
Abstract
Several early social communication skills are theorized to be important for later more complex social behaviors. These skills, such as joint attention, social referencing, and social engagement, emerge very early in young children who are typically developing. For children with autism spectrum disorder (ASD) and other developmental delays, these skills may not emerge naturally and may need specialized interventions. Luckily, early social communication skills are a growing area of research and there is a developing library of potentially effective practices for intervention on these skills. Across these studies, however, there is considerable variability in the terminology, topographies, and categorizations of these skills that can lead to under or over identification of evidence-based practices to address these skills. This systematic review of the literature presents 29 single-case and group design studies that target an early social communication skill and highlight the range of definitions of these pivotal skills. Results suggest that there are overlapping definitions of these early social communication skills that may leave specific skills unaddressed. Ideas for more cohesive definitions and assessment are offered as well as opportunities for future research.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Young children who are typically developing rapidly achieve a series of sequential and predictable milestones in the first years of life (Bricker et al. 1999; Hoff 2006). By the age of 3, typically developing children have developed language, motor, and adaptive skills that allow access to new environments and reinforcers (e.g., learn to walk, communicate). Research has also shown that failure to reach some of these early milestones at the appropriate time might indicate a pervasive delay or disorder (Landa et al. 2013). For example, a lack of spoken language early on can be an indicator of autism spectrum disorders and other potential delays. Further, there is research to suggest that interruption to early interactions with the environment may significantly impede development (Bagner and Graziano 2013). Early and reciprocal interactions with caregivers seem to be critical for early growth and development (Shire et al. 2016; Sitnick et al. 2015). For this reason, recent research has focused on early identification of missed milestones. Developmental screeners (e.g., Ages and Stages Questionnaire, Modified Checklist for Autism in Toddlers; Bricker et al. 1999; Robins et al. 2014) have been developed to identify young children who might benefit from further assessment that may then lead to intervention if necessary. Additional research has shown that early intervention has great potential to mitigate these early differences (e.g., Makrygianni and Reed 2010).
Among these early developmental milestones are early social communication skills (ESCS). These early social skills, like eye gaze (i.e., following social stimuli with eye contact, coordinated eye gaze shifting), joint attention (i.e., shared attention on an object or event between two individuals), social referencing (i.e., seeking social information from another individual following a surprising event), and social orienting (e.g., engagement with social stimuli in an environment), are typically developed in the first 2 years of life in the context of everyday interactions (DeQuinzio et al. 2016; Dube et al. 2004). Development of these early gestures is likely directly linked with typical development of more advanced verbal behavior (Bottema-Beutel et al. 2014; Gulsrud et al. 2014; Mundy et al. 2003; Warreyn et al. 2014). For the most part, children who are typically developing learn these skills without targeted intervention. For example, very young children will imitate the facial expressions of their caregiver (i.e., 2 months; Meltzoff and Moore 1992) and naturally orient toward social stimuli in the room (e.g., their parents voice; Dawson et al. 1998; Greene et al. 2011) and children as young as 6 months engage in early joint attention, by starting to follow their parent’s point or eye gaze (Mundy et al. 2007; Mundy and Sigman 2006). In late infancy, children can typically respond to joint attention bids, initiate joint attention, orient toward social stimuli, coordinate the attention of someone else, point to get attention, and use basic gestures and early speech to get access to reinforcers (Toth et al. 2006).
Although developmental research has indicated the typical sequence and timeline for these pivotal skills, there is little available information on how the development of these early skills is interrelated. Some evidence indicates that early gaze shifting predicts later coordinated joint attention, or that orientation to social stimuli effects later social skill development (Frischen et al. 2007; Presmanes et al. 2007). Deficits in social orienting early on correlate with deficits in joint attention, which in turn may be related to deficits in using information from a social exchange (i.e., social referencing; DeQuinzio et al. 2016). In addition, early imitation skills may be predictive of later joint attention, among other skills (Whalen and Schreibman 2003). Although individual skills may be viewed as predictors of future skill acquisition, further investigation is needed to determine more precisely the interaction between these early social communication skills. Additionally, these individual skills may be defined in a manner that is more precise, allowing for an enhanced analysis.
Children with autism spectrum disorder (ASD) typically do not develop early social communication skills in sequence with their same-aged peers (Mundy et al. 1986, 1990). Diagnostic criteria for ASD include deficits in social communication and the presence of restrictive and repetitive interests and behaviors (RRBIs; American Psychiatric Association 2013). Retrospective video analyses from first birthdays of young children who go on to receive an ASD diagnosis, for example, indicate differences from same-aged peers in terms of joint attention and social interest (Landa et al. 2007; Osterling and Dawson 1994). Deficits in early social communication and early RRBIs are some of the first behavior indicators of an ASD to emerge (Zwaigenbaum et al. 2005).
Despite the apparent foundational nature of early social communication skills, there is little information on the degree to which there is a causal relationship between the development of early social communication skills and later social and communication functioning. Mundy et al. completed a longitudinal study to examine language outcomes for two groups of young preschoolers, those with intact joint attention and those with joint attention deficits. Data suggest that children who had intact joint attention at the start of preschool achieved more during preschool including cognitive, social, and behavioral gains (Ingersoll and Schreibman 2006; Kasari et al. 2014; Whalen and Schreibman 2003). Several studies have looked at collateral effects of joint attention intervention on social communication skills and found there to be some substantial increases in more advanced social skills (e.g., play, conversation) following an intensive joint attention intervention (e.g., Kasari et al. 2008; Whalen and Schreibman 2003). Despite the theoretically pivotal nature of these skills, children with ASD may not develop early social communication skills without specific intervention, and in contrast with later developing social communication skills, these early skills are under researched (White et al. 2011).
Fortunately, there is a growing library of available interventions on early social communication skills. Joint attention, in particular, has been the subject of several recent literature reviews indicating useful teaching procedures for the development of response to joint attention and initiation of joint attention (Murza et al. 2016; Warreyn et al. 2014). In one recent review, authors found 25 studies with direct intervention on joint attention, with more studies focusing on teaching young children with ASD to initiate joint attention, and most studies being completed by an interventionist (White et al. 2011). In addition to these studies, several authors have completed successful randomized control trials to examine the effect of a packaged intervention on an array of social communication skills. For example, Joint Attention Social Play Emotional Regulation (JASPER) uses naturalistic teaching strategies to promote gains in joint attention and social play as well as reduction in RRBIs, and has shown to be effective in multiple RCTs across contexts (Chang et al. 2016; Lawton and Kasari 2012).
Despite the growing evidence for effective intervention, across the research on supporting early social communication skills, these early skills are defined differently, making it difficult to subdivide the literature and establish the most effective teaching procedures. Further, authors often aggregate early skills into omnibus terms like “social engagement,” and provide evidence that their intervention increases the aggregate of several early social communication skills, making it difficult to partition out effective teaching procedures for individual skills (e.g., Koegel et al. 2012; DiSalvo and Oswald 2002). Interventions on social functioning in general also preclude further analysis of the potential pivotal nature of these early skills. For example, it is difficult to say if teaching joint attention increases a specific play skill if all play skills (e.g., sharing, commenting) are simultaneously targeted. This analysis of the current literature on early social communication skills aims to (a) increase the precision of the definition and delineation of early social communication skills in children with autism, (b) identify effective interventions and the degree to which they target specific early social communication skills, and (c) provide next steps for research and intervention on these early skills.
Method
Search Procedures
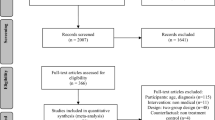
Systematic searches were completed by the first author and a trained graduate research assistant in three academic databases: Education Resource Information Center (ERIC), Academic Search Complete, and PsychNET. In all three databases, search terms were entered as follows: “joint attention or joint engagement or eye gaze or social interaction or social referencing or shared affect or social orienting or social gestures or behavioral regulation or synchronous engagement” and “autis* or ASD or PDD*” and “intervention or instruction or teach* or treat* or train*.” To capture changes in definitions of the dependent variables over time, year parameters were not applied to the searches. Searches returned 1728 abstracts.
From the returned abstracts, duplicates were removed, as were literature reviews, concept papers, and descriptive studies. The abstracts of the 38 remaining returned studies were examined to determine initial inclusion for further analysis. Nine studies were removed due to missing criteria (e.g., demographic variable was not an early social communication skill). The article was included for further analysis if the study appeared to report the results of an experimental analysis using single-case or group design methodology and target appropriate dependent variables (i.e., early social communication skills). Group designs were further examined to determine measurement method or tool and presence of individual early social communication skills on those scales. Following abstract screening, the full text of the remaining studies was reviewed for inclusion. Lastly, ancestral searches were completed on the studies in this review from 2015, and historical searches were completed on the three most commonly represented authors and journals for the years represented in the review (2001–2016). Four articles were added from historical searches.
Inclusion and Exclusion Criteria
Inclusion Criteria
In order to be included in this review, a study must have met the following requirements: (a) publication in an English language peer-reviewed journal; (b) use of a single-case research design (e.g., multiple-baseline, multiple probe, alternating treatment) or experimental group design (e.g., randomized control trial, waitlist control trial); (c) all participants needed to have or be at documented risk for ASD. Inclusion of an ASD diagnosis/educational classification was based on the diagnostic criterion outlined in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV-TR), which included children with a diagnosis of pervasive developmental disorder-not otherwise specified (PDD-NOS), and autistic disorder, or the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V), which included children who were noted as receiving services under the autism educational category, or had documented autism risk (e.g., sibling with ASD, early ASD markers) as reported by the researchers; and (d) all participants were between the ages of 12 and 83 months (i.e., ages 1–6). This age range was selected to capture assessment and intervention of the earliest social communication skills. Although a significant portion of research on early and pivotal social communication skills for children with ASD is on significantly older children, this review aimed to synthesize the available literature on early intervention on these skills and so excluded studies with older participants that may have altered their definitions to reflect appropriate skills for older children.
Exclusion Criteria
Studies were excluded if any participant was outside the age range outlined previously, or the intent of the study was not to intervene on a specific early and pivotal social communication skill. Studies that included an appropriate dependent variable but featured participants outside of the age range were not included in this analysis. Several studies looked at more general early social skills (e.g., “social engagement”), and these studies were excluded from the review (e.g., Hartzell et al. 2015). Studies were additionally excluded if they did not describe an intervention, or the intervention did not report child data (e.g., parent training; Radley et al. 2014). Twenty-nine studies sufficiently met inclusion criteria.
Search Procedure Inter-observer Agreement
Searches were completed again by a second trained research assistant. Inter-observer agreement was calculated by dividing the number of agreements by the sum of agreements and disagreements and multiplying by 100%. Inter-observer agreement (IOA) for searches was 90% (i.e., the initial articles saved for abstract review). Inclusion and exclusion decisions were calculated in the same way by the first and second authors. IOA for inclusion and exclusion was 86%.
Data Extraction
Data were extracted by the first and third author and were reported on the following variables for each of the 23 single-case studies: (a) methodology (type of single-case design), (b) participant characteristics (number, age, gender, diagnosis), (c) intervention type, (d) dependent variable (operational definition and quality of operational definition), and (d) results (outcome measure, success estimate, and non-overlap index (Tau-U)). For the 13 group designs, data were extracted on type of design, participant characteristics, intervention type, dependent variable, and results including effect size as reported by authors. Thirty percent of the final tables were recorded by a trained research assistant. IOA between the two observers calculated using a point-by-point method (i.e., number of agreements minus number of disagreements divided by total observations and multiplied by 100) was 100%.
Dependent Variable Quality
The quality of the operational definition was rated on a 16-point scale adapted from Reichow’s criteria for the use of high-quality research standards (Reichow et al. 2008), and the standards put forth for quality single-case research by Gast and Ledford (2009). Operational definitions of the dependent variable were rated on a 4-point scale across four factors: (a) variables are defined with replicable precision, (b) the details necessary to replicate the measures are provided, (c) the measures are linked to dependent variables, and (d) the measurement is conducted at appropriate times during the study for the given analysis and dependent variables are linked to a priori research questions. For the group designs, articles were rated based on author report of dependent variable or quality of definition of early social communication skill present in a standardized measure used in the group design data collection protocol. Studies were scored on a scale of 0–16, with a score of 14 or higher considered high quality, 12–14 moderate quality, and 12 or lower poor quality. Initial ratings were conducted by the first author. Inter-observer agreement for dependent variable ratings was collected by the second author and scored using a point-by-point method on a randomly selected 30% of included studies. IOA for dependent variable ratings was 90%. The data collection measure used is available from the first author upon request.
Visual Analysis and Non-overlap Index
Visual analysis of graphed data was conducted by the first and third authors. The strength of functional relation demonstrated by graphed data was rated using standards for the visual analysis of single-case design (i.e., change in level and/or trend in the intended direction, the level of variability, vertical analysis). Tau-U was calculated using the online calculator available at singlecaseresearch.org. Data were entered from digitized screen shots of included studies. Digitization (i.e., disaggregation of graphed data) was completed using Unscanit (https://www.silkscientific.com/graph-digitizer.htm). Digitized data were entered into the Tau-U online calculator (Vannest and Ninci 2015) and the available mechanism for the partial correction of autocorrelation was selected, where appropriate (i.e., if noticeable trend was present in baseline). Tau-U is a non-overlap index that measures change in data from baseline levels by comparing baseline data points to intervention (Vannest and Ninci 2015). For reliability, 33% of included studies were re-calculated by a graduate research assistant. IOA for Tau-U calculations was 100%. Tau-U is reported in terms of non-overlapping data, meaning a study with zero overlapping data would have a Tau-U score of 1.0. Guidelines for interpretation of Tau-U indicate a score of 0.65 or lower as weak, 0.66–0.92 as medium to high, and 0.93 or higher as large (Parker et al. 2011; Rakap 2015).
Effect Size of Included Group Design Studies
Data were extracted on effect size of group design studies as reported by the authors of these studies. Effect size estimates reported by the authors (i.e., Cohen’s d, d-estimates) are reported in Table 3. Group designs are synthesized separately from single-case data as the selected non-over-lap estimate (Tau-U) does not meet parametric assumptions necessary to compare it to a group design effect size estimator (Parker et al. 2011).
Results
Search procedures yielded 23 single-case studies and 13 group design studies. Table 1 reports the single-case results and Table 2 reports the group design results. Tables 1 and 2 report participants, dependent variable, intervention, and estimated effect.
Single-Case Results
Twenty-three single-case studies were returned from the systematic searches.
Participants and Settings
Across the 23 included studies, there were 79 total participants within the age range of 0 to 6 years. Of these participants, 16 were infants (i.e., 0–2), nine were toddlers (i.e., 2–3), and 54 were of preschool age (i.e., 3–6). Of the included participants, four were considered at risk for ASD, and 75 had an ASD diagnosis. ASD diagnosis or risk was reported using a range of developmental screeners and autism-specific assessment (i.e., Childhood Autism Scales [CARS]). A majority of the interventions were implemented by interventionists (i.e., clinicians or therapists or researchers) (47%), followed by family members (43%) and teachers (9%). Most studies (39%) occurred in clinical or laboratory settings followed by classrooms (21%) and home (39%).
Interventions
Single-case studies included in this review used a variety of interventions to improve early social communication skills for young children with ASD, either through direct intervention on the skill or a packaged intervention model (e.g., Early Start Denver Model). Interventions are reported using the descriptors included by the authors of the included studies. Fourteen studies used some form of naturalistic teaching paradigm (i.e., Benson and Joosten 2014; Ferraioli and Harris 2011; Gena et al. 2016; Ingersoll and Schreibman 2006; Jones 2009; Jones et al. 2006; Jones and Feeley 2009; Rocha et al. 2007; Vernon et al. 2012; Vismara and Lyons 2007; Vismara et al. 2013; Whalen and Schreibman 2003; Zercher et al. 2001). Other strategies included packaged interventions (e.g., Early Start Denver Model), behavioral teaching strategies, developmental teaching strategies, and natural change agent training.
Intervention Effects
Single-subject studies were primarily evaluated using standards for visual analysis (Gast and Ledford 2009; Kratochwill et al. 2010). Of the 23 included single-case studies, 12 demonstrated a strong effect (an immediate change in level or trend, low variability, and low rates of overlapping data), nine demonstrated a mixed effect (some tiers demonstrate change in level or trend, but may include some overlapping data or some tiers demonstrating no effect), and two did not demonstrate a functional relation (insufficient demonstration of changes in level or trend and/or high rates of overlapping data). Results of visual analysis are listed in Table 1. Visual analysis for these studies was supplemented, where appropriate, with Tau-U (i.e., for studies with sufficient data points and not designs unsuitable for this analysis such as changing criterion or alternating treatment without baseline). Tau-U for the included studies ranged from 0.1 to 1.0, with a weighted average across studies of 0.65, indicating an overall moderate effect of the reviewed interventions. Unweighted Tau-U was calculated throughout because no studies demonstrated concerns requiring weighted Tau-U (e.g., trend in baseline).
Group Design Studies
Participants and Settings
The included group design studies included 535 participants within the age range of 2- to 7-year-old participants. Across these participants, ages ranged within studies from 18 to 30 months. Most of the included group design studies did not report individual child age. Across the 11 studies, five took place in a clinical setting, four in an educational setting, and two in a natural setting (e.g., home).
Intervention Outcomes
Of the 11 studies included in this review, six reported an effect size. Of the reported effect sizes, three showed a strong effect (i.e., a d or d-estimator of 0.7 or higher), two showed a medium effect (0.5–0.7), and one showed a small or nominal effect (0.3 or below). About half (5) of the included group design studies did not report an effect size estimate.
Dependent Variable Measurement
Across the included group design studies, most studies used either a standardized measure, a measure specific to their intervention, or a behavioral measure of their target behavior. Of the studies that used a standardized assessment, most used the Early Social Communication Scales (ESCS). Other assessments included Preschool Language Scales (PLS), Autism Diagnostic Observation Scale-Generic (ADOS-G), and Motor Imitation Scales (MIS).
Dependent Variables
Based on developmental assessments, component analyses of early social communication interventions, and an iterative search process, the first author developed a list of dependent variables of interest. The following topics were dependent variables in at least one study included in this review, and occurred with varying frequency across studies and with varying definitions within terms. The quality of the resulting dependent variables for the single-case studies is listed in Table 3.
Joint Attention
Joint attention can be defined as the reciprocal attention between two individuals on an object or event. Eighty-three percent of included studies featured joint attention as at least one of the dependent variables assessed. Most studies used definitions of joint attention that followed the definition used in the Early Social Communication Scales, which does not include coordinated gaze shifting (e.g., Isaksen and Holth 2009; Jones and Feeley 2009; Yoder and Stone 2006).
Shared Attention/Social Orienting
Shared attention and social orienting are components of joint attention. Shared attention is the ability to share focus on something with someone else, but does not require the triadic focus of joint attention. Social orienting is used by some researchers to define this same precursor behavior. Four studies (13% of included studies) focused mainly on shared attention so or social orienting (e.g., Tsao and Odom 2006; Wong and Kwan 2010).
Social Referencing
Social referencing has the same features as joint attention but is the use of parents affect as information given a surprising or alarming event. One study focused on social referencing (i.e., Brim et al. 2009).
Synchronous Engagement/Joint Engagement
Synchronous or joint engagement is reciprocal interactions between caregiver and child (i.e., shared turn taking, imitation). Thirty percent of included studies evaluated a joint engagement or synchronous engagement variable (e.g., Vernon et al. 2012; Ingersoll et al. 2012).
Discussion
Early social communication skills are often missing or impaired in children with ASD. Results of the reviewed studies indicate there are a variety of definitions of early social communication skills and a growing variety of interventions to support them for young children with or at risk for ASD. The results of this review also indicate a range of effectiveness (i.e., M = 0.65; range 0.10–1.0) of interventions and a range in the quality of the definition of the dependent variables targeted in these studies (i.e., M = 12.5; range 9–16). Further, results of this review indicated a steadily increasing body of literature on early social communication skills and a range of contexts and agents for these early skills. For example, included studies ranged from more developmental naturalistic studies (e.g., teaching joint engagement in the home with parents; Ingersoll et al. 2012) to clinic-based targeted intervention on very specific topographical responses (e.g., Brim et al. 2009). Further, over the years included in this review (i.e., 2001–2016), there was a trend in increased focus on certain areas of study (i.e., joint attention initiations, joint engagement). Finally, results indicate that for dependent variables with multiple studies, the definition of the target behavior often varied considerably between the reviewed studies.
One potential problem with this body of literature identified by this review is this variety of definitions of dependent variables. Without consistently defined terms across studies, it is difficult to determine the best practices for ESCS interventions. For example, the reviewed papers indicated varying different definitions of joint attention with about half of the studies targeting joint attention requiring the child to also gaze shift to the social partner, and half not requiring that behavior. According to the National Professional Development Center on ASD and What Works Clearinghouse, joint attention intervention is considered an evidence-based practice. However, the research base that establishes best practices uses varying definitions of joint attention and broadly defined teaching procedures. Without adequately defined topography of ESCS, the most efficacious teaching procedures are difficult to determine. Another finding of interest from this review was the seemingly inverse relationship between the effects of the interventions and the specificity and quality of the definition of the dependent variable. Results of this analysis seem to indicate that the studies with broad definitions of the dependent variable had larger effects. For example, a study had a Tau-U of 1.0 and visual analysis indicated a strong functional relation, but the dependent variable received a low rating due to lack of specificity (e.g., Vernon et al. 2012). Conversely, some studies had a weak effect but received a relatively high rating as far as precision of the dependent variable (e.g., Ferraioli and Harris 2011). This finding could be the result of broader intervention targets that require less precise or lower-dose intervention. Important and potentially pivotal skills could be missed in interventions that aim only to increase social functioning in a broad sense.
Overlapping and imprecise definitions of these early terms also increase the difficulty of rating the appropriateness and timing of certain skill deficits for intervention. Although there is some literature to suggest that these early skills are pivotal (e.g., quality of joint attention skill predicts the quality of social and academic outcomes; e.g., Sullivan et al. 2015), the mechanisms underlying the emergence of ESCS are unclear. Further, children with ASD can develop intact vocal speech, basic conversation skills, and typical age vocabularies without acquiring ESCS milestones (e.g., joint attention; Moore and Dunham 2014), which necessitates further research on the pivotal nature of these skills. Much of the research on the longitudinal benefits of intact early social communication skills tracks children who acquire these skills in the context of typical development. Most definitions of joint attention (i.e., in the ESCS; Mundy et al. 2003) are formed on norms for very young children, but the larger effect of training those skills, later on, is unknown. Some research has been conducted to examine the collateral effects of joint attention intervention for children with ASD but in the context of a more global social communication intervention (e.g., Whalen and Schreibman 2003). However, research should also extend across early social communication skills to examine potential generalization of related skills and the collateral effects of targeted intervention for generalized social functioning.
To determine the presence of prerequisite skills and better inform intervention, appropriate assessment of ESCS is required. There are few assessments appropriate for the range of ESCS, potentially due to the variability of important early social communication skills and the differing definitions of these skills. In this review, a majority (86% of included studies) used the Early Social Communication Scales. The Early Social Communication Scales covers a wide array of social communication skills and has some data to support its suggested norms (Mundy et al. 2003); however, there are a few potential limitations if used as the sole tool in research and practice on ESCS. First, as evidenced by this review, this tool is most often used for children who are preschool-aged. The majority of included studies focused on children at the later end of the included age range (0–5 years). The Early Social Communication Scales was written to mimic developmental norms for very young children (up to 36 months) and not the interactions of children that have already entered preschool. Tools are needed that can reflect the development of these skills through early childhood and further, to insure that socially valid social skills are being trained in preschool-aged children. Without that measure, it is difficult to ascertain appropriate intervention targets for preschoolers and beyond. Additionally, the Early Social Communication Scales is designed to be completed by a trained tester and is time-intensive and ill-suited to be conducted in natural environments and with the input of those who might have had the most opportunity to observe the child. There have been some advancements in the development of parent-report screeners for joint attention (e.g., the Pictorial Infant Communication Scale; Ghilain et al. 2017) but these are specific to joint attention and may not target all ESCS.
Given developing ESCS are in fact pivotal skills, more information is needed as to how best to increase ESCS that will transfer to later more advanced social communication. Information about the generality of these early skills is of potential benefit to the formation of interventions that may increase more global social communication functioning. Comparative research is needed to look at the benefit of intervention on one potentially pivotal skill versus a global intervention on a set of early skills. Further, the timing of intervention may also be of interest and may help to determine what type of intervention is most effective and at what specific times. Research indicates that earlier intensive intervention yields better outcomes, but whether intensive intervention on ESCS for older children is effective is largely unknown. Many social communication interventions are packages that target both potentially pivotal skills (e.g., joint attention) and more age appropriate skills (e.g., symbolic play or classroom engagement). Contextualizing the early skill in terms of age appropriate social skills is logical, but more work is needed to assess whether this is more parsimonious than intensely targeting the missing prerequisite skill and supplementing with the global intervention. Component analyses of packaged interventions, as well as comparison studies, are needed to parse dosage and timing of intervention on ESCS.
Evaluating the exact relationship between these early variables is also needed. Although we understand these skills should develop early on and may be pivotal for the development of other related social communication skills, the relationships between these variables are still largely unclear. Developmental trajectories from research on children who are typically developing indicate sequence of early developing skills, but not to what extent these skills depend on each other. For example, data indicates that perhaps social orienting and/or social engagement emerges before response to joint attention and that response to joint attention and initiation of joint attention both emerge before social referencing (DeQuinzio et al. 2016). Developmental theory suggests that joint attention (i.e., shared attention of a parent and child on an object or event) is a prerequisite for social referencing (i.e., child referencing of adult emotional response given a surprising event; DeQuinzio et al. 2016). Subsequent research, however, has indicated that social referencing has been shown to increase response to joint attention behaviors in young children with ASD (e.g., if parent shows a more exaggerated reaction to stimuli, such as surprise or fear, the child is more likely to respond to their joint attention bid; Leavens et al. 2014). Understanding which ESCS might be prerequisites for other pivotal skills and the typical scope and sequence of these skills might increase the efficacy of interventions on ESCS. Further information about the interactions between ESCS would inform assessment and intervention on these skills.
In addition to barriers to assessment and definition of ESCS, recommendations to interventionists in support of ESCS are also hindered by a lack of research in a natural context. Across all these early-targeted skills, a majority of this research has been conducted in clinical settings. Failure to program for generalization during these interventions may limit the ability of this research to inform practice that will change child behavior across settings or stimuli. For example, use of a clinic room with novel stimuli and an interventionist may not transfer to the park with the child’s parent, or to a peer in the block area of a preschool classroom. Future research should include research in generalized settings and program environmental reinforcers to increase child engagement and acquisition of child skill. One potential advantage of those interventions with lower-quality definitions of dependent variables is that they may allow for training of ESCS that are more appropriate for the natural environment (Shreibman et al. 2015). For example, joint attention in the natural environment is controlled by naturally occurring discriminative stimuli and reinforcers and is unlikely to be as easily identified as in a clinical setting. Developmental norms for children who acquire ESCS later on, as well as best practices for targeting specific social communication skills in a natural context, are needed for more ecologically valid interventions.
Interventions on ESCS are also needed that use natural change agents who interact with the child most frequently given their age. Results of this review indicated a minority (33% of studies) were completed by natural change agents. Parents, peers, teachers, and other valid individuals should be interventionists on these skills. For children who are typically developing, many of these skills develop in context of parent-child interactions and are maintained by social reinforcers. For example, joint attention involves the child looking at what the parent has pointed out and back to the parent. Reinforcement for the child becomes available from the parent’s comment about the object, parent information about the object or event, and parent social praise (e.g., the parent might say “you see that blue bird!” Birds say, “cheep!”). For children with ASD, social reinforcement may not be as motivating (Rodriguez and Gutierrez 2017). Over time, this creates a learning history for parents as well, and joint attention bids to the child that are not reinforced get extinguished. Because of this lack of preference for social interaction, and history of extinction of parent bids for joint attention, there may be a need for researchers to contrive the motivating operation or pair social praise with primary reinforcers (Dube et al. 2004). Augmenting joint attention intervention with less naturalistic reinforcers is not contraindicated by the current research and, in many instances, leads to clinically and experimentally relevant gains, but fading the reinforcer may be difficult. By involving natural change agents in early intervention on social communication, reinforcement can be provided for making bids for early social communication skills and opportunities to respond can be increased for the child with ASD.
Limitations
There were limitations to this systematic review and analysis. Primarily, autism severity is related to the development of early social communication skills. Very young children with or at risk for ASD might respond differently to intervention on these early skills depending on the severity of ASD. The studies included in this review included participants over a range of ages and autism severity, and the heterogeneity of these participants may limit the generalizability of these results. Secondly, studies differed in how they defined or determined ASD diagnoses and severity. Further, this study focused on very young children in order to capture interventions on early social communication during the appropriate developmental period. However, children and even young adults with ASD may demonstrate skill deficits in ECSE. This review is unable to speak to the utility of interventions for these older children.
References
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: American Psychiatric Association.
Bagner, D. M., & Graziano, P. A. (2013). Barriers to success in parent training for young children with developmental delay: the role of cumulative risk. Behavior Modification, 37(3), 356–377.
Benson, R. L., & Joosten, A. V. (2014). Does video training increase adult and child joint attention and improve child outcomes? Two individual case studies in children with autism spectrum disorder. Journal of Intellectual and Developmental Disability, 39(4), 301–314.
Bottema-Beutel, K., Yoder, P. J., Hochman, J. M., & Watson, L. R. (2014). The role of supported joint engagement and parent utterances in language and social communication development in children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 44(9), 2162–2174.
Bricker, D. D., Squires, J., & Mounts, L. (1999). Ages & stages questionnaires: a parent-completed, child-monitoring system. Baltimore, MD: Paul H. Brookes.
Brim, D., Townsend, D. B., DeQuinzio, J. A., & Poulson, C. L. (2009). Analysis of social referencing skills among children with autism. Research in Autism Spectrum Disorders, 3(4), 942–958.
Casenhiser, D. M., Shanker, S. G., & Stieben, J. (2013). Learning through interaction in children with autism: preliminary data from asocial-communication-based intervention. Autism, 17(2), 220–241.
Chang, Y. C., Shire, S. Y., Shih, W., Gelfand, C., & Kasari, C. (2016). Preschool deployment of evidence-based social communication intervention: JASPER in the classroom. Journal of Autism and Developmental Disorders, 46(6), 2211–2223.
Dawson, G., Meltzoff, A. N., Osterling, J., Rinaldi, J., & Brown, E. (1998). Children with autism fail to orient to naturally occurring social stimuli. Journal of Autism and Developmental Disorders, 28(6), 479–485.
DeQuinzio, J. A., Poulson, C. L., Townsend, D. B., & Taylor, B. A. (2016). Social referencing and children with autism. The Behavior Analyst, 39(2), 319–331.
DiSalvo, C. A., & Oswald, D. P. (2002). Peer-mediated interventions to increase the social interaction of children with autism: consideration of peer expectancies. Focus on Autism and Other Developmental Disabilities, 17(4), 198–207.
Dube, W. V., MacDonald, R. P., Mansfield, R. C., Holcomb, W. L., & Ahearn, W. H. (2004). Toward a behavioral analysis of joint attention. The Behavior Analyst, 27(2), 197–207.
Ferraioli, S. J., & Harris, S. L. (2011). Teaching joint attention to children with autism through a sibling-mediated behavioral intervention. Behavioral Interventions, 26(4), 261–281.
Frischen, A., Bayliss, A. P., & Tipper, S. P. (2007). Gaze cueing of attention: visual attention, social cognition, and individual differences. Psychological bulletin, 133(4), 694.
Gast, D. L., & Ledford, J. R. (Eds.). (2009). Single subject research methodology in behavioral sciences. New York, NY: Routledge.
Gena, A., Galanis, P., Tsirempolou, E., Michalopoulou, E., & Sarafidou, K. (2016). Parent training for families with a child with ASD: a naturalistic systemic behavior analytic model. The European Journal of Counselling Psychology, 4(1), 4.
Ghilain, C. S., Parlade, M. V., McBee, M. T., Coman, D. C., Owen, T., Gutierrez, A., … & Alessandri, M. (2017). Validation of the Pictorial Infant Communication Scale for preschool-aged children with autism spectrum disorder. Autism, 21(2), 203–216.
Greene, D. J., Colich, N., Iacoboni, M., Zaidel, E., Bookheimer, S. Y., & Dapretto, M. (2011). Atypical neural networks for social orienting in autism spectrum disorders. NeuroImage, 56(1), 354–362.
Gulsrud, A. C., Hellemann, G. S., Freeman, S. F., & Kasari, C. (2014). Two to ten years: developmental trajectories of joint attention in children with ASD who received targeted social communication interventions. Autism Research, 7(2), 207–215.
Hartzell, R., Liaupsin, C., Gann, C., & Clem, S. (2015). Increasing social engagement in an inclusive environment. Education and Training in Autism and Developmental Disabilities, 50(3), 264.
Hoff, E. (2006). How social contexts support and shape language development. Developmental Review, 26(1), 55–88.
Ingersoll, B., & Schreibman, L. (2006). Teaching reciprocal imitation skills to young children with autism using a naturalistic behavioral approach: effects on language, pretend play, and joint attention. Journal of Autism and Developmental Disabilities, 36(4), 489–505.
Ingersoll, B., Meyer, K., Bonter, N., & Jelinek, S. (2012). A comparison of developmental social–pragmatic and naturalistic behavioral interventions on language use and social engagement in children with autism. Journal of Speech, Language, and Hearing Research, 55(5), 1301–1313.
Isaksen, J., & Holth, P. (2009). An operant approach to teaching joint attention skills to children with autism. Behavioral Interventions, 24(4), 215–236.
Jones, E. A. (2009). Establishing response and stimulus classes for initiating joint attention in children with autism. Research in Autism Spectrum Disorders, 3(2), 375–389.
Jones, E. A., & Feeley, K. M. (2009). Parent implemented joint attention intervention for preschoolers with autism. The Journal of Speech and Language Pathology – Applied Behavior Analysis, 4(1), 74–89.
Jones, E. A., Carr, E. G., & Feeley, K. M. (2006). Multiple effects of joint attention intervention for children with autism. Behavior Modification, 30(6), 782–834.
Kaale, A., Smith, L., & Sponheim, E. (2012). A randomized controlled trial of preschool-based joint attention intervention for children with autism. Journal of Child Psychology and Psychiatry, 53(1), 97–105.
Kasari, C., Freeman, S., & Paparella, T. (2006). Joint attention and symbolic play in young children with autism: a randomized controlled intervention study. Journal of Child Psychology and Psychiatry, 47(6), 611–620.
Kasari, C., Paparella, T., Freeman, S., & Jahromi, L. B. (2008). Language outcome in autism: randomized comparison of joint attention and play interventions. Journal of Consulting and Clinical Psychology, 76(1), 125.
Kasari, C., Shire, S., Factor, R., & McCracken, C. (2014). Psychosocial treatments for individuals with autism spectrum disorder across the lifespan: new developments and underlying mechanisms. Current Psychiatry Reports, 16(11), 512.
Koegel, L. K., Vernon, T. W., Koegel, R. L., Koegel, B. L., & Paullin, A. W. (2012). Improving social engagement and initiations between children with autism spectrum disorder and their peers in inclusive settings. Journal of Positive Behavior Interventions, 14(4), 220–227.
Kratochwill, T. R., Hitchcock, J., Horner, R. H., Levin, J. R., Odom, S. L., Rindskopf, D. M., & Shadish, W. R. (2010). U.S. Department of Education, Institute of Education Sciences, National Center for Education Evaluation and Regional Assistance, What Works Clearinghouse.
Krstovska-Guerrero, I., & Jones, E. A. (2013). Joint attention in autism: teaching smiling coordinated with gaze to respond to joint attention bids. Research in Autism Spectrum Disorders, 7(1), 93–108.
Landa, R. J., Holman, K. C., & Garrett-Mayer, E. (2007). Social and communication development in toddlers with early and later diagnosis of autism spectrum disorders. Archives of General Psychiatry, 64(7), 853–864.
Landa, R. J., Holman, K. C., O’Neill, A. H., & Stuart, E. A. (2011). Intervention targeting development of socially synchronous engagement in toddlers with autism spectrum disorder: a randomized controlled trial. Journal of Child Psychology and Psychiatry, 52(1), 13–21.
Landa, R. J., Gross, A. L., Stuart, E. A., & Faherty, A. (2013). Developmental trajectories in children with and without autism spectrum disorders: the first 3 years. Child Development, 84(2), 429–442.
Lawton, K., & Kasari, C. (2012). Teacher-implemented joint attention intervention: pilot randomized controlled study for preschoolers with autism. Journal of Consulting and Clinical Psychology, 80(4), 687.
Leavens, D. A., Sansone, J., Burfield, A., Lightfoot, S., O’Hara, S., & Todd, B. K. (2014). Putting the “Joy” in joint attention: Affective-gestural synchrony by parents who point for their babies. Frontiers in Psychology, 5, 879.
Leew, S. V., Stein, N. G., & Gibbard, W. B. (2010). Weighted vests’ effect on social attention for toddlers with autism spectrum disorders. Canadian Journal of Occupational Therapy, 77(2), 113–124.
Makrygianni, M. K., & Reed, P. (2010). A meta-analytic review of the effectiveness of behavioural early intervention programs for children with autistic spectrum disorders. Research in Autism Spectrum Disorders, 4(4), 577–593.
Martins, M. P., & Harris, S. L. (2008). Teaching children with autism to respond to joint attention initiations. Child & Family Behavior Therapy, 28(1), 51–68.
Meltzoff, A. N., & Moore, M. K. (1992). Early imitation within a functional framework: the importance of person identity, movement, and development. Infant Behavior and Development, 15(4), 479–505.
Moore, C., & Dunham, P. J. (Eds.). (2014). Joint attention: Its origins and role in development. Hillsdale: Lawrence Erlbaum Associates.
Mundy, P., & Sigman, M. (2006). Joint attention, social competence, and developmental psychopathology. In D. Cicchetti & D. J. Cohen (Eds.), Developmental psychopathology (pp. 293–332). New York, NY: Wiley.
Mundy, P., Sigman, M., Ungerer, J., & Sherman, T. (1986). Defining the social deficits of autism: The contribution of non‐verbal communication measures. Journal of Child psychology and Psychiatry, 27(5), 657–669.
Mundy, P., Sigman, M., & Kasari, C. (1990). A longitudinal study of joint attention and language development in autistic children. Journal of Autism and Developmental Disorders, 20(1), 115–128.
Mundy, P., Delgado, C., Block, J., Venezia, M., Hogan, A., & Seibert, J. (2003). Early social communication scales (ESCS). Coral Gables, FL: University of Miami.
Mundy, P., Block, J., Delgado, C., Pomares, Y., Van Hecke, A. V., & Parlade, M. V. (2007). Individual differences and the development of joint attention in infancy. Child Development, 78(3), 938–954.
Murza, K. A., Schwartz, J. B., Hahs-Vaughn, D. L., & Nye, C. (2016). Joint attention interventions for children with autism spectrum disorder: a systematic review and meta- analysis. International Journal of Language & Communication Disorders, 51(3), 236–251.
Muzammal, M. S., & Jones, E. A. (2016). Social-communication intervention for toddlers with autism spectrum disorder: effects on initiating joint attention and interactions with mother. Journal of Developmental and Physical Disabilities, 29(2), 203–221.
Osterling, J., & Dawson, G. (1994). Early recognition of children with autism: A study of first birthday home videotapes. Journal of Autism and Developmental Disorders, 24(3), 247–257.
Parker, R. I., Vannest, K. J., Davis, J. L., & Sauber, S. B. (2011). Combining nonoverlap and trend for single-case research: Tau-U. Behavior Therapy, 42(2), 284–299.
Presmanes, A. G., Walden, T. A., Stone, W. L., & Yoder, P. J. (2007). Effects of different attentional cues on responding to joint attention in younger siblings of children with autism spectrum disorders. Journal of Autism and Developmental Disorders, 37(1), 133–144.
Radley, K. C., O’Handley, R. D., Ness, E. J., Ford, W. B., Battaglia, A. A., McHugh, M. B., & McLemore, C. E. (2014). Promoting social skill use and generalization in children with autism spectrum disorder. Research in Autism Spectrum Disorders, 8(6), 669–680.
Rakap S. (2015). Effect sizes as result interpretation aids in single-subject experimental research: description and application of four nonoverlap methods. British Journal of Special Education, 42(1), 11–33.
Reichow, B., Volkmar, F. R., & Cicchetti, D. V. (2008). Development of the evaluative method for evaluating and determining evidence-based practices in autism. Journal of Autism and Developmental Disorders, 38(7), 1311–1319.
Robins, D. L., Casagrande, K., Barton, M., Chen, C. M. A., Dumont-Mathieu, T., & Fein, D. (2014). Validation of the modified checklist for autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics, 133(1), 37–45.
Rocha, M. L., Schreibman, L., & Stahmer, A. C. (2007). Effectiveness of training parents to teach joint attention in children with autism. Journal of Early Intervention, 29(2), 154–172.
Rodriguez, P. P., & Gutierrez, A. (2017). A comparison of two procedures to condition social stimuli to function as reinforcers for children with autism. Behavioral Development Bulletin, 22(1), 159.
Rudy, N. A., Betz, A. M., Malone, E., Henry, J. E., & Chong, I. M. (2014). Effects of video modeling on teaching bids for joint attention to children with autism. Behavioral Interventions, 29(4), 269–285.
Schertz, H. H., & Odom, S. L. (2007). Promoting joint attention in toddlers with autism: a parent-mediated developmental model. Journal of autism and developmental disorders, 37(8), 1562–1575.
Schertz, H. H., Reichow, B., Tan, P., Vaiouli, P., & Yildirim, E. (2012). Interventions for toddlers with autism spectrum disorders: an evaluation of research evidence. Journal of Early Intervention, 34(3), 166–189.
Schreibman, L., Dawson, G., Stahmer, A. C., Landa, R., Rogers, S. J., McGee, G. G., ... & McNerney, E. (2015). Naturalistic developmental behavioral interventions: Empirically validated treatments for autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(8), 2411–2428.
Shire, S. Y., Gulsrud, A., & Kasari, C. (2016). Increasing responsive parent–child interactions and joint engagement: comparing the influence of parent-mediated intervention and parent psychoeducation. Journal of Autism and Developmental Disorders, 46(5), 1737–1747.
Sitnick, S. L., Shaw, D. S., Gill, A., Dishion, T., Winter, C., Waller, R., … & Wilson, M. (2015). Parenting and the family check-up: changes in observed parent-child interaction following early childhood intervention. Journal of Clinical Child & Adolescent Psychology, 44(6), 970–984.
Sullivan, L., Mundy, P., & Mastergeorge, A. M. (2015). Joint attention in preschool children: is it a meaningful measure. Int J Sch Cog Psychol, 2(120), 2.
Toth, K., Munson, J., Meltzoff, A. N., & Dawson, G. (2006). Early predictors of communication development in young children with autism spectrum disorder: joint attention, imitation, and toy play. Journal of Autism and Developmental Disorders, 36(8), 993–1005.
Tsao, L. L., & Odom, S. L. (2006). Sibling-mediated social interaction intervention for young children with autism. Topics in Early Childhood Special Education, 26(2), 106–123.
Vaiouli, P., Grimmet, K., & Ruich, L. J. (2015). “Bill is now singing”: Joint engagement and the emergence of social communication of three young children with autism. Autism, 19(1), 73–83.
Vannest, K. J., & Ninci, J. (2015). Evaluating intervention effects in single-case research designs. Journal of Counseling & Development, 93(4), 403–411.
Vernon, T. W., Koegel, R. L., Dauterman, H., & Stolen, K. (2012). An early social engagement intervention for young children with autism and their parents. Journal of Autism and Developmental Disorders, 42(12), 2702–2717.
Vismara, L. A., & Lyons, G. L. (2007). Using perseverative interests to elicit joint attention behaviors in young children with autism: theoretical and clinical implications for understanding motivation. Journal of Positive Behavior Interventions, 9(4), 214–228.
Vismara, L. A., McCormick, C., Young, G. S., Nadhan, A., & Monlux, K. (2013). Preliminary findings of a telehealth approach to parent training in autism. Journal of Autism and Developmental Disorders, 43(12), 2953–2969.
Warreyn, P., & Roeyers, H. (2014). See what I see, do as I do: Promoting joint attention and imitation in preschoolers with autism spectrum disorder. Autism, 18(6), 658–671.
Warreyn, P., Paelt, S., & Roeyers, H. (2014). Social-communicative abilities as treatment goals for preschool children with autism spectrum disorder: the importance of imitation, joint attention, and play. Developmental Medicine & Child Neurology, 56(8), 712–716.
Wetherby, A. M., & Woods, J. J. (2006). Early social interaction project for children with autism spectrum disorders beginning in the second year of life: A preliminary study. Topics in Early Childhood Special Education, 26(2), 67–82.
Whalen, C., & Schreibman, L. (2003). Joint attention training for children with autism using behavior modification procedures. Journal of Child Psychology and Psychiatry, 44(3), 456–468.
White, P. J., O’Reilly, M., Streusand, W., Levine, A., Sigafoos, J., Lancioni, G., … & Aguilar, J. (2011). Best practices for teaching joint attention: a systematic review of the intervention literature. Research in Autism Spectrum Disorders, 5(4), 1283–1295.
Wong, V. C., & Kwan, Q. K. (2010). Randomized controlled trial for early intervention for autism: a pilot study of the Autism 1–2-3 Project. Journal of Autism and Developmental Disorders, 40(6), 677–688.
Yoder, P., & Stone, W. L. (2006). Randomized comparison of two communication interventions for preschoolers with autism spectrum disorders. Journal of Consulting and Clinical Psychology, 74(3), 426.
Zercher, C., Hunt, P., Schuler, A., & Webster, J. (2001). Increasing joint attention, play and language through peer supported play. Autism, 5(4), 374–398.
Zwaigenbaum, L., Bryson, S., Rogers, T., Roberts, W., Brian, J., & Szatmari, P. (2005). Behavioral manifestations of autism in the first year of life. International Journal of Developmental Neuroscience, 23(2), 143–152.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hansen, S.G., Carnett, A. & Tullis, C.A. Defining Early Social Communication Skills: a Systematic Review and Analysis. Adv Neurodev Disord 2, 116–128 (2018). https://doi.org/10.1007/s41252-018-0057-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41252-018-0057-5