
Abstract
Purpose of Review
This review aims to highlight the contribution of Interventional Radiology in the setting of vascular trauma beyond the abdomen and present the latest innovations in this field.
Recent Findings
A shift from surgical operative management to endovascular management has occurred over the past decade. Critically ill patients are treated in hybrid operating rooms, by methods of damage control interventional radiology at the same time that resuscitation and trauma evaluation take place.
Summary
Hemorrhagic shock is one the leading causes of death. Transarterial embolization (TAE), stent graft deployment, and/or balloon occlusion can expeditiously stop hemorrhage and prevent exsanguination in a patient in extremis. Avoiding the additional physiological stress of the traditional surgical approach, these minimally invasive methods can be performed under moderate sedation and are associated with low morbidity and reduced hospital stays. As interventional angiography is rapidly expanding and evolving, so do its applications in traumatic vascular injuries of the head, neck, thorax, pelvis, and extremities.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Trauma is the main cause of death in people under 40 and the third cause of death in all age groups. Approximately 31.6 million people require treatment in the emergency department (ED) for trauma-related injuries annually [1]. Hemorrhagic shock along with central nervous system injuries remains the principal cause of death in trauma patients. Vascular injury is highly morbid and can lead to fatal exsanguination but life-saving interventions are possible [2]. Mechanism of traumatic vascular injury varies widely, with most being caused by high-velocity weapons (70–80%), followed by stab wounds (10–15%), and finally, blunt trauma (5–10%) [3]. The last has some unique features, making it clinically occult and difficult to diagnose. After an acute traumatic injury, the early diagnosis of the extent and the degree of pathology is critical.
The role of radiology in trauma care is constantly expanding serving as a diagnostic, as well as a therapeutic modality. Vascular trauma can be classified into five categories according to the imaging appearance: (1) damage of the intima and/or media with or without narrowing of the vessel lumen and creation of a dissection plane, (2) aneurysmal dilatation and/or pseudoaneurysm formation, (3) complete vessel occlusion, (4) arteriovenous (AV) fistula, and (5) complete vascular transection [4]. Regardless of the mechanism of trauma, these patterns of vascular injury are a challenging problem in the poly-traumatized patient because open exposure and surgical repair can often be very difficult. The evolution of endovascular technology has brought innovative strategies to manage such complex vascular injuries by temporizing or providing definitive therapeutic intervention. Integrating a variety of minimally invasive therapies, interventional radiology has become a fundamental aspect of modern trauma care and changed the management of vascular trauma over the last decade.
Methods of Endovascular Treatment
Initial imaging survey in vascular trauma is completed with computed tomography angiography (CTA), which offers a fast, non-invasive method to accurately evaluate pathology. CT angiography (CTA) can assess large-vessel integrity and depict arterial occlusions, transections, dissections, and intimal tears [5]. The evolution of non-invasive multidetector CT (MDCT) angiography has largely limited the use of digital subtraction angiography (DSA) as a diagnostic tool in trauma. Modern trauma diagnostic protocols recommend DSA only in rare cases of dubious CTA diagnosis or in trauma cases in which accurate surgical planning is required [6]. Positive signs of acute vascular trauma are frank extravasation of injected contrast agent, which may be contained as in the case of a pseudoaneurysm or uncontained with free spill into the surrounding tissues, frank cutoff of a vessel, formation of an arteriovenous fistula, luminal abnormality consistent with anatomical injury, and dissection of a major artery with visible intimal flap [7•].
In the setting of acute trauma, endovascular intervention can effectively isolate the arterial injury from the circulation. Endovascular techniques implicate over-the-wire access to the arterial or venous system and placement of a sheath. Once access is achieved, wires and catheters are directed to the anatomic site of interest, by the aid of fluoroscopy. Moderate sedation is necessary for procedural comfort, assisting the patient to remain still and cooperative during angiography. Under moderate sedation, the patient should be able to respond to verbal commands and no intervention to maintain the airway is necessary [8]. Midazolam and fentanyl are the most commonly used drugs for moderate sedation. Nonetheless, due to the complexity of trauma patients, many procedures are performed under general anesthesia.
Percutaneous, endovascular access to a given anatomic region may be required to perform a diagnostic contrast study, accomplish large-vessel occlusion, or repair a vessel disruption. A combination of these techniques is also possible during endovascular approach to injury. More precisely, interventional treatment methods commonly utilized in the trauma setting are the following:
Transarterial Embolization
First described in 1972, transarterial embolization (TAE) has become an indispensable tool in the armamentarium for hemorrhage control and is widely employed for expeditious control of bleeding, avoiding extensive tissue disruption resulting from surgical interventions [9, 10]. TAE has an adjunctive role in managing polytrauma bleeding and studies have demonstrated a 91% success rate when it is utilized as a first-line therapeutic modality [11, 12]. Knowledge of the arterial anatomy, role of collateral arterial flow, available equipment, and procedural risks is crucial for effective TAE.
The procedure involves the introduction of particulate matter into the circulation to mechanically occlude bleeding vessels [13]. A variety of catheters and coaxial microcatheters designed for smaller vessels is readily available for super-selective catheterization of most parts of the arterial circulation. The choice of embolic agent is mainly based on the site and nature of the injury, the desire to maintain adequate collateral flow, and the operator’s experience and preference. Embolic agents differ according to their permanency and level of arterial occlusion [5]. Microcoils, glue, microparticles (permanent embolic agent), and gel foam slurries (absorbable embolic agent) are most commonly used. Glue and gel foam slurries may cause proximal vascular occlusion and ischemia if dislodged from the original site of deployment. The risk of non-targeted embolization, which may cause ischemic complications, can be eliminated by detachable coils and microcoils delivered via coaxial microcatheters, which are excellent for super-selective TAE [14]. Larger vessels require deployment of larger coils or vascular plugs, while traumatic AVMs can be treated with Onyx which is a novel liquid embolization agent. Direct comparison of embolic agents has not shown one to be superior to another [15••]. A frequent complication, which should be anticipated after TAE, is the delayed bleeding due to the dislodgment of a thrombus from a nearby artery or the vasodilation of an artery that was initially in spasm [16•].
Stent Grafts
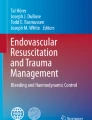
While injuries of expendable arteries with well-developed collateral supply can be treated with TAE, management of traumatic lacerations of main-donor arteries requires preservation of vascular luminal patency [17••]. Stent grafts are increasingly being applied for treatment of vessel injuries, avoiding complex surgical vascular repairs in areas with trauma-related anatomic distortion. Arterial ruptures, dissections, pseudoaneurysms, and arteriovenous communications can be managed by femoral or brachial artery access sites, depending on the location of the vascular injury. Accurate deployment of self-expandable stents requires a stiff guide wire for support. These stents are flexible, can conform to different diameters in a single vessel, and have a higher resistance to mechanical fatigue in mobile joint sites (Fig. 1). On the other hand, balloon expandable stents are usually applied in non-mobile areas such as the big trunk proximal vessels, offering great precision during deployment [18].

a DSA of a patient with one large post-endarterectomy 5 cm left common carotid artery pseudoaneurysm and smaller 2 cm pseudoaneurysm at the level of the carotid bifurcation. Following the positioning of a 9Fr sheath at the right common femoral artery, a sheath was positioned at the level of the common carotid artery and a hydrophilic guide wire was advanced within the internal carotid artery. b Following the deployment of an 8 × 60 self-expandable stent graft, both lesions were excluded from the circulation, while the common and internal carotid arteries remained patent. Hemostasis of the puncture site was obtained with the off-label use of the Starclose extravascular closure device
Balloon Occlusion
Inflation of an angioplasty balloon proximal to or at the site of a major arterial injury may temporally stabilize a patient in extremis, stopping life-threatening hemorrhage, and allowing preoperative planning for surgical or endovascular repair. This concept is the principle behind REBOA technique.
Evolution of Endovascular Techniques in Trauma
The management of vascular trauma has changed dramatically over the last decade. Trauma centers are increasingly endorsing a multidisciplinary approach to trauma care that involves not only surgeons but also interventional radiologists [16•]. The breakthroughs in imaging and device technology combined with the increasing expertise in endovascular techniques led to significant changes in the treatment algorithm of the injured patient.
Traditionally, hemodynamically unstable (HU) patients have been taken straight to OR rather than undergo a CT or an angiography study to localize and treat the hemorrhage [7•]. Today, it is widely accepted that even hemodynamically unstable patients can undergo endovascular treatment in the angiography suit, especially in cases in which surgery entails a high mortality risk [19]. Moreover, as hybrid operating rooms with imaging devices and endovascular equipment are implemented across the world, severely ill patients can now be treated at the same time that resuscitation and trauma evaluation take place [20•]. Advanced hemodynamic support and monitoring during angiography can be provided by anesthesiologists; however, in many cases, monitoring and sedation could also be provided by radiology nurses [21].
Many trauma centers, after the initial patient survey, conduct a CT Pan-scan and proceed with damage control interventional radiology (DCIR); the expansion of TAE into the trauma scene that focuses primarily on expeditious control of hemorrhage in HU patients rather than embolization precision [22••]. Several studies document this increase in the use of endovascular therapy for a wide variety of arterial injuries, including carotid arteries, subclavian and axillary arteries, thoracic aorta, iliac arteries, and upper and lower limb systems.
Head and Neck
Common/Internal Carotid Arteries
Neck trauma is frequently accompanied by vascular injury and carotid arteries are commonly affected [23]. Blunt carotid artery injury (BCAI) is found in 0.5% of all head trauma cases, while a combination of head and chest trauma has been reported to be correlated with a 14-fold increase in the likelihood of carotid artery injury [24, 25]. Without prompt diagnosis and proper treatment, blunt carotid injuries are associated with high mortality rates and permanent neurologic impairment in 40–80% of patients [26]. Generally, extracranial BCAI is asymptomatic and associated with a Glasgow Coma Scale (GCS) of > 8, while intracranial BCAI is frequently characterized by GCS < 8 and concurrent facial injuries [27]. Clinical manifestations of carotid injury include craniocervical or thoracic pain, bleeding, dysphagia, hoarseness, hypotension, expanding or pulsatile hematoma and neurologic deficits [28]. Onset of symptoms due to BCAI may occur immediately; however, many patients exhibit a latent period that can range from 1 h to several weeks [29].
The implementation of screening protocols, using CT angiography (CTA) to identify BCAI at admission, has significantly reduced diagnostic delay. In most trauma centers, CTA is routinely performed in patients with suspected neurovascular injury, including all patients with cervical spine injuries. On the other hand, DSA, the gold standard for diagnosis of BCAI is preferred in cases of penetrating neck injuries. Angiography can also be very useful when neurovascular injury proven on CTA needs further investigation, when there are acute focal neurological signs that significantly contradict the presentation on CT scan and when patients present with lower cranial nerve neuropathy or Horner’s syndrome.
A grading system of BCAI has been implicated for prognostic and therapeutic purposes. Grade I injury represents mild intimal injury, grade II injury consists of a dissection with a raised intimal flap or vessel thrombosis resulting in luminal narrowing greater than 25%, grade III injury is characterized by the formation of an aneurysm or a pseudoaneurysm, grade IV injury represents vessel occlusion or thrombosis, and finally, grade V injury is the complete transection of a vessel (Table 1). All these lesions have an increased risk of progression to stroke or death [30].
No randomized prospective study has determined optimal treatment for BCAI yet. The type of arterial injury, the hemodynamic and neurologic status as well as the presence of active bleeding foci, should all be evaluated before decision-making. In case of neurologically stable patients with grades I, II, and IV injuries, commonly accepted first-line treatment regimen is close surveillance with anticoagulation or antiplatelet medications [31]. However, administration of these medications may not always be feasible, as many patients have comorbid contraindications to blood thinners. Furthermore, most providers do not repair small dissecting aneurysms immediately but instead obtain frequent follow-up imaging and proceed with surgical or endovascular reconstruction if the lesion deteriorates [32]. Although small intimal injuries respond well to conservative measures, grade II injuries or greater are related to a worse prognosis. Indeed, only 20% of grade II injuries resolve at follow-up; the rest persists and can even worsen [30].
Carotid injuries are usually located near the base of the skull; a difficult area to approach and repair surgically. Extensive exposures, sometimes involving broad dissection, mandible subluxation, digastric muscle division, and styloid process removal, are necessary to achieve adequate proximal and distal vessel control and may result in significant cranial nerve damage and perioperative stroke [33, 34]. In cases of acute carotid bleeding, fluoroscopy followed by endovascular treatment can rapidly establish complete hemostasis. Adequate collateral cerebral circulation, via the circle of Willis, can be evaluated by balloon compression angiographic studies with injection of the contralateral carotid and the vertebral arteries. ICA can be selectively occluded in actively bleeding patients with good collateral cerebral circulation [35•]. However, a post procedural risk of stroke exists [36].
Traumatic ICA dissections can be treated with endovascular stent deployment especially in cases of hemodynamic compromise to the brain and/or contraindications to anticoagulation [32]. Stent devices adhere the dissecting intimal flap to the vessel wall and promote laminar flow through the vessel lumen, while the diversion of blood away from the dissection site promotes stent endothelialization over time. Although covered stents lack mechanical flexibility, they may be considered in the setting of frank arterial extravasation [37]. Endovascular stent reconstruction of carotid arterial dissection has been proven to be safe and technically feasible, with minimal or no complications [38].
Intracranial grade IV lesions, pseudoaneurysms, that lack a true vessel wall and are limited by organized hematoma and fibrosis usually become symptomatic in the following 1–3 weeks after the initial injury and present with a catastrophic intracranial hemorrhage or with a massive epistaxis episode [39, 40]. The mortality rate in this situation can be as high as 50% [41]. Even small pseudoaneurysms (2 cm) are known to deteriorate over time if managed expectantly as their natural history is to become bigger, thrombose or rupture [24, 42]. The surrounding tissues become inflamed and distorted, rendering therapeutic interventions more difficult.
While open surgery in this setting is technically demanding and associated poor outcomes, endovascular treatment is an effective and safe alternative with no reported mortality and very low morbidity [43]. Endovascular methods include TAE for obliteration of the parent artery of the pseudoaneurysm or bare stent deployment with or without detachable coil threading through the stent interstices. Covered ultra-thin PTFE stent grafts, both self and balloon expandable, can also be used and provide immediate exclusion of the pseudoaneurysm. However, care must be taken to ensure appropriate introduction of the stent graft into the distal carotid injury area due to its anatomic complexity and tortuosity [44].
Endovascular treatment with stent devices is associated with satisfactory results concerning short- and mid-term patency and dual antiplatelet regimen seems to be beneficial [45]. Nonetheless, questions may arise about the durability of carotid stenting.
External Carotid Arteries
Patients with traumatic lesions in ECA branches most likely present with epistaxis.
If conventional techniques fail to stop the bleeding, TAE using detachable coils, polyvinyl alcohol particles, Gelfoam, or a combination of these embolic materials is very effective with low rates of rebleeding or complications. When opting for TAE of the external carotid artery, meticulous angiographic work-up evaluating the presence of potential anastomotic channels between extracranial and intracranial circulation is crucial, as to avoid embolization of non-expendable vessels. Another important technical aspect is that the stumps proximal and distal to the bleeding focus should be identified and embolized together, as collateral vessels to the distal stump may cause recurrent bleeding [35•].
Vertebral Arteries
Vertebral artery injuries are rare and caused primarily by penetrating trauma to the neck and less frequently by blunt trauma [46]. CTA can adequately detect a VA lesion; however, as the potential for a missed injury must be recognized, DSA should be used when there is a high clinical suspicion arising from the trauma mechanism. While mild to moderate VA dissections can be asymptomatic and have a benign clinical course with spontaneous healing, VA pseudoaneurysms can progressively enlarge and lead to embolic or ischemic stroke [46, 47]. The initial therapeutic approach of the hemodynamically stable patient is based on anticoagulation with low-dose heparin for all VAIs except for those with grade V injury, unless absolute contraindications to systemic anticoagulation are present [48]. Hemodynamically unstable patients with vertebral artery transections are treated endovascularly [49].
Endovascular therapy is currently preferred as open surgical exposure of the V2 segment of the vertebral artery, the segment that is most prone to injury, appears challenging even for experienced surgeons due to its anatomic location within the vertebral column [50]. Vertebral artery injuries that do not involve the posterior inferior cerebral artery (PICA), can be safely treated by TAE in patients with adequate posterior cerebral circulation. On the other hand, dominant vertebral vessels should be revascularized by stenting [51•]. Grade III injuries can be treated with flow-diverters, a new generation of flexible self-expanding stent-like devices with high metal-to-surface coverage area that alters blood flow and promotes progressive thrombosis. The use of these devices appears promising, as in a clinical follow-up of 18 months there were no neurological complications and persistent pseudoaneurysm occlusion with full arterial patency was observed in all cases [51•, 52].
Thorax
Innominate Arteries
Innominate artery injuries have a very high morbidity and mortality, as these injuries are not easily accessible and are frequently associated with trauma of adjacent tissues. The risk of stroke and massive hemorrhage is high [53].
Unstable patients must go directly to the OR especially when bleeding cannot be controlled by endovascular balloon occlusion or Foley catheter tamponade [54]. A median sternotomy that may require extension into the neck is the approach of choice which may appear challenging in the emergency setting. In certain patients with a common arterial trunk giving rise to both carotids and to the right subclavian artery (bovine trunk), the situation becomes even more critical as deep hypothermic circulatory arrest with cardiopulmonary bypass must be utilized for cerebral protection [55].
Stable patients with injuries between the clavicle and the cricoid cartilage should undergo selective exploration with angiography. Available data indicates that endovascular repair of innominate artery injuries in patients sufficiently stable to undergo an angiogram was combined with minimal intensive care and hospital stay, decreased blood transfusions and reduced operative time and morbidity. Stent graft devices are most commonly used in order to preserve the patency of the affected vessel [54].
Axillosubclavian Arteries
Axillary and subclavian artery injuries (ASAI) are relatively rare, most commonly occurring after car accidents or falls [56]. Although ASAIs account for less than 9% of all vascular injuries, they are significantly morbid and they usually coexist with traumatic lesions of adjacent tissues like the brachial plexus, the aero-digestive tract, the venous and the lymphatic system and with several bone fractures [57]. Therefore, appropriate care must be taken to meticulously rule out ASAI in every trauma patient in order to avoid poor outcomes.
Findings that should alert the physician to investigate the possibility of a subclavian artery injury are the following: diminished radial pulse, fractured first rib, presence of a supraclavicular hematoma, chest film evidence of a widened superior mediastinum and finally, indication of a brachial plexus palsy [58]. CTA is imperative in such injury cases in order to plan for the optimal therapy and depict the anatomic relations of the lesion.
Open surgical approach for the management of ASAI is technically demanding and is associated with mortality rates ranging from 5 to 30% [57, 59]. Half of these injury cases require thoracotomy or sternotomy with open exposure of the clavicle, which poses the risk of damaging the surrounding neurovascular structures present in high density in the thoracic outlet [60].
As endovascular techniques have evolved, hemodynamically unstable patients can be expeditiously managed with balloon tamponade to stop ongoing hemorrhage at the site of the lesion and simultaneous endograft deployment to provide definite treatment or to temporize the injury and permit evaluation of concomitant injuries [61]. These interventions could be ideally performed in a hybrid endovascular–surgical suite under local anesthesia [62]. Complete transection of the axillary artery has no longer been considered as a contraindication for endovascular treatment as dual brachial and femoral access can be combined in a through-and-through approach to yield adequate guidewire manipulation and endograft positioning [62]. A potential drawback of the use of a stent graft is the coverage of collateral vessels such as the vertebral or the internal mammary artery. However, this condition is rare, as most of the injuries appear to the axillary instead of the proximal subclavian artery and a bare metal stent could be used as an alternative, if appropriate [63•].
Short- and mid-term results of endovascular revascularization are promising but data about long-term patency and durability are currently lacking [63•]. It seems that compliance with follow-up is critical to prevent ischemic outcomes due to loss of patency after covered stent placement for ASAI. Furthermore, additional research is required to clarify the ideal duration of dual antiplatelet therapy. In a trauma population that is usually young and active, stent graft durability may be limited. Nevertheless, stent failure does not preclude future revascularization, which if needed, may be done under less urgent circumstances, after the acute injury has been stabilized.
Breast Trauma
Blunt breast trauma is usually seen in motor vehicle accidents involving high speed and airbag deployment and results from direct compression. As breast hemorrhage may be difficult to control due to the loose areolar tissue, subselective catheterization and embolization is an excellent alternative to surgery for the rapid control of the bleeding [64].
Intercostal Arteries
Embolization of intercostal arteries could be a potential therapeutic option for arterial bleeding in blunt chest injury that involves multiple rib fractures, avoiding the morbid risks of thoracotomy [65].
Aorta
Blunt traumatic thoracic aortic injury (BTTAI) represents the second most common cause of death in trauma patients after intracranial hemorrhage and up to 85% of patients die before hospitalization [66]. BTTAI is usually caused by abrupt deceleration during a motor vehicle accident or a fall from a significant height that exerts shearing forces to the immobile aortic isthmus; the junction between the aortic arch and the descending aorta [67]. The osseous pinch theory is another mechanism of injury that has been described, according to which the aorta is crushed between the anterior and posterior bony thoracic structures [68]. Prognosis is generally dependent on the severity of accompanying injuries and some providers advocate delayed BTTAI repair, prioritizing hemodynamic stabilization and care of non-aortic traumatic injuries [69].
Available data shows that in-hospital mortality in patients managed non-operatively is high, whereas mortality is significantly lower for patients treated by surgery or endovascular repair [70]. Over the last decade, thoracic endovascular aortic repair (TEVAR) has become the first choice for the management of grade II or higher BTTAI and open surgery is currently indicated only for patients with traumatic femoral arteries and no alternative vascular access site or problematic stent landing zones [71]. The main reason behind this trend is the great speed and the significantly reduced invasiveness of endovascular repair, which allows concomitant abdominal, cranial, and orthopedic trauma to be addressed simultaneously without requiring patients’ spine injuries to be repositioned. Most physiologic insults involved in traditional surgical repair are eliminated, as thoracotomy, cardiopulmonary bypass, aortic cross-clamping, and single lung ventilation are not necessary. General anesthesia may possibly be avoided and heparinization can be minimized [72, 73]. These features of TEVAR are associated with significantly shorter hospital stays. Furthermore, the overall incidence of endovascular procedure adverse events such as aortic perforation or endograft misalignment is favorably low [74••].
Mid-term TEVAR outcomes are excellent but significant challenges remain regarding the long-term durability of this treatment [74••]. Given the lack of prospective randomized control trials, optimal follow-up surveillance schedule is still under investigation and remains empirically annual in many centers [75••]. However, annual CT imaging exposes patients to significant cumulative radiation dose and intravenous contrast agent toxicity. Taking into account that BTAI is more frequent in young people, these concerns become even stronger [76]. Considering the durability of modern endovascular devices, some authors propose that annual routine CTA may not be required and should be avoided after the first years of follow-up or substituted by alternative imaging modalities such as MRA [77•].
Pelvis
Pelvic fractures are associated with high mortality due to accompanying hemodynamic instability [9]. Despite the implementation of an early multidisciplinary approach in many trauma centers and the improved protocols in hemodynamic resuscitation, some patients do not respond; administration of more than 20 units of blood is correlated with mortality rates as high as 64% [78]. One critical priority in the management of pelvic fractures is to determine the bleeding source. Whole body CT with contrast should be the first-line imaging modality in pelvic trauma patients who respond at least partially to resuscitation [79•].
Pelvic hemorrhage is usually venous or bony in origin. The increased pelvic pressure resulting from concomitant hematoma can support hemostasis, especially if combined with pelvic packing and fixation procedures [80]. On the other hand, pelvic bleeding that leads to hemodynamic instability despite appropriate fluid resuscitation and mechanical stabilization of the pelvis is most commonly a result of an arterial injury [81, 82•]. Angiography can carefully evaluate the distal aorta and the branches of the internal iliac artery, such as the obturator and the internal pudendal artery and control hemorrhage by TAE (Fig. 2).

An 83-year old male with pelvic fracture and hemodynamically stable. Following right common femoral artery access, and right internal iliac artery (IIA) catheterization, active extravasation was noted (circles) at selective (a) and super-selective (b) DSA using a microcatheter. c, d Final selective DSA following Gelfoam embolization depicts the occlusion of the feeding vessel (arrows), without active extravasation of contrast and preservation of the patency of all main IIA branches
According to modern trauma algorithms, selective embolization of the internal iliac artery branches is considered as the first-line treatment for the management of traumatic pelvic hemorrhage. In the setting of pelvic trauma, hemodynamic stability, body temperature of more than 36 °C, normal respiratory rate, and associated injuries involving less than two organ systems are all factors that predict good embolization outcomes [83•]. The high technical and clinical success rate, as well as the minimal complications of TAE compare favorably to the risks of open surgery. As pelvic TAE is usually performed under emergent circumstances, Gelfoam, a non-permanent embolic agent that does not preclude future vessel revascularization, is usually preferred. This agent, capable of migrating distally inside the arterial lumen, is optimal for cases that do not allow for selective vessel catheterization. Some authors, however, associate the occlusion of the internal iliac artery with the risk of ischemic complications such as pelvic perineal infection, skin necrosis, and nerve damage; therefore, non-selective TAE of the internal iliac artery should be employed only in cases where prompt hemodynamic stabilization is required [84].
Angiography can also be very efficient for some special situations of pelvic trauma. A frequent pelvic anatomic variant, the direct communication between the obturator and the external iliac artery, termed “corona mortis,” can be easily detected in fluoroscopy and treated by embolization if lacerated [85]. Moreover, in case of intertrochanteric or ilium fracture, angiography can carefully evaluate for external iliac artery (EIA) branch vessel injury; an injury that is frequently missed as the threshold for bleeding detection directly relates to the distance of the catheter tip from the bleeding site [86, 87•].
Reboa
Management of vascular injury within the pelvis and the proximal femoral region is challenging [88]. In this anatomic location between the torso and the extremities, hemostasis cannot be achieved by direct pressure or tourniquet application and generally requires surgical intervention within the abdomen [89]. Surgical exposure and occlusion of the terminal aorta is a rate-limiting step that may impede prompt and effective resuscitation. Moreover, concurrent hemorrhagic shock may prevent patient transport to the angiographic suite for TAE.
An alternative method for hemorrhage control involves employment of an endovascular aortic balloon; this procedure has been named resuscitative endovascular balloon occlusion of the aorta (REBOA) when used in the trauma setting. Initially described in 1954 during the Korean War, this technique has been considered of limited application due to difficulties with positional balloon deployment [90]. As technology and modern trauma protocols have overcome initial technical obstacles, it is found that hemodynamically unstable patients suffering from blunt or penetrating injuries to the abdomen or pelvis, that do not respond to standard trauma resuscitation techniques, are likely to benefit from REBOA [91]. Currently, REBOA is used to stabilize the patient in order to perform life-saving surgical or endovascular damage control procedures or to allow transfer to a specialist trauma center [92].
REBOA procedure begins with femoral artery cannulation and introduction of a guide wire, atop which the occlusion balloon is advanced within the aorta. A 7Fr REBOA catheter was introduced in 2016, reducing complications of former larger sheaths. The diameter reduction leads to minimal intimal injury to the common femoral artery, improved arterial flow to the lower extremity and reduced turbulence, associated with a lower rate of thrombus formation [93•, 94].
Common femoral artery access, percutaneous under ultrasound guidance or surgical via a femoral cut-down, accounts for the majority of the procedural time and can be technically demanding in the profoundly shocked patient. Central aortic wire confirmation and accurate balloon inflation and positioning are essential in order to minimize adverse outcomes. Zone III, the location lying between the lowest renal artery and the bifurcation of aorta, is specifically used for pelvic trauma. While surgeon-performed FAST can consistently identify the aorta and the presence of the aortic guide wire, surface anatomy and the distance between the umbilicus and the femoral puncture site can provide a quick estimate about the balloon’s insertion depth [95, 96]. Some providers advocate contrast-enhanced ultrasonography as an alternative method of monitoring precise catheter placement and balloon inflation within zone III but questions arise concerning the availability and the additional time required for preparation of contrast material [97]. After balloon inflation, the disappearance of femoral pulses indicates appropriate balloon placement and should be carefully observed [92].
After a successful REBOA, the risk of shock reappearance due balloon deflation must be emphasized and anticipated as it can cause hemodynamic instability and sudden afterload reduction [92]. Moreover, as REBOA may cause tissue ischemia below the level of the occlusion, available procedural time is limited [98]. Partial REBOA (P-REBOA), a novel technique that allows controlled blood flow distal to the site of balloon deployment, can prolong the safe duration of aortic occlusion [94, 99•].
Although REBOA has already been included in the pre-hospital trauma management mainly in JAPAN and London (London’s Air Ambulance’s Physician-Paramedic team), its exact role in severe trauma remains to be determined as more data regarding safety and efficacy are required [100].
Extremities
Injuries of the extremity arteries are an unusual albeit serious consequence of trauma [5]. If not expeditiously treated, these lesions can result in hemorrhagic shock, limb ischemia, and neurologic injury with high risk of extremity loss. A delay in management of more than 6 h is associated with increased amputation rates [101].
In case of extremity artery injury with hemodynamic instability, immediate treatment is imperative. Classic surgical approach involving end-to-end vessel anastomosis or arterial suture with patch or graft introduction may be challenging in the emergency setting and can be complicated by several technical and anatomical factors [102, 103]. Moreover, tissue loss, hematoma formation, and trauma contamination, combined with the significant additional stress caused by the surgical operation, increase procedural morbidity [104].
Endovascular repair is great alternative for patients who cannot undergo immediate surgery due to concomitant injuries, or patients who are poor candidates for general anesthesia [105]. It can be used to stabilize the trauma patient temporary or serve as a bridge to future non-emergent conventional surgical repair [106]. Both TAE and stent grafting achieve very high immediate clinical success and low complication rates. Bleeding injuries of lower extremity branch vessels, such as the profunda femoralis and the infrapopliteal trifurcation can be safely and efficiently treated by TAE [107].
Endovascular techniques using stent grafts allow for rapid treatment of non-expendable bleeding arteries and reduce early mortality rates [106]. Self-expanding stents are usually preferred due to their flexibility which facilitates appropriate deployment in tortuous vessels, compared to more rigid balloon-expandable covered stents which are reserved for larger proximal vessels. The keynote to successful grafting of an extremity artery is appropriate sizing which certainly requires accurate pre-procedural CTA measurements. Notably, hypovolemia could lead to vessel diameter underestimation. As a general rule, self-expandable grafts should be oversized by 10–20% to achieve optimal sealing [17••]. Long-term durability of stent repair has not yet been established. Some published reports about long-term outcomes after endovascular repair in peripheral arterial vessels reveal satisfactory results [106]. However, lack of consensus exists regarding which anatomic locations may be approached endovascularly [108].
Conclusion
Uncontrolled hemorrhage remains as one of the leading causes of death in critically ill trauma patients, despite technological progress in cross-sectional imaging and implementation of novel transfusion and resuscitation protocols. Interventional angiography has made non-operative management of vascular injuries possible, avoiding the risks of open surgery. The application of endovascular treatment in the setting of trauma has been relatively belated; however, its effectiveness is rapidly being recognized. Today, many centers across the world employ interventional angiography methods for hemorrhage control and as endovascular management of trauma becomes more common, so do the indications for its use.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
NCIPC: Web-based Injury Statistics Query and Reporting System (WIQARS). http://www.cdc.gov/injury/wisqars.
Stewart RM, Myers JG, Dent DL, et al. Seven hundred fifty-three consecutive deaths in a level I trauma center: the argument for injury prevention. J Trauma. 2003;54:66–70. discussion −1
Mattox KL, Feliciano DV, Burch J, Beall AC Jr, Jordan GL Jr, De Bakey ME. Five thousand seven hundred sixty cardiovascular injuries in 4459 patients. Epidemiologic evolution 1958 to 1987. Ann Surg. 1989;209(6):698–705.
Kandarpa K, Gardiner GA Jr, Keller FS. Diagnostic arteriography. In: Kandarpa K, Machan LS, editors. Handbook of interventional radiologic procedures. Philadelphia: Lippincott Williams & Wilkins; 2011. p. 61–83.
Gould JE, Vedantham S. The role of interventional radiology in trauma. Semin Interv Radiol. 2006;23(3):270–8.
Uyeda JW, Anderson SW, Sakai O, Soto JA. CT angiography in trauma. Radiol Clin N Am. 2010;48(2):423–38.
• Yim NY, Kim YT, Kim HO, Kim JK, Kang YJ, Park YC, et al. Role of interventional radiology in trauma care: retrospective study from single trauma center experience. Am J Emerg Med. 2014;32(11):1315–8. https://doi.org/10.1016/j.ajem.2014.07.037. The above reference describes that interventional procedure can improve survival rate in patients with a traumatic vascular injury.
Rex DK. Review article: moderate sedation for endoscopy: sedation regimens for non-anaesthesiologists. Aliment Pharmacol Ther. 2006;24(2):163–71.
Eastridge BJ, Starr A, Minei JP, O'Keefe GE, Scalea TM. The importance of fracture pattern in guiding therapeutic decision-making in patients with hemorrhagic shock and pelvic ring disruptions. J Trauma. 2002;53:446–50. discussion 50–1
Kessel D. Trauma embolization: techniques. Presented at the annual meeting of the Cardiovascular and Interventional Society of Europe (CIRSE), September 19–23, 2009, Lisbon, Portugal.
Velmahos GC, Toutouzas KG, Vassiliu P, et al. A prospective study on the safety and efficacy of angiographic embolization for pelvic and visceral injuries. J Trauma. 2002;53:303–8. discussion 8
Velmahos GC, Demetriades D, Chahwan S, Gomez H, Hanks SE, Murray JA, et al. Angiographic embolization for arrest of bleeding after penetrating trauma to the abdomen. Am J Surg. 1999;178:367–73.
Lopera JE. Embolization in trauma: principles and techniques. Semin Interv Radiol. 2010;27:14–28.
Wallis A, Kelly MD, Jones L. Angiography and embolisation for solid abdominal organ injury in adults e a current perspective. World J Emerg Surg. 2010;5:18.
•• Jacks R, Degiannis E. Endovascular therapy and controversies in the management of vascular trauma. Scand J Surg. 2014;103(2):149–55. A report that highlights the advantages and describes the lack of indications for endovascular treatment.
• Shah AA, Rehman A, Haider AH, Sayani R, Sayyed RH, Ali K, et al. Angiographic embolization for major trauma in a low-middle income healthcare setting—a retrospective review. Int J Surg. 2015;18:34–40. https://doi.org/10.1016/j.ijsu.2015.03.023. The referenced article describes the feasibility of IR and especially angioembolization in severely injured patients in lower-middle income countries.
•• Katsanos K, Sabharwal T, Carrell T, Dourado R, Adam A. Peripheral endografts for the treatment of traumatic arterial injuries. Emerg Radiol. 2009;16(3):175–84. https://doi.org/10.1007/s10140-008-0771-9. The above reference describes the treatment of traumatic arterial injuries by covered stents.
Kalish J. Selective use of endovascular techniques in the management of vascular trauma. Semin Vasc Surg. 2011;23:243–8.
Thorson CM, Ryan ML, Otero CA, et al. Operating room or angiography suite for hemodynamically unstable pelvic fractures? J Trauma Acute Care Surg. 2012;72(2):364–70. discussion 371–2
• Branco BC, DuBose JJ, Zhan LX, Hughes JD, Goshima KR, Rhee P, et al. Trends and outcomes of endovascular therapy in the management of civilian vascular injuries. J Vasc Surg. 2014;60(5):1297–307, 1307. https://doi.org/10.1016/j.jvs.2014.05.028. The referenced article reports that endovascular therapy is associated with improved mortality and lower rates of sepsis.
Johnson Guy E, et al. The role of interventional radiology in trauma. J Radiol Nurs. 33(4):181–7.
•• Matsumoto J, Lohman BD, Morimoto K, Ichinose Y, Hattori T, Taira Y. Damage control interventional radiology (DCIR) in prompt and rapid endovascular strategies in trauma occasions (PRESTO): a new paradigm. Diagn Interv Imaging. 2015;96(7–8):687–91. https://doi.org/10.1016/j.diii.2015.06.001. The above reference describes the evolution of IR in the trauma setting.
Irish JC, Hekkenberg R, Gullane PJ, et al. Penetrating and blunt neck trauma: 10-year review of a Canadian experience. Can J Surg. 1997;40:33–8.
Mulloy J, Flick P, Gold R. Blunt carotid injury: a review. Radiology. 1998;207:571–85.
Parikh AA, Luchette FA, Valente JF, Johnson RC, Anderson GL, Blebea J, et al. Blunt carotid artery injuries. J Am Coll Surg. 1997;185(1):80–6.
Stein DM, Boswell S, Sliker CW, Liu FY, Scalea TM. Blunt cerebrovascular injuries: does treatment always matter? J Trauma. 2009;66(1):132–43. discussion 143-144
McKevitt EC, Kirkpatrick AW, Vertesi L, Granger R, Simons RK. Identifying patients at risk for intracranial and extracranial blunt carotid injuries. Am J Surg. 2002;183(5):566–70.
Munera F, Soto JA, Palacio D, Velez SM, Medina E. Diagnosis of arterial injuries caused by penetrating trauma to the neck: comparison of helical CT angiography and conventional angiography. Radiology. 2000;216:356–62.
Arthurs ZM, Starnes BW. Blunt carotid and vertebral artery injuries. Injury. 2008;39(11):1232–41.
Biffl W, Moore E, Offner P, Brega K, Franciose R, Burch J. Blunt carotid injuries: implications of a new grading scale. J Trauma. 1999;45:845–66.
Moulakakis KG, Mylonas S, Avgerinos E, Kotsis T, Liapis CD. An update of the role of endovascular repair in blunt carotid artery trauma. Eur J Vasc Endovasc Surg. 2010;40(3):312–9.
Jindal G, Fortes M, Miller T, Scalea T, Gandhi D. Endovascular stent repair of traumatic cervical internal carotid artery injuries. J Trauma Acute Care Surg. 2013;75(5):896–903. https://doi.org/10.1097/TA.0b013e3182a686be.
Maras D, Lioupis C, Magoufis G, Tsamopoulos N, Moulakakis K, Andrikopoulos V. Covered stent-graft treatment of traumatic internal carotid artery pseudo-aneurysms: a review. Cardiovasc Intervent Radiol. 2006;29(6):958–68.
Feugier P, Vulliez A, Bina N, Floccard B, Allaouchiche B. Urgent endovascular covered-stent treatment of internal carotid artery injury caused by a gunshot. Eur J Vasc Endovasc Surg. 2007;34(6):663–5.
• Zhao LB, Shi HB, Park S, Lee DG, Shim JH, Lee DH, et al. Acute bleeding in the head and neck: angiographic findings and endovascular management. AJNR Am J Neuroradiol. 2014;35(2):360–6. https://doi.org/10.3174/ajnr.A3761. An article that describes angiographic findings and endovascular treatment for head and neck artery injuries.
Mathis JM, Barr JD, Jungreis CA, Yonas H, Sekhar LN, Vincent D, et al. Temporary balloon test occlusion of the inter- nal carotid artery: experience in 500 cases. Am J Neuroradiol. 1995;16(4):749–54.
Felber S, Henkes H, Weber W, Miloslavski E, Brew S, Kühne D. Treatment of extracranial and intracranial aneurysms and arteriovenous fistulae using stent grafts. Neurosurgery. 2004;55(3):631–8.
Pham MH, Rahme RJ, Arnaout O, Hurley MC, Bernstein RA, Batjer HH, et al. Endovascular stenting of extracranial carotid and vertebral artery dissections: a systematic review of the literature. Neurosurgery. 2011;68(4):856–66. discussion 866
O’Brien D, O’Dell MW, Eversol A. Delayed traumatic cerebral aneurysm after brain injury. Arch Phys Med Rehabil. 1997;78:883–5.
Zhang CW, Xie XD, You C, Mao BY, Wang CH, He M, et al. Endovascular treatment of traumatic pseudoaneurysm presenting as intractable epistaxis. Korean J Radiol. 2010;11(6):603–11.
Buckingham MJ, Crone KR, Ball WS, Tomsick TA, Berger TS, Tew JM Jr. Traumatic intracranial aneurysms in childhood: two cases and a review of the literature. Neurosurgery. 1988;22:398–408.
Dennis J. Minimal vascular injuries. In: Rich N, Mattox K, Hirshberg AM, editors. Vascular trauma. 2nd ed. New York: Elsevier Science (USA); 2004. p. 85–96.
Cohen JE, Gomori JM, Segal R, Spivak A, Margolin E, Sviri G, et al. Results of endovascular treatment of traumatic intracranial aneurysms. Neurosurgery. 2008;63(3):476–85.
Stager V, Gandhi R, Stroman D, Timaran C, Broker H. Traumatic internal carotid artery injury treated with overlapping bare metal stents under intravascular ultrasound guidance. J Vasc Surg. 2011;53(2):483–6.
Li Z, Chang G, Yao C, Guo L, Liu Y, Wang M, et al. Endovascular stenting of extracranial carotid artery aneurysm: a systematic review. Eur J Vasc Endovasc Surg. 2011;42(4):419–26.
Schievink WI. Spontaneous dissection of the carotid and vertebral arteries. N Engl J Med. 2001;344:898–906.
Schittek A. Pseudoaneurysm of the vertebral artery. Tex Heart Inst J. 1999;26:90–5.
Biffl WL, Ray CE, Moore EE, et al. Treatment-related outcomes from blunt cerebrovascular injuries. Ann Surg. 2002;235:699–707.
Atar E, Griton I, Bachar GN, Bartal G, Kluger Y, Belenky A. Embolization of transected vertebral arteries in unstable trauma patients. Emerg Radiol. 2005;11(5):291–4.
Lleva P, Ahluwalia BS, Marks S, Sahni R, Tenner M, Risucci DA, et al. Traumatic and spontaneous carotid and vertebral artery dissection in a level 1 trauma center. J Clin Neurosci. 2012;19:1112–4.
• Cohen JE, Gomori JM, Rajz G, Rosenthal G, El Hassan HA, Moscovici S, et al. Vertebral artery pseudoaneurysms secondary to blunt trauma: endovascular management by means of neurostents and flow diverters. J Clin Neurosci. 2016;32:77–82. https://doi.org/10.1016/j.jocn.2016.03.023. The above reference describes treatment of vertebral artery pseudoaneurysms with the novel flow diverter device.
Fiorella D, Lylyk P, Szikora I, Kelly ME, Albuquerque FC, McDougall CG, et al. Curative cerebrovascular reconstruction with the pipeline embolization device: the emergence of definitive endovascular therapy for intracranial aneurysms. J Neurointerv Surg. 2009;1:56–65.
Fulton JO, De Groot MK, Von Oppell UO. Stab wounds of the innominate artery. Ann Thorac Surg. 1996;61(3):851–3.
Du Toit DF, Odendaal W, Lambrechts A, Warren BL. Surgical and endovascular management of penetrating innominate artery injuries. Eur J Vasc Endovasc Surg. 2008;36(1):56–62.
Mauney M, Cassada C, Kaza K, Long SM, Kern JA. Management of innominate artery injury in the setting of bovine arch anomaly. Ann Thorac Surg. 2001;72:2134e6.
Shalhub S, Starnes BW, Tran NT. Endovascular treatment of axillosubclavian arterial transection in patients with blunt traumatic injury. J Vasc Surg. 2011;53:1141–4. 1144
Demetriades D, Asensio JA. Subclavian and axillary vascular injuries. Surg Clin North Am. 2001;81:1357–73.
Sturm JT, Cicero JJ. The clinical diagnosis of ruptured subclavian artery following blunt thoracic trauma. Ann Emerg Med. 1983;12:17–9.
Buscaglia LC, Walsh JC, Wilson JD, Matolo NM. Surgical management of subclavian artery injury. Am J Surg. 1987;154:88–92.
Demetriades D, Chahwan S, Gomez H, Peng R, Velmahos G, Murray J, et al. Penetrating injuries to the subclavian and axillary vessels. J Am Coll Surg. 1999;188:290–5.
Carrick MM, Morrison CA, Pham HQ, Norman MA, Marvin B, Lee J, et al. Modern management of traumatic subclavian artery injuries: a single institution’s experience in the evolution of endovascular repair. Am J Surg. 2010;199(January (1)):28–34.
Xenos ES, Freeman M, Stevens S, Cassada D, Pacanowski J, Goldman M. Covered stents for injuries of subclavian and axillary arteries. J Vasc Surg. 2003;38:451–4.
• Matsagkas M, Kouvelos G, Peroulis M, Xanthopoulos D, Bouris V, Arnaoutoglou E. Endovascular repair of blunt axillo-subclavian arterial injuries as the first line treatment. Injury. 2016;47(5):1051–6. https://doi.org/10.1016/j.injury.2016.02.003. This article reports endovascular treamtment outcomes of blunt axillo-subclavian arterial injuries in the emergent setting.
Sanders C, Cipolla J, Stehly C, Hoey B. Blunt breast trauma: is there a standard of care? Am Surg. 2011;77:1066–9.
Hagiwara A, Yanagawa Y, Kaneko N, Takasu A, Hatanaka K, Sakamoto T, et al. Indications for transcatheter arterial embolization in persistent hemothorax caused by blunt trauma. J Trauma. 2008;65:589–94.
Teixeira PG, Inaba K, Barmparas G, Georgiou C, Toms C, Noguchi TT, et al. Blunt thoracic aortic injuries: an autopsy study. J Trauma. 2011;70:197–202.
Urgnani F, Lerut P, Da Rocha M, Adriani D, Leon F, Riambau V. Endovascular treatment of acute traumatic thoracic aortic injuries: a retrospective analysis of 20 cases. J Thorac Cardiovasc Surg. 2009;138:1129–38.
Crass J, Cohen A, Motta A, Tomashefski J, Wiesen E. A proposed new mechanism of traumatic aortic rupture: the osseous pinch. Radiology. 1990;176:645–9.
Pacini D, Angeli E, Fattori R, Lovato L, Rocchi G, di Marco L, et al. Traumatic rupture of the thoracic aorta: ten years of delayed management. J Thorac Cardiovasc Surg. 2005;129(4):880–4.
Lee WA, Matsumura JS, Mitchell RS, Farber MA, Greenberg RK, Azizzadeh A, et al. Endovascular repair of traumatic thoracic aortic injury: clinical practice guidelines of the Society for Vascular Surgery. J Vasc Surg. 2011;53:187–92.
Di Eusanio M, Folesani G, Berretta P, Petridis FD, Pantaleo A, Russo V, et al. Delayed management of blunt traumatic aortic injury: open surgical versus endovascular repair. Ann Thorac Surg. 2013;95(5):1591–7.
Kokotsakis J, Kaskarelis I, Misthos P, Athanasiou T, Kanakakis K, Athanasiou C, et al. Endovascular versus open re- pair for blunt thoracic aortic injury: short-term results. Ann Thorac Surg. 2007;84:1965–70.
Hoornweg LL, Dinkelman MK, Gos- lings JC, et al. Endovascular management of traumatic ruptures of the thoracic aorta: a retrospective multi- center analysis of 28 cases in the Netherlands. J Vasc Surg. 2006;43:1096–102.
•• Khoynezhad A, Donayre CE, Azizzadeh A, White R. RESCUE investigators. One-year results of thoracic endovascular aortic repair for blunt thoracic aortic injury (RESCUE trial). J Thorac Cardiovasc Surg. 2015;149(1):155–61.e4. https://doi.org/10.1016/j.jtcvs.2014.09.026. The above reference reports one year outcomes of endovascular treatment of blunt thoracic aortic injury in 50 patients.
•• Spiliotopoulos K, Kokotsakis J, Argiriou M, Dedeilias P, Farsaris D, Diamantis T, et al. Endovascular repair for blunt thoracic aortic injury: 11-year outcomes and postoperative surveillance experience. J Thorac Cardiovasc Surg. 2014;148(6):2956–61. https://doi.org/10.1016/j.jtcvs.2014.08.019. This article highlights midterm outcomes of TEVAR in patients with BTAI.
Miller LE. Potential long-term complications of endovascular stent grafting for blunt thoracic aortic injury. ScientificWorldJournal. 2012;2012:897489.
• Rimon U, Shinfeld A, Gayer G. Traumatic injury of the thoracic aorta treated with stent-graft: is long-term ct angiography follow-up justified? Clin Radiol. 2014;69:207–10. https://doi.org/10.1016/j.crad.2013.12.013. The referenced article investigates the need for annual CT surveillance in patients with traumatic injury of the thoracic aorta treated with a stent-graft.
Dutton RP, Lefering R, Lynn M. Database predictors of transfusion and mortality. J Trauma. 2006;60:S70–7.
• Ierardi AM, Duka E, Lucchina N, Floridi C, De Martino A, Donat D, et al. The role of interventional radiology in abdominopelvic trauma. Br J Radiol. 2016;89(1061):20150866. https://doi.org/10.1259/bjr.20150866. The above reference describes the feasibility of arterial embolization for hemorrhage control in abdominopelvic injuries.
Ben-Menachem Y, Coldwell DM, Young JW, Burgess AR. Hemorrhage associated with pelvic fractures: causes, diagnosis, and emergent management. AJR Am J Roentgenol. 1991;157:1005–14.
Agolini SF, Shah K, Jaffe J, Newcomb J, Rhodes M, Reed JF III. Arterial embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage. J Trauma. 1997;43:395–9.
• Marzi I, Lustenberger T. Management of bleeding pelvic fractures. Scand J Surg. 2014;103(2):104–11. This article proposes a treatment algorithm for the management of bleeding pelvic fractures.
• Tung CC, Yu JF, Lan SJ. Predictability of successful trans-arterial embolization in pelvic fracture bleeding based on patient initial presentation. Am J Emerg Med. 2017; https://doi.org/10.1016/j.ajem.2017.12.044. The above reference highlights the factors that predict a successful transarterial embolization.
Aygün A, Karaca Y, Ayan E, Suha T, Dinç H. Trauma-associated bleeding from the bilateral internal iliac arteries resolved using angiographic embolization. Ulus Travma Acil Cerrahi Derg. 2013;19(6):567–9.
Darmanis S, Lewis A, Mansoor A, Bircher M. Corona mortis: an anatomical study with clinical implications in approaches to the pelvis and acetabulum. Clin Anat. 2007;20:433–9.
Roy-Choudhury SH, Gallacher DJ, Pilmer J, Rankin S, Fowler G, Steers J, et al. Relative threshold of detection of active arterial bleeding: in vitro comparison of MDCT and digital subtraction angiography. AJR Am J Roentgenol. 2007;189:W238–46.
• Johnson GE, Sandstrom CK, Kogut MJ, Ingraham CR, Stratil PG, Valji K, et al. Frequency of external iliac artery branch injury in blunt trauma: improved detection with selective external iliac angiography. J Vasc Interv Radiol. 2013;24(3):363–9. https://doi.org/10.1016/j.jvir.2012.12.006. This article highlights the importance of selective angiography to detect an external iliac artery branch injury.
Schmal H, Markmiller M, Mehlhorn AT, et al. Epidemiology and outcome of complex pelvic injury. Acta Orthop Belg. 2005;71:41.
Morrison JJ, Percival TJ, Markov NP, Villamaria C, Scott DJ, Saches KA, et al. Aortic balloon occlusion is effective in controlling pelvic hemorrhage. J Surg Res. 2012;177(2):341–7.
Hughes CW. Use of an intra-aortic balloon catheter tamponade for controlling intra-abdominal hemorrhage in man. Surgery. 1954;36:65–8.
Perkins ZB, Lendrum RA, Brohi K. Resuscitative endovascular balloon occlusion of the aorta: promise, practice, and progress? Curr Opin Crit Care. 2016;22(6):563–71.
Martinelli T, Thony F, Declety P, et al. Intra-aortic balloon occlusion to salvage patients with life-threatening hemorrhagic shocks from pelvic fractures. J Trauma Acute Care Surg. 2010;68:942–8.
• Teeter WA, Matsumoto J, Idoguchi K, et al. Smaller introducer sheaths for REBOA may be associated with fewer complications. J Trauma Acute Care Surg. 2016;81(6):1039–45. The referenced article reports that 7Fr REBOA catheters can be efficient and are associated with fewer complications.
Matsumura Y, Matsumoto J, Kondo H, Idoguchi K, Ishida T, Kon Y, et al. Fewer REBOA complications with smaller devices and partial occlusion: evidence from a multicentre registry in Japan. Emerg Med J. 2017;34(12):793–9. https://doi.org/10.1136/emermed-2016-206383.
Linnebur M, Inaba K, Haltmeier T, Rasmussen TE, Smith J, Mendelsberg R, et al. Emergent nonimage guided REBOA catheter placement: a cadaver-based study. J Trauma Acute Care Surg. 2016;81:453–7. https://doi.org/10.1097/TA.0000000000001106.
Guliani S, Amendola M, Strife B, Morano G, Elbich J, Albuquerque F, et al. Central aortic wire confirmation for emergent endovascular procedures: as fast as surgeon-performed ultrasound. J Trauma Acute Care Surg. 2015;79(4):549–54. https://doi.org/10.1097/TA.0000000000000818.
Bogert JN, Patel BM, Johnson DJ. Ultrasound optimization for resuscitative endovascular balloon occlusion of the aorta. J Trauma Acute Care Surg. 2017;82(1):204–7. https://doi.org/10.1097/TA.0000000000001293.
Russo R, Neff LP, Johnson MA, Williams TK. Emerging endovascular therapies for non-compressible torso hemorrhage. Shock. 2016;46(3 Suppl 1):12–9. https://doi.org/10.1097/SHK.0000000000000641.
• Johnson MA, Neff LP, Williams TK, DuBose JJ, EVAC Study Group. Partial resuscitative balloon occlusion of the aorta (P-REBOA): clinical technique and rationale. J Trauma Acute Care Surg. 2016;81(5 Suppl 2 Proceedings of the 2015 Military Health System Research Symposium):S133–7. This article describes the technique of partial REBOA (P-REBOA).
Sadek S, Lockey DJ, Lendrum RA, Perkins Z, Price J, Davies GE. Resuscitative endovascular balloon occlusion of the aorta (REBOA) in the pre-hospital setting: an additional resuscitation option for uncontrolled catastrophic haemorrhage. Resuscitation. 2016;107:135–8.
Maynar M, Baro M, Qian Z, López-Benitez R, Ragheb D, Llorens R, et al. Endovascular repair of brachial artery transection associated with trauma. J Trauma. 2004;56:1336–41.
Lin PH, Koffron AJ, Guske PJ, Lujan HJ, Heilizer TJ, Yario RF, et al. Penetrating injuries of the subclavian artery. Am J Surg. 2003;185:580–4.
Danetz JS, Cassano AD, Stoner MC, Ivatury RR, Levy MM. Feasibility of endovascular repair in penetrating axillosubclavian injuries: a retrospective review. J Vasc Surg. 2005;41:246–54.
Chung HH, Cha SH, Cho SB, Kim JH, Lee SH, Shin JS, et al. Traumatic axillary artery dissection with radial artery embolism. Cardiovasc Intervent Radiol. 2006;29:294–7.
White R, Krajcer Z, Johnson M, Williams D, Bacharach M, O’Malley E. Results of a multicenter trial for the treatment of traumatic vascular injury with a covered stent. J Trauma. 2006;60:1189–95.
Piffaretti G, Tozzi M, Lomazzi C, Rivolta N, Caronno R, Laganà D, et al. Endovascular treatment for traumatic injuries of the peripheral arteries following blunt trauma. Injury. 2007;38(9):1091–7.
Fox N, Rajani RR, Bokhari F, Chiu WC, Kerwin A, Seamon MJ, et al. Evaluation and management of penetrating lower extremity arterial trauma: an eastern Association for the Surgery of trauma practice management guideline. J Trauma Acute Care Surg. 2012;73:S315–20.
Chong VE, Lee WS, Miraflor E, Victorino GP. Applying peripheral vascular injury guidelines to penetrating trauma. J Surg Res. 2014;190(1):300–4. https://doi.org/10.1016/j.jss.2014.03.035.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflicts of interest relevant to this manuscript.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Damage Control Beyond The Abdomen
Rights and permissions
About this article

Cite this article
Spiliopoulos, S., Vasiniotis Kamarinos, N. & Brountzos, E. Interventional Angiography Damage Control. Curr Trauma Rep 4, 187–198 (2018). https://doi.org/10.1007/s40719-018-0135-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40719-018-0135-1