
Abstract
Background
The timed up and go (TUG) test assesses balance and mobility performance.
Aim
This study aims to investigate the association between TUG time and mortality in Japanese older persons and to clarify possible moderation effects on mortality and TUG time.
Methods
In all, 874 participants who were ≥ 65 years of age completed the TUG test and had their anthropometric parameters and physical functions measured. We investigated the association between all-cause mortality and TUG using a Cox regression model that included confounders, and explored the time associated with mortality using a restricted cubic spline. We also performed subgroup analyses to explore whether age, sex, and body mass index (BMI) affected the relationship between TUG time and mortality.
Results
The median age and mean follow-up period were 74 and 8.5 years, respectively. Median TUG time was 7.4 s and the prevalence of mortality was 25.7%. TUG time in one second was positively associated with an increased risk of total mortality [hazard ratio (HR): 1.054 (1.016–1.093); P = 0.005] in the Cox regression model. The positive association of mortality and TUG time was present when the TUG was over 10.5 s in the restricted cubic spline curve. Older age (75 years or older) moderated the relationship between TUG time and mortality [Pinteraction = 0.096].
Conclusion
This study demonstrates that TUG time is associated with all-cause mortality in Japanese older adults.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Older adults experience a functional decline in mobility as they age [1, 2]. Mobility performance measures, such as gait speed and timed up and go (TUG) tests, are associated with frailty, future dependence, and all-cause mortality [3,4,5,6]. Slow mobility performance is associated with dementia and a greater number of falls [7, 8]. Therefore, the evaluation of mobility function in older adults plays a key role in individual future prognosis.
The TUG test is one of the most widely used tests for evaluating individual mobility function [9]. This test is easy to perform and can assess mobility via standing and walking abilities which are used in daily life. Thus, it is unsurprising that several research articles have reported that the TUG test is associated with physical functioning and activities of daily life (ADL) [10, 11]. Notably, slower TUG time has been associated with lower physical performance and an increased risk of mortality in European samples [12, 13]. However, little is known regarding the association between TUG time and mortality risk in Asian samples [14].
The TUG time observed in Asian samples is faster than that observed in African Americans and Caucasians, and there is a difference in reference time among different races in the TUG test itself [15]. Therefore, the association between TUG time and mortality might be different among races and should be investigated further. In addition, TUG time reportedly changes based on differences in age, sex, and Body Mass Index (BMI) [1, 6, 16, 17]. TUG time was slower with increased age and for women [1, 6]. Higher BMI (≥ 30) was also associated with slower time than normal BMI (18.5–< 30) [1]. These results may suggest a change in the association between TUG time and mortality under these specific situations. Thus, the association between TUG time and mortality may be moderated by differences in age, sex, and BMI. In examining the possibility of this moderation effect, specific subgroups may be uncovered that require intervention. Thus, the present study aims to investigate the association between TUG time and mortality in Japanese older persons and to clarify possible moderation effects on mortality and TUG time, specifically age, sex, and BMI.
Materials and methods
Data source
The Ogano study was a prospective observational study that began in 2004 to investigate the relationship between longevity and demographic information, social environment, biomarkers, and physical examinations in Ogano-machi, Saitama Prefecture, Japan [10, 18,19,20]. Ogano-machi is a town comprising approximately 12,000 residents, and the proportion of persons ≥ 65 years was 33.3% in 2015 [21]. Participants—all of whom were volunteers—were annually recruited using pamphlets distributed throughout the city. Participants were evaluated at the Ogano assembly hall using standardized questionnaires, anthropometric and physical functioning measurements, and laboratory examinations.
Study population and design
The present study used data from participants who were recruited between 2004 and 2016. We included participants who were ≥ 65 years at their first visit and 1067 participants met this criterion. To investigate the association between baseline data and mortality, we treated data obtained from the first visit as participants’ baseline data. However, those who had mobility limitations, motor dysfunction, mental disorders, or cognitive impairment as assessed by yes/no questions in the interview at their first visit were excluded. We also excluded cases where survival was not known at follow-up.
TUG test
For the TUG test, participants were seated on an armless chair. They then stood up and walked 3 m as fast as possible. Once they reached a colored corner indicating a 3-m distance, they turned around, walked back to the chair, and sat down as fast as possible. The total time to complete the TUG test was recorded using a digital stopwatch.
Other physical assessments
Hand grip strength (HGS) was measured in a standing position using a standard dynamometer in each hand that was adjusted to fit the participant’s hand size. Knee extension strength was measured by having participants engage in two maximum knee extension efforts against a force sensor placed bilaterally while participants were seated. HGS and knee extension strength values on the right and left sides were averaged and expressed as absolute values (kg). Walking speed was measured by asking participants to walk as fast as possible over a 10-m course. The time to complete the walk was measured using a digital stopwatch. One-leg standing time was measured for both legs with eyes open. Time taken was recorded using a digital stopwatch and was stopped if the participant made contact with any part of the room with any part of their body other than the supporting foot. The test was repeated for the other leg, and the longer of the two durations, one on each leg, was used as the one-leg standing time expressed in seconds. These measurements were performed only once, unless the participants performed the test incorrectly.
Outcome and follow-up period
We checked the date of death for each participant in September 2017 to assess all-cause mortality. All-cause mortality was defined as death from all causes in a population. Participants’ date of death data were obtained from public officials from Ogano-machi. For participants who were still living, the follow-up period was calculated as the time between the date of the first visit (from 2004 to 2016) and the 2017 follow-up. For deceased participants, the follow-up period was calculated as the date of the first visit and their date of death.
Standardized questionnaires and anthropometric measurements
To assure the quality and accuracy of their answers, the participants were asked interview questions regarding their past and present medical history, medications, and family history by trained interviewers. Height and body weight were measured while participants were wearing light clothing and no shoes. BMI was calculated as body weight in kilograms divided by body height in m2. Waist circumference was measured at the smallest girth midway between the lowest rib and the iliac crest at the end of normal expiration. Blood pressure was measured twice on the right arm using a standard mercury sphygmomanometer after a 5-min rest period in a seated position. The mean of these two measurements was recorded.
Statistical analyses
Statistical analyses were performed using SPSS version 22.0 for Windows (SPSS, Japan INC, Tokyo, Japan). Continuous variables were reported as medians (25th–75th percentile) and categorical variables as frequencies and percentages. A Cox proportional regression analysis was performed to evaluate the association of TUG time with all-cause mortality. Crude and adjusted models were built to conduct the survival analysis. An adjusted model was created to adjust for age, sex, and BMI as potential confounders. Furthermore, we constructed an adjusted model with current smoking status and past medical history. Hazard ratios (HR) and 95% confidence intervals (CI) were calculated for each model. In addition, we performed a multivariate Cox model with restricted cubic spline to explore the nonlinear exposure–response relationship between TUG time and all-cause mortality. The model was adjusted for possible confounders including age, sex, and BMI. We used median TUG time (7.4 s) as the reference and five knots placed at the 5th, 25th, 50th, 75th, and 95th percentiles for appropriate analysis. The analysis was completed using R for Windows (version 4.0.2).
To explore possible moderating variables, we created participant subgroups, such as men and women who were < 75 and ≥ 75 years of age and those with a BMI of < 25 and ≥ 25. We divided age into two groups—specifically < 75 and ≥ 75 years—because research indicates that TUG time is different among this age group and between men and women [6, 22]. In addition, research indicates that BMI is positively associated with functional limitations, and physical characteristics are different among BMI strata in Japanese persons [17]. Therefore, our participants were grouped into different BMI categories with Japanese criteria [16]; specifically, we divided BMI into two groups: obesity (BMI ≥ 25) and non-obesity (BMI < 25). To determine whether the relationship between TUG time and mortality differed between subgroups, we included a statistical interaction term in our Cox proportional hazard model. Given the known limitations in statistical power when examining interactions, the threshold for statistical significance for an interaction was < 0.10 [23]. We also performed a Cox model with restricted cubic spline if there is a significant difference in the subgroups. All tests were two-tailed, and P values of < 0.05 were considered statistically significant.
Results
Baseline characteristics of the participants
The total number of participants between 2004 and 2016 was 1067, and 194 participants were excluded because they were under 65 years of age and survival was unknown. Thus, the present study comprised a total of 874 participants (Supplementary Fig. 1). Median age and the mean follow-up period were 74 and 8.5 years, respectively. Table 1 shows the baseline characteristics of our participants. Men comprised 35.9% (314) of the participants and the prevalence of all-cause mortality was 25.7% (225). Mean HGS and median 3 m TUG were 22.5 kg and 7.4 s, respectively. Approximately half of the participants (51.4%) were treated with antihypertensive medication and 7.7% with antidiabetic medication, 12.5% had a history of coronary artery disease, and 4.8% had a history of stroke.

Relationship between TUG test time and mortality using a Cox regression analysis with restricted cubic spline. The model was adjusted for age, sex, and BMI. The HR based on a TUG time of 7.4 s (median) as reference was calculated. A knot is located at the 5th, 25th, 50th, 75th, and 95th percentiles for TUG time. The solid line represents the HR, and the shaded area represents the 95% CIs. The dashed line indicates an HR of 1.00, and the dotted line indicates the 10.5 s TUG time mark. TUG timed up and go, BMI body mass index, HR hazard ratio, CI confidence interval
All-cause mortality and restricted cubic spline curve
Table 2 shows the HR of mortality across TUG time. TUG time in one second significantly increased the risk of all-cause mortality in the crude model (HR 1.044, 95% CI 1.019–1.069; P < 0.001). The adjusted model also significantly increased the risk of all-cause mortality for TUG time in one second (HR 1.054, 95% CI 1.016–1.093; P = 0.005). The adjusted model that included current smoking status and past medical history resulted in no change in HR for the association between TUG time in one second and all-cause mortality compared with the adjusted model (Supplementary Table 1). The restricted cubic spline curve is shown in Fig. 1. Overall, the HR between TUG time and mortality increased monotonically. When the TUG time was over 10.5 s, the HR increased over one. On the other hand, when the time was under 7 s, the HR was less than one. Moreover, when the TUG time was over 15 s, the lower limit of the 95% CI was over one HR (Fig. 1).
Subgroup analyses and restricted cubic spline curve
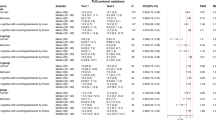
Figure 2 displays the results from our Cox hazard regression models, including interactions, stratified by age, sex, and BMI. Results indicated that increased TUG time was independently associated with mortality in the group aged 75 years and above. A moderation effect of age on TUG time was found between the 65–< 75 and ≥ 75 years of age groups (Pinteraction = 0.096). In addition, women and participants with a BMI of < 25 were positively associated with mortality. However, no significant moderation effects were found among the sex and BMI groups on TUG time and mortality. Figure 3a, b shows the relationship between TUG time and mortality in the participants aged 65– < 75 and ≥ 75 years using a Cox regression with restricted cubic spline, respectively. In the results of the participants aged 65 – < 75 years, although the HR increased over one between 6.5 and 7.4 s of TUG time, the HR was less than one in other TUG times (Fig. 3a). In the result of the participants aged ≥ 75 years, the HR was around one when the TUG time was between 7.4 and 10.5 s. When the time was over 10.5 s, the HR was over one (Fig. 3b).

Subgroup analysis of stratified age, sex, and BMI for the association between TUG time and mortality. The model is adjusted for age, sex, and BMI. HR: hazard ratio, CI confidence interval, TUG timed up and go, BMI body mass index

a Relationship between TUG time and mortality in 65–< 75 years old participants using a Cox regression analysis with restricted cubic spline. The model was adjusted for sex and BMI. The HR based on a TUG time of 7.4 s (median) as reference was calculated. A knot is located at the 5th, 25th, 50th, 75th, and 95th percentiles for TUG time. The solid line represents HR, and the shaded area represent the 95% CIs. The dashed line indicates an HR of 1.00. TUG timed up and go, HR hazard ratio, BMI body mass index, CI confidence interval. b Relationship between TUG test time and mortality in ≥ 75 years old participants using a Cox regression analysis with restricted cubic spline. The model was adjusted for sex and BMI. The HR based on a TUG time of 7.4 s (median) as reference was calculated. A knot is located at the 5th, 25th, 50th, 75th, and 95th percentiles for TUG time. The solid line represents the HR, and the shaded area represents the 95% CIs. The dashed line indicates an HR of 1.00, and the dotted line indicates the 10.5 s TUG time mark. TUG timed up and go, HR hazard ratio, BMI body mass index, CI confidence interval
Discussion
This prospective study investigated the association between mobility performance and mortality in community-dwelling healthy Japanese older adults. Our Cox regression analysis revealed that TUG time was associated with a significant increase in risk of mortality after adjusting for potential confounders. The HR of mortality was increased when TUG time was over 10.5 s. Moreover, age moderated the effect of TUG time and mortality.
To our knowledge, the finding that TUG time is associated with an increased risk of mortality in Japanese older adults is novel. The association between TUG time and mortality in Japanese older adults is consistent with previous reports examining this association in other races [6, 12]. Although this association has been identified in other Asian countries, such as Korea [14], our results confirm that the TUG test is related to mortality in a different Asian country, namely, Japan.
Older adults experience a decline in physical performance and have metabolic abnormalities [24, 25]. The TUG test expresses a comorbid burden that highlights the importance of multisystem interactions among several different systems involved in coordinating walking and balance. Previous research indicates that walking speed is associated with frailty and mortality, and that balance tests, such as one-leg standing time are related to frailty [3, 5, 26]. Thus, slow TUG time may reflect a decline of a multisystem interaction with aging and is expressed as low physical functioning. Research indicates that low physical performance and social dependence is positively associated with all-cause mortality in older adults [13, 27]. Therefore, the TUG test may also be associated with all-cause mortality.
As mentioned previously, the reference value of the TUG test is different among different races [15]. One meta-analysis, which did not include Asia, reported the mean TUG time for three age groups as 8.1, 9.2, and 11.3 s for those aged 60–69, 70–79, and 80–99 years, respectively [22]. In our study, median TUG time (7.4 s) was faster even though median age was 74 years old. It is not clearly known as to why TUG time in Asians is faster than in other races. Research indicates that the walking speed of older Japanese persons is faster than Caucasians and the median walking speed in our participants was similar to a previous study (1.41 m/s) [28]. Notably, walking speed is correlated with TUG performance.9 Therefore, the TUG time observed in Japanese older adults may be lower than the TUG time observed in other races because walking speed in Japanese is faster. However, further investigation will be needed to clarify why TUG time is faster in Asian persons compared to other races. Still, the association between TUG time and mortality is consistent with several races, even though there is a difference in the reference value of the TUG test in older adults.
Using a Cox model with restricted cubic spline, we demonstrated how much TUG time results in a risk of mortality and observed that mortality risk began at 10.5 s. When the TUG time reached over 15 s, which was over the lower limit of the 95% CI, there was a statistically significant increase in risk of mortality. Thus, risk of mortality may begin to increase when the TUG time is within the range of 10.5–15 s. Conversely, the TUG time range between 7 and 10 s was stagnated. That means this range of time was not different from the reference time for a risk of mortality. In fact, the risk of TUG time for mortality is also over 10 s in the Korean population [14]. Therefore, the risk of mortality in TUG time might begin from 10.5 s in older Japanese adults.
In the present study, age significantly moderated the relationship between mortality and TUG time. We divided age into two groups (65– < 75 years old and ≥ 75 years old); these groups exhibited different risks of mortality, even with the same TUG time. That is, the group that was 65– < 75 years of age was not associated with a risk of mortality, but the ≥ 75 years of age group was significantly associated with a risk of mortality. This finding suggests that mobility function may accelerate and increase the risk of all-cause mortality in persons aged ≥ 75 years. In fact, the HR for mortality increased with increasing TUG time in the participants aged ≥ 75 years in the restricted cubic spline. Many countries define “old” as ≥ 65 years, regardless of no clear medical or physiological evidence [29, 30]. The Japan Geriatrics Society recommends that “old” be defined as ≥ 75 years because persons aged 65– < 75 years are still mentally and physical healthy and can proactively participate in social activities [31]. Given that the relationship between mobility performance and elevated risk of mortality was stronger in participants who were ≥ 75 years of age, our results suggest that risk factors for mortality change from 75 years of age. Thus, this finding supports the recommendation to define “old” as ≥ 75 years.
The strength of this study is the long follow-up time and few cases of unknown survival. The median follow-up period was 8.5 years which is long compared to previous studies. The unknown survival rate was approximately 8.3% among the participants aged ≥ 65 years. The inclusion of only Japanese participants is another strength of this study, given the previously observed racial variability in TUG times. The association between TUG time and all-cause mortality was an interesting result, even though TUG times for Japanese individuals is generally faster than for other races. The present study has several limitations. First, our participants were all volunteers and may be healthier members of our target population. Generally, non-participants exhibit lower physical performance and higher mortality in population-based studies. Therefore, our results may have underestimated the relationship between the TUG test and all-cause mortality. Second, we evaluated the association between the TUG test and all-cause mortality. Generally, given that the TUG test is related to physical performance, participants with congestive heart failure and cancer—which are associated with sarcopenia and frailty—may participate in fewer activities [32, 33]. Thus, there could be a stronger association between physical performance and mortality if cause-specific mortality was investigated. Third, there are residual confounding factors to various degrees in all observational studies. We reviewed the previous reports regarding the associated factors between TUG time and mortality. However, we were unable to identify confounders to include in our data analyses. Therefore, we included key confounders in our analysis. Although we created a model that included participants’ smoking status and past medical history, there was no change in the results (Supplemental Table 1). Thus, background characteristics, such as current smoking status and past medical history, might exert little influence on the association between TUG time and all-cause mortality. Fourth, our participants came from a study conducted between 2004 and 2016 and their mortality was evaluated in 2017. Given that the minimum follow-up period of the participants was one year, it is possible that some deceased participants were included in the “still living” group. However, the number of new participants was 20 in 2016; therefore, the results from a possible number of deceased participants may be offset by the results of recent participants.
Conclusion
This study demonstrates that TUG time is associated with all-cause mortality in Japanese older adults. Moreover, the association between TUG time and mortality may begin from 10.5 s in Japanese older adults. These findings suggest that the evaluation of TUG time for mortality needs to consider race.
Data availability
The datasets generated and analyzed during the study are available from the corresponding author on reasonable request.
References
Huang C, Sun S, Tian X et al (2019) Age modify the associations of obesity, physical activity, vision and grip strength with functional mobility in Irish aged 50 and older. Arch Gerontol Geriatr 84:103895. https://doi.org/10.1016/j.archger.2019.05.020
Musich S, Wang SS, Ruiz J et al (2018) The impact of mobility limitations on health outcomes among older adults. Geriatr Nurs 39:162–169. https://doi.org/10.1016/j.gerinurse.2017.08.002
Kim M, Yabushita N, Kim M et al (2010) Mobility performance tests for discriminating high risk of frailty in community-dwelling older women. Arch Gerontol Geriatr 51:192–198. https://doi.org/10.1016/j.archger.2009.10.007
Shinkai S, Watanabe S, Kumagai S et al (2000) Walking speed as a good predictor for the onset of functional dependence in a Japanese rural community population. Age Ageing 29:441–446. https://doi.org/10.1093/ageing/29.5.441
Zhao W, Ukawa S, Tsushita K et al (2015) Association of gait speed with mortality among the Japanese elderly in the New Integrated Suburban Seniority Investigation Project: a prospective cohort study. Age Ageing 44:153–157. https://doi.org/10.1093/ageing/afu121
Bergland A, Jørgensen L, Emaus N et al (2017) Mobility as a predictor of all-cause mortality in older men and women: 11.8 year follow-up in the Tromsø study. BMC Health Serv Res 17:22. https://doi.org/10.1186/s12913-016-1950-0
Asai T, Oshima K, Fukumoto Y et al (2018) Association of fall history with the Timed Up and Go test score and the dual task cost: a cross-sectional study among independent community-dwelling older adults. Geriatr Gerontol Int 18:1189–1193. https://doi.org/10.1111/ggi.13439
Lee JE, Shin DW, Jeong S et al (2018) Association between Timed Up and Go test and future dementia onset. J Gerontol A Biol Sci Med Sci 73:1238–1243. https://doi.org/10.1093/gerona/glx261
Podsiadlo D, Richardson S (1991) The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 39:142–148. https://doi.org/10.1111/j.1532-5415.1991.tb01616.x
Coelho-Junior HJ, Rodrigues B, Gonçalves IO et al (2018) The physical capabilities underlying timed “Up and Go” test are time-dependent in community-dwelling older women. Exp Gerontol 104:138–146. https://doi.org/10.1016/j.exger.2018.01.025
Otsuka H, Kobayashi H, Suzuki K et al (2020) Mobility performance among healthy older adults eligible for long-term care in Japan: a prospective observational study. Aging Clin Exp Res. https://doi.org/10.1007/s40520-019-01404-2
Idland G, Engedal K, Bergland A (2013) Physical performance and 13.5-year mortality in elderly women. Scand J Public Health 41:102–108. https://doi.org/10.1177/1403494812466460
Roshanravan B, Robinson-Cohen C, Patel KV et al (2013) Association between physical performance and all-cause mortality in CKD. J Am Soc Nephrol 24:822–830
Son KY, Shin DW, Lee JE et al (2020) Association of timed up and go test outcomes with future incidence of cardiovascular disease and mortality in adults aged 66 years: Korean national representative longitudinal study over 5.7 years. BMC Geriatr 20:111
Kamide N, Takahashi K, Shiba Y (2011) Reference values for the Timed Up and Go test in healthy Japanese elderly people: determination using the methodology of meta-analysis. Geriatr Gerontol Int 11:445–451. https://doi.org/10.1111/j.1447-0594.2011.00704.x
Nonaka K, Murata S, Shiraiwa K et al (2018) Physical characteristics vary according to body mass index in Japanese community-dwelling elderly women. Geriatrics 3:87. https://doi.org/10.3390/geriatrics3040087
Woo J, Leung J, Kwok T (2007) BMI, body composition, and physical functioning in older adults. Obesity 15:1886–1894. https://doi.org/10.1038/oby.2007.223
Otsuka H, Yanai M, Kobayashi H et al (2018) High-molecular-weight adiponectin levels in healthy, community-dwelling, elderly Japanese volunteers: a 5-year prospective observational study. Aging Clin Exp Res 30:791–798. https://doi.org/10.1007/s40520-017-0840-6
Kobayashi H, Otsuka H, Yanai M et al (2018) Adiponectin is not associated with renal function decline in community-dwelling elderly adults. Medicine 97:e10847. https://doi.org/10.1097/MD.0000000000010847
Kobayashi H, Otsuka H, Yanai M et al (2019) Adiponectin receptor gene polymorphisms are associated with kidney function in elderly Japanese populations. J Atheroscler Thromb 26:328–339. https://doi.org/10.5551/jat.45609
Japan Medical Association. Japan Medical Analysis Platform [Internet]. [Cited 25 Jan 2020]. Available from: http://jmap.jp/cities/detail/city/11365.
Bohannon RW (2006) Reference values for the timed up and go test: a descriptive meta-analysis. J Geriatr Phys Ther 29:64–68. https://doi.org/10.1519/00139143-200608000-00004
Greenland S (1983) Tests for interaction in epidemiologic studies: a review and a study of power. Stat Med 2:243–251. https://doi.org/10.1002/sim.4780020219
Tieland M, Trouwborst I, Clark BC (2018) Skeletal muscle performance and ageing. J Cachexia Sarcopenia Muscle 9:3–19. https://doi.org/10.1002/jcsm.12238
Dominguez LJ, Barbagallo M (2016) The biology of the metabolic syndrome and aging. Curr Opin Clin Nutr Metab Care 19:5–11. https://doi.org/10.1097/MCO.0000000000000243
Drusini AG, Eleazer GP, Caiazzo M et al (2002) One-leg standing balance and functional status in an elderly community-dwelling population in northeast Italy. Aging Clin Exp Res 14:42–46. https://doi.org/10.1007/BF03324416
Millán-Calenti J, Tubío J, Pita-Fernández S et al (2010) Prevalence of functional disability in activities of daily living (ADL), instrumental activities of daily living (IADL) and associated factors, as predictors of morbidity and mortality. Arch Gerontol Geriatr 50:306–310. https://doi.org/10.1016/j.archger.2009.04.017
Aoyagi K, Ross PD, Nevitt MC et al (2001) Comparison of performance-based measures among native Japanese, Japanese-Americans in Hawaii and Caucasian women in the United States, ages 65 years and over: a cross-sectional study. BMC Geriatr 1:3. https://doi.org/10.1186/1471-2318-1-3
Gorman M (1999) Development and the rights of older people. In: Randel J, German T, Ewing D (eds) The ageing and development report: poverty, independence and the world’s older people. Earthscan Publications Ltd., London, pp 3–21
Thane P (1978) The muddled history of retiring at 60 and 65. New Society 45:234–236
Tokuda Y, Hinohara S (2008) Geriatric nation and redefining the elderly in Japan. Int J Gerontol 2:154–157. https://doi.org/10.1016/S1873-9598(09)70003-1
Yamada S, Kamiya K, Kono Y (2015) Frailty may be a risk marker for adverse outcome in patients with congestive heart failure. ESC Heart Fail 2:168–170. https://doi.org/10.1002/ehf2.12052
Handforth C, Clegg A, Young C et al (2015) The prevalence and outcomes of frailty in older cancer patients: a systematic review. Ann Oncol 26:1091–1101. https://doi.org/10.1093/annonc/mdu540
Funding
This study was partially supported by a grant from the “Strategic Research Base Development” Program for Private Universities, subsidized by the Ministry of Education, Culture, Sports, Science & Technology (MEXT) in Japan (2011), as well as a generous donation from the Saitama Prefecture University.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Statement of human and animal rights
Approval for the present study was obtained from the Research Committee of Nihon University School of Medicine, Tokyo, Japan. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Informed consent
Participants provided written and informed consent at their first visit.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Otsuka, H., Kobayashi, H., Suzuki, K. et al. Mobility performance impacts mortality risk in community-dwelling healthy older adults in Japan: a prospective observational study. Aging Clin Exp Res 33, 2511–2517 (2021). https://doi.org/10.1007/s40520-021-01787-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-021-01787-1