
Abstract
To evaluate the content of patient education and cognitive behavioural therapy and its effectiveness in the prevention of migraine for adults, a systematic search was conducted in the databases MEDLINE, EMBASE, PsycINFO and CINAHL. RCTs published in the past 10 years in German or English, reporting on any form of patient education or cognitive behavioural therapy for adult migraineurs, were included. Two reviewers independently searched and evaluated search results. The methodological quality of selected studies was assessed using the Cochrane risk of bias tool 2.0 independently by two reviewers. Data on content and effectiveness were extracted in a predesigned table. Across 1059 records, 14 studies were eligible, including 2266 participants (82,7% females). Contents of patient education included explanations on the link between thoughts and feelings, information on lifestyle influences on headaches, relaxation techniques and stress management, advice on diet and the benefit of physical activity. In addition, patient education focussed on the pathogenesis and diagnostic criteria of migraine, triggering factors and effective acute or prophylactic drug use. Outcome measures included headache frequency, medication intake, function and disability, as well as psychosocial status. Education reduced migraine frequency and improved quality of life. Effect sizes were small, and contents were heterogeneous. Educational and behavioural approaches can positively influence headache frequency. However, the content, duration and frequency and education formats varied widely. The level of evidence for education and cognitive behavioural therapy as a non-pharmacological intervention for migraine is still low. The protocol for the systematic review was registered in the database PROSPERO (PROSPERO 2019 CRD42019134463) prior to the data collection.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
General recommendations for effective management of chronic pain conditions point towards a multimodal approach including self-management, behavioural treatment and education as the most effective interventions [1]. Patient education is not clearly defined and varies largely in descriptive terms and specific aims. Different professional groups attribute different contents to education. Therefore, different terms are used, such as therapeutic patient education, self-management interventions, cognitive behavioural interventions and biobehavioural training (biofeedback, relaxation training, stress management). The evidence for pain neuroscience education to manage chronic pain, in general, is well accepted by clinicians and researchers, and the intervention is successfully used in, e.g., chronic low back pain populations [2, 3] or fibromyalgia populations [4]. The German guideline for low back pain (CLBP) recommends education and cognitive behavioural therapy as the main approach for the management of CLBP [5].
For patients with chronic migraine, national and international guidelines recommend dominantly pharmacological management combining medication for acute symptom management such as triptans and non-steroidal anti-inflammatory drugs with prophylactic drugs. Relaxation exercises, psychological therapy including stress reduction, coping strategies and behavioural therapy, as well as aerobic exercise, are recommended complimentary for the prevention of attacks [6,7,8]. Behavioural therapies, designed to reduce migraine frequency and enhance the quality of life, encourage patients to participate actively in their treatment and to employ self-management strategies, but evidence for their effectiveness is conflicting [9, 10].
According to the World Health Organisation, patient education is provided by health care professionals trained in the education of patients to enhance knowledge about treatment options and to train patients in self-management skills, in adapting the treatment to their specific chronic disease and in coping abilities and processes [11]. For migraine, this includes, e.g., changing maladaptive behaviours and catastrophizing thoughts, which might contribute to headache impact and pain intensity [9].
Research on biobehavioural treatment shows beneficial effects on disability and migraine-specific quality of life, indicating that better migraine self-management will consequently result in reduced migraine frequency and decreased overall drug consumption [9]. Recently, two systematic reviews by Raggi et al. [12] and Probyn et al. [3] reported positive effects of therapeutic patient education (TPE) and other behavioural treatments on the pain and disability of headache patients. However, the inclusion and exclusion criteria of the two reviews focussed on all types of headaches. The overall evidence for patient education to specifically manage migraine symptoms is unclear, especially regarding the contents that should be provided and the format, e.g., duration and frequency of education sessions.
This review is therefore aiming to provide an overview of the current level of evidence for the content, duration, frequency and effectiveness of education and cognitive behavioural therapy for the reduction of pain, disability and psychological outcomes of adults with migraine.
Methods
A systematic review was conducted following the recommendations from the Cochrane Handbook for Systematic Reviews of Interventions and reported according to the criteria of the PRISMA statement [13, 14]. Randomised controlled trials (RCTs) reporting on education or cognitive behavioural therapy (CBT) compared to a control intervention or to any other intervention were selected. Only studies published in English or German language were included.
Participants included in eligible trials had to be 18 years or older and diagnosed with migraine or chronic migraine according to the International Headache Society classification [15, 16]. Headache disorders other than migraine were excluded, but episodic tension-type headache and medication overuse headache were accepted as comorbidities. No restrictions were made for depression and/or anxiety.
RCTs had to focus on an educational or behavioural intervention for migraine. Single interventions, such as biofeedback, progressive muscle relaxation or other relaxation strategies, did not meet the eligibility criteria.
The main outcome measurement was headache frequency. Trials were included if they reported at least one of the following outcome measures: attack frequency per month, pain intensity or duration, drug use, disability, quality of life, depressive symptoms, anxiety, self-efficacy and locus of control. Furthermore, these outcomes had to be reported either for short term (< 3 months), intermediate (between 3 and 12 months), or long-term periods (> 12 months).
Searches in the scientific databases MEDLINE, EMBASE, PsycINFO and CINAHL were limited to publications from the last decade with 01.01.2010 being the first and 29.08.2021 being the final date for publication. An example of a combination of search terms used for Pubmed is presented in Table 1. The search strategy was adapted for each database as necessary. Additional studies were identified by hand searching the literature lists of reviews on the topic and by screening the contents of relevant journals in the field of headache (Headache Journal, Cephalalgia, Journal of Headache and Pain).
Two researchers screened all studies independently at two stages: title and abstract and at full-text level for those studies passing the first stage. A third reviewer was approached if disagreements were not solved in the discussion. The inter-rater reliability for study selection was assessed using Cohen’s kappa coefficient. Results were rated as follows: 0.01–0.20 interpreted as slight agreement, 0.41–0.60 as moderate agreement and 0.81–1.00 as almost perfect or perfect agreement [17]. Outcome data were collected in a predesigned data extraction table by one researcher and controlled for mistakes by the second researcher.
Risk of Bias Assessment
The risk of bias in included studies was evaluated by two researchers independently using the Cochrane risk of bias tool 2.0 [18]. The judgement involved assessing the overall risk of bias as ‘low risk’, ‘high risk’ or ‘some concerns’ with the last category indicating either lack of information or uncertainty about the potential risk of bias. The domains in the risk of bias table were sequence generation (selection bias), allocation sequence concealment (selection bias), blinding of participants and personnel (performance bias), blinding of outcome assessment (detection bias) and other potential sources of bias.
Results
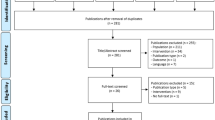
The database search resulted in 1059 records. Fourteen studies were included in the data analysis. These reported on 2266 participants, with the majority being female (82,7%). Figure 1 shows the PRISMA flow diagram of the review process. The Cohen’s k for agreement at abstract level was 0.93, at full-text level 0.94, which was interpreted as almost perfect agreement.

Prisma flow diagram
Table 2 shows the results of the assessment of the risk of bias according to the Risk of Bias Tool 2.0 recommended in the Cochrane Handbook. Three studies were rated with ‘low risk’, seven were rated with ‘some concerns’ and four studies reached a high risk of bias. The inter-rater reliability of the methodological quality assessment was high (Cohen’s k: 0.94, almost perfect agreement). All discrepancies were solved after discussion.
The characteristics of education are described in Table 3. The content of education interventions varied widely, including explanations about the link between thoughts and feelings, between symptoms and behaviours, thought monitoring and relaxation techniques or cognitive restructuring techniques. Behavioural interventions aimed at improving the lifestyle and stress coping, including pain management strategies during an attack, stress relief, advice regarding body posture, diet, attitude, physical activity, handling of emotions or dealing with the pathophysiology of migraine, stress physiology, behavioural management skills, identifying prodromal migraine warning signs and triggers, strategies for managing migraine triggers, effective acute drug use and in one study neuroscience-based information was provided.
Professionals performing education were psychotherapists, health psychologists, psychologists or master-level psychology students under the supervision of a clinical psychologist or trained instructor. Only in one study did family doctors or neurologists provide the education.
The duration and frequency of the behavioural approaches varied and ranged from three sessions of 60 min to 5 weeks with up to 12 weekly 2-h classes plus one retreat day of 6 h with additional training at home for 45 min on 5 days per week. Details are listed in Table 3.
Different educational formats were used, varying from brief-guided self-help CBT, books or leaflets or audiotapes to face-to-face sessions in single or group sessions, as well as internet-based approaches including relaxation audios, videos of patient case studies, interactive exercises and homework. All approaches are detailed in Table 3. Education was often accompanied by adjunct treatment: multimodal therapy, aerobic exercise, prophylactic medical therapy, endurance training, meditation, yoga, relaxation techniques, mindfulness, additional techniques focused on body posture and a healthy lifestyle. The control groups included standard medical or clinical care, as well as prophylactic beta-blockers or waiting lists.
There was great variability in outcome measurements across the studies. Outcomes were related to pain, function and disability, to psychosocial status as well as to days lost due to migraine-related disability. Measurement periods ranged from immediate effects up to 16-month follow-up, but most of the studies reported intermediate effects between 3 and 12 months after the intervention.
Results of two newer studies support that online behavioural training (oBT), as well as a waiting list, resulted in improvements in attack frequency, but only oBT increased self-efficacy, internal and external control and reduced triptan use [25, 30]. The 20-month follow-up of one of the studies [31] showed a stronger improvement in attack frequency for participants with more (4–6) attacks per month at baseline. Wells et al. [32] showed no significant results for the reduction of attack frequency, but improved self-efficacy and mindfulness.
Seminowicz et al. [26] demonstrated a greater reduction in headache days from baseline to 20 weeks post-intervention for mindfulness-based stress reduction (MBSR) compared to stress management for headache (SMH). Fifty-two percent of the MBSR group showed a response to treatment (50% reduction in headache days) compared to 23% in the SMH group (p = 0.004). There were no differences in clinical outcomes at 52 weeks.
In the study by Aguirrazabal et al. [19], 69% of patients (n = 37) in the intervention group (pain neuroscience education) and 34.6% in the control group (n = 18) reported reduced migraine-related work disability by at least 50%.
The results of Seng et al. [27] support that behavioural migraine management increases headache self-efficacy and internal locus of control. A secondary analysis of the data [28] found improvements in cognitive and behavioural responses to migraine (depression and catastrophisation), supporting the results of a web-based intervention designed to increase patient self-efficacy [20]. Simshäuser et al. [29] found that the primary outcome ‘reduction of migraine frequency’ showed no significant group difference, but mindfulness-based stress reduction (MBSR) showed greater improvements in variables related to psychological symptoms, pain self-efficacy and sensory pain perception compared to an education/relaxation group.
Detailed information on the individual interventions can be found in Table 3. In summary, most of the included studies reported a slight positive effect of education and behavioural therapy approaches for the reduction of the migraine frequency and improved quality of life of migraine sufferers as well as a decreased overall drug consumption or reduced migraine-related work disability. Data was not pooled in a meta-analysis due to the heterogeneity of outcome measures and intervention types, duration and delivery methods across studies (see Table 3).
Discussion
This systematic review is providing a comprehensive overview of the current evidence for cognitive behavioural therapy and education for patients with migraine. Results confirm the conclusions of a review published seven years earlier by Kindelan-Calvo et al. [9] about therapeutic patient education for migraine. This current review added 9 studies not included by Kindelan-Calvo et al. [9].
Other systematic reviews by Sullivan et al. [33], Harris et al. [34] and Raggi et al. [12] confirmed this overall positive influence of therapeutic patient education and other behavioural treatments and concluded that the compiled evidence supports the efficacy of psychological interventions on migraine. These reviews – in contrast to the current review – did not restrict the inclusion of migraine but included mixed headache types, making it difficult to draw conclusions on the effectiveness and content of migraine-specific education. Furthermore, children and adolescents were also included in previous reviews. The review by Raggi et al. [12] presented no assessment of the methodological quality of included studies. The review by Probyn et al. [3] reported no effect of education on headache frequency, but only four studies in their review were specifically targeting migraine. In their meta-analysis, Sharpe et al. [10] did not find any evidence that psychological interventions affected migraine frequency or medication usage, migraine-related disability or quality of life in the short term or long term. The authors focussed on psychological types of intervention. Neuroscience content, as in Aguirrazabal [19], was not included.
Two out of these other six reviews on education and behavioural therapy in migraine patients conducted a meta-analysis [9, 10]. All other authors decided against a meta-analysis due to the heterogeneity of content and extent of the interventions, different outcome measures and a low number of studies. Therefore the results of the two meta-analyses should be viewed with caution.
For other chronic pain diseases, such as CLBP, pain neuroscience education has been extensively studied and there is compelling evidence that education addressing the neurophysiology and neurobiology of pain has a positive effect on pain, disability, catastrophisation and physical performance [1, 2]. Previous research already showed some similarities of migraine and CLBP regarding, e.g., the functional connectivity of brain regions which in migraine are equally associated with the pain or salience network [35] as reported for CLBP [36], or behaviourally, altered elements of quantitative sensory testing [37] and reduced tactile acuity [38].
Despite these similarities and the view of migraine as a chronic pain disease, only one of the studies included in this review provided migraine patients with information on the neurophysiology of their pain in a structured or standardised manner [19]. This study was rated as having a low risk of bias, and the group receiving information on the neurophysiology of migraine benefitted more regarding the reduction of migraine attacks compared to routine medical care, thereby indicating that knowledge from CLBP management might be transferable to chronic migraine populations.
Interestingly, in all studies included in this review, psychologists delivered the treatment, while for patients with CLBP, education is commonly provided by physiotherapists. Since the management of especially chronic pain disorders is usually interprofessional, all health professionals including neurologists, psychologists and physiotherapists should be trained to provide education for chronic migraine patients.
The wide range of durations and frequencies of the intervention, as well as of the delivery methods, does not allow for a conclusive recommendation of the most effective behavioural intervention. Moreover, many different terms and definitions were used for the treatment, such as biobehavioural treatments, therapeutic patient education, neuroscience education, cognitive behavioural therapy or mindfulness-based therapy, making it difficult for patients and researchers to recognise these as similar treatment approaches or to recommend such treatment in guidelines. Despite the different names, most approaches share the general focus on lifestyle modifications such as managing stress factors and implementing exercise or relaxation strategies.
For most of the included studies in this review, education was often provided as an adjunct treatment or part of multimodal therapy, and therefore, the explanatory power of the results is restricted. Evidence for a stand-alone treatment is not yet available for patients with migraine.
Within multimodal pain therapy in a hospital, psychological treatments are mandatory [7, 39], while access to psychological therapies or educational or cognitive behavioural treatment outside of a hospital or day-clinic setting is restricted [40]. Only patients with a specific psychiatric or psychological indication (such as anxiety or depression) are usually referred to such treatments. This is in contrast to the guidelines for CLBP, where educational and behavioural approaches are recommended to be included as soon as possible [2, 5].
Clinical Implications
This systematic review revealed, in line with previous reports, some evidence for a positive effect of educational or biobehavioural treatments to decrease headache frequency and disability and to improve self-efficacy and the quality of life in adults with migraine. Therefore, behavioural therapy approaches, especially offered by a multidisciplinary team of specialists in the field of chronic pain management, should be included in any treatment and be accessible to all migraine patients. Besides psychologists providing behavioural treatment, neurologists and physical therapists specialised in the treatment of chronic pain and chronic migraine can provide education and are easier to access for the patients.
Implication for Research
Even though the effectiveness of behavioural approaches is scientifically proven, the content and extent of education are not defined and have to be investigated. Education should include approaches to help patients understand their symptoms from a neurophysiological point of view. It should be investigated whether the evidence of education from other chronic pain syndromes such as CLBP are applicable for chronic migraine. More randomised controlled trials investigating the efficacy of education alone without adjunct treatments are required to disentangle the effects of the various approaches.
Data Availability
All data generated or analysed during this study are included in this published article and its supplementary information files.
Code Availability
Not applicable.
References
Louw A, Diener I, Butler DS, Puentedura EJ. The effect of neuroscience education on pain, disability, anxiety, and stress in chronic musculoskeletal pain. Arch Phys Med Rahabil. 2011;2011(92):2041–56.
Butler D, Moseley GL. Schmerzen verstehen. Springer-Verlag Berlin Heidelberg 2016, 3. Auflage.
Probyn K, Bowers H, Mistry D, Caldwell F, Underwood M, Patel S, Sandhu HK, Matharu M, Pincus T. CHESS team. Non-pharmacological self-management for people living with migraine or tension-type headache: a systematic review including analysis of intervention components. BMJ Open. 2017;7(8):e016670. https://doi.org/10.1136/bmjopen-2017-016670.
Barrenengoa-Cuadra MJ, Muñoa-Capron-Manieux M, Fernández-Luco M, et al. Effectiveness of a structured group intervention based on pain neuroscience education for patients with fibromyalgia in primary care: a multicentre randomized open-label controlled trial. Eur J Pain. 2021;25:1137–49. https://doi.org/10.1002/ejp.1738.
Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV), Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF). Nationale VersorgungsLeitlinie Nicht-spezifischer Kreuzschmerz – Kurzfassung, 2. Auflage. Version 1. 2017 [cited: 2019–07–16]. https://doi.org/10.6101/AZQ/000377. www.kreuzschmerz.versorgungsleitlinien.de.
American Headache Society position statement on integrating new migraine treatments into clinical practice. Headache: J Head Face Pain. 2019;59:1–18. https://doi.org/10.1111/head.13456.
Diener HC, Gaul C, Kropp P et al. Therapie der Migräneattacke und Prophylaxe der Migräne, S1-Leitlinie. Deutsche Gesellschaft für Neurologie (Hrsg.). Leitlinien für Diagnostik und Therapie in der Neurologie. 2018.
Kropp P, Meyer B, Dresler T, et al. Entspannungsverfahren und verhaltenstherapeutische Interventionen zur Behandlung der Migräne. Leitlinie der Deutschen Migräne- und Kopfschmerzgesellschaft. Schmerz. 2017;31:433–47.
Kindelan-Calvo P, Gil-Martínez A, Paris-Alemany A, et al. Effectiveness of therapeutic patient education for adults with migraine. A systematic review and meta-analysis of randomized controlled trials. Pain Med. 2014;15:1619–36.
Sharpe L, Dudeney J, Williams ACDC, Nicholas M, McPhee I, Baillie A, Welgampola M, McGuire B. Psychological therapies for the prevention of migraine in adults. Cochrane Database Syst Rev. 2019;7:CD012295. https://doi.org/10.1002/14651858.CD012295.pub2.
World Health Organization. Regional Office for Europe. Therapeutic patient education: continuing education programmes for health care providers in the field of prevention of chronic diseases: report of a WHO working group. Copenhagen: WHO Regional Office for Europe. 1998. https://apps.who.int/iris/handle/10665/108151. Accessed 30 Dec 2021.
Raggi A, Grignani E, Leonardi M, Andrasik F, Sansone E, Grazzi L, D’Amico D. Behavioral approaches for primary headaches: recent advances. Headache. 2018;58(6):913–25. https://doi.org/10.1111/head.13337.
Higgins JPT, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions. 2nd ed. Chichester (UK): Wiley; 2019.
Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. BMJ. 2009;339:b2535. https://doi.org/10.1136/bmj.b2535
Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211.
Headache Classification Committee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia. 2013;33(9):629–808.
McHugh ML. Interrater reliability the kappa statistic. Biochem Med (Zagreb). 2012;22(3):276–82.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, Cates CJ, Cheng H-Y, Corbett MS, Eldridge SM, Hernán MA, Hopewell S, Hróbjartsson A, Junqueira DR, Jüni P, Kirkham JJ, Lasserson T, Li T, McAleenan A, Reeves BC, Shepperd S, Shrier I, Stewart LA, Tilling K, White IR, Whiting PF, Higgins JPT. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366: l4898.
Aguirrezabal I, de San Pérez, Román MS, Cobos-Campos R, Orruño E, Goicoechea A, Martínez de la Eranueva R, Arroniz M, Uzquiza E. Effectiveness of a primary care-based group educational intervention in the management of patients with migraine a randomized controlled trial. Prim Health Care Res Dev. 2019;13(20):e155.
Bromberg J, Wood ME, Black RA, Surette DA, Zacharoff KL, Chiauzzi EJ. A randomized trial of a web-based intervention to improve migraine self-management and coping. Headache. 2012;52(2):244–61. https://doi.org/10.1111/j.1526-4610.2011.02031.x.
Cousins S, Ridsdale L, Goldstein LH, et al. A pilot study of cognitive behavioural therapy and relaxation for migraine headache: a randomised controlled trial. J Neurol. 2015. https://doi.org/10.1007/s00415-015-7916-z.
Hedborg K, Muhr C. Multimodal behavioral treatment of migraine: an Internet-administered, randomized, controlled trial. Upsala J Med Sci. 2011;116:169–86.
Hedborg K, Muhr C. The influence of multimodal behavioral treatment on the consumption of acute migraine drugs: a randomized, controlled study. Cephalalgia. 2012. https://doi.org/10.1177/0333102412437386.
Holroyd K, Cottrell CK, O’Donnell FJ, et al. Effect of preventive (β blocker) treatment, behavioural migraine management, or their combination on outcomes of optimised acute treatment in frequent migraine: randomised controlled trial. BMJ. 2010;341: c4871.
Kleiboer A, Sorbi M, van Silfhout M, et al. Short-term effectiveness of an online behavioral training in migraine self-management: a randomized controlled trial. Behav Res Ther. 2014. https://doi.org/10.1016/j.brat.2014.07.009
Seminowicz DA, Burrowes SAB, Kearson A, Zhang J, Krimmel SR, Samawi L, Furman AJ, Keaser ML, Gould NF, Magyari T, White L, Goloubeva O, Goyal M, Peterlin BL, Haythornthwaite JA. Enhanced mindfulness-based stress reduction in episodic migraine: a randomized clinical trial with magnetic resonance imaging outcomes. Pain. 2020;161(8):1837–46. https://doi.org/10.1097/j.pain.0000000000001860.
Seng EK, Holroyd KA. Dynamics of changes in self-efficacy and locus of control expectancies in the behavioral and drug treatment of severe migraine. Ann Behav Med. 2010. https://doi.org/10.1007/s12160-010-9223-3.
Seng EK, Holroyd KA. Behavioral migraine management modifies behavioral and cognitive coping in people with migraine. Headache. 2014. https://doi.org/10.1111/head.12426.
Simshäuser K, Lüking M, Kaube H, Schultz C, Schmidt S. Is mindfulness-based stress reduction a promising and feasible intervention for patients suffering from migraine? A randomized controlled pilot trial. Complement Med Res. 2020;27(1):19–30. https://doi.org/10.1159/000501425.
Sorbi MJ, Kleiboer AM, van Silfhout HG, Vink G, Passchier J. Medium-term effectiveness of online behavioral training in migraine self-management: a randomized trial controlled over 10 months. Cephalalgia. 2015. https://doi.org/10.1177/0333102414547137
Sorbi MJ, Balk Y, Kleiboer,AM, Couturier EG. Follow-up over 20 months confirms gains of online behavioural training in frequent episodic migraine. Cephalalgia. 2017. https://doi.org/10.1177/0333102416657145
Wells RE, Burch R, Paulsen RH, Wayne PM, Houle TT, Loder E. Meditation for migraines: a pilot randomized controlled trial. Headache. 2014;54(9):1484–95. https://doi.org/10.1111/head.12420.
Sullivan A, Cousins S, Ridsdale L. Psychological interventions for migraine: a systematic review. J Neurol. 2016;263(12):2369–77. https://doi.org/10.1007/s00415-016-8126-z.
Harris P, Loveman E, Clegg A, Easton S, Berry N. Systematic review of cognitive behavioural therapy for the management of headaches and migraines in adults. Br J Pain. 2015;9(4):213–24. https://doi.org/10.1177/2049463715578291.
Chong CD, Schwedt TJ, Hougaard A. Brain functional connectivity in headache disorders: a narrative review of MRI investigations. J Cereb Blood Flow Metab. 2019;39(4):650–69. https://doi.org/10.1177/0271678X17740794.
Kim J, Mawla I, Kong J, Lee J, Gerber J, Ortiz A, Napadow V. Somatotopically specific primary somatosensory connectivity to salience and default mode networks encodes clinical pain. PAIN. 2019;160(7):1594–1605. https://doi.org/10.1097/j.pain.0000000000001541
Nahman-Averbuch H, Shefi T, Schneider VJ, Li D, Ding L, King CD, Coghill RC. Quantitative sensory testing in patients with migraine. Pain. 2018;159(7):1202–23. https://doi.org/10.1097/j.pain.0000000000001231.
Luedtke K, Adamczyk W, Mehrtens K, Moeller I, Rosenbaum L, Schaefer A, Wollesen B. Upper cervical two-point discrimination thresholds in migraine patients and headache-free controls. J Headache Pain. 2018;19(1).https://doi.org/10.1186/s10194-018-0873-z
Gaul C, Lieseruing-Latta E, Schäfer B, et al. Integrated multidisciplinary care of headache disorders: a narrative review. Cephalalgia. 2016;36(12):1181–91.
Fritsche G, Kröner-Herwig B, Kropp P, et al. Psychologische Prävention der Migräne. Systematische Übersicht Der Schmerz. 2013;27:263–74.
Funding
Open Access funding enabled and organized by Projekt DEAL. There were no other sources of support (internal and external) than the funding source for the corresponding author RM of the Friedrich-Ebert-Stiftung, doctoral funding, Godesberger Allee 149, 53175 Bonn.
Author information
Authors and Affiliations
Contributions
RM and AS searched, excluded or included and rated the quality of the studies. All three authors interpreted the results and contributed to the writing process. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
Not applicable.
Consent to Participate
As no patients were included in this present study, no informed consent was necessary. All studies included in this review stated that informed consent was obtained. Thus, the standards of good scientific practice were met.
Consent for Publication
Not applicable.
Competing Interests
The authors declare no competing interests. There are no amendments between protocol and review (PROSPERO 2019 CRD42019134463) available from https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=134463.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Medicine
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Meise, R., Schwarz, A. & Luedtke, K. Effectiveness of Patient Education and Cognitive Behavioural Treatment as a Non-Pharmacological Intervention for Migraine in Adults – a Systematic Review. SN Compr. Clin. Med. 4, 197 (2022). https://doi.org/10.1007/s42399-022-01279-x
Accepted:
Published:
DOI: https://doi.org/10.1007/s42399-022-01279-x