
Abstract
Problem presentation in problem-based learning can include the use of videos and interactive virtual patients. This review scopes the literature for this variation and what benefits or pitfalls there may be to their use. Themes indicate that videos and virtual patients may better prepare students for future difficult clinical interactions, while also increasing authenticity and memorability of cases. Findings are more inconsistent in determining whether they lead to clear knowledge or critical thinking gains. Despite inconsistent data, in an age where the use of technology is inevitable, the findings of this scoping review can inform future practice and guide innovation.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Problem-based learning (PBL), although now widely adopted at medical schools across the country and world, had its beginnings roughly 50 years ago [1]. Born out of the frustrations of a “boring” traditional lecture-based curriculum at McMaster University in Canada, PBL was a novel idea that encouraged students to engage in active learning [1]. Servant-Miklos, in her research of the historical beginnings of PBL, wrote that the principles laid out by its founder included small-group learning, a focus on patient-centered problems, limited lecture-based teachings, and overall flexibility in structure [1]. Barrows further defined PBL as having five major components that included learning that was (1) student-centered, (2) occurred in small student groups, (3) utilized teachers that were facilitators or guides, (4) used problems to provide focus and stimulus for learning and for the development of clinical problem-solving skills, and (5) emphasized self-directed learning to gain new information [2]. The historical tenants of PBL encourage the question that guides this review: how has technology mediated the ways in which PBL is conducted?
In more recent years, the use of technology in medical education has become essential given the need for distance learning (for instance, during stay-at-home directives), the increasing quality of online third party materials, and the amount of knowledge that has increased exponentially. Some computer-based interventions in medical school curricula have included the use of virtual small group sessions, online pre-recorded lectures and other materials, use of video to supplement patient simulations, and the use of “virtual patients” (VPs) to encourage decision-making through simulating a real patient-encounter [3]. As Ellaway writes, “there has been a proliferation of personal digital devices in recent years, to the point that (digital) technologies have become a near-ubiquitous presence in the training of tomorrow’s doctors” [4].
Technology can be used within medical education as a way to mediate the learning process. Thus, a term such as “technology enhanced learning” highlights the importance of technology being seen as a means to an end, not the end itself [4]. Ellaway writes of the concept of “blended learning,” stating that technology mediation is “entangled with other types of mediation” and that there is some evidence to suggest that a blended approach leads to better learning outcomes [4].
Technology mediation in PBL has not been extensively reviewed, though technology certainly has been “blended” into PBL in different ways. This paper aims to summarize through a scoping review how video and VPs have been used in the presentation of the problem (or “trigger”) in PBL. As Charlin et al. wrote, problem presentation is one of 10 dimensions through which the execution of PBL can vary from practice to practice [5]. Therefore, in a time where technology is heavily used, this review aims to better clarify another means in which it facilitates PBL in undergraduate medical education. It is guided by the overarching question: how are videos and VPs being used as triggers in PBL cases designed for undergraduate medical students? A secondary question is what are some of the benefits and outcomes of using these triggers, if any, within both quantitative and qualitative domains? Lastly, in the hopes that this review will inform future practice, what are some challenges to consider in the use of video or VP triggers in PBL?
Methods
Four steps were taken to conduct this scoping review, as outlined by Arksey and O’Malley’s and Levac et al.’s protocols: identifying the research question, identification of relevant studies, study selection, and chart, collate, and summarize report results [6, 7].
Identification of Relevant Studies
A research team of three qualified and experienced individuals reviewed potential databases to query, and selected the following based on database reputation and content relevant to medical education: PubMed, PsycINFO, CINAHL, MEDLINE, and ERIC. Supplementary Table 1 includes detailed search terms for each database and the number of results that were yielded. Most were a variation of (“problem-based learning” AND “video”) or (“problem-based learning” AND “virtual patients”). Consultation with a health information scientist confirmed the use of our search terms and database selection as relevant to the scope of our study.
Study Selection
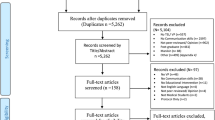
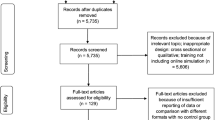
Figure 1 details the study selection process. After the databases were initially searched, titles and abstracts were collated into a data collection sheet. This was then given to each of the three authors who served as screeners and reviewers (NN, GN, RF). The abstracts were screened independently using the same inclusion and exclusion criteria. After studies were selected through this initial abstract screen, full-text versions of the articles were then obtained and again screened independently by the same authors, using the same inclusion and exclusion criteria.

Identifying relevant studies
Inclusion and Exclusion Criteria
Studies selected for this scoping review were research studies only, with an included methodology section. The population studied was deemed appropriate only if it included medical students in the undergraduate phase of their training. All articles that encompassed graduate medical education were excluded. In review of the methodology, only articles that included a traditional definition of PBL, including the five major components outlined by Barrows, were deemed appropriate [2]. Lastly, only articles after the year 2000 were considered.
A “snowball” technique was also used, where the references of each full-text article that passed the initial screen were hand searched for relevant studies to be included in the review based on their title, before assessing whether they met inclusion and exclusion criteria [8, 9].
Charting the Data
After the study selection process was completed, two authors (NN and GN) read each article in full and used a data collection sheet to chart data that was relevant to each article, including authors, type of study (quantitative or qualitative), sample size, year of undergraduate medical education, study location, types of comparisons that were made, and main findings.
Collating, Summarizing, and Reporting Results
Two authors (NN and GN) read the articles in full and performed a thematic analysis, in accordance with methodologies outlined by Pham et al. [10]. The identification of themes was guided by the process discussed by Braun and Clarke [11]. Through adjudication sessions, both authors (NN and GN) met to discuss and collate their independently identified categories into key overarching themes, before summarizing and reporting results.
Results
Description of Included Studies
Table 1 below summarizes the main comparisons made by each article. Table 2 gives details about how PBL cases were accessed by students. Some variations included PBL cases conducted synchronously via video conferencing or in-person, or asynchronously using web-based applications. Table 3 outlines major characteristics of each of the included studies.
Key Themes
Using Videos and VPs in PBL Can Help Mediate the Difficulty of Future Clinical Encounters
The type of PBL cases that utilized VPs or video problem presentation spanned multiple organ systems and basic science topics. However, some of the cases helped better prepare students for what they perceive as difficult real-life patient interactions, such as those involving patients with a mental health diagnosis or newborns with a variety of disorders [16, 17, 19, 28, 29]. Kamin et al. chose to focus on a pediatric case of newborn altered mental status for their third-year students, indicating that students have limited opportunities to work with a variety of pediatric patients depending on the season [19]. Therefore, they may not have the opportunity to gain sufficient knowledge and skills in areas such as “child abuse, genetic disease, and adolescents during a pediatrics clerkship,” thus making the argument for the utility of video-cases as an adjunct to real-life clinical exposure [19]. Lajoie et al. also used cases to break “bad news” to patients virtually, mentioning how doing so could pave the way for future telemedicine interactions with patients [20].
The Effect of Video and VPs on Deep or Critical Thinking Is Debated
There is conflicting evidence of whether VPs or video problem presentation in PBL can evoke critical thinking skills. In a randomized crossover study of video-based versus text/paper-based PBL, video cases led to significantly lower levels of deep thinking, especially when students were engaging in problem exploration [12]. Woodham et al. noted similar findings [30]. Conversely, multiple studies have found higher levels of critical thinking with VPs in PBL [19, 20, 29].
Several of the articles that used video problem presentation (whether within a VP module or not) indicated that clinical reasoning was enhanced [13, 17, 29]. Kleinert et al. showed that students summarized their diagnosis and identified an appropriate therapy better after exposure to VP cases [22]. However, Raupach et al. found no difference in clinical reasoning in their experimental asynchronous VP PBL group [25].
Videos Might Increase Cognitive Load of Learners
Of note, one disadvantage to varying forms of problem presentation is related to cognitive load theory. In a study by Basu Roy and McMahon, critical thinking was suppressed among students experiencing video problem presentation [12]. This was thought to be due, in part, to the cognitive load required to work through complex pathophysiology learning objectives alongside the use of video. They state that the use of video may require more working memory, thus increasing cognitive load and potentially less capacity for critical thinking [12]. However, in a different study, Kamin et al. discussed “dual coding theory,” which states that “the use of visualization enhances learning and recall” [19]. Dual coding theory would then support that VPs or videos might actually reduce cognitive load for learners.
Virtual Patients in PBL Enhance Learning Through Non-linear Decision-making
In a paper case, because the information is presented in a linear fashion, students are not able to manipulate data or make decisions in the evaluation of a patient. However, several studies note the unique advantage of cases becoming “branched” when virtual patient modules are utilized [21,22,23]. The use of decision-PBL branched virtual cases allowed students to “manipulate learning to a higher level,” thus uniquely distinguishing themselves from paper cases [21].
Videos Augment Authenticity and Memorability
One of the ways students responded positively to the use of video in PBL was by valuing the ability of videos to increase authenticity, therefore making the cases more memorable and increasing motivation [14, 17,18,19, 26, 29]. One study in particular suggested that videos enabled students to create realistic mental pictures of patients [14].
Novice Learners Were More Likely to Prefer Paper Cases Compared to Cases with Video or VPs
Two studies found that first- and second-year students preferred traditional paper-based cases compared to videos [15, 30]. Woodham et al. found that second-year transitional students claimed videos slowed the pace of PBL [30]. Similarly, Ghanchi et al. found that first-year students thought paper cases were more effective, “interesting, engaging and helpful in enhancing group discussion, dynamics and communication skills” [15]. Other studies looking at more advanced students past their second year preferred the use of video [17,18,19]. Similarly, two studies found that third-year students preferred VPs [22, 27].
Effect of Video or VP Triggers on Knowledge Recall
In some studies, the use of video or VP triggers in PBL increased knowledge recall, and in others it did not. Ikegami et al. found that recall was no different in their video-group at six months [17]. Other studies looking at VP use reported similar findings [25, 27]. Conversely, others found that there were increases in knowledge retention in students using VPs [22, 24].
Discussion
This scoping review of video and VP problem presentation in PBL noted differences in the way PBLs were conducted: synchronous video-conferenced or in-person groups, and asynchronous online modules, as outlined in Table 2. Regardless of the format, the themes among the studies related to the nature of the PBL cases, the cognitive effects of these triggers, and students’ general acceptance and impressions of the process.
The ability of videos and VPs to augment the intimidating nature of difficult clinical scenarios was highlighted by the first theme. This may be a way that these forms of technology can facilitate learning. Medical teachers might consider this format of PBL if they are looking to specifically prepare students for difficult future clinical encounters, perhaps closer to the start of their clinical experiences. Further, the addition of patient videos in PBL may mimic a telemedicine interface that is becoming more widely accepted in medicine and potentially important for future doctors to have exposure to in medical school.
Our review noted that using technology in PBL may or may not have a negative effect on deep or critical thinking. As Ellaway points out, “teachers teach and learners learn; it is how they do these things (and what follows) that is changed by their use of technology” [4]. Studies that found negative cognitive effects with video or VP forms of PBL may have incorporated this technology poorly, or may have done so with the wrong learners. Early in their medical education curriculum, novice learners may not have the working memory necessary to extract information from VPs or video, which may also explain the findings pertaining to the negative effects of cognitive load and the preference differential between novice and advanced learners noted in some of the studies. Thus, future research comparing video or VP use in PBL and whether they strengthen critical thinking or clinical reasoning, as well as programs looking to adopt one of these forms of problem presentation, should take this into consideration. Programs might also consider using more of a “blended” approach that has both text and video or VP components, instead of exclusively one or the other.
Future research interested in studying specific outcomes such as knowledge acquisition and retention should also consider measuring outcomes directed at the benefits that video or VPs have to offer [24]. For example, the VP cases that offered branched decision-making cases might then test learners based on the ability to make these types of decisions.
Although there is not enough empirical evidence to support whether the use of videos or VPs leads to better outcomes for learners (such as knowledge acquisition, retention, and clinical decision-making), studies did provide evidence for increased authenticity of cases. This may be particularly appealing to adult learners, especially through an andragogical lens that states real and simulated experiences appeal to adults [32]. Medical curricula interested in maximizing patient-centered learning might also benefit from the authenticity that videos and VPs can provide in PBL cases. A visual, authentic patient-centered approach could also aid in integrating a patient’s presenting illness script to underlying basic science concepts. Moreover, if institutions are conducting PBL asynchronously or synchronously over a remote conferencing medium, the need to augment authenticity as much as possible may be paramount.
Conclusion
PBL has been widely adopted in medical education since its birth in the 1960s. How PBL is conducted, however, is not universal from institution to institution. The way in which problems are presented to students is one of the ways in which PBL can vary. Technology, in its ability to mediate learning, has been blended with more traditional ways to present problems in PBL through the use of VPs or video. Future studies and more systematic approaches to review such as meta-analyses may be needed to better understand whether videos and VPs in PBL lead to more or less critical thinking, clinical reasoning, or long-term retention. Doing so may also limit multiple studies conducted at the same location from contributing to bias, which this broad-based scoping review was unable to accomplish. Regardless, this scoping review supports that videos and VPs in PBL are worth pursuing to help increase the authenticity of cases and better prepare learners for difficult clinical experiences.
Data Availability
All data generated or analyzed during this study are included in this published article (and its supplementary information files).
References
Servant-Miklos VF. Fifty years on: a retrospective on the world’s first problem-based learning programme at McMaster University Medical School. Health Profess Educ. 2019;5(1):3–12.
Barrows HS. Problem-based learning in medicine and beyond: a brief overview. New Dir Teach Learn. 1996;1996(68):3–12.
Berman NB, Durning SJ, Fischer MR, Huwendiek S, Triola MM. The role for virtual patients in the future of medical education. Acad Med. 2016;91(9):1217–22.
Ellaway RH. Technology-enhanced learning. In: Swanwick T, Forrest K, O’Brien BC, editors. Understanding medical education: evidence, theory, and practice. Hoboken: Wiley-Blackwell; 2019. p. 139–49.
Charlin B, Mann K, Hansen PB. The many faces of problem-based learning: a framework for understanding and comparison. Med Teach. 1998;20(4):323–30.
Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32.
Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implement Sci. 2010;5(1):69.
Hepplestone S, Holden G, Irwin B, Parkin HJ, Thorpe L. Using technology to encourage student engagement with feedback: a literature review. Res Learn Technol. 2011;19(2).
Jaskiewicz W, Tulenko K. Increasing community health worker productivity and effectiveness: a review of the influence of the work environment. Hum Resour Health. 2012;10(1):38.
Pham MT, Rajić A, Greig JD, Sargeant JM, Papadopoulos A, McEwen SA. A scoping review of scoping reviews: advancing the approach and enhancing the consistency. Res Synth Methods. 2014;5(4):371–85.
Clarke V, Braun V. Using thematic analysis in counselling and psychotherapy research: a critical reflection. Couns Psychother Res. 2018;18(2):107–10.
Basu Roy R, McMahon GT. Video-based cases disrupt deep critical thinking in problem-based learning. Med Educ. 2012;46(4):426–35.
Chan LK, Patil NG, Chen JY, Lam JC, Lau CS, Ip MS. Advantages of video trigger in problem-based learning. Med Teach. 2010;32(9):760–5.
De Leng BA, Dolmans DH, Van de Wiel MW, Muijtjens A, Van Der Vleuten CP. How video cases should be used as authentic stimuli in problem-based medical education. Med Educ. 2007;41(2):181–8.
Ghanchi NK, Khan S, Afridi A, Sajid S, Afzal S, Ahmed I, et al. Video or paper for delivery of problem-based learning cases? Med Educ. 2013;47(11):1131.
Hassoulas A, Forty E, Hoskins M, Walters J, Riley S. A case-based medical curriculum for the 21st century: the use of innovative approaches in designing and developing a case on mental health. Med Teach. 2017;39(5):505–11.
Ikegami A, Ohira Y, Uehara T, Noda K, Suzuki S, Shikino K, et al. Problem-based learning using patient-simulated videos showing daily life for a comprehensive clinical approach. Int J Med Educ. 2017;8:70–6.
Kamin C, Deterding R, Lowry M. Student’s perceptions of a virtual PBL experience. Acad Med. 2002;77(11):1161–2.
Kamin C, O’Sullivan P, Deterding R, Younger M. A comparison of critical thinking in groups of third-year medical students in text, video, and virtual PBL case modalities. Acad Med. 2003;78(2):204–11.
Lajoie SP, Hmelo-Silver CE, Wiseman JG, Chan LK, Lu J, Khurana C, et al. Using online digital tools and video to support international problem-based learning. Interdiscip J Problem-Based Learning. 2014;8(2):60–75.
Ellaway RH, Poulton T, Jivram T. Decision PBL: a 4-year retrospective case study of the use of virtual patients in problem-based learning. Med Teach. 2015;37(10):926–34.
Kleinert R, Heiermann N, Plum PS, Wahba R, Chang D-H, Maus M, et al. Web-based immersive virtual patient simulators: positive effect on clinical reasoning in medical education. J Med Internet Res. 2015;17(11):e263.
Poulton T, Conradi E, Kavia S, Round J, Hilton S. The replacement of ‘paper’ cases by interactive online virtual patients in problem-based learning. Med Teach. 2009;31(8):752–8.
Poulton T, Ellaway RH, Round J, Jivram T, Kavia S, Hilton S. Exploring the efficacy of replacing linear paper-based patient cases in problem-based learning with dynamic Web-based virtual patients: randomized controlled trial. J Med Internet Res. 2014;16(11):e240.
Raupach T, Muenscher C, Anders S, Steinbach R, Pukrop T, Hege I, et al. Web-based collaborative training of clinical reasoning: a randomized trial. Med Teach. 2009;31(9):e431–e7.
Smith SR, Cookson J, Mckendree J, Harden RM. Patient-centred learning—back to the future. Med Teach. 2007;29(1):33–7.
Sobocan M, Turk N, Dinevski D, Hojs R, Pecovnik Balon B. Problem-based learning in internal medicine: virtual patients or paper-based problems? Intern Med J. 2017;47(1):99–103.
Lee MT, Jacobs JL, Kamin CS. Video-enhanced problem-based learning to teach clinical skills. Med Educ. 2006;40(5):473–4.
McLean M, Brazil V, Johnson P. How we “breathed life” into problem-based learning cases using a mobile application. Med Teach. 2014;36(10):849–52.
Woodham LA, Ellaway RH, Round J, Vaughan S, Poulton T, Zary N. Medical student and tutor perceptions of video versus text in an interactive online virtual patient for problem-based learning: a pilot study. J Med Internet Res. 2015;17(6):e151.
Yoon BY, Choi I, Choi S, Kim T-H, Roh H, Rhee BD, et al. Using standardized patients versus video cases for representing clinical problems in problem-based learning. Korean J Med Educ. 2016;28(2):169–78.
Knowles MS, Holton III EF, Swanson RA. The adult learner: the definitive classic in adult education and human resource development. Routledge; 2014.
Daudt HM, van Mossel C, Scott SJ. Enhancing the scoping study methodology: a large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med Res Methodol. 2013;13(1):48.
Code Availability
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 14 kb)
Glossary
- Scoping review
-
a research approach that aims to “map the literature on a particular topic or research area and provide an opportunity to identify key concepts; gaps in the research; and types and sources of evidence to inform practice, policymaking, and research” [33].
- Triggers
-
means of problem presentation within problem-based learning [13].
- Virtual patients (VPs)
-
“interactive computer simulation of real-life clinical scenarios for the purpose of healthcare and medical training, education, or assessment” [21].
Rights and permissions
About this article

Cite this article
Noverati, N., R. Naro, G., J. Fischer, R. et al. Using Video and Virtual Patients in Problem-Based Learning: a Scoping Review. Med.Sci.Educ. 30, 1685–1691 (2020). https://doi.org/10.1007/s40670-020-01108-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40670-020-01108-7