
Abstract
Purpose
To evaluate the characteristics of patients referred for dizziness to a Syncope Unit.
Methods
This is a retrospective study. Of 491 patients referred to the Syncope Unit of Careggi Hospital in 2015, 198 (40.3%) who experienced dizziness alone or associated with a history of transient loss of consciousness were enrolled. All the patients underwent an initial evaluation according to the European Society of Cardiology guidelines on syncope. We compared the clinical characteristics and final diagnosis of patients referred for dizziness alone (n = 64) to those of patients with dizziness and history of transient loss of consciousness (n = 134).
Results
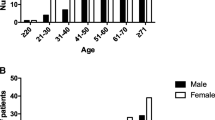
The study population had a mean age of 62 ± 20 years (range 16–96 years) and 101 (51%) were female. A final diagnosis of pre-syncope was made in about the 80% of the patients without a previous history of transient loss of consciousness. In this group, other diagnoses were benign paroxysmal positional vertigo (6.3%), transient ischemic attack (4.7%) or psychogenic dizziness (7.8%). Syncope was diagnosed in the 82.7% of the patients with dizziness and history of transient loss of consciousness.
Conclusion
Dizziness was the main reason for referral to the Syncope Unit in almost one-third of the patients, in whom pre-syncope was the most frequent final diagnosis. Otological, neurological and psychiatric disorders should be also considered as differential diagnosis, highlighting the importance of a multidisciplinary approach.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of dizziness is around 15–30% in the general population and 54% in the oldest old [1]. Dizziness represents one of the most frequently aspecific reasons for referral to the Emergency Department, after falls and balance disorders [2], and according to Drachman et al. [3] it is often identified as vertigo, pre-syncope, disequilibrium or lightheadedness. “Vertigo” refers to the illusion of environmental motion, classically described as “spinning” or “whirling”, and always it reflects dysfunction at some level of the vestibular system. Pre-syncope means that the patient senses impending loss of consciousness, without experienced a complete loss of consciousness. Disequilibrium represents a disturbance in balance or coordination such that confident ambulation is impaired. Lightheadedness refers to a sensation “in the head” that is clearly not vertiginous or pre-syncopal, and that is not invariably related to ambulation [3]”. Given its heterogeneity, dizziness is managed from different specialists [4].
The aim of the present study is to evaluate retrospectively the clinical characteristics and management of patients referred for dizziness to a Syncope Unit.
Methods
Between January and December 2015, 491 patients were referred to the Syncope Unit of Careggi University Hospital; 198 patients (40.3%), who experienced dizziness alone or associated with a history of Transient-Loss of Consciousness (T-LOC), have been enrolled and underwent an initial evaluation according to the European Society of Cardiology guidelines on syncope [5]. The initial evaluation consisted of a careful clinical history, a physical examination (including blood pressure measurements in supine and standing position) and 12-lead electrocardiogram (ECG) [5]. Those patients in whom a reliable diagnosis could not be achieved after the initial evaluation, underwent a complete neuro-autonomic evaluation including Tilt Testing (TT) in baseline conditions and, when negative for 15 min, after administration of sublingual nitro-glycerine, according to a validated protocol [6]. The test was considered positive if induction of either reflex hypotension/bradycardia was associated with symptoms reproduction [5]. Neurally mediated syncope was defined according to the VASIS classification (Vasovagal Syncope International Study) [7]. TT was also a diagnostic tool for the assessment of autonomic failure, especially for the reproduction of delayed orthostatic hypotension (which could not be detected by active standing because of its delayed onset) and postural orthostatic tachycardia syndrome (POTS).
Carotid Sinus Massage (CSM) was performed according to the “method of symptoms” in the supine and upright position, 3 min after the beginning of the upright phase of the TT [8]. TT and CSM were performed under continuous ECG and blood pressure beat-to-beat monitoring (Task Force Monitor, CNSystems Medizin-technik, Austria). A diagnosis of Carotid Sinus Syndrome (CSS) was made if CSM caused bradycardia (asystole) and/or hypotension, reproducing spontaneous symptoms [5]. A written, informed consent to perform neuro-autonomic evaluation was obtained from each patient.
In case of unexplained episodes after a complete diagnostic work-up, patients were referred to a third level evaluation performed by cardiologist, neurologist, audiologist or psychiatrist.
We have compared the clinical characteristics and final diagnosis of patients referred for dizziness alone (n = 64) to those of patients with dizziness and history of T-LOC (n = 134).
All the information were recorded from patients as part of the routine clinical care, and collected into a database anonymously, for the purpose of the present analysis.
No Ethics Committee formal approval was needed for this study, as recent Italian Legislation [General Authorization to Process Personal Data for Scientific Research Purposes-1 March 2012 (web document no. 1884019)] conceded that, in case of retrospective studies, where no intervention was made on patients, who had given informed consent to the use of their clinical data, Ethics Committee should only be informed.
Statistical analysis
Statistical analysis was performed using SPSS version 23. Student’s t test for unpaired data was used to compare continuous data between groups. The χ2 test was used to compare dichotomous variables. A p value < 0.05 was considered significant. Data were reported as mean ± standard deviation or as percentages.
Results
The prevalence of dizziness in the population referred to our Syncope Unit in 1 year, was 50%. The characteristics of patients referred for dizziness alone (n = 64), and of those patients with dizziness and history of transient loss of consciousness (n = 134) are listed in Table 1. Patients without history of syncope, experienced dizziness more often without predisposing factors and precipitating events as postural changes, exercise, micturition, defecation, cough, swallowing (64.1 vs 78.4%, p = 0.034). A history of orthostatic hypotension was significantly more frequent in patients with a history of T-LOC, compared to those with dizziness alone (43.3 vs 28.1%, p 0.04). The tests performed in Syncope Unit are listed in Table 2. Dizzy patients without history of T-LOC, had a positive response to TT in the 61.9% of the test performed (13/21), showing mostly vaso-depression.
The different final diagnosis are reported in Table 3. A final diagnosis of pre-syncope was made in about the 80% of the patients without a previous history of T-LOC. Patients without history of T-LOC had a final diagnosis of benign paroxysmal positional vertigo (6.3%), transient ischemic attack (4.7%) or psychogenic dizziness (7.8%), as confirmed by audiologist, neurologist or psychiatrist after a third level evaluation, performed when the diagnostic work-up in Syncope Unit was negative.
Syncope was diagnosed in the 82.7% of the patients with dizziness and history of T-LOC.
Discussion
Syncope is a very common condition, with quite various clinical presentations and prodromal symptoms, especially in the older patient. It is also known the overlap with symptoms that fall into the spectrum of vertigo districts, as indeed dizziness, which is one of the most frequent reasons for referral to the ED after falls and balance disorders. In this clinical context a wide and standardized evaluation in a specific syncope clinic may be beneficial [9]. To the best of our knowledge, this is the first research paper assessing features of patients with dizziness in a Syncope Unit. Lawson et al. [10] have previously reported a 33% of dizziness in patients referred to the Falls and Syncope Unit in Newcastle in 1 year, focusing only on vestibular disorders.
A multidisciplinary care pathway, based on current guidelines of syncope and falls, has already been developed to evaluate unexplained non-accidental falls and/or syncope in geriatric patients [11]. Indeed, the management of falls and syncope in a geriatric population is challenging, because in up to 60% of the cases a witness account is not available and about 35% of the patients are left without a good explanation for their syncope. Thus, older patients with frequent unexplained falls and/or syncope visit different specialists, undergo various diagnostic tests, which sometimes are also repeated more than once, extending the time for diagnosis. Furthermore, it may be questioned whether all the patients have undergone the appropriate diagnostic pathway. The same applies to geriatric patients with dizziness, not always related to syncopal or pre-syncopal mechanism, but rather due to labyrinthine disorders, transient ischemic attack or psychogenic dizziness.
All the patients referred for dizziness without history of T-LOC, received a diagnosis at the end of the diagnostic work-up: a pre-syncope was most frequently diagnosed. A similar prevalence of pre-syncope was identified by O’Mahony et al. [12] in a smaller sample of geriatric patients. Different diagnosis, have been identified in the 20% of patients with dizziness alone as transient ischemic attack, psychogenic dizziness and vestibular vertigo, according to previous studies [10, 13].
Orthostatic dizziness is defined as a non-vertiginous dizziness occurring when patient passes from the supine or seated to the upright position [14]. It is often complained as an impending loss of consciousness or light-headedness [15]. This condition accounts for the 42% of generic dizziness and for the 55% of non-vestibular dizziness and the prevalence increases with the age. It is common belief that orthostatic dizziness depends on orthostatic hypotension, although they must in fact be considered distinctly [16]. Kim et al. [15] demonstrated that only the 51% of the patients with orthostatic dizziness had orthostatic hypotension, mostly the classic or delayed type [5, 13]. Jeon et al. [17] showed that the second more frequent diagnosis was benign paroxysmal positional vertigo.
The relationship between orthostatic dizziness and orthostatic hypotension is not completely understood and future research studies are needed.
Limits
A possible limitation of the present study is the selected sample, not representing the general population of patients with dizziness.
In defining the concept of dizziness, we referred to the definition proposed by Drachman et al. [3], because the most recent definition of the International Classification of Vestibular Disease [18] is too generalizing and not entirely applicable to a sample of complex patients, as ours.
Conclusions
The Syncope Unit can play an important role in the assessment of patients with dizziness, as confirmed by the present study in which pre-syncope and syncope, initially suspected as the underlying mechanism of dizziness, have been confirmed in the 80% of cases. Selected patients should then be managed and treated according to the European Society of Cardiology Guidelines of Syncope [5] and, when needed, referred to a multidisciplinary approach, considering possible otological, neurological or psychiatric nature of dizziness.
References
Gassmann KG, Rupprecht R, IZG Study Group (2009) Dizziness in an older community dwelling population: a multifactorial syndrome. J Nutr Health Aging 13(3):278–282
Nemec M, Koller MT, Nickel CH, Maile S, Winterhalder C, Karrer C et al (2010) Patients presenting to the emergency department with non-specific complaints: the Basel Non-specific Complaints (BANC) Study. Acad Emerg Med 17(3):284–292
Drachman DA, Hart CW (1972) An approach to the dizzy patient. Neurology 22(4):323–334
Lin HW, Bhattacharyya N (2012) Balance disorders in the elderly: epidemiology and functional impact. Laryngoscope 122(8):1858–1861
Brignole M, Moya A, de Lange FJ et al (2018) 2018 ESC Guidelines for the diagnosis and management of syncope. The Task Force for the diagnosis and management of syncope of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA). Eur Heart J 1–69
Bartoletti A, Alboni P, Ammirati F et al (2000) “The Italian Protocol”: a simplified head-up tilt testing potentiated with oral nitroglycerin to assess patients with unexplained syncope. Europace 2:339–342
Brignole M, Menozzi C, Del Rosso A, Vasovagal Syncope International Study et al (2000) New classification of haemodynamics of vasovagal syncope: beyond the VASIS classification. Analysis of the pre-syncopal phase of the tilt test without and with nitroglycerin challenge. Europace 2:66–76
Puggioni E, Guiducci V, Brignole M et al (2002) Results and complications of the carotid sinus massage performed according o the ‘‘method of symptoms’’. Am J Cardiol 89:599–601
O’Dwyer C, Kenny RA (2010) Syncope clinics and the older adult. Eur Geriatr Med 1:41–44
Lawson J, Johnson I, Bamiou DE, Newton JL (2005) Benign paroxysmal positional vertigo: clinical characteristics of dizzy patients referred to a Falls and Syncope Unit. QJM 98(5):357–364
Wold GFH, Ruiter JH, Cornel JH, Vogels RLC, Jansen RWMM (2015) A multidisciplinary care pathway for the evaluation of falls and syncope in geriatric patients. Eur Geriatr Med 6:487–494
O’Mahony D, Foote C (1998) Prospective evaluation of unexplained syncope, dizziness, and falls among community-dwelling elderly adults. J Gerontol A Biol Sci Med Sci 53(6):M435–M440
Aoki M (2017) The impaired subjective perception of verticality independent of peripheral vestibular function in dizzy elderly with orthostatic hypotension. Aging Clin Exp Res 29:647–653
Baloh R, Kerber K (2011) Baloh and Honrubia’s clinical neurophysiology of the vestibular system, 4th edn. Oxford University Press, Oxford
Kim HA, Lee H, Park KJ, Lim JG (2013) Autonomic dysfunction in patients with orthostatic dizziness: validation of orthostatic grading scale and comparison of Valsalva maneuver and head-up tilt testing results. J Neurol Sci 325(1–2):61–66
Radtke A, Lempert T, von Brevern M, Feldmann M, Lezius F, Neuhauser H (2011) Prevalence and complications of orthostatic dizziness in the general population. Clin Auton Res 21(3):161–168
Jeon EJ, Park YS, Park SN, Park KH, Kim DH, Nam IC et al (2013) Clinical significance of orthostatic dizziness in the diagnosis of benign paroxysmal positional vertigo and orthostatic intolerance. Am J Otolarngol 34(5):471–476
Bisdorff A, von Brevern M, Lempert T et al (2009) Classification of vestibular symptoms: towards an international classification of vestibular disorders. J Vestib Res 19(1–2):1–13
Funding
This research did not receive any specific Grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Ceccofiglio, A., Peruzzi, G., Pecci, R. et al. Retrospective analysis of patients with dizziness evaluated in Syncope Unit: a real life experience. Eur Geriatr Med 9, 383–387 (2018). https://doi.org/10.1007/s41999-018-0058-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41999-018-0058-y