
Abstract
Background
Gait patterns of healthy aging are needed to allow a comparison with pathological situations. However, little data is available.
Objective
To present gait pattern of healthy older specially selected to be “healthy walkers”.
Method
Fifty-seven older people benefited from a geriatric assessment including clinical and functional evaluations to include only those without gait disorders. Gait data were simultaneously recorded using a tri-axial accelerometer placed on the waist and four 3D position markers placed on the feet at the level of the heel and the toe. Volunteers walked at comfortable self-selected speed (CW), fast self-selected speed (FW), and finally in dual task walking condition (DTW). The extracted gait parameters were: gait speed, stride length, stride frequency, regularity and symmetry, swing, stance and double support time and ratio and minimum toe clearance. Gait speed and stride length were normalized to the right leg length.
Results
Fifty-seven older people with a mean age of 69.7 ± 4.2 years old (range from 65 to 82 years) were included. Data were analyzed according to the gender and according to the age (<70 or ≥70 years old). After normalization to leg length, the main significant differences were shown for stride length and minimum toe clearance in CW, FW and in DTW that were shorter in women. The regularity in FW was significantly lower among older volunteers.
Conclusions
This work provides a data set considering 14 gait parameters obtained from 57 healthy old people strictly selected and assessed for three walking conditions and shows that GS, SL and MTC have to be related to the gender. The age-related impact on gait performances appears reduced in this cohort.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Trunk accelerometers have been described as reliable tools for human gait analysis outside the laboratory (i.e. in clinical environment) [1–4]. They offer many advantages such as an easy handling and a low-cost technology. Furthermore, pilot studies have previously shown their accuracy to differentiate the gait profiles from cognitively healthy and cognitively impaired older people [5, 6]. Unfortunately, reference data obtained with this method for healthy older people and comparison with gold standard laboratories methods like optoelectronic systems are still lacking. Nevertheless and considering the growing interest using the gait pattern as a marker of risk of negative clinical outcomes or as a marker of robustness and to use this to suggest specific drugs, intervention or rehabilitation, the development of such database seems essential as a reference to pathological conditions analysis. Several impediments explain this lack of available literature.
A few papers show reference data but some important clinical information is missing (e.g. functional status, cognitive performance, mood disorders, medications, and previous falls) to check the global and complete health status of the patients. Additionally, in several papers about specific gait conditions (e.g. Parkinson’s disease), control volunteers are selected based on the absence of the pathology of interest but mostly without considering health-related criteria. In 2011, Hollman et al. published a notable reference data set showing 23 gait parameters from healthy older adults assessed in comfortable walking condition (CW) and using a 5.6 m electronic walkway [7]. However, some motion and gait analysis laboratories are equipped with other instrumental systems, then showing gait data obtained with other instrumental methods could be useful and could allow comparing the results from different data acquisitions and data process. Another issue is the lack of mention or adjustment to the height, known to influence gait speed and stride length [8, 9]. Finally, some papers highlight the importance to consider not only the CW but also the dual task walking condition (DTW) and the fast walking condition (FW). Considering all these aspects, the aim of this study is to assess the gait pattern of healthy old people during these three clinically relevant walking conditions (CW,FW and DTW) using simultaneously an accelerometer and an opto-electronic method and to show gait parameters normalized to the leg length. This study would provide accurate gait pattern of healthy old people and help other researchers to compare these data to their own. Finally, the authors will compare their results to those of Hollman et al.
Methodology
Population
Volunteers were selected from a prospective study aiming to clarify the interest of gait analysis associated to brain imaging to earlier discern old people at risk of cognitive decline and falls, the Gait Analysis and Brain Imagery Study (GABI Study).
Inclusion criteria
To be at least 65 years old, living independently at home, to understand French, to be able to reach the motion analysis laboratory, to approve inform consent.
Exclusion criteria
Exclusion criteria included fall in the previous year, history of stroke, physiotherapeutic cares, recent hip or knee prosthesis (≤1 year), musculoskeletal pain during walking, Timed Up and Go (TUG) longer than 10 s, an acute respiratory or cardiac illness (<6 month), cognitive disorders according to the MoCA score (<26/30), mood disorder according GDS-4 (people with a score of 2/ were included were the score was linked to the status of proxy and the fear to become ill because of this responsibility of caregiving), frailty according to the Edmonton score (>5/17) and neoplasm (people with a cancer in remission since more than 5 years were included).
Clinical and functional assessment
Subjects were assessed for socio-demographic and anthropometric data and benefited from a complete functional assessment (Table 1). The ADL and IADL scale scores were calculated to confirm the independency of included volunteers. Considering that some housework are usually and preferentially done by the same member of the family (e.g. the gardening or the meals), the IADL score was calculated by considering the sum of the results obtained in the items applicable to each subject, divided by the sum of the maximum possible scores in the applicable items (to not consider the volunteer disable for a housework he or she never did).
Materials
During walking test all subjects were assessed using simultaneously two validated methods to collect data; a triaxial accelerometer (Locometrix®) and an optoelectronic device (CodaMotion®). Combined together, these two methods are used to assess 14 parameters frequently shown in the literature and clinically relevant regarding the adverse clinical age-related outcomes (e.g. the fall risk). To our knowledge, this is the first published work using simultaneously these two methods.
The accelerometric system (Locometrix®, Centaure Metrix, Evry, France) is a validated method [2] comprising an acceleration sensor, a recording device and a computer program for processing the acceleration signal. The acceleration sensor is composed of three accelerometers placed perpendicularly to each other in a plastic box with the recording device. The sensor’s box is incorporated in an elastic abdominal belt, behind the back over the L3–L4 intervertebral lumbar space (the 3rd lumbar vertebra level). The acquisition frequency of the signal is 100 Hz.
The Codamotion® system (Charnwood Dynamics, Rothley, UK) is a 3-dimensional kinematic tool validated for its use in laboratory [10–12]. The 3-dimensional position and orientation of the feet were tracked using four Codamotion CX1 units at a sampling rate of 200 Hz. Two position markers were attached on each shoe of the volunteers; one on the heel and one on the toe. These four position markers give accurate measurements of the position of the feet in 3D in the Codamotion® system covers 4 to 5 stride cycles (depending on the subject and the walking condition). See Fig. 1.

Plan and organization of the motion laboratory and walking distances the volunteers has to walk for each walking condition (CW, FW and DTW) in one way
Gait tests
Clinical and functional assessments were realized by the same examiner. Subjects were asked to wear comfortable shoes. After familiarization and once the subject equipped, gait was recorded under three different experimental conditions: self-selected comfortable walking speed (CW) (to assess spontaneous gait pattern), self-selected fast walking speed (FW) (because its relevance considering the relationship to the risk of cognitive decline [13, 14] and disability [15]) and during dual-task walking condition (DTW) (because of the spread brain areas and neuronal networks implicated in gait disturbances and associated to normal aging [16] and considering his relationship to the cognitive decline [5, 6] and to the disability [17]). The instruction for FW was “walk quickly without running in order not to miss your train” and for DTW “walk at a comfortable walking speed while simultaneously making arithmetic (seven counting down since the number “100” to increase gait pattern modifications [18]). Because explicit instruction concerning the prioritization could affect dual tasking [19], the single instruction gave to the volunteers was “make both tasks simultaneously and as well as you can”. The CW was always the first walking condition done. The order of fast and dual-task walking was randomized to avoid a systematic measurement error. The starting point was on the left side of the Fig. 1. The volunteer has to walk 5 m to increase their walking speed and reach a walking steady state. The examiner starts the stopwatch when the first foot of the volunteer cross the time line. Time needed to walk 23 m is assessed. The last 5 m are used to decrease the walking gait and stop. In the middle of the 23 m, four position cameras allow computing the position of heels and toes on 8 m.
Data processing
Concerning Locometrix®, the mean gait speed (GS) was computed from the time needed to cover 23 m. Time was recorded by means of a stopwatch. The following gait variables were inferred from the walking speed and 20.48 s of stationary cranial-caudal acceleration signal:
-
the stride frequency (SF) or number of cycles per second (Hz) was calculated from the cranio-caudal acceleration following the application of the Fourier transform,
-
the stride length (SL) was deduced from the equation [speed (m/s) = frequency (Hz) × stride length (m)] and expressed in meters.
-
the stride regularity and symmetry were automatically derived from two coefficients (C1 and C2) computed from an autocorrelation function on the cranial-caudal signal. The autocorrelation coefficients C1 and C2 quantify the peak values of the first and second dominant periods of the autocorrelation function, respectively, corresponding to the step regularity and to the stride regularity [1]. These coefficients are automatically transformed according to equations detailed in the paper of Auvinet et al. [2]. Regularity and symmetry indexes are dimensionless. The regularity index describes the similarity of vertical movements over successive strides. The symmetry index describes the similarity of left and right cranial-caudal movements and it is independent of fluctuations in the successive movement of each limb.
The Codamotion® system is used to measure reference kinematic signals: the vertical (horizontal) heel position Z h (X h) and the vertical (horizontal) toe position Z t (X t). A signal-processing algorithm is then applied to these signals to extract—during consecutive strides—gait events of importance: the heel strike (HS) and the toe off (TO). This algorithm is based on a piecewise linear fitting method [20] that identifies accurately HS and TO in local position signals. Temporal gait parameters are extracted based on these gait events as follows:
-
Stance Time (StT) (time between HS and TO during stride i) = TO(i) − HS(i).
-
Swing Time (SwT) (time between TO of stride i and HS of stride i + 1) = HS(i + 1) − TO(i).
-
Right double support duration [time between left HS (HSleft) and right TO (TOright) during stride i] = TOright(i) − HSleft(i).
-
Left double support duration [time between right HS (HSright) and left TO (TOleft) during stride i] = TOleft(i) − HSright(i).
The time of minimum toe clearance (MTC) is extracted as being the moment at which the toe reaches a local minimal vertical position during the swing phase.
In fact the Codamotion® system also allows extracting GS, SL and SF. However, considering the longer walking distance covered by the accelerometric method (23 m compare to 8 m using the Codamotion® system), the authors will consider and present GS, SL and SF measured using the accelerometric method.
Considering the potential confounder effect of the height on the gait speed and the stride length and to decrease the gender effect (considering that men are often higher than women), these gait parameters were normalized to the length of the right lower limb (measured to the trochanter until the heel) as the following formula: “normalized gait parameter = (gait parameter/right leg length) × 100”.
Statistical analysis
Statistical analyses were performed using Statistica 13 (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP.) and MATLAB R2013a (Math Works, Natick, MA). Clinical parameters were expressed as mean ± standard deviation (SD), median, percentile 25 (P25), percentile 75 (P75), minimal and maximal values. Gait parameters obtained considering the left and the right side (double support, stance and swing time) were expressed as the mean values of both sides. Left and right measures were previously checked to be not significantly different side by side using the Student’s paired t test. Normality was tested using the Shapiro–Wilk test and investigating mean and median values, histograms and Quantile–Quantile plots. Homoscedasticity was tested using the Levenne test. Paired off groups were compared using the Welch–Satterthwaite t test. Results were considered significant at the 5% critical level (p value <0.05). 95% confidence intervals (CI 95%) for means were also calculated for men and women. Intra-class coefficient correlation (ICC) (2, k) were additionally calculated for gait parameters both extracted by the Locometrix® and the Codamotion® system.
Results
Characteristics of the population
After applying severe exclusion criteria (see previously), 57 healthy old people were included. Table 1 shows the main clinical and functional characteristics of the 57 selected subjects, including 25 men (43.86%) and 32 women (56.14%). Mean age was 69.7 ± 4.2 years old. The group of volunteers <70 years old included 44 persons (with 25 women) and the group of volunteers ≥70 years old included 23 persons (with seven women). All volunteers realized the TUG faster than 10 s. Median values highlighted the high physical and functional performances of the group.
Gait parameters
The 14 gait parameters obtained from CW including “normalized gait parameters” are presented considering the gender in the Table 2. During CW, the GS (p = 0.002), the SL (p < 0.001), the NSL (p = 0.002) and the MTC (p < 0.001) showed a significant difference according to the gender. Gait parameters obtained in FW are presented in the Table 3. During FW, the GS (p < 0.001), the SL (p < 0.001), the NSL (p < 0.001), the SF (p = 0.019), the SwT (p = 0.002), the MTC (p < 0.001) and the StT (p = 0.018) showed a significant difference according to the gender.
Gait parameters obtained in DTW are presented in the Table 4. During DTW, the GS (p = 0.028), the SL (p = 0.007) and the MTC (p < 0.001) showed a significant difference between groups according to the gender.
The REG in FW showed a significant difference according to the age (p = 0.049) with a mean = 327 and a SD = 47 among volunteers <70 years old and with a mean = 301 and a SD = 48 among oldest group. Considering all walking conditions, no other parameter showed a significant clinical or statistical difference according to the age.
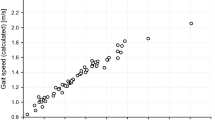
Concerning the consistency between gait parameters both extracted by the two methods. ICC (2, k) considering GS were 0.94 in CW, 0.91 in FW and 0.96 in DTW. ICC considering SL were 0.96 in CW, 0.94 in FW and 0.80 in DTW. ICC considering SF were 0.96 in CW, 0.87 in FW and 0.82 in DTW.
Discussion
Briefly, this work provides gait patterns of healthy old people selected with great care and assessed for three different walking conditions widely used in research and clinical settings. For each walking condition, 14 gait parameters, chosen because of their clinical relevance, are presented considering gender. To not underestimate age-related gait modifications and according to the median age reached by this cohort, the authors divided the cohort in two groups; one including volunteers <70 years old and another group including those ≥70 years old. Furthermore, to decrease the gender effect due to the height, the most height-dependent-gait parameters like GS and SL were showed as “raw data” but also as “normalized data”. Then researchers could easily compare this data set to the gait pattern obtained in their own cohort.
After a first look, an important observation to do is that the same gait parameters (GS, the SL, the normalized SL and the MTC) show a difference according to the gender in the three walking conditions (except for the NSL in DTW). This observation underlies the relevance of these parameters and the reliability of the data acquisitions. In FW the SwT and the StT presented statistical differences between groups (p value <0.05), but these numerical differences remain skinny and clinically irrelevant. Of course, some other clinical variables could partially explain the observed difference between the groups but the normalization to right leg length and the strict selection of the volunteers, applying several exclusion criteria, has limited potentials confounders.
In CW, the GS, the SL, the SF obtained from trunk accelerations are comparable to those published by Auvinet et al. [2], Senden et al. [8, 9] and Ko et al. [21], where men are faster than women and they show longer stride length. However, applying the normalization to the leg length, this study showed a difference according to the gender only for SL (and normalized SL).
The REG and SYM are similar in both gender as previously showed by Auvinet et al., Senden et al. and Patterson et al. [22].
The MTC shown in this study are consistent with the MTC obtained by Dadashi et al. [23]. Nevertheless, the MTC showed in the Swiss study did not show a difference according to the gender. In our opinion, the overall precision of 9 mm of the inertial extraction method used (not allowing to measure a difference <9 mm as recorded in our sample) could explain these differences in the results shown.
After comparison with the results published by Hollman and even if he used another instrumental method, our results are similar. Indeed, in the Hollman study, men were faster than women and their stride length were longer. In the same line, the swing ratio and the stance ratio are similar in the two studies. The double support time and ratio expressed in the Hollman study express the sum of the double support ratio of the left and the right step. In our study, the double support time and ratio were assessed stride by stride, that could explain the difference (almost twice more) shown in the two studies. Actually Hollman and al. showed an influence of age on gait performances. Conversely this work did not find the same results. Two components could explain this inconsistency; first the small size of our cohort and the small number of very old volunteers (only two people older than 80) furthermore the lower proportion of women (slower than men and with shorter stride length) included in the ≥70 years old group could hide the age-related impact on gait speed and stride length. Nevertheless, the consistency of the two studies agrees with the reliability and the validity of the gait parameters assessed and the data acquisition protocol used.
In FW, our results are similar to those founded by Laufer using the GaitRite walkway system [24]. The DSR is lower in our cohort (around 14 and 12% of the stride time during CW and FW, respectively) than in the Laufer’s cohort (30 and 25%, respectively). However, the reductions of DSR secondary to the increase of GS were similar in the two populations (reduction of 17% in Laufer’s cohort and reduction of 15% in our cohort).
In DTW, and as found by van Iersel et al. [25], Hausdorff et al. [26] and Yogev-Seligmann et al. [19], GS decreases during dual tasking even for old people free of cognitive disorder. Interestingly in DTW, the normalized SL did not remain significantly different in both gender (like in CW and FW). Even if the mean values between the two groups are high, the higher SD in men than in women could explain this statistical result (related to the sample size effect). Unfortunately, this work has some limitations to take into account. The sample size was modest because of several exclusion criteria and the cost of the cognitive task was not accounted for. Finally, due to the limited number of available CX1 measurement units, only 8 meters of stabilized walk are available for gait analysis based on the opto-electronic method (meaning 4 or 5 gait cycles/each volunteer). Nevertheless, the excellent ICC concerning gait parameters measured by the two instrumental methods and the consistency between our results and those previously published (even those obtained using other instrumental methods) confirm the reliability of data acquisition and data analysis used in this work.
Finally, even considering to the small size of the cohort, the limited age-related gait modifications showed in this work is, in our opinion, an important fact to underline. Indeed, these results support the idea that people with gait disorders have to benefit at least of a clinical examination to detect some pathological condition linked to the gait performances and so even in case of advanced age.
Conclusion
This work provides a data set of gait parameters obtained from 57 healthy old people assessed for three walking conditions using a tri-axial accelerometer and an optoelectronic method allowing researchers to compare with their own data. In healthy old people, the gait speed, the stride length and the minimal toe clearance have to be related to the gender. The age-related impact on gait performances appears reduced in this cohort. The strict selection of the old people included and the consistency with previous published data allow considering the present data set as reference values.
Abbreviations
- CW:
-
Comfortable walking condition
- FW:
-
Fast walking condition
- GS:
-
Gait speed
- DSR:
-
Double support ratio
- DST:
-
Double support time
- DTW:
-
Dual task walking condition
- MTC:
-
Minimum toe clearance
- NGS:
-
Normalised GS
- NSL:
-
Normalised SL
- REG:
-
Regularity
- StR:
-
Stance ratio
- SwR:
-
Swing ratio
- StT:
-
Stance time
- SwT:
-
Swing time
- SF:
-
Stride frequency
- SL:
-
Stride length
- SYM:
-
Symmetry
References
Moe-Nilssen R, Helbostad JL (2004) Estimation of gait cycle characteristics by trunk accelerometry. J Biomech 37:121–126. doi:10.1016/S0021-9290(03)00233-1
Auvinet B, Berrut G, Touzard C et al (2002) Reference data for normal subjects obtained with an accelerometric device. Gait Posture 16:124–134. doi:10.1016/S0966-6362(01)00203-X
Bautmans I, Jansen B, Van Keymolen B et al (2011) Reliability and clinical correlates of 3D-accelerometry based gait analysis outcomes according to age and fall-risk. Gait Posture 33:366–372. doi:10.1016/j.gaitpost.2010.12.003
Hartmann A, Luzi S, Murer K et al (2009) Concurrent validity of a trunk tri-axial accelerometer system for gait analysis in older adults. Gait Posture 29:444–448. doi:10.1016/j.gaitpost.2008.11.003
Gillain S, Warzee E, Lekeu F et al (2009) The value of instrumental gait analysis in elderly healthy, MCI or Alzheimer’s disease subjects and a comparison with other clinical tests used in single and dual-task conditions. Ann Phys Rehab Med 52:453–474. doi:10.1016/j.rehab.2008.10.004
Gillain S, Dramé M, Lekeu F et al (2015) Gait speed or gait variability, which one to use as a marker of risk to develop Alzheimer disease? A pilot study. Aging Clin Exp Res 28:249–255. doi:10.1007/s40520-015-0392-6
Hollman JH, McDade EM, Petersen RC (2011) Normative spatiotemporal gait parameters in older adults. Gait Posture 34 (1):111–118. doi:10.1016/j.gaitpost.2011.03.024
Senden R, Grimm B, Heyligers IC et al (2009) Acceleration-based gait test for healthy subjects: Reliability and reference data. Gait Posture 30:192–196. doi:10.1016/j.gaitpost.2009.04.008
Senden R, Meijer K, Heyligers IC et al (2012) Importance of correcting for individual differences in the clinical diagnosis of gait disorders. Physiotherapy 98:320–324. doi:10.1016/j.physio.2011.06.002
Gorton Iii GE, Hebert DA, Gannotti ME (2009) Assessment of the kinematic variability among 12 motion analysis laboratories. Gait Posture 29:398–402. doi:10.1016/j.gaitpost.2008.10.060
O’Sullivan K, O’Sullivan L, Campbell A et al (2012) Towards monitoring lumbo-pelvic posture in real-life situations: concurrent validity of a novel posture monitor and a traditional laboratory-based motion analysis system. Man Ther 17:77–83. doi:10.1016/j.math.2011.09.006
Schwartz C, Denoël V, Forthomme B et al (2015) Merging multi-camera data to reduce motion analysis instrumental errors using Kalman filters. Comput Methods Biomech Biomed Eng 18:952–960. doi:10.1080/10255842.2013.864640
Deshpande N, Metter EJ, Bandinelli S et al (2009) Gait speed under varied challenges and cognitive decline in older persons: a prospective study. Age Ageing 38:509–514. doi:10.1093/ageing/afp093
Fitzpatrick AL, Buchanan CK, Nahin RL et al (2007) Associations of gait speed and other measures of physical function with cognition in a healthy cohort of elderly persons. J Gerontol Ser A Biol Sci Med Sci 62:1244–1251
Artaud F, Singh-Manoux A, Dugravot A et al (2015) Decline in fast gait speed as a predictor of disability in older adults. J Am Geriatr Soc 63:1129–1136. doi:10.1111/jgs.13442
Scherder E, Eggermont L, Swaab D et al (2007) Gait in ageing and associated dementias; its relationship with cognition. Neurosci Biobehav Rev 31:485–497. doi:10.1016/j.neubiorev.2006.11.007
Verghese J, Holtzer R, Lipton RB et al (2012) Mobility stress test approach to predicting frailty, disability, and mortality in high-functioning older adults. J Am Geriatr Soc 60:1901–1905. doi:10.1111/j.1532-5415.2012.04145.x
Montero-Odasso M, Muir SW, Speechley M (2012) Dual-task complexity affects gait in people with mild cognitive impairment: the interplay between gait variability, dual tasking, and risk of falls. Arch Phys Med Rehabil 93:293–299. doi:10.1016/j.apmr.2011.08.026
Yogev-Seligmann G, Rotem-Galili Y, Mirelman A et al (2010) How does explicit prioritization alter walking during dual-task performance? Effects of age and sex on gait speed and variability. Phys Ther 90:177–186. doi:10.2522/ptj.20090043
Boutaayamou M, Schwartz C, Stamatakis J et al (2015) Development and validation of an accelerometer-based method for quantifying gait events. Med Eng Phys 37:226–232. doi:10.1016/j.medengphy.2015.01.001
Ko S-u, Tolea MI, Hausdorff JM et al (2011) Sex-specific differences in gait patterns of healthy older adults: results from the baltimore longitudinal study of aging. J Biomech 44:1974–1979. doi:10.1016/j.jbiomech.2011.05.005
Patterson KK, Nadkarni NK, Black SE et al (2012) Gait symmetry and velocity differ in their relationship to age. Gait Posture 35:590–594. doi:10.1016/j.gaitpost.2011.11.030
Dadashi F, Mariani B, Rochat S et al (2014) Gait and foot clearance parameters obtained using shoe-worn inertial sensors in a large-population sample of older adults. Sens Basel Sens 14:443–457. doi:10.3390/s140100443
Laufer Y (2005) Effect of age on characteristics of forward and backward gait at preferred and accelerated walking speed. J Gerontol Ser A Biol Sci Med Sci 60:627–632. doi:10.1093/gerona/60.5.627
van Iersel MB, Ribbers H, Munneke M et al (2007) The effect of cognitive dual tasks on balance during walking in physically fit elderly people. Arch Phys Med Rehabil 88:187–191. doi:10.1016/j.apmr.2006.10.031
Hausdorff JM, Schweiger A, Herman T et al (2008) Dual-task decrements in gait: contributing factors among healthy older adults. J Gerontol Ser A Biol Sci Med Sci 63:1335–1343
Acknowledgements
The authors would like to thank the Dr. Sophie Christelbach and Ms Vinciane Wojtasik for helping with the volunteers recruitment and the Drs. Claire Geurten and Xavier Schmitz for helping with data acquisition. This study was supported by a Grant from the Belgian fund for scientific research (F.N.R.S.).
Author contribution statement
SG: concept and design of the study, data acquisition, presentation and discussion of the results, writing. MB: data extraction, statistical analysis, discussion of the results, writing. ND: statistical analysis, writing. CS: data acquisition, data extraction, discussion of the results, writing. MD: data acquisition, data extraction, discussion of the results, writing. CG: data acquisition, writing. FD: data acquisition, writing, corrections as native speaker. ES: concept and design of the study, methodological advice, writing. GG: concept and design of the study, methodological advice, writing. OB: concept and design of the study, methodological advice, writing. OB: concept and design of the study, methodological advice, writing. JLC: concept and design of the study, methodological advice, writing. JP: concept and design of the study, methodological advice, writing.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors disclose any financial and personal relationships with other people or organization that could inappropriately influence their work.
Statement of human and animal rights
The medical ethical committee of the University hospital of Liège (CHU Liège, Belgium) approved the protocol.
Informed consent
All participants signed inform consent.
Rights and permissions
About this article

Cite this article
Gillain, S., Boutaayamou, M., Dardenne, N. et al. Data set of healthy old people assessed for three walking conditions using accelerometric and opto-electronic methods. Aging Clin Exp Res 29, 1201–1209 (2017). https://doi.org/10.1007/s40520-017-0730-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-017-0730-y