
Abstract
Background and aims
Gait speed estimation using wearable inertial sensors during daily activities suffers from high complexity and inaccuracies in distance estimation when integrating acceleration signals. The aim of the study was to investigate the agreement between the methods of gait speed estimation using the persons’ walk ratio (step-length/step-frequency relation) or step-frequency (number of steps per minute) and a “gold standard”.
Methods
For this cross-sectional validation study, 20 healthy community-dwelling older persons (mean age 72.1 years; 70% women) walked at slow, normal, and fast speed over an instrumented walkway (reference measure). Gait speed was calculated using the person’s pre-assessed walk ratio. Furthermore, the duration of walking and number of steps were used for calculation.
Results
The agreement between gait speed calculation using the walk ratio or step-frequency (adjusted to body height) and reference was r = 0.98 and r = 0.93, respectively. Absolute and relative mean errors of calculated gait speed using pre-assessed walk ratio ranged between 0.03–0.07 m/s and 1.97–4.17%, respectively.
Discussion and conclusions
After confirmation in larger cohorts of healthy community-dwelling older adults, the mean gait speed of single walking bouts during activity monitoring can be estimated using the person’s pre-assessed walk ratio. Furthermore, the mean gait speed can be calculated using the step-frequency and body height and can be an additional parameter in stand-alone activity monitoring.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Walking is a core activity of younger and older persons. Declining walking speed in older persons is associated with negative health outcomes, such as falls [1], frailty [2], hospital admission [3], and mortality [4]. Gait speed is increasingly discussed as the sixth vital sign [5].
There are differences in supervised walking speed assessed in the laboratory and non-supervised gait speed in the real-world environment [6]. Furthermore, assessment methods in the laboratory do not fully reflect real-world walking performance [7]. Therefore, gait speed should also be measured in natural environments to achieve ecological validity and to better understand activity and adaptability. Unfortunately, gait speed estimation using wearable inertial sensors during normal daily activities [8, 9] is influenced by contextual factors and other confounders adding to high complexity and potential inaccuracies in distance estimation when integrating acceleration signals.
So far, the step-frequency is used as a correlate of walking intensity and gait speed and to predict clinical outcomes [10, 11]. Analysing single walking bouts extracted from real-world measurements step-frequency gives further insight into the intensity of gait [12].
A simple method to estimate gait speed in healthy young persons in the free-living condition used the pre-assessed persons walk ratio and showed good agreement between the estimated gait speed and the gait speed measured by an odometer/speedometer combination [13]. The walk ratio represents the step-length/step-frequency relation, which is individually constant over a range of gait speeds [14, 15] and therefore may reflect spatiotemporal coordination of habitual gait during daily activities. Using the individual walk ratio from a laboratory assessment and using in addition the duration of a walking bout and the number of steps during this walking bout (representing step-frequency), free-living gait speed can be calculated. The latter parameters can be provided by wearable sensors during daily activity measurement [16, 17].
This study aims to test the feasibility of gait speed estimation using the persons walk ratio (proof-of-concept) in older adults. Furthermore, this concept of gait speed estimation was compared to the gait speed estimation using the step-frequency.
Methods
Subjects and design
For this cross-sectional validation study, healthy community-dwelling older persons were recruited among social volunteers in a south-west German hospital. The sample size for this feasibility study was set pragmatically [18]. Inclusion criteria were the age of 60 years or more and being able to walk without personal assistance. Exclusion criteria were neurologic diseases (self-report), acute pain affecting walking performance (self-report), poor vision (not recognizing markers on the ground), and terminal illness. All participants gave written informed consent. The study protocol was approved by the ethical committee of the Medical Faculty at the University of Tuebingen (240/2019BO2).
Gait analysis
Although the proposed method of gait speed estimation is intended to be used for data analysis of wearable sensors during activity monitoring, this proof-of-concept study uses an instrumented walk-way because of the high accuracy [19]. Nevertheless, for the estimation of gait speed only those parameters (duration of walking, number of steps) were used, which also can be measured by wearable sensors and which alone are not sufficient to calculate gait speed.
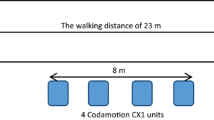
All gait analyses were performed on 8 m long instrumented walk-way (GAITRite, CIR Systems, Franklin NJ, USA). The validity of the system to measure spatiotemporal parameters, including gait speed, step-length, number of steps, heel strike and toe off, has been shown [19]. For the assessment of the persons´ walk ratio, they walked 3-times with normal speed over the walk-way. Thereafter, the person was instructed to walk once a bit slower than normal, once at normal speed and once a bit faster than normal. For each walk, the person walked 3 additional meters before and after the walk-way to exclude acceleration and deceleration effects during the measurements [20].
The person´s walk ratio of the first 3 walks (normal gait speed) was calculated as the step-length divided by step-frequency and the mean walk ratio [cm min] of these 3 walks was used for further calculations. For the next 3 walks (a bit slower than normal speed, normal speed, a bit faster than normal speed; i.e. simulation of free-living condition) the gait speed was estimated in 4 calculation steps using the person’s walk ratio (first 3 walks) and those parameters from the GAITRite system, which validly also could be measured by a wearable sensor system, i.e. duration of walking and number of steps:
-
1.
Step-frequency [steps/min] = number of steps/duration of walking
-
2.
Step-length [m] = walk ratio × step-frequency
-
3.
Distance of walking [m] = step-length × number of steps
-
4.
Mean gait speed [m/s] = distance of walking/duration of walking
These calculated gait speeds of three different target speeds (a bit slower than normal speed, normal speed, a bit faster than normal speed) were compared with the gait speed measured by the GAITRite system as the ground truth.
In order to describe the association between step-frequency and gait speed, these parameters measured by the GAITRite system during the last 3 walks (a bit slower than normal speed, normal speed, a bit faster than normal speed) were correlated.
Descriptive parameters
Person characteristics were described by age, sex, body weight, and height (self-report). The general health status was assessed by the Charlson Comorbidity Index [21] scoring 16 diseases with a weighted score value of 0 (best) to 33 (worst). In addition, the number of falls in the previous year was asked and classified to no fall, 1 or 2 falls or more than 2 falls. Habitual gait speed was used as a capacity marker of global physical performance [22]. The mean walk ratio [cm min], the mean stride-length variability [%], and the mean step-length difference [cm] of the first 3 walks (normal walking) were used as qualitative parameters describing walking performance [22]. The range of the walk ratio was calculated over all 6 walks on the walk-way. Furthermore, the use of walking aids was recorded.
Statistics
The manifestation of parameters was expressed as mean, 95% confidence interval (CI), minimum and maximum. The linear association between estimated and measured gait speed and between measured step-frequency and measured gait speed was expressed as Pearson´s coefficient of correlation. A linear regression model was used to explain the effect of step-frequency on gait speed. With regard to disagreement, CIs were used to show differences between measurements (ground truth versus calculation). All statistics were calculated by open access R-software, version 3.6.1.
Results
Twenty community-dwelling older persons (14 women, 70%) were recruited for the study. Fourteen (70%) reported no fall in the previous year. Five (25%) and 1 person (5%) reported 1 or 2 falls and more than 2 falls, respectively. None of them used a walking aid. The description of the persons in detail is shown in Table 1.
With regard to gait speed calculation using the walk ratio, the coefficient of correlation between ground truth and calculation was r = 0.98 (Fig. 1). Based on overlapping CIs there was no difference between measured (ground truth) and calculated gait speeds of slow, habitual, and fast walking. Absolute and relative mean differences/errors were smallest for habitual walking (0.03 m/s; 1.97%) and approximately doubled for slow and fast walking but were below 5%. For slow, habitual, and fast walking 4, 1 and 6 individual calculations, respectively, exceeded the 5% difference. The disagreement between ground truth and calculation was higher when the measured walk ratio differed from the pre-assessed walk ratio (first 3 walks). The results are shown in detail in Table 2.

Scatter plot of gait speed calculated using pre-assessed walk ratio and measured by GAITRite walk-way of all 20 community-dwelling older persons walking with normal gait speed, a bit slower and a bit faster (n = 60)
The coefficient of correlation between gait speed and step-frequency, both measured by GAITRite (slow, habitual, fast), was r = 0.85 and was r = 0.93 when step-frequency was adjusted to body height. A linear regression including step-frequency and body height as independent variables explained 85% of variation of gait speed. The resulting formula (1) of gait speed calculation was:
with V = gait speed, SF = step-frequency and H = body height.
Discussion
In this study, a healthy group of community-dwelling older adults with an unimpaired walking performance was investigated. The proper walking performance is based on an appropriate gait speed [23,24,25] and walk ratio [26], a low stride-length variability [25] and a small step-length difference [26], in total reflecting high capacity and quality of walking [22].
The general agreement between ground truth and gait speed calculated using the persons’ walk ratio was very high demonstrating the proof-of-concept of this method. The results are comparable to a study including younger persons [13]. Our suggested approach outperforms the method using step-frequency for gait speed calculation in our study. So far, the method appears valid for community-dwelling older adults with an unimpaired walking performance. The method should be confirmed in other clinical and multi-morbid geriatric cohorts to be applied in clinical studies.
If a gait analysis in a laboratory is included in a study protocol, the persons’ walk ratio can be used to calculate the mean gait speed of single walking bouts during activity monitoring. The added value would be that additional parameters, such as the median mean gait speed of all walking bouts, the range of gait speeds or the complexity of gait speed can be calculated and may provide further insight into real-world activity monitoring [22]. The predictive validity of these gait speed parameters concerning health-related parameters, such as mortality, hospital admission, mobility decline or others has to be shown in future studies. Furthermore, the results of these studies have to be compared to the existing literature with results gained by gait speed measurements in the laboratory. With regard to future falls, the predictive validity of gait quality parameters has already been shown [27].
There was a small, but considerable range of the walk ratio across target gait speeds negatively affecting the accuracy of gait speed calculation. A possible explanation could be that the test persons were advised to walk a bit slower or faster in the laboratory. This is supported by other studies [14, 15] with differing walk ratios at fixed advised gait speeds or step-frequencies and dual tasks. Since an instruction of walking speed during real-world activity monitoring is not likely, the accuracy of gait speed estimation by the proposed method might be even higher than in our study.
The method of gait speed calculation using step-frequency does not need an accompanying gait analysis. Agreement with ground truth was very high but was lower than the method using the walk ratio. Only body height is needed and can be asked from the person to be included into the gait speed calculation. For existing activity monitor systems, this method could easily be integrated to provide additional parameters, such as median, minimum, and maximum gait speed of walking bouts. Further accuracy may be obtained by measuring leg length instead of asking body height.
For this proof-of-concept study with intra-individual comparisons only, a normalization of the results to anatomical characteristics was not necessary. Nevertheless, a normalization is necessary for inter-individual comparison or when comparing different cohorts [28]. An example is a comparison between men and women, because gait kinematics are different in both groups [29].
It is a limitation that our results are valid only for healthy community-dwelling older adults with an unimpaired walking performance. Future studies should test this method in larger patient cohorts and in geriatric patients representing lower, mid and upper level gait disorders and multifactorial gait disorders. Relevant examples are hip fracture and osteoarthritis patients with a potentially higher step-length difference [26] or Parkinson`s disease and normal pressure hydrocephalus where a lower walk ratio might be expected [30, 31] and persons with higher stride-length variability. Although the walking performance is likely impaired in these cohorts, our proposed method of gait speed calculation might still be acceptable, because of lower resources to change/adapt walking in these cohorts and so affecting the walk ratio. Another limitation is the fact that only the mean gait speed can be calculated by this method suggesting steady-state walking. Our method might be still acceptable, because longer walking bouts, characterized by lower variability of step-frequency/gait intensity and reflecting “purposeful walking”, are more interesting in this context [12]. These longer walking bouts are less affected by acceleration and deceleration of walking. Furthermore, this method of gait speed estimation is intended to be used in the real-world environment (activity monitoring) with wearable sensors but was tested for the “proof-of-concept” in a laboratory setting. Thus, the accuracy of gait speed estimation with wearable sensors relies on the accuracy of these sensors to detect the duration of walking and the number of steps. Unfortunately, there is no gold standard of gait speed measurement during daily life to compare with the proposed method. Therefore, the development of an accurate and continuous measurement of gait speed during a walking bout is desirable.
Conclusion
After confirmation in larger cohorts of healthy community-dwelling older adults, the mean gait speed of single walking bouts during activity monitoring can be estimated using the person’s pre-assessed walk ratio. Furthermore, the mean gait speed can be calculated using the step-frequency and body height and can be an additional parameter in stand-alone activity monitoring.
Availability of data and materials
The datasets generated during this study are not publicly available but are available from the corresponding author on reasonable request.
Code availability
Not applicable.
References
Quach L, Galica AM, Jones RN et al (2011) The nonlinear relationship between gait speed and falls: the maintenance of balance, independent living, intellect, and zest in the elderly of Boston Study. J Am Geriatr Soc 59:1069–1073
Schoon Y, Bongers K, Van Kempen J, Melis R, Olde Rikkert M (2014) Gait speed as a test for monitoring frailty in community-dwelling older people has the highest diagnostic value compared to step length and chair rise time. Eur J Phys Rehabil Med 50:693–701
Cesari M, Kritchevsky SB, Penninx BWJH et al (2005) Prognostic value of usual gait speed in well-functioning older people–results from the health, aging and body composition study. J Am Geriatr Soc 53:1675–1680
Studenski S, Perera S, Patel K et al (2011) Gait speed and survival in older adults. JAMA 305:50–58
Fritz S, Lusardi M (2009) White paper: “walking speed: the sixth vital sign”. J Geriatr Phys Ther 32:46–49
Foucher KC, Thorp LE, Orozco D, Hildebrand M, Wimmer MA (2010) Differences in preferred walking speeds in a gait laboratory compared with the real world after total hip replacement. Arch Phys Med Rehabil 91:1390–1395
Stellmann JP, Neuhaus A, Götze N et al (2015) Ecological validity of walking capacity tests in multiple sclerosis. PLoS One 10:e0123822
Moe-Nilssen R, Helbostad JL (2004) Estimation of gait cycle characteristics by trunk accelerometry. J Biomech 37:121–126
Zijlstra W (2004) Assessment of spatio-temporal parameters during unconstrained walking. Eur J Appl Physiol 92:39–44
Tudor-Locke C, Aguiar EJ, Han H et al (2019) Walking cadence (steps/min) and intensity in 21–40 year olds: CADENCE-adults. Int J Behav Nutr Phys Act 16:8
Brown JC, Harhay MO, Harhay MN (2014) Walking cadence and mortality among community-dwelling older adults. J Gen Intern Med 29:1263–1269
Granat M, Clarke C, Holdsworth R, Stansfield B, Dall P (2015) Quantifying the cadence of free-living walking using event-based analysis. Gait Posture 42:85–90
Schimpl M, Lederer C, Daumer M (2011) Development and validation of a new method to measure walking speed in free-living environments using the actibelt® platform. PLoS ONE 6:e23080
Bogen B, Moe-Nilssen R, Ranhoff AH, Aaslund KM (2018) The walk ratio: investigation of invariance across walking conditions and gender in community-dwelling older people. Gait Posture 61:479–482
Egerton T, Danoudis M, Huxham F, Iansek R (2011) Central gait control mechanisms and the stride length—cadence relationship. Gait Posture 34:178–182
Paraschiv-Ionescu A, Buchser EE, Rutschmann B, Najafi B, Aminian K (2004) Ambulatory system for the quantitative and qualitative analysis of gait and posture in chronic pain patients treated with spinal cord stimulation. Gait Posture 20:113–125
Taraldsen K, Askim T, Sletvold O et al (2011) Evaluation of a body-worn sensor system to measure physical activity in older people with impaired function. PhysTher 91:277–285
Thabane L, Ma J, Chu R et al (2010) A tutorial on pilot studies: the what, why and how. BMC Med Res Methodol 10:1
Cutlip RG, Mancinelli C, Huber F, DiPasquale J (2000) Evaluation of an instrumented walkway for measurement of the kinematic parameters of gait. Gait Posture 12:134–138
Lindemann U, Najafi B, Zijlstra W et al (2008) Distance to achieve steady state walking speed in frail elderly persons. Gait Posture 27:91–96
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Lindemann U (2020) Spatiotemporal gait analysis of older persons in clinical practice and research: which parameters are relevant? Z Gerontol Geriatr 53:171–178
Aboutorabi A, Arazpour M, Bahramizadeh M, Hutchins SW, Fadayevatan R (2016) The effect of aging on gait parameters in able-bodied older subjects: a literature review. Aging Clin Exp Res 28:393–405
Bohannon RW (1997) Comfortable and maximum walking speed of adults aged 20–79 years: reference values and determinants. Age Ageing 26:15–19
Hollman JH, McDade EM, Petersen RC (2014) Normative spatiotemporal gait parameters in older adults. Gait Posture 34:111–118
Thingstad P, Egerton T, Ihlen EF, Taraldsen K, Moe-Nilssen R, Helbostad JL (2015) Identification of gait domains and key gait variables following hip fracture. BMC Geriatr 15:150
Van Schooten KS, Pijnappels M, Rispens SM et al (2016) Daily-life gait quality as predictor of falls in older people: a 1-year prospective cohort study. PLoS ONE 11:e0158623
Moe-Nilssen R, Helbostad JL (2020) Spatiotemporal gait parameters for older adults—an interactive model adjusting reference data for age, gender, and body height. Gait Posture 82:220–226
Bruening DA, Frimenko RE, Goodyear CD, Bowden DR, Fullenkamp AM (2015) Sex differences in whole body gait kinematics at preferred speeds. Gait Posture 41:540–545
Morris ME, Iansek R, Matyas TA, Summers JJ (1994) The pathogenesis of gait hypokinesia in Parkinson’s disease. Brain 117:1169–1181
Relkin N, Marmarou A, Klinge P, Bergsneider M, Black PM (2005) Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery 57(3 Suppl):S4-16
Acknowledgements
We thank Lara Popp for data collection.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Data collection and analysis were performed by UL and JK. The first draft of the manuscript was written by UL, LS and JK and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Clemens Becker has received consultant fees from E. Lilly company and Bosch Health care. He has also received speaker honoraria from Amgen and Nutricia. Lars. Schwickert has received consultant fees from Rölke Pharma GmbH. On behalf of all other authors, the corresponding author states that there is no conflict of interest.
Ethical approval
The study was performed in accordance with the 1964 Helsinki Declaration and its later amendments. This article does not contain any studies with animals performed by any of the authors. The study protocol was approved by the ethical committee of the University of Tuebingen (240/2019BO2).
Informed consent
All participants of this project gave written informed consent for data analysis and publication.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lindemann, U., Schwickert, L., Becker, C. et al. Estimate of gait speed by using persons’ walk ratio or step-frequency in older adults. Aging Clin Exp Res 33, 2989–2994 (2021). https://doi.org/10.1007/s40520-021-01832-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-021-01832-z