
Abstract
The present study explored the 18-kDa translocator protein radioligand 18F-PBR06 as a PET imaging biomarker for diagnosis of inflammation and compared it with 18F-FDG for differentiation of inflammation and lung tumors in animals. 18F-PBR06 was synthesized with an average decay-corrected radiochemical yield of 30–40% (end of synthesis, EOS), and the radiochemical purity was greater than 99%. The inflammation-to-blood ratio of 18F-PBR06 (3.53 ± 0.26) was higher than the tumor-to-blood ratio (1.77 ± 0.35) (P < 0.001). The inflammation-to-muscle ratio of 18F-PBR06 (2.33 ± 0.64) was also higher than the tumor-to-muscle ratio (1.45 ± 0.14) (P = 0.036). Micro-PET/CT images showed high uptake of 18F-FDG in both inflamed muscles and lung tumor tissues. However, 18F-PBR06 uptake in inflamed muscles remained higher than that in the lung tumor tissues, following 90 min of dynamic Micro-PET/CT imaging. Further, macrophages in the inflammatory regions showed a higher fluorescence signal than in lung tumor tissues. Results of the study confirmed that 18F-PBR06 PET/CT imaging allowed for diagnosis of inflammation. Moreover, 18F-PBR06 uptake in the inflammatory regions was significantly higher than in lung tumor tissues, suggesting that 18F-PBR06 PET/CT imaging has potential to differentiate between peripheral lung cancer and inflammation nodules.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
Inflammation is a common defense reaction to injury in vascularized living tissues, which is shared by many diseases [1]. Positron emission tomography (PET) imaging using fluorine-18-fluorodeoxyglucose (18F-FDG) has been widely used to evaluate focal and generalized infectious and inflammatory disorders [2]. Further, 18F-FDG PET/CT imaging has been widely used in tumor detection, staging, and therapy response monitoring [3, 4]. Therefore, inflammation-specific imaging tracers are needed to provide more accurate diagnosis of inflammatory diseases and better understanding of the pathological process.
Accurate pulmonary nodule detection is a crucial step in diagnosing pulmonary cancer [5]. Currently, differentiating peripheral lung cancer and inflammation nodules remains a fundamental unsolved problem [6]. Alternative methods for distinguishing between peripheral lung cancer and inflammation nodules include delayed PET/CT imaging of 18F-FDG uptake [7]. However, results of delayed 18F-FDG PET/CT imaging may provide additional false positive results due to its low specificity. Thus, it is essential to develop an inflammation-specific tracer to provide more accurate diagnosis of pulmonary cancer.
Furthermore, macrophages play a significant role in inflammation progression [8]. In inflammation progression, macrophages are activated to defend against invasive pathogens. Following activation, the recruited macrophages act either as defenders against invasive pathogens or promoters to stimulate local inflammatory responses by releasing various chemokines and cytokines, thereby serving as appropriate biological targets for inflammation-specific PET imaging tracers [9, 10].
The translocator protein (TSPO), also known as peripheral benzodiazepine receptor (PBR), is a 18-kDa outer mitochondrial membrane protein that participates in the regulation of numerous cellular processes, including cholesterol metabolism, steroid biosynthesis, cellular proliferation, and apoptosis [11, 12]. This protein is localized on the outer mitochondrial membrane of several cell types, including macrophages, neutrophils, and glioma cells, and has been shown to exhibit low expression in many tumor cells [11, 12]. This evidence indicated that TSPO tracers have greater potential as tracers to specifically target inflammation and to differentiate between peripheral lung cancer and inflammation nodules. 18F-N-fluoroacetyl-N-(2,5-dimethoxybenzyl)-2-phenoxyaniline (18F-PBR06) is a second-generation PET-targeting TSPO tracer, which has been used in human studies, and has increased binding affinity, higher signal-to-noise ratio, and low lipophilicity [12,13,14]. Previously, 18F-PBR06 has displayed high uptake in neuroinflammation [15]; however, the potential to detect inflammation in peripheral tissues has not yet been evaluated.
In this study, we performed Micro-PET/CT imaging using 18F-PBR06 and 18F-FDG in rodent lung tumor and inflammation models. Herein, we aimed to investigate the feasibility of these tracers to detect and differentiate between inflammation and lung tumors.
2 Materials and methods
2.1 Synthesis of PET tracers
The radiotracer 18F-FDG was manufactured via a fully automated FDG MX module (GE Medical Systems, Germany). The radiochemical purity of 18F-FDG was > 98%.
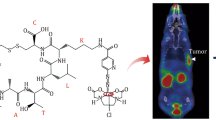
An automated TRACERlab FXF-N radiosynthetic module (GE Medical Systems, USA) was used to prepare 18F-PBR06 as previously reported [16]. Further, 18F-PBR06 was synthesized using a novel tosylate precursor as described previously [17]. The synthetic procedures of 18F-PBR06 are shown in Fig. 1a. Radiosynthesis of 18F-PBR06 using the new tosylated precursor provided similar radiochemical purity, higher specific activity, and higher radiochemical yield in comparison with radiosynthesis using bromine precursor [17]. The decay-corrected radiochemical yields of 18F-PBR06 were 30–40% (end of synthesis, EOS), and the radiochemical purity of 18F-PBR06 was greater than 99%.

a Synthetic procedures of 18F-PBR06 using a novel tosylate precursor. b Radio-HPLC analysis of 18F-PBR06. c Flow chart of the animal study design. Models of inflammation and lung cancer (n = 3 each) were used for 18F-FDG Micro-PET/CT imaging, followed by 18F-PBR06 Micro-PET/CT imaging 3 days later. Subsequently, the animals were killed for immunofluorescence analysis (Color online)
2.2 Animal models
The animal study protocol was in accordance with the principles and procedures outlined in the Guide for the Care and Use of Laboratory Animals and approved by Zhongshan Hospital. FVB/N (FVB) and athymic nude mice (both female, 6–8 weeks) were purchased from Peking University Laboratory Animal Center (Beijing, China). Each athymic nude moue was inoculated with 2 × 106 A549 lung cancer tumor cells to establish the lung cancer model. When the A549 tumor volumes in athymic nude mice reached 0.5 cm3, the FVB mice were injected with 20 µL turpentine into the muscles of their left hind legs to establish the inflammation model. In total, 14 animals were used in the whole study. Three mice each of inflammation and lung cancer models were used for 18F-FDG Micro-PET/CT imaging and 18F-PBR06 Micro-PET/CT imaging. Subsequently, the animals were killed for immunofluorescence analysis (Fig. 1c). Further, additional four mice each of inflammation and lung cancer models were used for the biodistribution study. All mice were maintained in a temperature-controlled environment under a 12-h light/dark cycle with free access to food and water.
2.3 Biodistribution studies for 18F-PBR06
The inflammation and lung cancer models were intravenously injected with 5.56 MBq of 18F-PBR06 (n = 4) and killed 120 min later by ethyl ether anesthesia. Blood was collected from the heart, and normal tissues (kidneys, brain, liver, spleen, intestine, lung, stomach, pancreas, and muscles of the right hind leg), inflamed muscles, and A549 tumors were excised. All samples were weighed, and the radioactivity was measured by a GC-1200 gamma counter (HYMI-1403-015), followed by decay correction. Tracer accumulations of a three-dimensional region of interest (3D-ROI) for a volume were calculated as follows: 3D-ROI = (radioactivity of organs/radioactivity of injected drugs)/quality of organs. The results were expressed as the percentage of injected dose per gram of tissue (% ID/g).
2.4 Micro-PET/CT imaging
A Siemens Inveon Micro-PET/CT scanner (Siemens Preclinical Solutions, Knoxville, TN, USA) was used for Micro-PET/CT scans and imaging analysis. For the inflammation models, 10-min PET images and 5-min CT images were acquired on day 4 post-injection of turpentine oil at 1 h following the 5.56 MBq 18F-FDG injection via the tail vein. Furthermore, 1.5-h dynamic PET images and 5-min CT images were obtained on day 7 post-injection of turpentine oil following the 5.56 MBq 18F-PBR06 injection via the tail vein. For the lung cancer models, 10-min PET images and 5-min CT images were performed at 1 h following the 5.56 MBq 18F-FDG injection via the tail vein on day 25 post-inoculation. Subsequently, 1.5-h dynamic PET images and 5-min CT images were performed following the 5.56 MBq 18F-PBR06 injection via the tail vein on day 28. The data were reconstructed using a 3D OSEM algorithm and segmented attenuation. 3D-ROIs were placed on the inflamed lesions or tumor tissues, and a threshold of 40% of the maximum uptake was used for the final ROI drawing.
2.5 Immunofluorescence
The inflammatory regions on day 7 after turpentine injection and lung cancer models on day 28 after inoculation into mice were excised and embedded in paraffin. The inflamed muscle slices and tumor tissue sections were incubated with rabbit anti-CD68 antibody (1:100, Abcam, USA) for 1 h, followed by Cy3-conjugated anti-rabbit secondary antibodies (1:200, Jackson Immuno Research Laboratories) for 30 min in the dark at room temperature. After washing with PBS, the slices were mounted with VECTASHIELD® mounting medium containing DAPI and coverslipped before visualization by epifluorescence microscopy (IX-81, Olympus).
2.6 Statistical analysis
The data are expressed as mean and standard deviation (SD). P-values < 0.05 were considered statistically significant.
3 Results and discussion
3.1 Biodistribution of 18F-PBR06
The biodistribution data of 18F-PBR06 in the inflammation and tumor models achieved at 120 min post-injection are presented in Fig. 2a. 18F-PBR06 displayed higher uptake in the inflamed lesions (4.79 ± 0.48), whereas relatively lower uptake in the lung tumor tissues (1.55 ± 0.29) (P < 0.001) was found. Considering that accumulation in the brain, spleen, lung, blood, kidneys, right hind leg muscles, and intestines of the inflammation models was higher than of the lung cancer models (all P < 0.05), we used the target-to-nontarget ratios at 120 min post-injection in the animal models to explore the potential of 18F-PBR06 to differentiate the inflamed lesions from lung tumor tissues.

a Biodistribution of 18F-PBR06 at 2 h in inflammation and lung cancer models. b Parameters of target to nontarget at 2 h after injection in inflammation and lung cancer models (Color online)
The ratio of inflammation to blood (I/B) was 3.53 ± 0.26, and the ratio of tumor to blood (T/B) was 1.77 ± 0.35 (P < 0.001). The ratio of inflammation to muscle (I/M) was 2.33 ± 0.64, and the ratio of tumor to muscle (T/M) was 1.45 ± 0.14 (P = 0.036). The results revealed that 18F-PBR06 had relatively high uptake in the inflammatory regions, and accumulation of 18F-PBR06 in the lung tumor tissues was lower than in the inflammatory regions.
3.2 Micro-PET/CT imaging
The time activity curves obtained from the dynamic Micro-PET/CT imaging of 18F-PBR06 are shown in Fig. 3, indicating that 18F-PBR06 uptake in the inflamed muscles remained higher than normal muscles during the 90 min of dynamic Micro-PET/CT imaging (all P < 0.05). Moreover, 18F-PBR06 uptake in the inflamed muscles remained higher than tumor tissues. Based on the biodistribution results, it further confirmed the specificity of 18F-PBR06 for TSPO evaluation.

a Time activity curves (TACs) of inflamed muscles during 90-min 18F-PBR06 dynamic Micro-PET/CT imaging. b TACs of lung tumor tissues during 90-min 18F-PBR06 dynamic Micro-PET/CT imaging (Color online)
Figure 4 shows the Micro-PET/CT images of both tracers obtained from the inflammation and lung cancer models. All images were viewed from the top. 18F-FDG showed high uptake in both inflamed muscles and lung tumor tissues. However, 18F-PBR06 showed high uptake in inflamed muscles, but low uptake in lung tumor tissues. The results revealed that, compared to 18F-FDG, 18F-PBR06 showed superior specificity for inflammation.

18F-PBR06 and 18F-FDG images of an inflammation model and lung cancer model. a, d, g, j Coronal views; b, e, h, k transverse views; and c, f, i, l sagittal views. 18F-FDG accumulation showed high uptake during inflammation (g–i). 18F-FDG accumulation showed high uptake in A549 tumor tissues (j–l). 18F-PBR06 accumulation showed high uptake during inflammation (a–c). 18F-PBR06 accumulation showed low uptake in A549 tumor tissues (d–f) (Color online)
3.3 Immunofluorescence
Immunofluorescence staining revealed macrophages in all specimens of the inflammation and lung cancer models. As shown in Fig. 5, macrophages in the inflammatory regions showed a higher fluorescence signal than the lung tumor tissue. These results revealed that the number of macrophages in the inflammatory regions was significantly higher than the lung tumor tissue. Therefore, the amount of TSPO in the inflammatory regions was also significantly higher than the lung tumor tissue. These results were consistent with the biodistribution and Micro-PET/CT imaging results.

Immunofluorescence of a specimen excised from an inflammation model and lung cancer model. A specimen from an inflamed muscle (a–c) and A549 tumor (d–f) (all samples were stained with CD68+ and magnified × 200). The nuclei were stained blue, and TSPO was stained green. a, d Merged images, and the fluorescence signal of TSPO in inflamed muscle was much higher than the A549 tumor (Color online)
3.4 Statistical analysis
The time activity curves obtained from the dynamic Micro-PET/CT imaging of 18F-PBR06 revealed higher uptake in the inflamed muscles than lung tumor tissues during the 90-min imaging (all P < 0.05). Biodistribution demonstrated that the parameters of inflammation to blood in 18F-PBR06 were significantly higher than those of tumor to blood (P < 0.001). Additionally, the parameters of inflammation to muscle in 18F-PBR06 were higher than those of tumor to muscle (P = 0.036).
4 Discussion
18F-FDG showed increased accumulation in the inflamed muscles and lung tumor tissues in this study, which was in agreement with previous reports, wherein 18F-FDG has high sensitivity but low specificity [5]. However, 18F-PBR06 exhibited high uptake during inflammation, but low uptake by the lung tumor tissues. Thus, 18F-PBR06 can be considered as a higher specificity inflammation imaging tracer compared to 18F-FDG. Furthermore, 18F-PBR06 may have potential to differentiate between lung cancer and inflammation.
18F-FDG has been used for diagnosis of inflammation and detection of infectious loci [18,19,20]. In the experimental inflammatory muscles, 18F-FDG uptake was significantly higher than uptake in general muscle tissues. However, 18F-FDG accumulated not only in the inflamed lesions, but also in a variety of tumors, including lung tumors [21, 22]. Furthermore, 18F-FDG leads to high local uptake in inflammation and recurrent tumors for evaluation of changes in lesions after radio- or chemotherapy. Therefore, the inflammatory changes and recurrent tumors could not be differentiated from inflammation by 18F-FDG PET/CT imaging [23, 24].
18F-PBR06 is a novel radioligand that can characterize inflammation by measuring TSPO receptors; thus, 18F-PBR06 PET/CT imaging can be a new tool for characterization of inflammation. Studies of some of the TSPO-specific tracers have been reported in neuroinflammatory diseases [25, 26] and inflammatory diseases of the peripheral tissues [27, 28]. In our study, we selected 18F-PBR06 for its increased binding affinity, higher signal-to-noise ratio, and low lipophilicity, and it has been used in human studies.
In the current study, we used turpentine oil-induced inflammatory models to investigate the feasibility of 18F-PBR06 PET/CT imaging in diagnosing inflammatory diseases. Thus, we selected day 7 after turpentine oil injection as the window for the macrophage infiltration in the inflammatory regions. In the acute inflammation phase, the cell population within the inflammatory regions primarily included lymphocytes and neutrophils, and the chronic inflammation phase mainly displayed monocytes and macrophages [29]. The turpentine oil would not be cleared easily, and hence, on days 3–6 post-turpentine oil injection, the inflammatory reaction would become chronic inflammation [30]. Therefore, 18F-PBR06 uptake would reach a high level on day 7, and combined with the immunofluorescent images, we demonstrated that 18F-PBR06 PET/CT imaging reflected macrophage infiltration during chronic inflammation. Therefore, the findings of the current study may indicate the feasibility of using 18F-PBR06 PET/CT imaging for assessing inflammation via macrophage infiltration.
Compared to 18F-FDG, 18F-PBR06 exhibited lower uptake in lung tumor tissues, thereby designating 18F-PBR06 as a specific tracer to characterize inflammation. In addition, 18F-PBR06 showed low uptake in lung tumor tissues (1.55 ± 0.29), but high uptake during inflammation (4.79 ± 0.48). Previous reports showed elevated TSPO levels within some specific tumors, such as ovary, breast, colon, and prostate cancer [31]. However, in this study, lung tumor tissues exhibited significantly low uptake of 18F-PBR06 (T/B = 1.77 ± 0.35, T/M = 1.45 ± 0.14) as compared to the inflamed muscles (I/B = 3.53 ± 0.26, I/M = 2.33 ± 0.64). In 18F-PBR06 Micro-PET/CT imaging, the lung tumor tissues showed lower uptake than the inflamed muscles (Fig. 4). Combined with the immunofluorescence results, the number of macrophages and the amount of TSPO in the inflammatory regions were significantly higher than the lung tumor tissues. There would also be macrophage infiltration in pulmonary inflammation nodules [32], suggesting that 18F-PBR06 PET/CT imaging may allow for diagnosis of pulmonary inflammation nodules. Therefore, 18F-PBR06 may be utilized to differentiate between peripheral lung cancer and inflammation nodules, thus enhancing accuracy in detection of pulmonary nodules.
Nevertheless, the present study had some limitations. For better comparisons of the data, this experiment could be improved by using mice bearing both inflammation and tumors in the same tissue. 18F-PBR06 showed increased accumulation in the lung that was higher than uptake in the inflamed muscles; however, a previous study reported that 18F-PBR06 showed very low uptake by the lung in the biodistribution of humans [12]. Moreover, a previous study reported that a TSPO-specific tracer might be a useful tool for evaluating lung inflammation [28]. Turpentine was used to induce inflammation in this study; however, turpentine inhalation might lead to pulmonary inflammation and empyema [33]. Therefore, pulmonary inflammation induced by turpentine inhalation might be the reason why 18F-PBR06 showed increased accumulation in the lung in our study. Taken together, further verification is essential to evaluate the usefulness of 18F-PBR06 in differentiating peripheral lung cancer and inflammation nodules.
5 Conclusion
In summary, 18F-PBR06 exhibited a significant uptake in the inflamed muscles; however, uptake in the lung tumors was low as compared to 18F-FDG. Therefore, this study confirmed that 18F-PBR06 PET/CT imaging is useful in diagnosing inflammation, and 18F-PBR06 can be considered as a superior inflammation imaging tracer of greater specificity compared to 18F-FDG. Moreover, 18F-PBR06 PET imaging may have potential in differentiating peripheral lung cancer and inflammation nodules based on its specificity, thereby enhancing the accuracy of pulmonary nodule detection.
References
C. Nathan, Points of control in inflammation. Nature 420, 846–852 (2002). https://doi.org/10.1038/nature01320
C. Love, M.B. Tomas, G.G. Tronco et al., FDG PET of infection and inflammation. Radiographics 25, 1357–1368 (2005). https://doi.org/10.1148/rg.255045122
M. Caglar, C. Yener, E. Karabulut, Value of CT, FDG PET-CT and serum tumor markers in staging recurrent colorectal cancer. Int. J. Comput. Assist. Radiol. Surg. 10, 993–1002 (2015). https://doi.org/10.1007/s11548-014-1115-8
N. Seymour, G. Burkill, M. Harries, An analysis of true- and false-positive results of vocal fold uptake in positron emission tomography-computed tomography imaging. J. Laryngol. Otol. 132, 270 (2018). https://doi.org/10.1017/S002221511700247X
I. Vlahos, K. Stefanidis, S. Sheard et al., Lung cancer screening: nodule identification and characterization. Transl. Lung Cancer Res. 7, 288–303 (2018). https://doi.org/10.21037/tlcr.2018.05.02
C. Decotiis, Y. Hu, A.K. Greenberg et al., Inflammatory cytokines and non-small cell lung cancer in a CT-scan screening cohort: background review of the literature. Cancer Biomark. 16, 219–233 (2016). https://doi.org/10.3233/CBM-150559
P. Yang, X.Y. Xu, X.J. Liu et al., The value of delayed (18)F FDG-PET imaging in diagnosis of solitary pulmonary nodules: a preliminary study on 28 patients. Quant. Imaging Med. Surg. 1, 31–34 (2011). https://doi.org/10.3978/j.issn.2223-4292.2011.11.03
L.M. Coussens, Z. Werb, Inflammation and cancer. Nature 420, 860–867 (2014). https://doi.org/10.1038/nature01322
C.J. Van Der Laken, E.H. Elzinga, M.A. Kropholler et al., Noninvasive imaging of macrophages in rheumatoid synovitis using 11C-(R)-PK11195 and positron emission tomography. Arthritis Rheumatol. 58, 3350–3355 (2008). https://doi.org/10.1002/art.23955
Y.Y. Gent, A.E. Voskuyl, R.W. Kloet et al., Macrophage positron emission tomography imaging as a biomarker for preclinical rheumatoid arthritis: findings of a prospective pilot study. Arthritis Rheumatol. 64, 62–66 (2012). https://doi.org/10.1002/art.30655
V. Papadopoulos, M. Baraldi, T.R. Guilarte et al., Translocator protein (18 kDa): new nomenclature for the peripheral-type benzodiazepine receptor based on its structure and molecular function. Trends Pharmacol. Sci. 27, 402–409 (2006). https://doi.org/10.1016/j.tips.2006.06.005
Y. Fujimura, Y. Kimura, F.G. Simeon et al., Biodistribution and radiation dosimetry in humans of a new PET ligand, (18)F-PBR06, to image translocator protein (18 kDa). J. Nucl. Med. 51, 145–149 (2010). https://doi.org/10.2967/jnumed.109.068064
S. Zhang, L. Yang, X. Ling et al., Tumor mitochondria-targeted photodynamic therapy with a translocator protein (TSPO)-specific photosensitizer. Acta Biomater. 28, 160–170 (2015). https://doi.org/10.1016/j.actbio.2015.09.033
M. Imaizumi, E. Briard, S.S. Zoghbi et al., Kinetic evaluation in nonhuman primates of two new pet ligands for peripheral benzodiazepine receptors in brain. Synapse 61, 595–605 (2010). https://doi.org/10.1002/syn.20394
F.M. Lartey, G.O. Ahn, B. Shen et al., PET imaging of stroke-induced neuroinflammation in mice using [18F]PBR06. Mol. Imaging Biol. 16, 109–117 (2014). https://doi.org/10.1007/s11307-013-0664-5
E. Briard, S.S. Zoghbi, F.G. Simeon et al., Single-step high-yield radiosynthesis and evaluation of a sensitive 18F-labeled ligand for imaging brain peripheral benzodiazepine receptors with PET. J. Med. Chem. 52, 688–699 (2009). https://doi.org/10.1021/jm8011855
M. Wang, M. Gao, K.D. Miller et al., Synthesis of [11C]PBR06 and [18F]PBR06 as agents for positron emission tomographic (PET) imaging of the translocator protein (TSPO). Steroids 76, 1331–1340 (2011). https://doi.org/10.1016/j.steroids.2011.06.012
S. Vaidyanathan, C.N. Patel, A.F. Scarsbrook et al., FDG PET/CT in infection and inflammation—current and emerging clinical applications. Clin. Radiol. 70, 787–800 (2015). https://doi.org/10.1016/j.crad.2015.03.010
A.M. Chacko, S. Watanabe, K.J. Herr et al., 18F-FDG as an inflammation biomarker for imaging dengue virus infection and treatment response. JCI Insight (2017). https://doi.org/10.1172/jci.insight.93474
M. Meyer, P. Fernandez, P. Zanotti-Fregonara, 18F-FDG imaging of chronic inflammation associated with promontofixation of the uterus. Clin. Nucl. Med. 42, 42–43 (2017). https://doi.org/10.1097/RLU.0000000000001420
S. Han, S. Woo, H.S. Chong et al., A systematic review of the prognostic value of texture analysis in 18F-FDG PET in lung cancer. Ann. Nucl. Med. (2018). https://doi.org/10.1007/s12149-018-1281-9
J. Toyohara, P.H. Elsinga, K. Ishiwata et al., Evaluation of 4′-[methyl-11C] thiothymidine in a rodent tumor and inflammation model. J. Nucl. Med. 53, 488–494 (2012). https://doi.org/10.2967/jnumed.111.098426
S. Wagner, H.J. Breyholz, C. Holtke et al., A new 18F-labelled derivative of the MMP inhibitor CGS 27023A for PET: radiosynthesis and initial small-animal PET studies. Appl. Radiat. Isot. 67, 606–610 (2009). https://doi.org/10.1016/j.apradiso.2008.12.009
O. Devinsky, A. Vezzani, S. Najjar et al., Glia and epilepsy: excitability and inflammation. Trends Neurosci. 36, 174–184 (2013). https://doi.org/10.1016/j.tins.2012.11.008
H. Boutin, C. Prenant, R. Maroy et al., [18F]DPA-714: direct comparison with [11C]PK11195 in a model of cerebral ischemia in rats. PLoS ONE 8, e56441 (2013). https://doi.org/10.1371/journal.pone.0056441
D. Harhausen, V. Sudmann, U. Khojasteh et al., Specific imaging of inflammation with the 18 kDa translocator protein ligand DPA-714 in animal models of epilepsy and stroke. PLoS ONE 8, e69529 (2013). https://doi.org/10.1371/journal.pone.0069529
O. Gaemperli, J. Shalhoub, D.R. Owen et al., Imaging intraplaque inflammation in carotid atherosclerosis with 11C-PK11195 positron emission tomography/computed tomography. Eur. Heart J. 33, 1902–1910 (2012). https://doi.org/10.1093/eurheartj/ehr367
A. Hatori, J. Yui, T. Yamasaki et al., PET imaging of lung inflammation with [18F]FEDAC, a radioligand for translocator protein (18 kDa). PLoS ONE 7, e45065 (2012). https://doi.org/10.1371/journal.pone.0045065
M.A. Ingersoll, A.M. Platt, S. Potteaux et al., Monocyte trafficking in acute and chronic inflammation. Trends Immunol. 32, 470–477 (2011). https://doi.org/10.1016/j.it.2011.05.001
J. Toyohara, M. Sakata, K. Oda, Longitudinal observation of [11C]4DST uptake in turpentine-induced inflammatory tissue. Nucl. Med. Biol. 40, 240–244 (2013). https://doi.org/10.1016/j.nucmedbio.2012.10.008
C. Wu, X. Yue, L. Lang et al., Longitudinal PET imaging of muscular inflammation using 18F-DPA-714 and 18F-Alfatide II and differentiation with tumors. Theranostics 4, 546–555 (2014). https://doi.org/10.7150/thno.8159
C.H. Xu, J.S. Xue, X.W. Zhang et al., The value of macrophage inhibitory cytokine-1 level in differentiating benign from malignant solitary pulmonary nodules. Clin. Respir. J. 12, 1473–1478 (2018). https://doi.org/10.1111/crj.12693
A.J. Khan, R.P. Akhtar, Z.S. Faruqui, Turpentine oil inhalation leading to lung necrosis and empyema in a toddler. Pediatr. Emerg. Care 22, 355–357 (2006). https://doi.org/10.1097/01.pec.0000215371.48859.fd
Author information
Authors and Affiliations
Corresponding authors
Additional information
This work was funded in part by the National Natural Science Foundation of China (Nos. 11875114, 81471706, and 81871407), Science and Technology Commission of Shanghai Municipality (No. 16410722700), and sponsored by the Shanghai Sailing Program (No. 17YF1417400).
Rights and permissions
About this article

Cite this article
Zhang, H., Tan, H., Mao, WJ. et al. 18F-PBR06 PET/CT imaging of inflammation and differentiation of lung cancer in mice. NUCL SCI TECH 30, 83 (2019). https://doi.org/10.1007/s41365-019-0597-z
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s41365-019-0597-z