
Abstract
Background
The dialysis dose (Kt/V) and normalized protein catabolic rate (PCRn) are the most useful indices derived from the urea kinetic model (UKM) in haemodialysis (HD) patients. The kidney urea clearance (Kru) is another important UKM parameter which plays a key role in the prescription of incremental HD. Ideally, the three kinetic parameters should be assessed using the complex software Solute Solver based on the double pool UKM. In the clinical setting, however, the three indices are estimated with simplified formulae. The recently introduced software SPEEDY assembles the aforementioned equations in a plain spreadsheet, to produce quite accurate results of Kru, Kt/V and PCRn. Unfortunately, specific equations to compute Kt/V and PCRn for patients on a once-weekly HD regimen (1HD/wk) were not available at the time SPEEDY was built-up. We devised a new version of SPEEDY (SPEEDY-1) and an even simpler variant (SPEEDY-1S), using two recently published equations for the 1HD/wk schedule . Moreover, we also added a published equation to estimate the equivalent renal clearance (EKR) normalized to urea distribution volume (V) of 35 L (EKR35) from Kru and Kt/V . Aim of the present study was to compare the results obtained using the new methods (SPEEDY-1 and SPEEDY-1S) with those provided by the reference method Solute Solver.
Subjects and methods
One hundred historical patients being treated with the once-weekly HD regimen were enrolled. A total of 500 HD sessions associated to the availability of monthly UKM studies were analysed in order to obtain Kru, single pool Kt/V (spKt/V), equilibrated Kt/V (eKt/V), V, PCRn and EKR35 values by using Solute Solver, SPEEDY-1 and SPEEDY-1S.
Results
When comparing the paired values of the above UKM parameters, as computed by SPEEDY-1 and Solute Solver, respectively, all differences but one were statistically significant at the one-sample t-test; however, the agreement limits at Bland–Altman analysis showed that all differences were negligible. When comparing the paired values of the above UKM parameters, as computed by SPEEDY-1S and Solute Solver, respectively, all differences were statistically significant; however, the agreement limits showed that the differences were negligible as far as Kru, spKt/V and eKt/V are concerned, though much larger regarding V, PCRn and EKR35.
Conclusions
We implemented SPEEDY with a new version specific for the once-weekly HD regimen, SPEEDY-1. It provides accurate results and is presently the best alternative to Solute Solver. Using SPEEDY-1S led to a larger difference in PCRn and EKR35, which could be acceptable for clinical practice if SPEEDY-1 is not available.
Graphic abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The dialysis dose (Kt/V) and the normalized protein catabolic rate (PCRn) are the most useful indices derived from the urea kinetic model (UKM) in haemodialysis (HD) patients [1]. The kidney urea clearance (Kru) is another important UKM parameter which plays a key role in the prescription of incremental HD, starting with a low dialysis dose and a low frequency to be progressively increased to compensate for any subsequent loss in Kru [2]. Ideally, the three kinetic parameters should be assessed using a complex software based on the double pool UKM, as is, for instance, Solute Solver [3], the web-based software recommended by the 2015 KDOQI clinical practice guidelines for HD adequacy [4]. In the routine clinical setting, however, the three indices are currently being estimated with simple formulae, derived from UKM-based studies [5,6,7,8,9,10]. Recently, a software called SPEEDY has been introduced; it assembles the aforementioned simplified equations in a plain spreadsheet, to automatically produce quite accurate results of Kru, Kt/V and PCRn from a simple input data set [11]. SPEEDY is freely available at www.era-edta.org/en/eudial/ (then click on ongoing projects). Unfortunately, at the time SPEEDY was built, the available equations for estimating Kru and Kt/V were not specifically devised for patients on the once-weekly HD (1HD/wk) regimen, so that it may not be correct to use these equations with the latter HD regimen. Moreover, an equation estimating PCRn in the once-weekly HD was lacking. In order to fill these gaps, very recently Casino et al. introduced specific equations for Kt/V [12] and PCRn [13].
We devised a new version of SPEEDY (SPEEDY-1) and an even simpler variant (SPEEDY-1S), assembling the above equations to assess Kt/V and PCRn in the once-weekly HD regimen. Moreover, in these versions, we also added a published equation that estimates the equivalent renal clearance (EKR) from Kru, the urea distribution volume (V) and the equilibrated Kt/V (eKt/V) [14].
Aim of the present study was to compare the results obtained using the new methods (SPEEDY-1 and SPEEDY-1S) with those provided by the reference method Solute Solver.
Subjects and methods
Subjects
One hundred historical patients being treated with the once-weekly HD regimen at the Dialysis Centres of San Pedro de Alcantara Hospital and Virgen del Puerto Hospital, Cáceres, Spain, were enrolled into the study. All patients had given verbal and written informed consent to the choice of HD as first dialysis modality of renal replacement therapy; furthermore, they had accepted to start with the 1HD/wk regimen. Criteria for inclusion in the study were the status of incident patients in the 1HD/wk regimen and the availability of a complete dataset for UKM analysis with Solute Solver. A total of 500 HD sessions associated to the available monthly UKM studies were retrieved from the local electronic clinical databases.
Methods
Kru, single pool Kt/V (spKt/V), eKt/V, V, PCRn and EKR values in the patients on the 1HD/wk regimen were obtained by using three different methods:
Method 1
Solute Solver [3]: it is the reference method and is freely available at www.ureakinetics.org; current version: 2.12, June 4, 2019. Of note, Solute Solver provides EKR values in terms of mL/min. For comparative purposes, the correspondent normalised EKR value was computed as follows: EKR35 = EKR/V * 35 [14].
Method 2
SPEEDY-1: it is a modified version of the original SPEEDY [11], which is available at www.era-edta.org/en/eudial (ongoing projects). In SPEEDY-1, the equations for estimating Kru, Kt/V, and PCRn have been replaced by slightly modified versions of the original formulae, as shown below:
where, UUN is the urinary urea nitrogen concentration (mg/dL); C0pw (mg/dL) is the pre-dialysis concentration (C0) of Blood Urea Nitrogen (BUN) in the plasma water (i.e., C0 divided by 0.93); UO is the daily urinary output (mL); and 1,440 is the number of minutes in a day. It is a modified version of the Daugirdas [9] and Obi et al. Equations (10), in which the time-averaged concentration (TAC) of urea nitrogen in serum water (TAC-SUNwater) over the urine collection period has been replaced by C0pw.
Equation 2 is the “second-generation” equation of the spKt/V introduced by Daugirdas [5], in which the original generation term of 0.008, which refers to the thrice-weekly schedule, has been replaced by the recalculated generation term of 0.0035, which is specific for the once-weekly HD schedule [12]; furthermore, R is the post-dialysis to pre-dialysis BUN ratio; t is the session length (min); UF is the intra-dialysis body weight loss (L); and BWT is the post-dialysis body weight (kg).
Equation 3 is the equation introduced by Tattersall et al. [15], as slightly modified by Daugirdas et al. [3], that estimates eKt/V from spKt/V and the session time, t. Of note, this equation is the one that is already present in the original version of SPEEDY; it was included “as is” in its modified version (SPEEDY-1).
Equation 4 is the recently introduced equation estimating PCRn (ePCRn) [13], absent in SPEEDY, and added in SPEEDY-1. Equation 4 requires the knowledge of V and of the dialyzer urea clearance (K) values. To this end, as detailed elsewhere [11], SPEEDY firstly estimates K from the dialyzer mass transfer-area coefficient for urea (KoA, mL/min), using the same data and equations as Solute Solver does [16]; then it computes a single pool V (Vsp) from the Kt/spKt/V ratio, and finally transforms Vsp into a double pool V [17]. SPEEDY-1 does the same as SPEEDY does.
Equation 5 estimates EKR35 from Kru, V and eKt/V [14], as corrected for the typical modelled urea distribution volume (V) of 35 L (EKR35, mL/min/35 L).
The whole sequence of equations in SPEEDY-1 is provided in the Supplementary Material.
Method 3
SPEEDY-1S: it is a simplified version of SPEEDY-1. In fact, as exemplified in the Appendix, it uses only the Eqs. 1–5; furthermore, by assuming that V coincides with the anthropometric estimate of total body water (Vant), as computed by the Watson et al. formula (18), SPEEDY-1S is able to compute ePCRn and EKR35 without all of the complexities associated to the estimates of both K and V, as outlined above.
Statistics
Microsoft Excel 2010 software was used for calculating means and standard deviations (SD), and drawing graphs. All statistical inferences were made using IBM SPSS Statistics 16.0 (SPSS Inc., Chicago, IL, USA) and values of P < 0.05 were assumed as statistically significant. The Bland–Altman analysis [19] and the one-sample t-test were used when appropriate.
Results
Table 1 shows the main data of the group of 100 patients at the start of the once-weekly HD regimen. On average, data from about 5 HD sessions per patient were available. Table 2 shows the main data of 500 dialysis sessions associated to monthly UKM studies: they were used as input for the subsequent calculations.
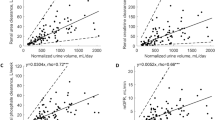
Table 3 shows the comparison between the paired values of UKM parameters, as computed by SPEEDY-1 and Solute Solver, respectively. All differences but one were statistically significant at the one-sample t-test; however, the agreement limits at Bland–Altman analysis (mean difference − 2SD and mean difference + 2SD) showed that all differences were negligible: this was true for the two Kru datasets (difference ranging from − 0.21 to − 0.05 mL/min), the two spKt/V datasets (difference ranging from − 0.05 to + 0.03), the two eKt/V datasets (difference ranging from − 0.05 to + 0.03), the two V datasets (difference ranging from − 1.01 to + 1.48 L), the two PCRn datasets (difference ranging from − 0.14 to + 0.13 g/kg/day), and the two EKR35 datasets (differences ranging from − 0.75 to + 0.82 mL/min/35 L).
Table 4 shows the comparison between the paired values of UKM parameters, as computed by SPEEDY-1S and Solute Solver, respectively. Of note, the results concerning Kru, spKt/V and eKt/V were the same as those shown in Table 3, the same formulae and the same data being used. However, the agreement limits at Bland–Altman analysis between the Vant and the double pool V values were relatively good: in fact, the SDs were quite large, so that the individual differences ranged from − 9.83 to + 11.28 L. Similarly, the agreement limits at Bland–Altman analysis between the PCRn and EKR35 values computed using the Vant and the corresponding ones obtained with Solute Solver were relatively good, their difference ranging from − 0.26 to + 0.22 g/kg/day and from − 1.85 to + 1.65 mL/min/35 L, respectively.
A list of abbreviations is provided in the Supplementary Material.
Discussion
Until recently, no simplified formulae were available for the routine assessment of Kru, Kt/V and PCRn in the once-weekly HD regimen. This was likely due to the fact that this regimen was rarely prescribed in the past and usually for short time periods in the early phase of the renal replacement therapy. On the contrary, nowadays there is an increasing interest in an incremental approach to HD, be it with one or two sessions per week [20,21,22,23]. As a matter of fact, a recent meta-analysis of cohort studies concluded that incremental dialysis “allows longer preservation of residual kidney function (RKF) thus deferring full-dose dialysis by about 1 year in HD and PD, with no increase in mortality risk” [24]. No randomized clinical trials testing incremental HD have yet been published [25]. Actually, one clinical trial, named IHDIP, is ongoing [26] and another one, named REAL LIFE, is starting patient enrolment [27]. Interestingly, both trials base the prescription of the once-weekly HD regimen on the recently introduced “Variable Target Model” (VTM) [14]. At variance with the so called “Fixed Target Model” (FTM), using VTM allows a lower dialysis dose and a lower Kru with respect to the current concepts of dialysis adequacy in incremental HD [14]. In short, FTM assumes that adequacy in incremental HD requires that the sum of dialysis clearance and kidney clearance be constant. One could easily realise that this is a wrong assumption by simply considering that, if it is only the sum of dialysis clearance and kidney clearance that matters, at the extremes, it should be indifferent if the given total clearance were obtained only by the native kidneys (patient not yet on dialysis) or only by dialysis (dialysis patient in anuria). To try to correct, at least in part, the mistakes derived by using a “fixed” target for the total clearance, Casino and Basile suggested using a “variable” target [14]. In short, by expressing the total (kidney + dialytic) clearance in terms of EKR, they hypothesized that the adequate EKR could vary from a minimum, at a selected Kru threshold to start HD, to a maximum corresponding to the selected adequate dialysis dose in the anuric state [14]. In conclusion, basing adequacy on VTM could allow to prescribe the 1HD/wk regimen in patients whose Kru is comprised between 5 and 3 mL/min/35 L, with a delivered spKt/V of about 1.2 [27]. Of note, neither trial [26, 27] requires the formal prescription of a strict low-protein diet to start and maintain incremental HD, essentially because, even if a low- protein diet could very likely help to preserve RKF, its mandatory prescription would drastically reduce the number of patients that could be offered the incremental approach. In fact, an important study focusing on a Combined Diet Dialysis Program concluded that “a low-protein diet combined with weekly hemodialysis can be considered only in motivated and selected ESRD patients” [21]. On the contrary, our hypothesis is that an infrequent HD schedule is the main factor that can help to preserve RKF: here, it must be stressed that the conditio sine qua non of the prescription of the once-weekly HD regimen is very strict monitoring of both RKF [23] and of the clinical status of the patients with a timely increase in the dose and/or frequency of treatment if needed [26, 27]. Clearly, the results of the two trials will confirm or reject their underlying hypotheses, including, among others, not only the validity of VTM but also the possibility of prescribing the 1HD/wk regimen to patients with preserved Kru without a strict low-protein diet [26, 27].
In any case, selected adequacy targets apart, the availability of simplified formulae to compute Kru, Kt/V and PCRn for patients in the 1HD/wk regimen could favour further studies on this issue. As stated above, two such equations have been introduced and validated to estimate spKt/V [12] and PCRn [13], respectively. The latter equations have been introduced into the new version of SPEEDY, SPEEDY-1. Moreover, we also tested a simple formula (Eq. 1) to assess Kru, based on the hypothesis that the well known slow increment in BUN over the last 24 h prior to the weekly HD session could allow using the pre-dialysis BUN, in terms of plasma water concentration, as a proxy for the TAC-SUNwater [9, 10] over the urine collection time period.
To summarize: we improved the original version of SPEEDY [11], by replacing the old equations estimating Kru and spKt/V with Eqs. 1 and 2, respectively, and adding two formulae for estimating PCRn and EKR35, respectively. This modified version, SPEEDY-1, provides accurate results and is the best alternative to Solute Solver as shown in Table 3. However, it is relatively complex because it has to estimate K and V. Thus, we tested a simplified version of SPEEDY-1, SPEEDY-1S: actually, we tested whether using Vant, that avoids the assessment of K and V, could provide acceptable PCRn results, in spite of the well known fact that Vant can markedly overestimate V [28]. As shown in Table 4, using Vant led to a difference in PCRn ranging from − 0.26 to + 0.22 g/kg/day, quite an important difference corresponding to − 25% and + 21%, respectively.
In conclusion, we implemented SPEEDY with a new version that is specific for the once-weekly HD regimen, SPEEDY-1. It provides accurate results and is the best alternative to Solute Solver. Using Vant instead of V in SPEEDY-1S led to a larger difference in PCRn and EKR35, which could be acceptable in clinical practice if SPEEDY-1 is not available.
References
Gotch FA, Sargent JA (1985) A mechanistic analysis of the National Cooperative Dialysis Study (NCDS). Kidney Int 28:526–534
Keshaviah PR, Emerson PF, Nolph KD (1999) Timely initiation of dialysis: a urea kinetic approach. Am J Kidney Dis 33:344–348
Daugirdas JT, Depner TA, Greene T et al (2009) Solute-solver: a web-based tool for modeling urea kinetics for a broad range of hemodialysis schedules in multiple patients. Am J Kidney Dis 54:798–809
National Kidney Foundation (2015) KDOQI clinical practice guidelines for hemodialysis adequacy: 2015 update. Am J Kidney Dis 66:884–930
Daugirdas JT (1993) Second generation logarithmic estimates of single-pool variable volume Kt/V: an analysis of error. J Am Soc Nephrol 4:1205–1213
Daugirdas JT, Leypoldt KJ, Akonur A, The FHN Trial Group et al (2013) Improved equation for estimating single-pool Kt/V at higher dialysis frequencies. Nephrol Dial Transpl 28:2156–2160
Depner TA, Daugirdas JT (1996) Equations for normalized protein catabolic rate based on two-point modeling of hemodialysis urea kinetics. J Am Soc Nephrol 7:780–785
Daugirdas JT (2017) Errors in computing the normalized protein catabolic rate due to use of single-pool urea kinetic modeling or to omission of the residual kidney urea clearance. J Ren Nutr 27:256–259
Daugirdas JT (2016) Estimating time-averaged serum urea nitrogen concentration during various urine collection periods: a prediction equation for thrice weekly and biweekly dialysis schedules. Semin Dial 29:507–509
Obi Y, Kalantar-Zadeh K, Streja E et al (2018) Prediction equation for calculating residual kidney urea clearance using urine collections for different hemodialysis treatment frequencies and interdialytic intervals. Nephrol Dial Transpl 33:530–539
Casino FG, Basile C (2018) A user-friendly tool for incremental haemodialysis prescription. Nephrol Dial Transpl 33:1046–1053
Casino FG, Deira J, Suárez MA et al (2021) Improving the “second generation Daugirdas equation” to estimate Kt/V on the once-weekly haemodialysis schedule. J Nephrol. https://doi.org/10.1007/s40620-020-00936-5
Casino FG, Mostacci SD, Sabato A et al (2020) The lacking equation that estimates the protein catabolic rate in patients on once-weekly haemodialysis. J Nephrol. https://doi.org/10.1007/s40620-020-00843-9
Casino FG, Basile C (2017) The variable target model: a paradigm shift in the incremental haemodialysis prescription. Nephrol Dial Transpl 32:182–190
Tattersall JE, DeTakats D, Chamney P et al (1996) The post-hemodialysis rebound: predicting and quantifying its effect on Kt/V. Kidney Int 50:2094–2102
Michaels AS (1966) Operating parameters and performance criteria for hemodialyzers and other membrane-separation devices. Trans Am Soc Artif Intern Organs 12:387–392
Daugirdas JT, Smye SW (1997) Effect of a two-compartment distribution on apparent urea distribution volume. Kidney Int 51:1270–1273
Watson PE, Watson ID, Blatt RD (1980) Total body water volumes for adult males and females estimated from simple anthropometric measurements. Am J Clin Nutr 33:27–29
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 327:307–310
Kalantar-Zadeh K, Casino FG (2014) Let us give twice-weekly hemodialysis a chance: revisiting the taboo. Nephrol Dial Transpl 29(9):1618–1620
Caria S, Cupisti A, Sau G, Bolasco P (2014) The incremental treatment of ESRD: a low-protein diet combined with weekly hemodialysis may be beneficial for selected patients. BMC Nephrol 15:172
Wong J, Vilar E, Davenport A et al (2015) Incremental haemodialysis. Nephrol Dial Transpl 30:1639–1648
Obi Y, Streja E, Rhee CM, Ravel V, Amin AN, Cupisti A, Chen J, Mathew AT, Kovesdy CP, Mehrotra R (2016) Kalantar-zadeh k incremental hemodialysis, residual kidney function, and mortality risk in incident dialysis patients: a cohort study. Am J Kidney Dis 68(2):256–265
Garofalo C, Borrelli S, De Stefano T et al (2019) Incremental dialysis in ESRD: systematic review and meta-analysis. J Nephrol 32:823–836
Basile C, Casino FG (2019) Incremental haemodialysis and residual kidney function: more and more observations but no trials. Nephrol Dial Transpl 34:1806–1811
Deira J, Suárez MA, López F et al (2019) IHDIP: a controlled randomized trial to assess the security and effectiveness of the incremental hemodialysis in incident patients. BMC Nephrol 20(1):8. https://doi.org/10.1186/s12882-018-1189-6
Casino FG, Basile C, Kirmizis D et al (2020) The reasons for a clinical trial on incremental haemodialysis. Nephrol Dial Transpl 35:2015–2019
Daugirdas JT, Greene T, Depner T, for the Hemodialysis (HEMO) Study Group et al (2003) Anthropometrically estimated total body water volumes are larger than modeled urea volume in chronic hemodialysis patients: effects of age, race and gender. Kidney Int 64:1108–1119
Funding
No funding agency granted the present study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Research involving human participants and/or animals
This article does not contain any studies with animals performed by any of the authors.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Numerical example of the use of SPEEDY-1S with input data from a patient.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Casino, F.G., Deira, J., Suárez, M.A. et al. Routine assessment of kidney urea clearance, dialysis dose and protein catabolic rate in the once-weekly haemodialysis regimen. J Nephrol 34, 2009–2015 (2021). https://doi.org/10.1007/s40620-021-01033-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40620-021-01033-x