
Abstract
Prescription opioids still account for a large proportion of overdose deaths and contribute to opioid use dependence (OUD). Studies earlier in the epidemic suggest clinicians were less likely to prescribe opioids to racial/ethnic minorities. As OUD-related deaths have increased disproportionately amongst minority populations, it is essential to understand racial/ethnic differences in opioid prescribing patterns to inform culturally sensitive mitigation efforts. The purpose of this study is to estimate racial/ethnic differences in opioid medication use among patients prescribed opioids. Using electronic health records and a retrospective cohort study design, we estimated multivariable hazard models and generalized linear models, assessing racial/ethnic differences in OUD diagnosis, number of opioid prescriptions, receiving only one opioid prescription, and receiving ≥18 opioid prescriptions. Study population (N=22,201) consisted of adult patients (≥18years), with ≥3 primary care visits (ensuring healthcare system linkage), ≥1 opioid prescription, who did not have an OUD diagnoses prior to the first opioid prescription during the 32-month study period. Relative to racial/ethnic minority patients, White patients, in both unadjusted and adjusted analyses, had a greater number of opioid prescriptions filled, a higher proportion received ≥18 opioid prescriptions, and a greater hazard of having an OUD diagnosis subsequent to receiving an opioid prescription (all groups p<0.001). Although opioid prescribing rates have declined nationally, our findings suggest White patients still experience a high volume of opioid prescriptions and greater risk of OUD diagnosis. Racial/ethnic minorities are less likely to receive follow-up pain medications, which may signal low care quality. Identifying provider bias in pain management of racial/ethnic minorities could inform interventions seeking balance between adequate pain treatment and risk of opioid misuse/abuse.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The opioid epidemic remains a major public health crisis [1,2,3,4]. Despite increased attention and efforts to reduce opioid-related morbidity and mortality, the number of opioid-related overdose deaths continues to rise [5, 6]. Nationally, between 1999 and 2019, there were 495,892 opioid-related deaths [7, 8]. In 2019 alone, there were more than 49,800 overdose deaths associated with opioids, the highest number in one year to date.
The initial rise in opioid-related mortality was primarily driven by opioid prescriptions for pain management. Medical providers were treating pain as the 5th vital sign and made a concerted effort to minimize the amount of pain experienced by patients [9, 10]. While opioids are an effective way to treat acute pain when properly managed by a medical professional [11, 12], there is little evidence that the therapeutic benefits of opioids extend to chronic non-cancer pain [13,14,15,16]. The addictive chemical compounds of opioids [17] and the liberal prescribing practices contributed to prescription opioid misuse, development of opioid use disorder [18], and increased rates of fatal and non-fatal opioid-related overdose [19,20,21,22].
Differential prescribing and pain management have contributed to discrepancies in opioid-related morbidities and mortalities across diverse populations. Studies have shown that relative to Whites, racial/ethnic minorities are prescribed opioids at lower rates and are less likely to receive a diagnosis of pain disorder, even after adjustment for objective measures of pain [23,24,25]. Clinicians are more likely to be concerned of misuse or opioid diversion when dealing with minority patients [26,27,28,29]. These differences led to much higher opioid prescribing rates among Whites than Blacks and Latinos, contributing to elevated levels of opioid-related misuse and death among Whites ([30]; Jordan M. Harrison et al., 2018; [31,32,33]). Between 1990 and 2010, the rate of opioid-related mortality for Whites increased by 225% while decreased for Blacks and Latinos, 3% and 17%, respectively [34].
The nature of the epidemic has evolved over recent years. Prescribing management strategies [35], pharmacologic similarities between illicit and prescription opioids [36], as well as the cost and availability of illicit opioids have contributed to an increase in heroin and synthetic opioids use [37,38,39]. As the overdose epidemic has shifted from predominantly prescription opioid use (1999–2006) to now heroin and synthetic opioid (2006–present) [40]. Black and Latino populations have experienced a disproportionate increase in opioid-related mortality rates as compared to Whites [41]. Between 2015-2020, the overall rate of opioid-related mortality in the USA increased by 322%, 218% and 86% for Black, Latino, and White individuals, respectively [42]. This pattern is reflected in Massachusetts specifically, between 2015 and 2020, opioid-related mortality increased by 155%, 115%, and 20%, for Black, Latinx, and White residents, respectively [42]. The problem was further exacerbated in Massachusetts by the onset of the COVID-19 pandemic where the cumulative excess mortality for Black residents outpaced that of all other racial/ethnic groups [43].
In response to the dangers of overprescribing, in 2018 the U.S. Department of Justice created the Prescription Interdiction and Litigation (PIL) Taskforce, with the goal of pursuing criminal and civil law enforcement focused on opioid manufacturers, distributors, and prescribers [44]. Despite emerging attention and regulatory reinforcement to mitigate overprescribing risks, prescription opioids still accounted for approximately 30% of opioid-related overdose deaths in 2019 [7]. While the Department of Justice is still actively convicting providers for the unnecessary, unlawful, and harmful distribution of prescription opioids [45,46,47] continued efforts are needed to better understand the heterogeneity in opioid prescribing and opioid dependence to identify high-risk patients and inform the development of culturally-relevant harm-reducing interventions and policies.
The purpose of this study is to describe racial/ethnic differences in opioid medication use among patients prescribed opioids. Through analysis of electronic health records from an urban academic safety-net healthcare system, we conducted a retrospective analysis to assess differences in the number of opioid prescriptions, receiving only one opioid prescription, receiving an opioid use disorder diagnosis, and receiving 18 or more opioid prescriptions (95th percentile of the number of opioid prescriptions). We hypothesize that racial/ethnic minority patients will have higher rates of receiving only one opioid prescription and lower rates of 18 or more opioid prescriptions and progression from a single opioid prescription to an opioid use disorder diagnosis.
Methods
Data and Sample Description
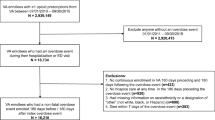
In this retrospective cohort study, electronic health records were analyzed from an urban academic safety-net healthcare system that provides services to over 140,000 patients annually who are predominately low-income, publicly insured, racial/ethnic/linguistic minorities. The healthcare system is comprised of three hospitals and fifteen community clinics that provide primary care, inpatient and outpatient specialty mental health care and substance use treatment. This study focused on opioid prescription fills between January 1, 2016 and August 31, 2018 among adults who were 18 years of age and older at the start of the study period (N=203,859). To ensure persons included in the sample were regular patients in the healthcare system, those with fewer than 3 primary care visits during the 32-month study period were excluded (N=142,177). This exclusion increases the likelihood that patients obtained all of their opioid prescriptions and follow-up treatment within the healthcare system under study. Our final analytic sample consisted of 22,201 adults that had at least three primary care visits, at least one opioid prescription, and did not have an opioid use disorder diagnoses prior to their first opioid prescription during the 32-month study period. The study was approved by the institutional review board. Data are not publicly available due to privacy and HIPAA restrictions.
Dependent Variables
We assessed racial/ethnic differences in prescription opioid use. Use outcomes included count of opioid prescriptions, probability of having only one opioid prescription, probability of receiving 18 or more opioid prescriptions (95th quantile or higher), and the probability of having an opioid use disorder diagnosis subsequent to the initial opioid prescription. The 95th quantile of service use has been used in prior studies to characterize extreme use of behavioral healthcare services ([48]; Cook, 2013; [49]).
Independent Variables
Our primary variable of interest was race/ethnicity, which we classified using the US census categories non-Latino White (referred to as White), non-Latino Black (referred to as Black), Hispanic/Latino (referred to as Latino), and non-Latino Asian (referred to as Asian). To address confounding, regression models included the following covariates: age (18–24, 25–34, 35–44, 45-54, 55–64, 65+), sex (males, females), indicator for chronic pain, and indicators for behavioral health disorder diagnoses (anxiety disorder, bipolar disorder, major depression disorder, schizophrenia disorder, alcohol use disorder, cocaine use disorder, cannabis use disorder, and tobacco use disorder). We used ICD-10 codes, as in prior research [50], to identify chronic pain in the electronic health record.
Statistical Analysis
We first compared racial/ethnic minority (Black, Latino, and Asian) patients to White patients on sociodemographic characteristics, clinical diagnoses, and opioid use patterns using chi-square tests and t-tests for dichotomous and continuous variables, respectively. Next, to compare the number of opioid prescriptions between racial/ethnic minority patients versus White patients, we estimated a multivariable generalized linear model (GLM) with a negative binomial distribution and a log link function with robust standard errors. A negative binomial distribution was selected due to the overdispersion of the outcome measure. The GLM was adjusted for previously mentioned covariates. To estimate racial/ethnic differences in the probability of having one opioid prescription and the probability of being in the 95th percentile of opioid prescriptions, we estimated GLMs with binomial distributions, logit link functions, robust standard errors, and adjusted for previously mentioned covariates. We used predictive margins methods [51] to transform regression coefficients into predicted probabilities and predicted means. As such, binary outcomes were reported as percentage-point differences in predicted probabilities for racial/ethnic minority patients compared to White patients. Count outcomes were reported as the difference in mean counts for racial/ethnic minority patients compared to White patients.
To estimate the hazard rates of developing opioid use disorder subsequent to receiving an opioid prescription fill and to statistically compare differences between racial/ethnic minority patients versus White groups, we specified Cox proportional hazard models, adjusting for previously described covariates. In using a cox-proportional hazard model we assume the hazard in the comparison groups is proportional to that of the reference group. We plotted log-minus-log survival plots to graphically inspect for violations of the assumption [52]. To empirically test for violations of proportionality, we conducted the Schoenfeld Residual Test [52]. We also plotted Kaplan-Meier survival curves to measure differences between racial/ethnic minority patients and White patients in obtaining an opioid use disorder diagnosis subsequent to receiving an opioid prescription fill [53]. The Logrank test was used to determine if there were significant differences between the patient groups during the study period [52]. In estimating Kaplan-Meier survival functions, we accounted for differences in exposure time and the right censoring of patients [53]. We estimated curves for each patient group, White, Black, Asian, and Latino, adjusting for sociodemographic and clinical characteristics. Analyses were conducted using Stata release 16.1. P ≤ .05 (2-tailed) was considered statistically significant. Full regression model results are in Appendix Table 3. We conducted a complete case analysis. There was less than 2% of data missing for our outcomes, primary variable of interest, and covariates. Based on prior literature, less than 5% missing data is considered acceptable [54].
Results
Table 1 provides an unadjusted comparison of outcomes, patient demographics, service use, and behavioral health disorder diagnoses by race/ethnicity. Concerning outcomes, relative to White patients, racial/ethnic minority patients had a lower mean number of opioid prescriptions, probability of being in the 95th percentile of opioid prescriptions, and probability of having an opioid use disorder diagnosis subsequent to an opioid prescription (all p<0.001). Compared to White patients, all racial/ethnic minority patients were more likely to be female, Latino patients were more likely to be younger whereas Asian patients were more likely to be older. All racial/ethnic minority patients had lower substance use and mental health disorder diagnoses compared to White patients (all p<0.001).
In Fig. 1, adjusted regression results suggest that Black, Latino, and Asian patients had a lower mean number of opioid prescription compared to White patients (e.g., Black −1.6; p<0.001; 95%CI, −1.9 to −1.3). Relative to White patients, Latino patients were 3.9 percentage-points (p<0.001; 95%CI, −5.3 to −2.4) less likely to receive only one opioid prescription during the study period (Fig. 2) but there were no significant differences with Black and Asian patients. All racial/ethnic minority patients had a lower probability of receiving 18 or more opioid prescriptions (Fig. 3; e.g., Black −4.5%; p<0.001; 95%CI, −5.5 to −3.6%). In adjusted Cox proportional hazard models (Table 2), White patients had a greater hazard than racial/ethnic minority patients of having an opioid use disorder diagnosis subsequent to receiving an opioid prescription. Fig. 4 shows graphically that Whites with an opioid prescription had a greater cumulative hazard over time than Black, Latino, and Asian patients of subsequently receiving a opioid use disorder diagnosis in the electronic health record.

Adjusted mean number of opioid prescriptions by race/ethnicity a. *p<0.05; **p<0.01; ***p<0.001—Comparisons between racial/ethnic minorities and Whites; aSample consisted of adults that had at least three primary care visits, at least one opioid prescription, and did not have an opioid use disorder diagnoses prior to their first opioid prescription during the 32-month study period (n=22,201); regression model adjust for age, sex, chronic pain, anxiety disorder, bipolar disorder, major depression disorder, schizophrenia disorder, alcohol use disorder, cocaine use disorder, cannabis use disorder, and tobacco use disorder

Adjusted probability of having one opioid prescription by race/ethnicitya. *p<0.05; **p<0.01; ***p<0.001–comparisons between racial/ethnic minorities and Whites; asample consisted of adults that had at least three primary care visits, at least one opioid prescription, and did not have an opioid use disorder diagnoses prior to their first opioid prescription during the 32-month study period (n=22,201); regression model adjust for age, sex, chronic pain, anxiety disorder, bipolar disorder, major depression disorder, schizophrenia disorder, alcohol use disorder, cocaine use disorder, cannabis use disorder, and tobacco use disorder

Adjusted probability of having 18+ opioid prescriptions by race/ethnicitya. *p<0.05; **p<0.01; ***p<0.001—comparisons between racial/ethnic minorities and Whites; asample consisted of adults that had at least three primary care visits, at least one opioid prescription, and did not have an opioid use disorder diagnoses prior to their first opioid prescription during the 32-month study period (n=22,201); regression model adjust for age, sex, chronic pain, anxiety disorder, bipolar disorder, major depression disorder, schizophrenia disorder, alcohol use disorder, cocaine use disorder, cannabis use disorder, and tobacco use disorder

Cumulative hazard rates of an opioid use disorder diagnosis
Discussion
In this study, we used longitudinal electronic health records to assess differences in prescription opioid use among racial/ethnic minority patients versus White patients. We used patient data collected between January 2016 and August 2018, during the third wave of the opioid overdose epidemic in which heroin and opioid analogues (i.e., fentanyl) accounted for the majority of opioid related deaths [40]. Our adjusted results demonstrate that White patients, relative to patients from racial/ethnic minority groups, had a significantly higher number of opioid prescriptions filled, a larger proportion were in the 95th percentile of opioid prescriptions, and had an elevated risk of having an opioid use disorder diagnosis subsequent to an opioid prescription. Findings also suggested that Latino patients were less likely to have only one opioid prescription.
Our results suggest that the lower rates of opioid prescriptions among racial/ethnic minorities found earlier in the opioid epidemic in ED [32] and primary care settings [55] persisted as the epidemic has matured, at least in this urban safety net location. Despite significant attention in prior studies [56,57,58] and the lay press [59], it appeared that differential prescribing among racial/ethnic groups continues. Our finding of differential prescribing may in part be due to providers’ biased heuristics about pain thresholds for racial/ethnic minorities patterns [24,25,26, 56,57,58] and clinician concern of misuse or opioid diversion when dealing with minority patients [27,28,29]. This differential prescribing reduced the risk for a progression to an opioid use disorder diagnosis for racial/ethnic minorities, but may also represent poor pain management for racial/ethnic minority patients. This finding suggests distinctive etiologies for opioid use disorder amongst racial/ethnic minorities as compared to White patients, and indicates a need for demographic-specific prevention and intervention efforts.
One exception to these persistent findings is that, relative to White patients, Latinos were less likely to receive only one opioid prescription during the study period, suggesting that pain management for Latino patients may have been more effectively distributed over time. This aligns with research from Harrison and colleagues that found national trends in opioid prescribing among racial/ethnic groups are beginning to narrow (J. M. Harrison et al., 2018). However, patients of color are less likely to have a usual source of care (Radley, 2021) and receive guideline concordant care ([60]; Radley, 2021; [61]) which may contribute to critical information not being shared regarding the risks of prescription opioid use. Moreover, patients of color have low rates of health literacy compared to White patients [62], which may contribute to risky prescription opioid use even when the appropriate information is shared. Equitable pain management and prescription opioid monitoring is needed to ensure the appropriate use of medically needed opioid treatment.
Opioid prescribing is commonly informed by patient characteristics, prescriber attitudes about opioids, as well as decision processing tools [63,64,65,66]. Opioid risk assessment screeners, urine toxicology screenings, standardized pain scales, and prescription drug monitoring systems are all resources in place intended to guide and standardize prescribing decisions [67,68,69,70,71], yet evidence shows that their use and impact are not widespread [72,73,74,75]. It is imperative to educate providers so they are equipped to make informed prescribing decisions, initiate conversations with their patients about opioid misuse, accurately monitor patients’ pain and drug use, and utilize non-opioid analgesic strategies in a standardized and equitable fashion across patient populations [76, 77].
The finding that White patients were more likely to be in the 95th percentile of opioid prescriptions may be partially attributed to the disproportionately large number (70%) of long-term opioid treatment patients that are of White race within the healthcare system. There is little evidence on the effectiveness of long-term opioid therapy for chronic non-cancer pain [78, 79]. Though guidelines exist for opioid prescribing and monitoring [80], there is limited guidance from expert groups such as the American Pain Society and the American Academy of Pain Medicine to inform clinicians on best practices for treating patients on long-term opioid treatment [81]. Clinicians need more alternatives to pain management and appropriate tapering regimens while considering their patient’s quality of life, physical functioning, and pain thresholds [10, 77, 82]. Future research should examine best practices for addressing the needs of patients on long-term opioid therapy.
Even though national rates of opioid-related mortality are rising among Blacks and Latinos [6], Whites continue to have a higher likelihood of transitioning from an opioid prescription to an opioid use disorder diagnosis. This may be the result of racial/ethnic minorities’ lower access to treatment given that an opioid use disorder diagnosis is only recorded in the electronic health record if the patient actually receives treatment; racial/ethnic minority patients are less likely to have a usual source of care [83,84,85], less likely to access healthcare service use than White patients [86, 87], and have fewer interactions with the medical system [84, 88], which may limit the opportunity for medical providers to identify and diagnose an opioid use disorder. Future studies that track individuals with an opioid prescription in community settings will help to understand whether these lower rates of transition to opioid use disorder are explained by poorer access to treatment. There is a continuing need to improve diagnosis and referral processes in primary care and community health settings.
Despite our findings, the overall mortality rate associated with prescription opioids have steadily declined in the state of Massachusetts (the location of the healthcare system under study) since 2015 [89]. This is in part attributed to the implementation of wide-reaching prevention, harm reduction, and treatment initiatives. For example, the state signed two bills into law in 2016 (“An Act relative to substance use, treatment, education and prevention, ” 2016) and 2018 (“An Act relative to the prescription monitoring program, ” 2018), which placed limits on the length of time on opioid prescriptions, increased oversight of opioid prescriptions through the Prescription Monitoring Program, removal of insurance-related barriers for substance abuse evaluations, increased naloxone training for laypersons, clinicians and first responders. The onset of the COVID-19 pandemic has contributed to an uptick in opioid-related deaths [90] which may have moderated the gains achieved through these policies and shifted resources needed to combat the concurrent opioid epidemic. Now more than ever, it is imperative to rigorously evaluate the impact of these policies at the state and community level to assess their effectiveness at equitably reducing prescription opioid misuse, illicit opioid use, development of opioid use disorder, as well as fatal and non-fatal opioid overdose.
Our findings should be considered within the context of several limitations. First, though we used time to rule out reverse temporal relationships between opioid prescribing and opioid use disorder documentation in the electronic health record; it is possible that opioid use disorder onset occurred prior to the opioid prescription. Nonetheless, our approach allows for the identification of patients within the healthcare system that are likely to benefit from harm-reducing activities. Second, we were unable to observe opioid prescribing outside of the current hospital system. We tried to address this potential limitation by restricting our sample to patients that had at least three primary care visits during the time of study. While there is still the possibly that some patients accessed outside services, this only presents a problem if this occurred differentially across racial/ethnic groups—we have no reason to be believe this occurred. Future studies should leverage datasets, such as all-payer claims, to obtain a comprehensive picture of the services commonly used prior to opioid-related death. Third, our results may not be generalizable to other healthcare systems and patient populations since our sample was generated from a safety-net hospital system that serves a primarily low-income population with higher proportions of racial and ethnic minorities. However, our study may serve as a case-study that describes opioid prescribing patterns among racial/ethnic patients receiving care within an urban safety-net academic healthcare system. Finally, we were unable to determine the pain severity associated with chronic pain diagnoses.
Conclusion
Our findings provide insight on opioid prescribing patterns among racial/ethnic groups in a safety-net academic healthcare system. As we continue to endure the opioid epidemic that is currently fueled by illicitly manufactured fentanyl, it is important to maintain vigilance on the extent to which prescription opioids are prescribed and potentially misused. Attention and resources are shifting to fight illicit opioids and the concurrent COVID-19 pandemic. Patients of color continue to experience differential prescribing and pain management. Efforts should be made to provide guideline concordant care that is equitable as well as culturally and linguistically appropriate to all patients regardless of their race/ethnicity and language capacity.
References
Damiescu R, Banerjee M, Lee DYW, Paul NW, Efferth T. Health(care) in the crisis: reflections in science and society on opioid addiction. Int J Environ Res Public Health. 2021;18(1):341. https://doi.org/10.3390/ijerph18010341.
Honein MA, Boyle C, Redfield RR. Public health surveillance of prenatal opioid exposure in mothers and infants. Pediatrics. 2019;143(3):e20183801. https://doi.org/10.1542/peds.2018-3801.
Kirson NY, Scarpati LM, Enloe CJ, Dincer AP, Birnbaum HG, Mayne TJ. The economic burden of opioid abuse: updated findings. J Manag Care Spec Pharm. 2017;23(4):427–45. https://doi.org/10.18553/jmcp.2017.16265.
National Institute on Drug Abuse [NIDA]. Drug use and viral infections (HIV, Hepatitis) DrugFacts. 2020. Retrieved from https://nida.nih.gov/publications/drugfacts/drug-use-viral-infections-hiv-hepatitis. Accessed 2 March 2023.
Centers for Disease Control and Prevention. Drug overdose mortality by state. 2018. Retrieved from https://www.cdc.gov/nchs/pressroom/sosmap/drug_poisoning_mortality/drug_poisoning.htm. Accessed 2 March 2023.
Scholl L, Seth P, Kariisa M, Wilson N, Baldwin G. Drug and opioid-involved overdose deaths—United States, 2013–2017. Morb Mortal Wkly Rep. 2019a;67(5152):1419.
Centers for Disease Control and Prevention. Multiple cause of death, 1999-2019. 2020. Retrieved from https://wonder.cdc.gov/mcd.html. Accessed 2 March 2023.
Kaiser Family Foundation. Opioid Overdose deaths and opioid overdose deaths as a percent of all drug overdose deaths. (2020a). Retrieved from https://www.kff.org/other/state-indicator/opioid-overdose-deaths/?activeTab=graph¤tTimeframe=0&startTimeframe=19&selectedDistributions=opioid-overdose-deaths&selectedRows=%7B%22wrapups%22:%7B%22united-states%22:%7B%7D%7D%7D&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D. Accessed 2 March 2023.
Lanser P, Gesell S. Pain management: the fifth vital sign. Healthc. Benchmarks. 2001;8(6):68–70.
Mandell BF. The fifth vital sign: A complex story of politics and patient care. Cleve Clin J Med. 2016;83(6):400–1. https://doi.org/10.3949/ccjm.83b.06016.
Dickenson A. Mechanisms of the analgesic actions of opiates and opioids. Br Med Bull. 1991;47(3):690–702.
Stein C. New concepts in opioid analgesia. Expert Opin Investig Drugs. 2018;27(10):765–75. https://doi.org/10.1080/13543784.2018.1516204.
Coffin PO, Rowe C, Oman N, Sinchek K, Santos G-M, Faul M, Bagnulo R, Mohamed D, Vittinghoff E. Illicit opioid use following changes in opioids prescribed for chronic non-cancer pain. PloS One. 2020;15(5):e0232538.
Freynhagen R, Geisslinger G, Schug SA. Opioids for chronic non-cancer pain. BMJ. 2013;346. https://doi.org/10.1136/bmj.f2937.
Kalso E, Edwards JE, Moore RA, McQuay HJ. Opioids in chronic non-cancer pain: systematic review of efficacy and safety. Pain. 2004;112(3):372–80.
Nury E, Schmucker C, Nagavci B, Motschall E, Nitschke K, Schulte E, Wegwarth O, Meerpohl JJ. Efficacy and safety of strong opioids for chronic noncancer pain and chronic low back pain: a systematic review and meta-analyses. Pain. 2022;163(4):610–36.
Comer SD, Sullivan MA, Whittington RA, Vosburg SK, Kowalczyk WJ. Abuse liability of prescription opioids compared to heroin in morphine-maintained heroin abusers. Neuropsychopharmacology. 2008;33(5):1179–91. https://doi.org/10.1038/sj.npp.1301479.
Vowles KE, McEntee ML, Julnes PS, Frohe T, Ney JP, van der Goes DN. Rates of opioid misuse, abuse, and addiction in chronic pain: a systematic review and data synthesis. Pain. 2015;156(4):569–76.
Kim B, Nolan S, Beaulieu T, Shalansky S, Ti L. Inappropriate opioid prescribing practices: a narrative review. Am J Health Syst Pharm. 2019;76(16):1231–7.
Rudd RA, Seth P, David F, Scholl L. Increases in drug and opioid-involved overdose deaths - United States, 2010-2015. MMWR. Morb. Mortal. Wkly. Rep. 2016;65(50-51):1445–52. https://doi.org/10.15585/mmwr.mm655051e1.
Seth P, Rudd RA, Noonan RK, Haegerich TM. Quantifying the epidemic of prescription opioid overdose deaths [Article]. Am J Public Health. 2018a;108(4):500–2. https://doi.org/10.2105/AJPH.2017.304265.
Seth P, Scholl L, Rudd RA, Bacon S. Overdose deaths involving opioids, cocaine, and psychostimulants - United States, 2015-2016. MMWR. Morb Mortal Wkly Rep. 2018b;67(12):349–58. https://doi.org/10.15585/mmwr.mm6712a1.
Hoffman KM, Trawalter S, Axt JR, Oliver MN. Racial bias in pain assessment and treatment recommendations, and false beliefs about biological differences between blacks and whites. Proc Natl Acad Sci U S A. 2016, Apr 19;113(16):4296–301. https://doi.org/10.1073/pnas.1516047113.
Morales ME, Yong RJ. Racial and ethnic disparities in the treatment of chronic pain. Pain Med. 2021;22(1):75–90.
Morden NE, Chyn D, Wood A, Meara E. Racial inequality in prescription opioid receipt—role of individual health systems. N Engl J Med. 2021;385(4):342–51.
Haq N, McMahan VM, Torres A, Santos G-M, Knight K, Kushel M, Coffin PO. Race, pain, and opioids among patients with chronic pain in a safety-net health system. Drug Alcohol Depend. 2021;222:108671.
Hirsh AT, Anastas TM, Miller MM, Quinn PD, Kroenke K. Patient race and opioid misuse history influence provider risk perceptions for future opioid-related problems. Am. Psychol. 2020;75(6):784.
Moskowitz D, Thom DH, Guzman D, Penko J, Miaskowski C, Kushel M. Is primary care providers’ trust in socially marginalized patients affected by race? J Gen Intern Med. 2011;26(8):846–51. https://doi.org/10.1007/s11606-011-1672-2.
Vijayaraghavan M, Penko J, Guzman D, Miaskowski C, Kushel MB. Primary care providers’ views on chronic pain management among high-risk patients in safety net settings. Pain Med. 2012;13(9):1141–8. https://doi.org/10.1111/j.1526-4637.2012.01443.x.
Anderson KO, Green CR, Payne R. Racial and ethnic disparities in pain: causes and consequences of unequal care. J Pain. 2009;10(12):1187–204. https://doi.org/10.1016/j.jpain.2009.10.002.
Kaiser Family Foundation. Opioid Overdose deaths by race/ethnicity. 2020b. Retrieved from https://www.kff.org/other/state-indicator/opioid-overdose-deaths-by-raceethnicity/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D. Accessed 2 March 2023.
Pletcher MJ, Kertesz SG, Kohn MA, Gonzales R. Trends in opioid prescribing by race/ethnicity for patients seeking care in US emergency departments. JAMA. 2008;299(1):70–8. https://doi.org/10.1001/jama.2007.64.
Singhal A, Tien YY, Hsia RY. Racial-ethnic disparities in opioid prescriptions at emergency department visits for conditions commonly associated with prescription drug abuse. PloS One. 2016;11(8):e0159224. https://doi.org/10.1371/journal.pone.0159224.
Centers for Disease Control and Prevention. Wide-ranging online data for epidemiologic research [WONDER]. 2020. Retrieved from http://wonder.cdc.gov. Accessed 2 March 2023.
Kaiser Family Foundation. States reporting medicaid FFS Pharmacy benefit management strategies for opioids in place. 2019. Retrieved from https://www.kff.org/medicaid/state-indicator/states-reporting-medicaid-ffs-pharmacy-benefit-management-strategies-for-opioids-in-place/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Location%22,%22sort%22:%22asc%22%7D. Accessed 2 March 2023.
Compton WM, Jones CM, Baldwin GT. Relationship between nonmedical prescription-opioid use and heroin use. N Engl J Med. 2016;374(2):154–63.
Hoopsick RA, Homish GG, Leonard KE. Differences in opioid overdose mortality rates among middle-aged adults by race/ethnicity and sex, 1999-2018. Public Health Rep. 2021;136(2):192–200.
Mattson CL, Tanz LJ, Quinn K, Kariisa M, Patel P, Davis NL. Trends and geographic patterns in drug and synthetic opioid overdose deaths—United States, 2013–2019. Morb Mortal Wkly Rep. 2021;70(6):202.
National Academies of Sciences, Engineering, and Medicine. Pain management and the opioid epidemic: balancing societal and individual benefits and risks of prescription opioid use. Washington, DC: The National Academies Press. 2017. https://doi.org/10.17226/24781.
Centers for Disease Control and Prevention. Understanding the opioid overdose epidemic. 2021. Retrieved from https://www.cdc.gov/opioids/basics/epidemic.html. Accessed 2 March 2023.
Scholl L, Seth P, Kariisa M, Wilson N, Baldwin G. Drug and opioid-involved overdose deaths—United States, 2013–2017. Morb Mortal Wkly Rep. 2019b;67(51-52):1419.
Centers for Disease Control and Prevention (CDC). Multiple cause of death, 2015-2020. 2020. Retrieved from https://wonder.cdc.gov/mcd.html. Accessed 2 March 2023.
Liao CY, Garcia GGP, DiGennaro C, Jalali MS. Racial disparities in opioid overdose deaths in Massachusetts. JAMA Network Open. 2022;5(4):e229081.
Department of Justice, O. o. P. A. (2018). Attorney General sessions announces new prescription interdiction & litigation task force
Department of Justice. Former Delaware doctor sentenced to 20 years in prison for unlawfully distributing opioid pills. 2022a. Retrieved from https://www.justice.gov/opa/pr/former-delaware-doctor-sentenced-20-years-prison-unlawfully-distributing-opioid-pills. Accessed 2 March 2023.
Department of Justice. Former Tennessee clinic owner sentenced for opioid distribution. 2022b. Retrieved from https://www.justice.gov/opa/pr/former-tennessee-clinic-owner-sentenced-opioid-distribution. Accessed 2 March 2023.
Department of Justice. Pain Clinic owners convicted of unlawfully distributing opioids and multimillion-dollar health care fraud. 2022c. Retrieved from https://www.justice.gov/opa/pr/pain-clinic-owners-convicted-unlawfully-distributing-opioids-and-multimillion-dollar-health. Accessed 2 March 2023.
Cook B, Manning WG. Thinking beyond the mean: a practical guide for using quantile regression methods for health services research. Shanghai Arch Psychiatry. 2013;25(1):55–9. https://doi.org/10.3969/j.issn.1002-0829.2013.01.011.
Cook BL, Manning WG. Measuring racial/ethnic disparities across the distribution of health care expenditures. Health Serv Res. 2009;44(5p1):1603–21.
Denis CM, Morales KH, Wu Q, Metzger DS, Cheatle MD. Association between diagnoses of chronic noncancer pain, substance use disorder, and HIV-related outcomes in people living with HIV. J Acquir Immune Defic Syndr. 2019;82(2):S142–7.
Graubard BI, Korn EL. Predictive margins with survey data. Biometrics. 1999;55(2):652–9.
Vittinghoff E, Glidden DV, Shiboski SC, McCulloch CE. Regression methods in biostatistics: linear, logistic, survival, and repeated measures models: Springer Science & Business Media; 2011.
Rothman KJ, Greenland S, Lash TL. Modern epidemiology: Lippincott Williams & Wilkins; 2008.
Schafer JL. Multiple imputation: a primer. Stat Methods Med Res. 1999;8(1):3–15. https://doi.org/10.1177/096228029900800102.
Olsen Y, Daumit GL, Ford DE. Opioid prescriptions by U.S. primary care physicians from 1992 to 2001. J Pain. 2006;7(4):225–35. https://doi.org/10.1016/j.jpain.2005.11.006.
Becker WC, Starrels JL, Heo M, Li X, Weiner MG, Turner BJ. Racial differences in primary care opioid risk reduction strategies. Ann Fam Med. 2011;9(3):219–25.
Hausmann LRM, Gao S, Lee ES, Kwoh CK. Racial disparities in the monitoring of patients on chronic opioid therapy. PAIN®. 2013;154(1):46–52. https://doi.org/10.1016/j.pain.2012.07.034.
Hirsh AT, Hollingshead NA, Ashburn-Nardo L, Kroenke K. The interaction of patient race, provider bias, and clinical ambiguity on pain management decisions. J Pain. 2015;16(6):558–68. https://doi.org/10.1016/j.jpain.2015.03.003.
Frakt A, Monkovic T. A ‘Rare Case Where Racial Biases’ Protected African-Americans: The New York Times; 2019. https://www.nytimes.com/2019/11/25/upshot/opioid-epidemic-blacks.html
Burgess DJ, van Ryn M, Crowley-Matoka M, Malat J. Understanding the provider contribution to race/ethnicity disparities in pain treatment: insights from dual process models of stereotyping. Pain Med. 2006;7(2):119–34. https://doi.org/10.1111/j.1526-4637.2006.00105.x.
Shavers VL, Bakos A, Sheppard VB. Race, ethnicity, and pain among the U.S. adult population. J Health Care Poor Underserved. 2010;21(1):177–220. https://doi.org/10.1353/hpu.0.0255.
Schillinger D. The Intersections between social determinants of health, health literacy, and health disparities. Stud Health Technol Inform. 2020;269:22–41. https://doi.org/10.3233/shti200020.
Dickason RM, Chauhan V, Mor A, Ibler E, Kuehnle S, Mahoney D, Armbrecht E, Dalawari P. Racial differences in opiate administration for pain relief at an academic emergency department. Western. J Emerg Med. 2015;16(3):372–80. https://doi.org/10.5811/westjem.2015.3.23893.
Hussain MI, Nelson AM, Yeung BG, Sukumar L, Zheng K. How the presentation of patient information and decision-support advisories influences opioid prescribing behavior: A simulation study. J Am Med Inform Assoc. 2020;27(4):613–20. https://doi.org/10.1093/jamia/ocz213.
Pomerleau AC, Perrone J, Hoppe JA, Salzman M, Weiss PS, Nelson LS. Impact of prior therapeutic opioid use by emergency department providers on opioid prescribing decisions. Western. J Emerg Med. 2016;17(6):791–7. https://doi.org/10.5811/westjem.2016.8.30965.
Spitz A, Moore AA, Papaleontiou M, Granieri E, Turner BJ, Reid MC. Primary care providers’ perspective on prescribing opioids to older adults with chronic non-cancer pain: A qualitative study. BMC Geriatr. 2011;11(1):35. https://doi.org/10.1186/1471-2318-11-35.
Chou R, Gordon DB, de Leon-Casasola OA, Rosenberg JM, Bickler S, Brennan T, Carter T, Cassidy CL, Chittenden EH, Degenhardt E, Griffith S, Manworren R, McCarberg B, Montgomery R, Murphy J, Perkal MF, Suresh S, Sluka K, Strassels S, et al. Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131–57. https://doi.org/10.1016/j.jpain.2015.12.008.
Ducharme J, Moore S. Opioid use disorder assessment tools and drug screening. Mo Med. 2019;116(4):318–24. https://pubmed.ncbi.nlm.nih.gov/31527982.
Fraenkel L, Falzer P, Fried T, Kohler M, Peters E, Kerns R, Leventhal H. Measuring pain impact versus pain severity using a numeric rating scale. J Gen Intern Med. 2012;27(5):555–60.
Kwong TC, Magnani B, Moore C. Urine and oral fluid drug testing in support of pain management. Crit Rev Clin Lab Sci. 2017;54(6):433–45. https://doi.org/10.1080/10408363.2017.1385053.
Pomerleau AC, Nelson LS, Hoppe JA, Salzman M, Weiss PS, Perrone J. The Impact of prescription drug monitoring programs and prescribing guidelines on emergency department opioid prescribing: a multi-center survey. Pain Med. 2017;18(5):889–97. https://doi.org/10.1093/pm/pnw032.
Chaudhary S, Compton P. Use of risk mitigation practices by family nurse practitioners prescribing opioids for the management of chronic nonmalignant pain. Subst Abus. 2017;38(1):95–104. https://doi.org/10.1080/08897077.2016.1265038.
Paulozzi LJ, Kilbourne EM, Desai HA. Prescription Drug monitoring programs and death rates from drug overdose. Pain Med. 2011;12(5):747–54. https://doi.org/10.1111/j.1526-4637.2011.01062.x.
Tournebize J, Gibaja V, Muszczak A, Kahn J-P. Are Physicians safely prescribing opioids for chronic noncancer pain? A systematic review of current evidence. Pain Pract. 2016;16(3):370-383. https://doi.org/10.1111/papr.12289.
Vila H Jr, Smith RA, Augustyniak MJ, Nagi PA, Soto RG, Ross TW, Cantor AB, Strickland JM, Miguel RV. The efficacy and safety of pain management before and after implementation of hospital-wide pain management standards: is patient safety compromised by treatment based solely on numerical pain ratings? Anesth Analg. 2005;101(2):474–80, table of contents. https://doi.org/10.1213/01.Ane.0000155970.45321.A8.
Rolin-Gilman C, Fournier B, Cleverley K. Implementing best practice guidelines in pain assessment and management on a women’s psychiatric inpatient unit: exploring patients’ perceptions. Pain Manag. Nurs. 2017;18(3):170–8. https://doi.org/10.1016/j.pmn.2017.03.002.
Tompkins DA, Hobelmann JG, Compton P. Providing chronic pain management in the "Fifth Vital Sign" Era: Historical and treatment perspectives on a modern-day medical dilemma. Drug Alcohol Depend. 2017;173 Suppl 1(Suppl 1):S11–s21. https://doi.org/10.1016/j.drugalcdep.2016.12.002.
Chou R, Deyo R, Devine B, Hansen R, Sullivan S, Jarvik JG, Blazina I, Dana T, Bougatsos C, Turner J. The effectiveness and risks of long-term opioid treatment of chronic pain. Evid Rep Technol Assess (Full Rep). 2014;(218):1–219. https://doi.org/10.23970/ahrqepcerta218.
Chou R, Hartung D, Turner J, Blazina I, Chan B, Levander X, McDonagh M, Selph S, Fu R, Pappas M. Opioid treatments for chronic pain. Comparative effectiveness review no. 229. (Prepared by the Pacific Northwest Evidence-based Practice Center under Contract No. 290-2015-00009-I.) AHRQ Publication No. 20-EHC011. Rockville, MD: Agency for Healthcare Research and Quality. 2020. https://doi.org/10.23970/AHRQEPCCER229.
Frieden TR, Houry D. Reducing the risks of relief—the CDC opioid-prescribing guideline. N Engl J Med. 2016;374(16):1501–4.
Berna C, Kulich RJ, Rathmell JP. Tapering long-term opioid therapy in chronic noncancer pain: evidence and recommendations for everyday practice. Mayo Clin Proc. 2015;90(6):828–42.
Phillips JL, Heneka N, Hickman L, Lam L, Shaw T. Can a complex online intervention improve cancer nurses’ pain screening and assessment practices? Results from a multicenter, pre-post test pilot study. Pain Manag Nurs. 2017;18(2):75–89.
Gaskin DJ, Arbelaez JJ, Brown JR, Petras H, Wagner FA, Cooper LA. Examining racial and ethnic disparities in site of usual source of care. J Natl Med Assoc. 2007;99(1):22–30.
Manuel JI. Racial/ethnic and gender disparities in health care use and access. Health Serv Res. 2018;53(3):1407–29.
Singh KA, Wilk AS. Affordable Care Act Medicaid expansion and racial and ethnic disparities in access to primary care. J Health Care Poor Underserved. 2019;30(4):1543–59. https://doi.org/10.1353/hpu.2019.0088.
Canedo JR, Miller ST, Schlundt D, Fadden MK, Sanderson M. Racial/ethnic disparities in diabetes quality of care: the role of healthcare access and socioeconomic status. J Racial Ethn Health Disparities. 2018;5(1):7–14.
Wheeler SM, Bryant AS. Racial and ethnic disparities in health and health care. Obstet Gynecol Clin North Am. 2017;44(1):1–11. https://doi.org/10.1016/j.ogc.2016.10.001.
Burgess DJ, Ding Y, Hargreaves M, van Ryn M, Phelan S. The association between perceived discrimination and underutilization of needed medical and mental health care in a multi-ethnic community sample. J Health Care Poor Underserved. 2008;19(3):894–911. https://doi.org/10.1353/hpu.0.0063.
National Institute on Drug Abuse. Massachusetts: opioid-involved deaths and related harms. 2020. Retrieved from https://www.drugabuse.gov/drug-topics/opioids/opioid-summaries-by-state/massachusetts-opioid-involved-deaths-related-harms. Accessed 2 March 2023.
Massachusetts Department of Public Health (2021). Opioid-related overdose deaths rose by 5 percent in 2020. https://www.mass.gov/news/opioid-related-overdose-deaths-rose-by-5-percent-in-2020
Funding
This work was funded by the Harvard Catalyst PFDI Faculty Fellowship from Harvard Medical School.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to the study conception and design. Michael Flores acquired the data and analyzed the data. All authors aided in data interpretation. All authors contributed to manuscript drafting and revised it critically for important intellectual content. All authors read and approved the final manuscript. All authors agree to be accountable for all aspects of the work ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Competing Interests
The authors have no relevant financial or non-financial interests to disclose.
Ethics Approval
This study was approved by the Institutional Review Board.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Flores, M.W., Sharp, A., Lu, F. et al. Examining Racial/Ethnic Differences in Patterns of Opioid Prescribing: Results from an Urban Safety-Net Healthcare System. J. Racial and Ethnic Health Disparities 11, 719–729 (2024). https://doi.org/10.1007/s40615-023-01555-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40615-023-01555-z