
Abstract
Background
Irritable bowel syndrome (IBS) is a functional disorder that leads to abdominal pain; its diagnosis is based on Rome IV criteria (recurrent abdominal pain at least 1 day per week in the last 3 months with more than two of the following: related to defecation, associated with a change in stool frequency and/or with a change in stool appearance).
Objective
To characterize an outpatient population diagnosed with IBS in Colombia during 2017–2018.
Methods
A cross-sectional study based on a review of clinical records of patients with a primary diagnosis of IBS. A representative sample of 380 individuals was recruited from a population of 38,182 people with a new diagnosis of IBS from a drug-claim database. Sociodemographic, clinical (symptoms, type of IBS, alarm features, etc.), treatment (pharmacological or not), and follow-up variables (for those with additional medical care at 3–12 months) were analyzed. The diagnosis and treatment used in the consultation were compared with clinical guidelines.
Results
Most of the 380 patients were women (n = 238; 62.6%), and the mean age was 40.1 ± 15.0 years. None of the physicians recorded the Rome IV criteria in the medical records. Unclassified IBS was the most prevalent subtype (n = 311; 81.8%), and the main symptom was abdominal pain (n = 327; 86.1%). Only 73 patients (19.2%) had follow-up data. The most frequently used drugs were aluminum hydroxide (n = 203; 53.4%) and hyoscine N-butyl bromide (n = 200; 52.6%). Regarding drugs included in the clinical practice guidelines, 19 people received loperamide (5.0%), 3 received trimebutine (0.8%), and 1 received sertraline (0.3%).
Conclusions
The patients were diagnosed without clearly established criteria, and they were treated symptomatically with little follow-up.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Most patients diagnosed with IBS were unclassified and lacked clear diagnostic criteria. |
The majority of drugs prescribed were to treat symptoms and are not supported by evidence. |
A low proportion of patients had follow-up consultations during the next 3–12 months after initial IBS diagnosis. |
1 Introduction
Irritable bowel syndrome (IBS) is a functional bowel disorder in which abdominal pain is associated with changes in the frequency and consistency of defecation. It is assumed that there is no structural alteration that causes the symptoms [1]. IBS can be classified as IBS with predominant constipation, IBS with predominant diarrhea, IBS with mixed bowel habits, and unclassified IBS [2].
IBS is a disease with an estimated worldwide prevalence ranging from 10.0% to 20.0% [3, 4]. Literature on IBS in Colombia is scarce; however, a study conducted in Bogotá found a prevalence of 24.0% with a predominance of IBS with constipation (41.9%), followed by unclassified IBS (25.1%) [5].
Currently, the diagnosis of IBS is based on the Rome IV criteria, which have been revised over the years since 1999 [6]. According to the Rome IV criteria, recurrent abdominal pain (as a predominant symptom) must be present at least 1 day per week on average in the last 3 months, in addition to two or more of the following criteria: pain related to defecation, with a change in the frequency of feces and/or with a change in the appearance of feces [7]. In some patients with alarm features (warning signs or “red flag” symptoms that may indicate an underlying organic cause), initial complementary studies should be performed before making the diagnosis of IBS [6].
The therapeutic approach is based on the IBS subtype and predominant symptoms [6], and can be nonpharmacological or pharmacological [8]. Nonpharmacological treatment is focused on lifestyle and dietary changes [for example, a low fermentable oligosaccharides, disaccharides, monosaccharides, and polyols (FODMAP) diet ], while pharmacological treatment is aimed at managing different symptoms, such as abdominal pain, constipation, diarrhea, and abdominal distension [6, 8].
Considering the limited knowledge about the pathology of IBS and the therapeutic approach for patients with IBS at the local level, this study sought to determine the clinical characteristics and treatment of IBS among a random sample of Colombian patients in the primary care setting during the years 2017 and 2018.
2 Materials and Methods
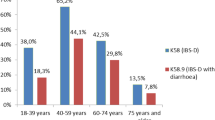
A descriptive cross-sectional study was conducted. The patients were identified from a population in a drug-claim database, belonging to Audifarma SA, the largest drug dispensing company in the country, which has information on more than 8.5 million Colombians. In this database, 38,182 patients, aged 18 years and older, from one health insurer (which provides access to individual medical records) who presented a diagnosis of IBS for the first time were identified. The diagnoses were recognized by codes of the International Classification of Diseases, tenth edition (ICD-10: K580, K589), during the period from September 2017 to October 2018. Pregnant patients were excluded.
To review the details of the clinical records of each study patient, a simple random sample was calculated and selected using Epidat v4.2, with a confidence interval of 95% and an error of 5%, which resulted in 380 individuals. The information was directly reviewed in the medical records (clinical data were not available in a structured database).
The following data were collected and measured from the included patients at the time of first diagnosis of IBS.
(a) Sociodemographic: age, sex, education and origin.
(b) Clinical symptoms (e.g., abdominal pain, bloating, diarrhea, constipation, nausea, flatus, etc.), alarm features (age over 50 years, gastrointestinal bleeding, unintentional weight loss, family history of inflammatory bowel disease or colorectal cancer, palpable abdominal mass or lymphadenopathy, severe nonfluctuating symptoms, anemia, and refractory diarrhea) [6], type of diagnosis (IBS with constipation, IBS with diarrhea, or mixed IBS and unclassified IBS). Additional diagnostic procedures (e.g., fecal occult blood test, stool tests, hemograms, colonoscopies, endoscopies, etc.) were also recorded. The IBS assessment should be made routinely using only the clinical diagnostic criteria; however, some patients may be eligible to undergo additional diagnostic procedures, especially those with alarm features to evaluate organic causes.
Regarding the type of IBS, we included those recorded by the treating physician (diagnosis codes) but also reclassified them using the symptoms described in the clinical records.
(c) Comorbidities (e.g., arterial hypertension, type 2 diabetes mellitus, dyspepsia, hypothyroidism, dyslipidemia, etc., as well as the sum of comorbidities).
(d) Treatment (nonpharmacological, such as low FODMAP diet or general recommendation of dietary changes [9]; pharmacological). The pharmacological treatment of IBS was reviewed, which is usually divided by clinical practice guidelines according to symptomatology or type of IBS: pain (peppermint oil, otilonium bromide, pinaverium bromide, trimebutine, mebeverine, tricyclic antidepressants, selective serotonin reuptake inhibitors), abdominal distension (rifaximin, pinaverium bromide), IBS with diarrhea (rifaximin, ondansetron, alosetron, cilansetron, ramosetron, tricyclic antidepressants, loperamide), and IBS with constipation (polyethylene glycol, bisacodyl, lubipristone, psyllium, linaclotide, sodium picosulfate) [6]. Medications prescribed by the doctor for the treatment of IBS that were not specifically described in the Colombian clinical practice guidelines (which are in line with international recommendations) were also identified [6], as well as the associated comedications. The duration of pharmacotherapy was not assessed.
The follow-up consultations of those patients who had additional medical care within 3 to 12 months after the initial diagnosis of IBS were also reviewed to analyze their symptoms, type of IBS, and number of attentions.
Clinical history software was used to review the previously mentioned characteristics of the study population. The data were validated, and any inconsistency was adjusted by at least two researchers to guarantee their reliability. Access to the clinical records application was provided by the health insurer. SPSS v26.0 was used for statistical analysis.
This research was classified according to resolution 8430/93 of the Ministry of Health of Colombia as a risk-free study and was endorsed by the Bioethics Committee of the Universidad Tecnológica de Pereira and the research ethics committee of the insurer. The data of the patients were handled confidentially, and it was not necessary to apply individual informed consent.
3 Results
A total of 238 of the 380 patients were female (62.6%). The average age was 40.1 ± 15.0 years. The age group of 31–49 years (162 patients; 42.6%) was the most frequent. Regarding the regions, more than half of the sample came from the Andean region. Most of the patients presented with a secondary educational level. Table 1 presents the other sociodemographic variables.
The predominant type of IBS reported by the physician was unclassified IBS (81.8%), followed by IBS with diarrhea. Unclassified IBS was slightly more common in women. IBS with diarrhea was more frequent in men. The most common symptoms were abdominal pain, bloating, and diarrhea (see Table 2). None of the physicians explicitly recorded or mentioned the Rome IV criteria in the medical records.
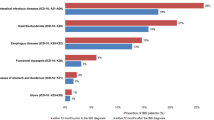
The most common comorbidity was arterial hypertension (14.2%), followed by dyslipidemia and dyspepsia. Similarly, the most common comedications were angiotensin II receptor antagonists, antidiabetics, and lipid-lowering drugs.
The diagnostic procedures performed were fecal occult blood test (n = 21, 5.5% of patients) and stool test (n = 21, 5.5%), and for 83 cases (21.9%), various other procedures were performed. Only one patient had a record of a colonoscopy (0.3%). A total of 123 patients (32.4%) presented alarm features; the most common were age over 50 years, rectal bleeding, and anemia. Table 2 presents the clinical variables of the people included in the sample.
The treatment received by the patients was based mainly on aluminum hydroxide, hyoscine N-butyl bromide, and recommendations for dietary changes. Of the medications indicated by the clinical practice guidelines, they only received loperamide, bisacodyl, trimebutine, and sertraline. The calculated mean dose of hyoscine N-butyl bromide was 30 mg/day, while omeprazole was the most used in the proton pump inhibitors group at an average dose of 20 mg/day. Of note, 52 patients (13.7%) received mesalazine and 25.0% were prescribed an antiparasitic agent (especially those with IBS with predominant diarrhea). Table 3 presents the different therapies found, as well as their distribution of use according to the type of IBS.
Only 73 patients (19.2%) had follow-up consultations for their disease within the following 3 to 12 months after diagnosis, including 44 women (60.3%) and 29 men (39.7%), mainly between 31 and 49 years of age. During follow-up, the most frequently described symptoms were abdominal pain (55 patients; 75.3%), abdominal distension (29 patients; 39.7%), flatus (20 patients; 27.4%) and diarrhea (19 patients; 26.0%).
The follow-up consultations showed that the most common subtype of IBS was unclassified IBS (n = 57, 78.1% of those with follow-up), followed by IBS with diarrhea (n = 14, 19.2%).
4 Discussion
The present study describes the clinical and treatment characteristics of IBS in a group of Colombian patients. It was found that IBS occurs more frequently in women, consistent with findings from previous studies [10,11,12,13]. The average age of the people included in this study is also close to that reported in other studies [10,11,12].
The research found that the most common subtype was unclassified IBS. In contrast, other studies report that the most common subtypes were IBS with predominant constipation, mixed bowel habits IBS, or IBS with predominant diarrhea [5, 10, 12]. In addition, one previous study recorded differences by sex and found a greater prevalence of mixed IBS among women and a greater prevalence of IBS with diarrhea among men [12]. The higher prevalence of unclassified IBS found herein may be due to the lack of application of the Rome criteria in these patients, thus it may generate erroneous diagnoses, in which symptoms are nonspecific and can be easily attributed to another disease.
The results of this research differ from the literature regarding alarm features, since it was found that the main feature was age over 50 years, while in another report, the most common was nocturnal symptoms [14]. It is worth mentioning that, for this variable, the published information is scarce, and there are no recent studies that focus directly on this topic, so the distribution of the frequency of alarm features could change over the years and should be examined in future studies.
The predominant symptom was abdominal pain, followed by distension and diarrhea, similar to the findings of Hungin et al. in the USA [15]. It is common for patients to present to healthcare institutions mainly due to the discomfort generated by the pain and the discomfort that accompanies abdominal distension, while other symptoms such as constipation require less consultation with the physician.
It was found that the most commonly prescribed treatment was aluminum hydroxide, followed by the antispasmodic hyoscine N-butyl bromide and dietary changes. In a study that reviewed the treatments used and their satisfaction in the USA, antispasmodics were the most commonly used drugs to treat IBS with diarrhea, a result comparable to this study, while polyethylene glycol, lubiprostone, and linaclotide were used to treat IBS with constipation. The most recommended nonpharmacological management was the use of probiotics, followed by dietary changes [16]. Regarding aluminum hydroxide, no information was found to support its formulation as a first-line therapy for IBS. Regarding the use of hyoscine N-butyl bromide in IBS, the evidence is limited, and although its usefulness has been shown in some studies [17, 18], it is still low compared with other antispasmodic medications [19]. Other treatments proposed, such as rifaximin or probiotics, were not identified in the patients included in this study [20]. A high proportion of patients also received antiparasitic agents or mesalazine, which is indicated only for inflammatory bowel disease, raising further concerns about the appropriateness of the treatments and diagnoses made in these group of patients that consult with gastrointestinal symptomatology.
Contrary to what the literature dictates, it was observed that diagnostic procedures are formulated for patients who consult for IBS, a practice that, apart from generating a monetary cost to the user, does not support the diagnosis of the disease, since it has been demonstrated in several studies that the diagnosis of IBS is mainly clinical and that any other action aimed at confirming its presence, including colonoscopy, stool studies, and hematological studies, among others, has low efficacy [14, 21,22,23]. However, it must be considered that the treating physician may request these diagnostic aids to rule out other pathologies that are generating the clinical manifestations.
Among the limitations of this analysis is its observational nature and the extraction of information from clinical records and not directly from patients, so it is possible that some variables of interest for follow-up were not evaluated, for example, if patients were referred or not to consultation by a specialist in gastroenterology or if they had a change in the diagnosis of irritable bowel over time. We had to use a random sample of patients because we did not have access to the clinical information of the entire population. Furthermore, the patients selected were from only one healthcare insurer, limiting the generalizability of the results to the entire population. The information regarding drugs different from those prescribed by the physician was not available (e.g., use of over-the-counter medications, such as probiotics).
On the other hand, it presented relevant strengths. The data was reviewed directly in clinical records and allowed to analyze symptoms and diagnostic approach. It includes drug patterns as well as other useful information, i.e., alarm features, use of diagnostic procedures or number of follow-ups after the initial diagnosis, making this manuscript an important descriptive evidence regarding IBS symptoms and treatment in Colombia.
5 Conclusions
These findings suggest that the majority of patients with IBS are women, individuals with few comorbidities, who present to medical consult mainly for pain, abdominal distension, and diarrhea, but who were diagnosed without clearly established criteria. Their symptoms are often treated with antacids and antispasmodics. Finally, they had little follow-up of the disease, which opens the possibility for new studies that investigate the possible long-term clinical outcomes of these patients.
Availability of data and material (name of repository)
Protocolos.io.
Code availability
Dx.doi.org/10.17504/protocols.io.e6nvwkr8dvmk/v1.
References
Defrees DN, Bailey J. Irritable bowel syndrome: epidemiology, pathophysiology, diagnosis, and treatment. Prim Care. 2017;44(4):655–71. https://doi.org/10.1016/j.pop.2017.07.009.
Drossman DA, Hasler WL. Rome IV-functional GI disorders: disorders of Gut-Brain interaction. Gastroenterology. 2016;150(6):1257–61. https://doi.org/10.1053/j.gastro.2016.03.035.
Lacy BE, Patel NK. Rome criteria and a diagnostic approach to irritable bowel syndrome. J Clin Med. 2017Oct 26;6(11):99. https://doi.org/10.3390/jcm6110099.
Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology. 2006;130(5):1480–91. https://doi.org/10.1053/j.gastro.2005.11.061.
Cañón M, Ruiz AJ, Rondón M, Alvarado J. Prevalence of irritable bowel syndrome and health-related quality of life in adults aged 18 to 30 years in a Colombian University: an electronic survey. Ann Gastroenterol. 2017;30(1):67–75. https://doi.org/10.20524/aog.2016.0093.
Alvarado BJ, Otero RW, Jaramillo Santos MA, Roa BPA, Puentes LGA, Jiménez FAM, et al. Clinical practice guideline for the diagnosis and management of adult patients with irritable bowel syndrome. Rev Colomb Gastroenterol. 2015;30:43–56.
Mearin F, Lacy BE, Chang L, Chey WD, Lembo AJ, Simren M, Spiller R. Bowel disorders. Gastroenterology. 2016;S0016–5085(16):00222–5. https://doi.org/10.1053/j.gastro.2016.02.031.
Sultan S, Malhotra A. Irritable Bowel Syndrome. Ann Intern Med. 2017;166(11):ITC81-ITC96. doi: https://doi.org/10.7326/AITC201706060.
Molina-Infante J, Serra J, Fernandez-Bañares F, Mearin F. The low-FODMAP diet for irritable bowel syndrome: lights and shadows. Gastroenterol Hepatol. 2016;39(2):55–65. https://doi.org/10.1016/j.gastrohep.2015.07.009.
Van den Houte K, Carbone F, Tack CC, Colomier E, Clevers E, Arts J, et al. Determinants of quality of life impact in irritable bowel syndrome patients diagnosed in primary care. Gastroenterology. 2019;156(6). https://doi.org/10.1016/S0016-5085(19)38884-5
Gómez Alvarez DF, Morales Vargas JG, Rojas Medina LM, Mújica Oviedo SC, Camacho López PA, Rueda Jaimes GE. Prevalence of irritable bowel syndrome and associated factors according to the Rome III diagnostic criteria in a general population in Colombia. Gastroenterol Hepatol. 2009;32(6):395–400. https://doi.org/10.1016/j.gastrohep.2009.01.177.
Choghakhori R, Abbasnezhad A, Amani R, Alipour M. Sex-related differences in clinical symptoms, quality of life, and biochemical factors in irritable bowel syndrome. Dig Dis Sci. 2017;62(6):1550–60. https://doi.org/10.1007/s10620-017-4554-6.
Palsson OS, Whitehead W, Törnblom H, Sperber AD, Simren M. Prevalence of Rome IV functional bowel disorders among adults in the United States, Canada, and the United Kingdom. Gastroenterology. 2020;158(5):1262-1273.e3. https://doi.org/10.1053/j.gastro.2019.12.021.
Whitehead WE, Palsson OS, Feld AD, Levy RL, Korff VON, M, Turner MJ, Drossman DA. Utility of red flag symptom exclusions in the diagnosis of irritable bowel syndrome. Aliment Pharmacol Ther. 2006;24(1):137–46. https://doi.org/10.1111/j.1365-2036.2006.02956.x.
Hungin AP, Chang L, Locke GR, Dennis EH, Barghout V. Irritable bowel syndrome in the United States: prevalence, symptom patterns and impact. Aliment Pharmacol Ther. 2005;21(11):1365–75. https://doi.org/10.1111/j.1365-2036.2005.02463.x.
Rangan V, Ballou S, Shin A, Camilleri M; Beth Israel Deaconess Medical Center GI Motility Working Group, Lembo A. Use of Treatments for Irritable Bowel Syndrome and Patient Satisfaction Based on the IBS in America Survey. Gastroenterology. 2020;158(3):786-788.e1. doi: https://doi.org/10.1053/j.gastro.2019.10.036.
Ford AC, Talley NJ, Spiegel BM, Foxx-Orenstein AE, Schiller L, Quigley EM, Moayyedi P. Effect of fibre, antispasmodics, and peppermint oil in the treatment of irritable bowel syndrome: systematic review and meta-analysis. BMJ. 2008;337: a2313. https://doi.org/10.1136/bmj.a2313.
Moayyedi P, Andrews CN, MacQueen G, Korownyk C, Marsiglio M, Graff L, Kvern B, Lazarescu A, Liu L, Paterson WG, Sidani S, Vanner S. Canadian association of gastroenterology clinical practice guideline for the management of irritable bowel syndrome (IBS). J Can Assoc Gastroenterol. 2019;2(1):6–29. https://doi.org/10.1093/jcag/gwy071.
Poynard T, Regimbeau C, Benhamou Y. Meta-analysis of smooth muscle relaxants in the treatment of irritable bowel syndrome. Aliment Pharmacol Ther. 2001;15(3):355–61. https://doi.org/10.1046/j.1365-2036.2001.00937.x.
Camilleri M. Diagnosis and treatment of irritable bowel syndrome: a review. JAMA. 2021;325(9):865–77. https://doi.org/10.1001/jama.2020.22532.
Hamm LR, Sorrells SC, Harding JP, Northcutt AR, Heath AT, Kapke GF, Hunt CM, Mangel AW. Additional investigations fail to alter the diagnosis of irritable bowel syndrome in subjects fulfilling the Rome criteria. Am J Gastroenterol. 1999;94(5):1279–82. https://doi.org/10.1111/j.1572-0241.1999.01077.x.
Lieberman DA, Holub J, Eisen G, Kraemer D, Morris CD. Utilization of colonoscopy in the United States: results from a national consortium. Gastrointest Endosc. 2005;62(6):875–83. https://doi.org/10.1016/j.gie.2005.06.037.
Vanner SJ, Depew WT, Paterson WG, DaCosta LR, Groll AG, Simon JB, Djurfeldt M. Predictive value of the Rome criteria for diagnosing the irritable bowel syndrome. Am J Gastroenterol. 1999;94(10):2912–7. https://doi.org/10.1111/j.1572-0241.1999.01437.x.
Acknowledgments
To Soffy Claritza López for her work in obtaining the database.
Funding
The present study did not receive funding.
Author information
Authors and Affiliations
Contributions
A.G.M.: drafting of the manuscript, data collection, data analysis, description of results, and discussion; D.A.H.V.: drafting of the manuscript, statistical analysis; E.R.M.: description of results and discussion of the article; J.D.M.M.: description of results and discussion of the article; J.S.G.C.: description of results and discussion of the article; K.M.P.; description of results and discussion of the article; L.P.M.: description of results and discussion of the article; M.G.M.: description of results and discussion of the article; J.E.M.A.: drafting of the manuscript, critical revision of the manuscript for important intellectual content, and study supervision. All authors read and approved the final version.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Ethics Approval
The protocol was approved by the Bioethics Committee of the Universidad Tecnologica de Pereira in the risk-free research category. The ethical principles established by the Declaration of Helsinki were respected. Patient personal data were not considered.
Consent to Participate
No applicable, is a retrospective observational study.
Writing Assistance
The manuscript was translate to English by American Journal Experts
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Hernández-Velásquez, D.A., Rodríguez-Martínez, E., Montoya-Meneses, J.D. et al. Clinical Characteristics and Treatment of Irritable Bowel Syndrome in a Colombian Population: A Cross-Sectional Study. Drugs - Real World Outcomes 10, 651–658 (2023). https://doi.org/10.1007/s40801-023-00395-x
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40801-023-00395-x