that a portion of training scenarios will take place away from a clinic or specialized training facility. Integrating technology—specifically the ability to remotely access objective data acquired by the devices—will allow practitioners to monitor progression throughout training and appropriately adjust it based on objective, quantified data.
Summary and Future Directions
In addition to the limitations noted in previous OPTIMAL PREP literature [24, 25], limitations of the practical applications proposed warrant discussion. Firstly, some of our instruction-based examples use tasks that have not been empirically studied for every youth population, age range, and/or training scenario, precluding conclusive insight into the potential widespread effectiveness of OPTIMAL PREP strategies. However, the extant motor learning literature in numerous related populations, ages, and tasks [123] supports the opportunity for all three pillars to be effective for youth injury resistance and exercise performance. Secondly, while relatively uncommon, some individuals may experience cyber sickness with aspects of technology-based approaches, such as while interacting with virtual reality environments; hypothesized to arise from sensory conflicts involving afferent signals from the visual, vestibular, and somatic systems [12, 16, 79]. However, the likelihood of cyber sickness can be reduced by having the visual field correspond in a one-to-one fashion to individual movements [74]. Lastly, our proposed technologies of the future, while more accessible than those prior, are not completely free of resources or technical expertise. Indeed, current and emergent technologies will continue to require an appropriate level of technical competency and familiarity with a given technology, particularly if practitioners aim to synchronize multiple devices, utilize ‘real-time’ data streaming, and/or implement research-grade protocols utilizing in-house programming. Fortunately, there are many free online tutorials that practitioners could complete to achieve higher technical competency and more technological familiarity. Furthermore, extensive programming knowledge may not be needed, or only to a very basic extent, as numerous openly accessible platforms for code-share (e.g., Github, Gitlab) and data-share (e,g, Figshare, Dryad, Zenodo) have emerged.
Despite currently known limitations, we have proposed a conceptual framework for the application of OPTIMAL PREP training strategies in youth [24, 25]. Importantly, we do not suggest traditional training methods such as strength training principles be superseded, rather highlight their potential for enhancement through the additive inclusion of the pillars supporting OPTIMAL PREP. Traditional, contemporary, and emergent injury management and exercise performance programs, with any level of current effectiveness, could potentially benefit from incorporating "instruction-based" recommendations and/or future technologies without a significant disruption to their current approaches. Despite minimal widespread clinical implementation, we anticipate future research to further deconstruct the manner in which OPTIMAL PREP strategies may interact with other important training-related variables for injury resistance, such as loading/periodization, psychological factors, and/or age-related factors associated with general physical, emotional, and psychological maturity. In summary, we are excited for the future applications of OPTIMAL PREP training strategies whereby clinicians and researchers work together to support an active, healthy, and injury-resistant lifestyle across the spectrum of youth populations, in both males and females.
Data Availability
Not applicable.
Code Availability
Not applicable.
References
Abdollahipour R, Psotta R, Land WM. The influence of attentional focus instructions and vision on jump height performance. Res Q Exerc Sport. 2016;87(4):408–13. https://doi.org/10.1080/02701367.2016.1224295.
Adams K, Kiefer A, Panchuk D, Hunter A, MacPherson R, Spratford W. From the field of play to the laboratory: Recreating the demands of competition with augmented reality simulated sport. J Sports Sci. 2020;38(5):486–93. https://doi.org/10.1080/02640414.2019.1706872.
Andersen MB, Williams JM. A model of stress and athletic injury: Prediction and prevention. J Sport Exerc Psychol. 1988;10(3):294–306. https://doi.org/10.1123/jsep.10.3.294.
Anderson DI, Magill RA, Sekiya H. Motor learning as a function of KR schedule and characteristics of task-intrinsic feedback. J Mot Behav. 2001;33(1):59–66. https://doi.org/10.1080/00222890109601903.
Armitano-Lago CN, Morrison S, Hoch JM, Bennett HJ, Russell DM. Anterior cruciate ligament reconstructed individuals demonstrate slower reactions during a dynamic postural task. Scand J Med Sci Sports. 2020;30(8):1518–28. https://doi.org/10.1111/sms.13698.
Armitano CN, Haegele JA, Russell DM. The use of augmented information for reducing anterior cruciate ligament injury risk during jump landings: a systematic review. J Athl Train. 2018;53(9):844–59. https://doi.org/10.4085/1062-6050-320-17.
Bahmani M, Diekfuss JA, Rostami R, Ataee N, Ghadiri F. Visual illusions affect motor performance, but not learning in highly skilled-shooters. J Motor Learn Dev. 2018;6(2):220–33. https://doi.org/10.1123/jmld.2017-0011.
Bahmani M, Wulf G, Ghadiri F, Karimi S, Lewthwaite R. Enhancing performance expectancies through visual illusions facilitates motor learning in children. Hum Mov Sci. 2017;55:1–7. https://doi.org/10.1016/j.humov.2017.07.001.
Behm DG, Faigenbaum AD, Falk B, Klentrou P. Canadian Society for Exercise Physiology position paper: resistance training in children and adolescents. Appl Physiol Nutr Metab. 2008;33(3):547–61. https://doi.org/10.1139/h08-020.
Benjaminse A, Otten B, Gokeler A, Diercks RL, Lemmink KA. Motor learning strategies in basketball players and its implications for ACL injury prevention: a randomized controlled trial. Knee Surg Sports Traumatol Arthrosc. 2017;25(8):2365–76. https://doi.org/10.1007/s00167-015-3727-0.
Benjaminse A, Welling W, Otten B, Gokeler A. Transfer of improved movement technique after receiving verbal external focus and video instruction. Knee Surg Sports Traumatol Arthrosc. 2018;26(3):955–62. https://doi.org/10.1007/s00167-017-4671-y.
Bles W, Bos JE, De Graaf B, Groen E, Wertheim AH. Motion sickness: only one provocative conflict? Brain Res Bull. 1998;47(5):481–7. https://doi.org/10.1016/s0361-9230(98)00115-4.
Bonnette S, DiCesare CA, Diekfuss JA, Grooms DR, MacPherson RP, Riley MA, Myer GD. Advancing anterior cruciate ligament injury prevention using real-time biofeedback for amplified sensorimotor integration. J Athl Train. 2019;54(9):985–6. https://doi.org/10.4085/1062-6050-54.083.
Bonnette S, DiCesare CA, Kiefer AW, Riley MA, Barber-Foss KD, Thomas S, Diekfuss JA, Myer GD. A technical report on the development of a real-time visual biofeedback system to optimize motor learning and movement deficit correction. J Sports Sci Med. 2020;19(1):84–94.
Bonnette S, DiCesare CA, Kiefer AW, Riley MA, Barber Foss KD, Thomas S, Kitchen K, Diekfuss JA, Myer GD. Injury risk factors integrated into self-guided real-time biofeedback improves high-risk biomechanics. J Sport Rehab. 2019;. https://doi.org/10.1123/jsr.2017-0391.
Bos JE, Bles W, Groen EL. A theory on visually induced motion sickness. Displays. 2008;29(2):47–57. https://doi.org/10.1016/j.displa.2007.09.002.
Burland JP, Lepley AS, Frechette L, Lepley LK. Protracted alterations in muscle activation strategies and knee mechanics in patients after Anterior Cruciate Ligament Reconstruction. Knee Surg Sports Traumatol Arthrosc. 2020. https://doi.org/10.1007/s00167-019-05833-4.
Caserman P, Garcia-Agundez A, Konrad R, Göbel S, Steinmetz R. Real-time body tracking in virtual reality using a Vive tracker. Virtual Real. 2019;23(2):155–68. https://doi.org/10.1007/s10055-018-0374-z.
Chauvel G, Wulf G, Maquestiaux F. Visual illusions can facilitate sport skill learning. Psychon Bull Rev. 2015;22(3):717–21. https://doi.org/10.3758/s13423-014-0744-9.
Chiviacowsky S, Wulf G, Lewthwaite R. Self-controlled learning: the importance of protecting perceptions of competence. Front Psychol. 2012;3:458. https://doi.org/10.3389/fpsyg.2012.00458.
Dhawale AK, Smith MA, Ölveczky BP. The role of variability in motor learning. Annu Rev Neurosci. 2017;40:479–98. https://doi.org/10.1146/annurev-neuro-072116-031548.
DiCesare CA, Kiefer AW, Bonnette SH, Myer GD. Realistic soccer-specific virtual environment exposes high-risk lower extremity biomechanics. J Sport Rehabil. 2020,29(3):294–300. https://doi.org/10.1123/jsr.2018-0237.
Diekfuss JA, Grooms DR, Bonnette S, DiCesare CA, Thomas S, MacPherson RP, Ellis JD, Kiefer AW, Riley MA, Schneider DK, Gadd B, Kitchen K, Barber Foss KD, Dudley JA, Yuan W, Myer GD. Real-time biofeedback integrated into neuromuscular training reduces high-risk knee biomechanics and increases functional brain connectivity: a preliminary longitudinal investigation. Psychophysiology. 2020. https://doi.org/10.1111/psyp.13545.
Diekfuss JA, Grooms DR, Hogg JA, Singh H, Slutsky AB, Bonnette S, Riehm C, Anand M, Nissen KS, Wilkerson GB, Myer GD. Targeted application of motor learning theory to leverage youth neuroplasticity for enhanced injury-resistance and exercise performance: OPTIMAL PREP. J Sci Sport Exerc. 2020;. https://doi.org/10.1007/s42978-020-00085-y.
Diekfuss JA, Hogg JA, Grooms DR, Slutsky AB, Singh H, Bonnette S, Anand M, Wilkerson GB, Myer GD. Can we capitalize on central nervous system plasticity in young athletes to inoculate against injury? J Sci Sport Exerc. 2020;. https://doi.org/10.1007/s42978-020-00080-3.
Diekfuss JA, Janssen JA, Slutsky AB, Berry NT, Etnier JL, Wideman L, Raisbeck LD. An external focus of attention is effective for balance control when sleep-deprived. Int J Exerc Sci. 2018;11(5):84–94.
Diekfuss JA, Rhea CK, Schmitz RJ, Grooms DR, Wilkins RW, Slutsky AB, Raisbeck LD. The influence of attentional focus on balance control over seven days of training. J Mot Behav. 2019;51(3):281–92. https://doi.org/10.1080/00222895.2018.1468312.
Dingenen B, Janssens L, Claes S, Bellemans J, Staes FF. Postural stability deficits during the transition from double-leg stance to single-leg stance in anterior cruciate ligament reconstructed subjects. Hum Mov Sci. 2015;41:46–58. https://doi.org/10.1016/j.humov.2015.02.001.
Dorsey ER, Topol EJ. State of telehealth. N Engl J Med. 2016;375(2):154–61. https://doi.org/10.1056/NEJMra1601705.
Eime RM, Young JA, Harvey JT, Charity MJ, Payne WR. A systematic review of the psychological and social benefits of participation in sport for children and adolescents: informing development of a conceptual model of health through sport. Int J Behav Nutr Phys Act. 2013;10:98. https://doi.org/10.1186/1479-5868-10-98.
Ericksen HM, Thomas AC, Gribble PA, Armstrong C, Rice M, Pietrosimone B. Jump–landing biomechanics following a 4-week real-time feedback intervention and retention. Clin Biomech. 2016;32:85–91. https://doi.org/10.1016/j.clinbiomech.2016.01.005.
Ericksen HM, Thomas AC, Gribble PA, Doebel SC, Pietrosimone BG. Immediate effects of real-time feedback on jump-landing kinematics. J Orthop Sports Phys Ther. 2015;45(2):112–8. https://doi.org/10.2519/jospt.2015.4997.
Faiella F, Ricciardi M. Gamification and learning: a review of issues and research. J e-Learn Knowl Soc. 2015;11(3):13–211. https://doi.org/10.20368/1971-8829/1072.
Favre J, Clancy C, Dowling AV, Andriacchi TP. Modification of knee flexion angle has patient-specific effects on anterior cruciate ligament injury risk factors during jump landing. Am J Sports Med. 2016;44(6):1540–6. https://doi.org/10.1177/0363546516634000.
Ford KR, DiCesare CA, Myer GDD, Hewett TE. Real-time biofeedback to target risk of anterior cruciate ligament injury: a technical report for injury prevention and rehabilitation. J Sport Rehabil Tech Notes. 2015. https://doi.org/10.1123/jsr.2013-0138.
Ford P, De Ste Croix M, Lloyd R, Meyers R, Moosavi M, Oliver J, Till K, Williams C. The long-term athlete development model: Physiological evidence and application. J Sports Sci. 2011;29(4):389–402. https://doi.org/10.1080/02640414.2010.536849.
Friden T, Roberts D, Movin T, Wredmark T. Function after anterior cruciate ligament injuries: influence of visual control and proprioception. Acta Orthop Scand. 1998;69(6):590–4. https://doi.org/10.3109/17453679808999261.
Gokeler A, Benjaminse A, Welling W, Alferink M, Eppinga P, Otten B. The effects of attentional focus on jump performance and knee joint kinematics in patients after ACL reconstruction. Phys Ther Sport. 2015;16(2):114–20. https://doi.org/10.1016/j.ptsp.2014.06.002.
Grooms D, Appelbaum G, Onate J. Neuroplasticity following anterior cruciate ligament injury: a framework for visual-motor training approaches in rehabilitation. J Orthop Sports Phys Ther. 2015;45(5):381–93. https://doi.org/10.2519/jospt.2015.5549.
Grooms DR, Kiefer AW, Riley MA, Ellis JD, Thomas S, Kitchen K, DiCesare CA, Bonnette S, Gadd B, Barber Foss KD, Yuan W, Silva P, Galloway R, Diekfuss JA, Leach J, Berz K, Myer GD. Brain-behavior mechanisms for the transfer of neuromuscular training adaptions to simulated sport: Initial findings from the train the brain project. J Sport Rehab. 2018;27(5):1–5. https://doi.org/10.1123/jsr.2017-0241.
Grooms DR, Page S, Onate JA. Brain activation for knee movement measured days before second anterior cruciate ligament injury: neuroimaging in musculoskeletal medicine. J Athl Train. 2015;50(10):1005–10. https://doi.org/10.4085/1062-6050-50-10-02.
Grooms DR, Page SJ, Nichols-Larsen DS, Chaudhari AM, White SE, Onate JA. Neuroplasticity associated with anterior cruciate ligament reconstruction. J Orthop Sports Phys Ther. 2017;47(3):180–9. https://doi.org/10.2519/jospt.2017.7003.
Guadagnoli MA, Lee TD. Challenge point: a framework for conceptualizing the effects of various practice conditions in motor learning. J Mot Behav. 2004;36(2):212–24. https://doi.org/10.3200/JMBR.36.2.212-224.
Harsted S, Holsgaard-Larsen A, Hestbæk L, Boyle E, Lauridsen HH. Concurrent validity of lower extremity kinematics and jump characteristics captured in pre-school children by a markerless 3D motion capture system. Chiropr Man Therap. 2019;27(1):39. https://doi.org/10.1186/s12998-019-0261-z.
Hartman JM. Self-controlled use of a perceived physical assistance device during a balancing task. Percept Mot Skills. 2007;104(3):1005–16. https://doi.org/10.2466/pms.104.3.1005-1016.
Hewett TE, Di Stasi SL, Myer GD. Current concepts for injury prevention in athletes after anterior cruciate ligament reconstruction. Am J Sports Med. 2013;41(1):216–24. https://doi.org/10.1177/0363546512459638.
Iwatsuki T, Abdollahipour R, Psotta R, Lewthwaite R, Wulf G. Autonomy facilitates repeated maximum force productions. Hum Mov Sci. 2017;55:264–8. https://doi.org/10.1016/j.humov.2017.08.016.
Iwatsuki T, Navalta JW, Wulf G. Autonomy enhances running efficiency. J Sports Sci. 2019;37(6):685–91. https://doi.org/10.1080/02640414.2018.1522939.
Karsh N, Eitam B. I control therefore I do: Judgments of agency influence action selection. Cognition. 2015;138:122–31. https://doi.org/10.1016/j.cognition.2015.02.002.
Landers M, Wulf G, Wallmann H, Guadagnoli M. An external focus of attention attenuates balance impairment in patients with Parkinson's disease who have a fall history. Physiotherapy. 2005;91(3):152–8. https://doi.org/10.1016/j.physio.2004.11.010.
Landers RN. Developing a theory of gamified learning: Linking serious games and gamification of learning. Simul Gaming. 2014;45(6):752–68. https://doi.org/10.1177/1046878114563660.
Leotti LA, Delgado MR. The inherent reward of choice. Psychol Sci. 2011;22(10):1310–18. https://doi.org/10.1177/0956797611417005.
Lewthwaite R, Chiviacowsky S, Drews R, Wulf G. Choose to move: The motivational impact of autonomy support on motor learning. Psychon Bull Rev. 2015;22(5):1383–8. https://doi.org/10.3758/s13423-015-0814-7.
Lloyd RS, Cronin JB, Faigenbaum AD, Haff GG, Howard R, Kraemer WJ, Micheli LJ, Myer GD, Oliver JL. National strength and conditioning association position statement on long-term athletic development. J Strength Cond Res. 2016;30(6):1491–509. https://doi.org/10.1519/JSC.0000000000001387.
Lloyd RS, Faigenbaum AD, Myer G, Stone M, Oliver J, Jeffreys I, Pierce K. UKSCA position statement: youth resistance training. Prof Strength Cond. 2012;26:26–39. https://doi.org/10.1136/bjsports-2013-092952.
Lloyd RS, Meyers RW, Oliver JL. The natural development and trainability of plyometric ability during childhood. Strength Cond J. 2011;33(2):23–32. https://doi.org/10.1519/SSC.0b013e3182093a27.
Lloyd RS, Oliver JL. The youth physical development model: a new approach to long-term athletic development. Strength Cond J. 2012;34(3):61–72. https://doi.org/10.1519/SSC.0b013e31825760ea.
Lloyd RS, Oliver JL. Strength and conditioning for young athletes: science and application. Amsterdam: Routledge; 2019.
Lloyd RS, Oliver JL, Faigenbaum AD, Howard R, Croix MBDS, Williams CA, Best TM, Alvar BA, Micheli LJ, Thomas DP. Long-term athletic development, part 2: barriers to success and potential solutions. J Strength Cond Res. 2015;29(5):1451–64. https://doi.org/10.1519/01.JSC.0000465424.75389.56.
Lloyd RS, Oliver JL, Hughes MG, Williams CA. The influence of chronological age on periods of accelerated adaptation of stretch-shortening cycle performance in pre and postpubescent boys. J Strength Cond Res. 2011;25(7):1889–977. https://doi.org/10.1519/JSC.0b013e3181e7faa8.
Lloyd RS, Oliver JL, Meyers RW, Moody JA, Stone MH. Long-term athletic development and its application to youth weightlifting. Strength Cond J. 2012;34(4):55–66. https://doi.org/10.1519/SSC.0b013e31825ab4bb.
Lloyd RS, Read P, Oliver JL, Meyers RW, Nimphius S, Jeffreys I. Considerations for the development of agility during childhood and adolescence. Strength Cond J. 2013;35(3):2–11. https://doi.org/10.1519/SSC.0b013e31827ab08c.
Maddison R, Prapavessis H, Clatworthy M. Modeling and rehabilitation following anterior cruciate ligament reconstruction. Ann Behav Med. 2006;31(1):89–98. https://doi.org/10.1207/s15324796abm3101_13.
Magill R. Motor learning and control. New York: McGraw-Hill Publishing; 2010.
Malina RM, Cumming SP, Morano PJ, Barron M, Miller SJ. Maturity status of youth football players: a noninvasive estimate. Med Sci Sports Exerc. 2005;37(6):1044–52.
McArdle S. Psychological rehabilitation from anterior cruciate ligament–medial collateral ligament reconstructive surgery: a case study. Sports Health. 2010;2(1):73–7. https://doi.org/10.1177/1941738109357173.
McNamara SW, Becker KA, Silliman-French LM. The differential effects of attentional focus in children with moderate and profound visual impairments. Front Psychol. 2017;8:1804. https://doi.org/10.3389/fpsyg.2017.01804.
Myer GD, Chu DA, Brent JL, Hewett TE. Trunk and hip control neuromuscular training for the prevention of knee joint injury. Clin Sports Med. 2008;27(3):425–48. https://doi.org/10.1016/j.csm.2008.02.006.
Myer GD, Faigenbaum AD, Chu DA, Falkel J, Ford KR, Best TM, Hewett TE. Integrative training for children and adolescents: techniques and practices for reducing sports-related injuries and enhancing athletic performance. Physician Sports Med. 2011;39(1):74–84. https://doi.org/10.3810/psm.2011.02.1864.
Myer GD, Ford KR, Brent JL, Hewett TE. An integrated approach to change the outcome part II: targeted neuromuscular training techniques to reduce identified ACL injury risk factors. J Strength Cond Res. 2012;26(8):2272–92. https://doi.org/10.1519/JSC.0b013e31825c2c7d.
Myer GD, Ford KR, Hewett TE. Rationale and clinical techniques for anterior cruciate ligament injury prevention among female athletes. J Athl Train. 2004;39(4):352.
Myer GD, Lloyd RS, Brent JL, Faigenbaum AD. How young is “too young” to start training? ACSM's Health Fit J. 2013;17(5):14. https://doi.org/10.1249/FIT.0b013e3182a06c59.
Myer GD, Paterno MV, Ford KR, Hewett TE. Neuromuscular training techniques to target deficits before return to sport after anterior cruciate ligament reconstruction. J Strength Cond Res. 2008;22(3):987–1014. https://doi.org/10.1519/JSC.0b013e31816a86cd.
Ng AK, Chan LK, Lau HY. A study of cybersickness and sensory conflict theory using a motion-coupled virtual reality system. Displays. 2020;61:101922. https://doi.org/10.1016/j.displa.2019.08.004.
Niederer D, Giesche F, Janko M, Niemeyer P, Wilke J, Engeroff T, Stein T, Frank J, Banzer W, Vogt L. Unanticipated jump-landing quality in patients with anterior cruciate ligament reconstruction: how long after the surgery and return to sport does the re-injury risk factor persist? Clin Biomech. 2020;72:195–201. https://doi.org/10.1016/j.clinbiomech.2019.12.021.
Nwachukwu BU, Adjei J, Rauck RC, Chahla J, Okoroha KR, Verma NN, Allen AA, Williams RJ 3rd. How much do psychological factors affect lack of return to play after anterior cruciate ligament reconstruction? A systematic review. Orthop J Sports Med. 2019;7(5):2325967119845313. https://doi.org/10.1177/2325967119845313.
Oliver J, Barillas S, Rhodri L, Moore I, Pedley J. External cueing influences drop jump performance in trained young soccer players. J Strength Cond Res. 2019. https://doi.org/10.1519/JSC.0000000000002935.
Oliver JL, Lloyd RS. Long-term athlete development and trainability during childhood: A brief review. Prof Strength Cond J. 2012;26:19–24. https://doi.org/10.1080/02640414.2010.536849.
Oman CM. A heuristic mathematical model for the dynamics of sensory conflict and motion sickness hearing in classical musicians. Acta Otolaryngol. 1982;94(S392):4–44. https://doi.org/10.3109/00016488209108197.
Otte FW, Davids K, Millar S-K, Klatt S. When and how to provide feedback and instructions to athletes? How sport psychology and pedagogy insights can improve coaching interventions to enhance self-regulation in training. Front Psychol. 2020;11:1444. https://doi.org/10.3389/fpsyg.2020.01444.
Palaniappan SM, Duerstock BS. Developing rehabilitation practices using virtual reality exergaming. In: 2018 IEEE International Symposium on Signal Processing and Information Technology (ISSPIT), IEEE. 2018. pp. 090–094. https://doi.org/10.1109/ISSPIT.2018.8642784.
Palmer K, Chiviacowsky S, Wulf G. Enhanced expectancies facilitate golf putting. Psychol Sport Exerc. 2016;22:229–32. https://doi.org/10.1016/j.psychsport.2015.08.009.
Palmieri-Smith RM, Thomas AC. A neuromuscular mechanism of posttraumatic osteoarthritis associated with ACL injury. Exerc Sport Sci Rev. 2009;37(3):147–53. https://doi.org/10.1097/JES.0b013e3181aa6669.
Pamukoff DN, Pietrosimone BG, Ryan ED, Lee DR, Blackburn JT. Quadriceps function and hamstrings co-activation after anterior cruciate ligament reconstruction. J Athl Train. 2017;52(5):422–8. https://doi.org/10.4085/1062-6050-52.3.05.
Park SH, Yi CW, Shin JY, Ryu YU. Effects of external focus of attention on balance: a short review. J Phys Ther Sci. 2015;27(12):3929–31. https://doi.org/10.1589/jpts.27.3929.
Paterno MV, Flynn K, Thomas S, Schmitt LC. Self-reported fear predicts functional performance and second ACL injury after ACL reconstruction and return to sport: a pilot study. Sports health. 2018;10(3):228–33. https://doi.org/10.1177/1941738117745806.
Patterns ALEM. Instruction of jump-landing technique using videotape feedback. Am J Sports Med. 2005;33(6):831. https://doi.org/10.1177/0363546504271499.
Pichardo AW, Oliver JL, Harrison CB, Maulder PS, Lloyd RS. Integrating models of long-term athletic development to maximize the physical development of youth. Int J Sports Sci Coach. 2018;13(6):1189–99. https://doi.org/10.1177/1747954118785503.
Porter J, Anton PM, Wu WFW. Increasing the distance of an external focus of attention enhances standing long jump performance. J Strength Cond Res. 2012;26(9):2389–93. https://doi.org/10.1519/JSC.0b013e31823f275c.
Porter J, Makaruk H, Starzak M. The role of vision and movement automization on the focus of attention effect. J Mot Learn Dev. 2016;4(2):152–68. https://doi.org/10.1123/jmld.2015-0020.
Porter J, Ostrowski EJ, Nolan RP, Wu WFW. Standing long-jump performance is enhanced when using an external focus of attention. J Strength Cond Res. 2010;24(7):1746–50. https://doi.org/10.1519/JSC.0b013e3181df7fbf.
Raisbeck LD, Diekfuss JA. Verbal cues and attentional focus: a simulated target-shooting experiment. J Mot Learn Dev. 2017;5(1):148–59. https://doi.org/10.1123/jmld.2016-0017.
Raisbeck LD, Diekfuss JA, Rhea CK. Does an external focus improve single-leg jump distance for individuals with chronic ankle instability? Athl Train Sports Health Care. 2020. https://doi.org/10.3928/19425864-20191106-01.
Raisbeck LD, Yamada M. The effects of instructional cues on performance and mechanics during a gross motor movement. Hum Mov Sci. 2019;66:149–56. https://doi.org/10.1016/j.humov.2019.04.001.
Raisbeck LD, Yamada M, Diekfuss JA, Kuznetsov NA. The effects of attentional focus instructions and task difficulty in a paced fine motor skill. J Mot Behav. 2020;52(3):262–70. https://doi.org/10.1080/00222895.2019.1614900.
Rhea CK, Diekfuss JA, Fairbrother JT, Raisbeck LD. Postural control entropy is increased when adopting an external focus of attention. Mot Control. 2019;23(2):230–42. https://doi.org/10.1123/mc.2017-0089.
Riley MA, Turvey MT. Variability and determinism in motor behavior. J Mot Behav. 2002;34(2):99–125. https://doi.org/10.1080/00222890209601934.
Salmoni AW, Schmidt RA, Walter CB. Knowledge of results and motor learning: a review and critical reappraisal. Psychol Bull. 1984;95(3):355. https://doi.org/10.1037/0033-2909.95.3.355.
Sanli EA, Patterson JT, Bray SR, Lee TD. Understanding self-controlled motor learning protocols through the self-determination theory. Front Psychol. 2013;3:611. https://doi.org/10.3389/fpsyg.2012.00611.
Schmidt RA, Lee TD. Motor learning and control: a behavioral emphasis. Champaign: Human Kinetics; 2005.
Simon JE, Millikan N, Yom J, Grooms DR. Neurocognitive challenged hops reduced functional performance relative to traditional hop testing. Phys Ther Sport. 2020;41:97–102. https://doi.org/10.1016/j.ptsp.2019.12.002.
Slater M, Sanchez-Vives MV. Enhancing our lives with immersive virtual reality. Front Robot AI. 2016;3:74. https://doi.org/10.3389/frobt.2016.00074.
Spitzley KA, Karduna AR. Feasibility of using a fully immersive virtual reality system for kinematic data collection. J Biomech. 2019;87:172–6. https://doi.org/10.1016/j.jbiomech.2019.02.015.
Stoate I, Wulf G, Lewthwaite R. Enhanced expectancies improve movement efficiency in runners. J Sports Sci. 2012;30(8):815–23. https://doi.org/10.1080/02640414.2012.671533.
Swanik CB, Covassin T, Stearne DJ, Schatz P. The relationship between neurocognitive function and noncontact anterior cruciate ligament injuries. Am J Sports Med. 2007;35(6):943–8. https://doi.org/10.1177/0363546507299532.
Tipton CC, Telfer S, Cherones A, Gee AO, Kweon CY. The use of microsoft Kinect ™ for assessing readiness of return to sport and injury risk exercises: a validation study. Int J Sports Phys Ther. 2019;14(5):724–30.
Truong LK, Mosewich AD, Holt CJ, Le CY, Miciak M, Whittaker JL. Psychological, social and contextual factors across recovery stages following a sport-related knee injury: a scoping review. Br J Sports Med. 2020. https://doi.org/10.1136/bjsports-2019-101206.
Tsai Y-T, Jhu W-Y, Chen C-C, Kao C-H, Chen C-Y. Unity game engine: Interactive software design using digital glove for virtual reality baseball pitch training. Microsyst Technol. 2019; https://doi.org/10.1007/s00542-019-04302-9.
Urbach D, Nebelung W, Becker R, Awiszus F. Effects of reconstruction of the anterior cruciate ligament on voluntary activation of quadriceps femoris a prospective twitch interpolation study. J Bone Jt Surg Br. 2001;83(8):1104–10. https://doi.org/10.1302/0301-620x.83b8.11618.
Vance J, Wulf G, Töllner T, McNevin N, Mercer J. EMG activity as a function of the performer's focus of attention. J Mot Behav. 2004;36(4):450–9. https://doi.org/10.3200/JMBR.36.4.450-459.
Ward SH, Blackburn JT, Padua DA, Stanley LE, Harkey MS, Luc-Harkey BA, Pietrosimone B. Quadriceps neuromuscular function and jump-landing sagittal-plane knee biomechanics after anterior cruciate ligament reconstruction. J Athl Train. 2018;53(2):135–43. https://doi.org/10.4085/1062-6050-306-16.
Welling W, Benjaminse A, Gokeler A, Otten B. Enhanced retention of drop vertical jump landing technique: A randomized controlled trial. Hum Mov Sci. 2016;45:84–95. https://doi.org/10.1016/j.humov.2015.11.008.
Widenhoefer TL, Miller TM, Weigand MS, Watkins EA, Almonroeder TG. Training rugby athletes with an external attentional focus promotes more automatic adaptions in landing forces. Sports Biomech. 2019;18(2):163–73. https://doi.org/10.1080/14763141.2019.1584237.
Wilkerson GB. Neurocognitive reaction time predicts lower extremity sprains and strains. Int J Athl Ther Train. 2012;17(6):4–9. https://doi.org/10.1123/ijatt.17.6.4.
Wu WFW, Porter JM, Brown LE. Effect of attentional focus strategies on peak force and performance in the standing long jump. J Strength Cond Res. 2012;26(5):1226–31. https://doi.org/10.1519/JSC.0b013e318231ab61.
Wulf G. Self-controlled practice enhances motor learning: implications for physiotherapy. Physiotherapy. 2007;93(2):96–101. https://doi.org/10.1016/j.physio.2006.08.005.
Wulf G. Attentional focus and motor learning: a review of 15 years. Int Rev Sport Exerc Psychol. 2013;6(1):77–104. https://doi.org/10.1080/1750984X.2012.723728.
Wulf G, Adams N. Small choices can enhance balance learning. Hum Mov Sci. 2014;38:235–40. https://doi.org/10.1016/j.humov.2014.10.007.
Wulf G, Chiviacowsky S, Schiller E, Ávila LTG. Frequent external focus feedback enhances motor learning. Front Psychol. 2010;1:190. https://doi.org/10.3389/fpsyg.2010.00190.
Wulf G, Dufek JS, Lozano L, Pettigrew C. Increased jump height and reduced EMG activity with an external focus. Hum Mov Sci. 2010;29(3):440–8. https://doi.org/10.1016/j.humov.2009.11.008.
Wulf G, Freitas HE, Tandy RD. Choosing to exercise more: small choices increase exercise engagement. Psychol Sport Exerc. 2014;15(3):268–71. https://doi.org/10.1016/j.psychsport.2014.01.007.
Wulf G, Höß M, Prinz W. Instructions for motor learning: differential effects of internal versus external focus of attention. J Mot Behav. 1998;30(2):169–79. https://doi.org/10.1080/00222899809601334.
Wulf G, Lewthwaite R. Optimizing performance through intrinsic motivation and attention for learning: the OPTIMAL theory of motor learning. Psychon Bull Rev Psychon Bul Rev. 2016. https://doi.org/10.3758/s13423-015-0999-9.
Wulf G, Töllner T, Shea CH. Attentional focus effects as a function of task difficulty. Res Q Exerc Sport. 2007;78(3):257–64. https://doi.org/10.1080/02701367.2007.10599423.
Zachry T, Wulf G, Mercer J, Bezodis N. Increased movement accuracy and reduced EMG activity as the result of adopting an external focus of attention. Brain Res Bull. 2005;67(4):304–9. https://doi.org/10.1016/j.brainresbull.2005.06.035.
Zainuddin Z, Chu SKW, Shujahat M, Perera CJ. The impact of gamification on learning and instruction: a systematic review of empirical evidence. Educ Res Rev. 2020;30:100326. https://doi.org/10.1016/j.edurev.2020.100326.
Funding
There is no funding source.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Diekfuss, J.A., Bonnette, S., Hogg, J.A. et al. Practical Training Strategies to Apply Neuro-Mechanistic Motor Learning Principles to Facilitate Adaptations Towards Injury-Resistant Movement in Youth. J. of SCI. IN SPORT AND EXERCISE 3, 3–16 (2021). https://doi.org/10.1007/s42978-020-00083-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s42978-020-00083-0