
Abstract
Background
Impairment of postural adjustments in elderly is associated with decreased functional mobility, balance confidence and quality of life.
Aims
We studied the effects of anticipatory postural adjustments focused training on postural preparation, balance confidence and quality of life of the elderly.
Methods
It was a single-blind randomized controlled trial. The sample included 60 males with history of falling (at least once in the past 6 months). They were matched and randomly assigned into three groups: perturbation, balance, and no training. The electrical activity of the muscles was measured by electromyography. The Activities-specific Balance Confidence (ABC) scale and the SF-36 questionnaire were used to assess balance confidence and quality of life, respectively. Repeated-measures ANOVA was used for data analysis (significant level 0.05).
Results
The type of training had significant interaction effect on muscle latency (F(2, 46) ≥ 71.06, P ≤ 0.001, η2 ≥ 0.75). Compared to the other two groups, perturbation training group showed significantly more improvement in ABC scale (F(2, 46) = 14.94, P ≤ 0.000, η2 ≥ 0.39). It also significantly showed more improvement than no training group in all areas of SF-36 questionnaire, except for mental health (F(2, 46) ≥ 6.56, P ≤ 0.03, η2 ≥ 0.22).
Conclusions
Our findings support the use of perturbation training, as it reduced the probability of falling (by decreasing muscle latency and increasing posture preparation), improved the balance confidence for daily activities, and improved the quality of life.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Prevention and treatment of infectious and chronic degenerative diseases have significantly increased the life expectancy and the population of the elderly [1]. Furthermore, aging is directly associated with reduction in muscle mass, muscle strength, and nervous reactions [2]. They intensify the risk of falling which is one of the causes of disability and inability for the elderly. The fear of repeated falls is one of the consequences of falling which is experienced by a large number of the elderly [3]. Although the fear of falling is mostly a psychological problem and not a motor difficulty, it reduces self-imposed functional mobility and activities of daily living (ADL) due to a lack of dynamic self-confidence. Reduction of functional mobility and ADL, in turn, decreases the neuromuscular abilities and increases both the risk of falling and the fear linked to it and this defective cycle continues [4]. There is also an inverse relationship between both falling and fear of falling with quality of life (QOL). Generally, either falling or the fear of falling can cause a range of adverse health outcomes, including poor health conditions, functional impairments, and decreased self-esteem and QOL [5]. To control the risk of falling and avoid its negative physical, psychological, or social consequences, researchers have introduced various treatments. Within this wide range of treatments, exercise programs have been of great interest to researchers, leading to the development of a variety of exercise protocols. Accordingly, choosing the best exercise program with the most impact is an important area for research.
When a person is perturbed, the central nervous system (CNS) uses two main strategies to maintain and restore balance: anticipatory postural adjustment (APA) and compensatory postural adjustment (CPA) [6]. The APA occurs before a predictable perturbation or motion happens, while the CPA acts after a perturbation and they depend on the delay and extent of the APA for the restoration of balance. As a result, these two strategies are interrelated, and the researchers have investigated whether or not the activation of APA will reduce the need for a larger activation of CPA. A better APA reduces the displacement of the center of pressure (COP). It, in turn, increases the chance of recovery of balance and reduces the chance of falling [7]. Aging is associated with impaired and delayed APA and consequently disturbed balance [8]. It is reported that a single training session of catching ball improved the APA and reduced the CPA activation for the elderly. As a result, the volume of COP displacement was also reduced, and the recovery of balance happened more efficiently [9]. Jagdhane et al. examined the feasibility of APA training in three older adults and reported that 4 weeks of APA training reduced the muscle delay contraction and that it was effective in restoring the balance of the elderly [10].
In this study, we addressed some limitations and unknowns in current APA-focused training literature, e.g., lack of specificity and feasibility of exercise protocols, inadequacy of sample size and/or duration of training, and lack of information about the impact of APA training on postural preparation, and about the prevention of falling and quality of life in the elderlies with a history of falling. We also compared the effects of APA-focused training with balance training and examined whether APA-focused training could increase the effects of balance training on postural preparation (muscle delay), balance confidence and quality of life in elderly with a history of falling. In this text, APA-focused training and perturbation training (PT) are used interchangeably.
Materials and methods
Participants
It was a single-blind matched randomized controlled trial approved by the Research Ethics Board of University of Isfahan (the approval code is IR.UI.REC1396.065). The target population included elderly males with a history of at least one fall during the past 6 months. Advertisements were distributed to elderly attending mosques, parks and libraries, and those with a history of fall were invited to participate in the study. The inclusion criteria were being male, aged between 65 and 80 years, ability to walk without help, normal or corrected vision and hearing, and positive response to all questions listed in Physical Activity Readiness Questionnaire (PARQ), and obtaining a score more than 24 (out of 30) in Mini-Mental State Examination (MMSE). The exclusion criteria consisted of free will to withdraw from the study, absence in more than one-third of exercise sessions, or not being able to comply with the exercise protocol. Before the beginning of the study, all participants signed the consent form and underwent a screening evaluation by a blind assessor. All the measurements carried out in the laboratory of the Faculty of Exercise Sciences, University of Isfahan. Sixty participants were recruited, matched, and randomly assigned into three groups of perturbation training (PT), balance training (BT) and no training (NT). Matching was based on scores of “functional reach test”.
Procedure and experimental setup
All tests were administered pre- and post-intervention. We used Activities-specific Balance Confidence scale (ABC) to measure balance confidence (BC), and the SF-36 questionnaire to measure QOL. Perturbations were externally induced by pendulum impact (Fig. 1) to measure the muscle latency (ML) [6, 8, 11]. During the externally induced perturbations, the participants were asked to stand barefoot on the ground with open eyes. At first, 5% of the participants’ body weight was added to the end of the pendulum. Then, the participants were asked to bring their hands up at shoulder level and put their palms against the pendulum. The participants received each pendulum impact from a 30° angle and were asked to maintain their balance after the impact [8, 10]. Three practice trials were given before the test. Five trials were performed in each test to achieve performance stability.

The experimental setup for pendulum impact test. EMG activity of six muscles was recorded (i.e., TA tibialis anterior, MGC medial gastrocnemius, RF rectus femoris, BF biceps femoris, RA rectus abdominis, ES erector spine)
Measurement of muscle latency
An electromyography instrument (ME6000) was used to record the surface activity of the tibialis anterior (TA), medial gastrocnemius (MGC), rectus femoris (RF), biceps femoris (BF), rectus abdominis (RA) and erector spinae (ES). The skin was cleaned and shaved, and disposable self-adhesive electrodes were attached on the non-dominant side of the subject’s muscle bellies, with their centers approximately 2 cm apart from each other. The ground electrode was attached to the superior anterior part of the tibia bone. The foot switch was used to record the moment of impact (T0). It was attached to the lower end of the pendulum and marked the moment of impact on electromyographic signals [12].
Measurement balance confidence
To measure the BC, an ABC scale was used. Researchers have reported that the ABC scale is better than the fall efficacy scale and includes a wider range of ADL. The ABC scale consists of a 16-item questionnaire that asks participants to evaluate their confidence (from 0% = low to 100% = high) to perform ADLs. Each item has 100 scores, and the participants’ score in this scale is the total score of all the items divided by 16. The minimum and maximum possible score on this scale will be zero and 100, respectively. A higher score in this scale means higher BC, less fear of falling and less chance of falling [13]. Also, the higher score in ABC is associated with higher scores in Berg Balance [14], Single Leg Stand and Timed Up and Go tests [15]. Validity and reliability of the Persian version of this scale in Iranian society have been well reported [16]. The ABC scale was administered by an assessor who was blind about the classification of groups.
Measurement quality of life
An SF-36 questionnaire was used to measure QOL. Researchers have reported that the SF-36 form is the most widely used tool in studies on QOL [17]. The questionnaire consists of 36 items, each ranging from 0 to 100 scores. A lower score means a worse condition of the measured variable and a higher score means a better condition of it. The questionnaire is divided into eight different domains of health conditions including functional capacity (FC), physical aspects (PA), pain (P), general health (GH), vitality (V), social aspects (SA), emotional aspect (EA), mental health (MH), and a total score of QOL. Each domain is scored from 0 to 100, and the total score of QOL is the total score of eight domains divided by eight [18]. The validity and reliability of the Iranian version of the questionnaire have been reported to be high as well [19].
Training protocol
The training program of both PT and BT groups lasted for 8 weeks and included 3 sessions of 1-h training per week (a total of 24 sessions). The exercise protocol of PT group included up to 9 min of warm-up, 42 min of main exercises and up to 9 min of cool-down. The main exercises of PT group consisted of six 7-min parts (Table 1). There were also six types of variations for main exercises of PT group. For details of these variations refer to Table 2. For example, at the 17th session, “22–28 min” column’s code is A3.B3.C1.D2.E1.F1. The code means that the 7-min training session of this part is done in “standing position (A3)” and includes “pass by hand to the wall (B3)”, with volleyball ball (C1), from a distance of 3 meters (D3), in the height of chest (E1), with air pass (F1).
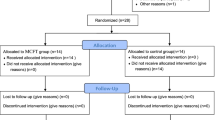
The exercise protocol of BT group included up to 7 min of warm-up, 45 min of main exercises and up to 7 min of cool-down. The main exercises of BT group consisted of three 15-min parts of standing balance, walking balance and strength training. Variations of standing balance training included: base of support (narrow/wide), foot position (single/double), ground surface (hard/soft), balance board (rocker/wobble), carrying object (single/double hand), balance moves (tandem stand/single leg stand/star excursion balance). Variations of walking balance training included ground surface (soft/hard), speed (slow/fast), foot contact with ground (toes/heel/lateral/whole), walking direction (forward/backward/sideward), carrying object (single/double hand), barriers (low/high). Strength training included three movements of push-ups, heel raises, and squat. The position of the body and the range of motions depended on the level of physical fitness of participants. The workout consisted of 3 sets of 8–12 repetitions with a load of 75% of 1RM. The NT group had no exercise program during study period and were asked to have no changes in their routine activities (Fig. 2).

Teager–Kaiser energy operator method for determining muscle latencies. ms millisecond, T0 moment of impact, mv millivolt
Data processing
All signals were processed offline using MATLAB software (MathWorks Inc). All EMG signals were rectified and filtered with a band-pass (10–250 Hz) bidirectional, second-order, Butterworth filter. Sample rate was 1000 Hz. Depending on the foot switch signal that was visible on the electromyographic signals, the moment of impact was identified as time zero” (T0). Data in the range from − 1000 ms (before T0) to + 1000 ms (after T0) were selected for further analysis [10]. Teager–Kaiser energy operator (TKEO) method was used to determine muscle latencies. The muscle onset latency was detected in a time window from − 500 ms to + 200 ms in relation to T0 as the instant lasting for at least 25 ms when EMG amplitude for a given muscle was greater (activation) or smaller (inhibition) than the mean ± 3 SD of its baseline (− 1000 to − 850) value (Fig. 3) [20, 21].

The flowchart of participant recruitment. FRT functional reach test, PTG PT group, BTG BT group, NTG NT group
Statistical analysis
Data were statistically analyzed by SPSS statistical software version 23. Normal distribution of data was examined by Shapiro–Wilk test. Demographic characteristics (height, age, weight and MMSE) of groups were examined by one-way ANOVA. Repeated-measures ANOVA was used for two-way comparisons on muscle latency, balance confidence and quality of life. In these comparisons, between factor was training type (PT, BT, NT groups) and within factor was time of testing (pre- and post-training). Tukey post hoc test was used for pairwise comparisons. Significance level was set at 0.05 for all statistical analyses.
Results
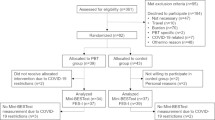
Out of 60 recruited participants, 49 succeeded in completing the study to the end of measurements (18, 16, and 15 in PT, BT, and NT groups, respectively). The flowchart of the participant recruitment process from the start to the end of study is presented in Fig. 4. Table 3 demonstrates the demographic characteristics of the participants. As there is no significant difference among the groups (P > 0.05), we can conclude that demographic characteristics of three groups of the study are homogeneous.

The bar chart of the rate of muscle latency for studied muscles in three groups of the study (TA tibialis anterior, MGC medial gastrocnemius, RF rectus femoris, BF biceps femoris, RA rectus abdominis, ES erector spine, PT perturbation training, BT balance training, NT no training)
Muscle latency
Postural activity in anticipation of the external perturbation showed more progress in PT group as compared to two other groups. The bar chart of this statistical analysis is presented in Fig. 4. According to post hoc pairwise comparison presented in Table 4, the rate of progress of latency of all six muscles in PT group was significantly more than that of the other two groups (P < 0.05). When comparing BT group with NT group, the difference in progress rate is just significant for RF and BF muscles (P < 0.05).
Thus, the onset of APA activity pre- and post-intervention in PT, BT and NT groups was as follows: in PT group in TA (pre: − 51.23 ± 8.09 ms, post: − 215.14 ± 69 ms); MGC (pre: − 67.68 ± 20.36 ms, post: − 294.45 ± 84.40 ms); RF (pre: − 71.85 ± 14.06 ms, post: − 159.06 ± 23.72 ms); BF (pre: − 72.08 ± 16.60 ms, post: − 266.05 ± 48.07 ms); RA (pre: − 61.06 ± 21.57 ms, post: − 188.15 ± 23.94 ms); ES (pre: − 79.92 ± 18.01 ms, post: − 210.69 ± 43.04 ms), in BTG in TA (pre: − 49.15 ± 11.61 ms, post: − 99.71 ± 24.48 ms); MGC (pre: − 70.60 ± 23.03 ms, post: − 145.43 ± 40.95 ms); RF (pre: − 81.98 ± 19 ms, post: − 109.63 ± 21.09 ms); BF (pre: − 75.51 ± 14.32 ms, post: − 160.15 ± 26.20 ms); RA (pre: − 95.62 ± 24.68 ms, post: − 171.81 ± 27.74 ms); ES (pre: − 76.85 ± 17.17 ms, post: − 101.86 ± 16.30 ms), and in NTG in TA (pre: − 57.67 ± 9.75 ms, post: − 60.45 ± 12.70 ms); MGC (pre: − 75.43 ± 11.22 ms, post: − 68.85 ± 19.73 ms); RF (pre: − 81.01 ± 9.78 ms, post: − 66.55 ± 11.55 ms); BF (pre: − 90.42 ± 15.28 ms, post: − 92.80 ± 11.24 ms); RA (pre: − 45.04 ± 7 ms, post: − 39.18 ± 10.06 ms); ES (pre: − 83.12 ± 15.23 ms, post: − 74.09 ± 16.17 ms).
Balance confidence and quality of life
Table 5 represents the results of repeated-measures ANOVA for BC and QOL. It suggests that effects of PT, BT, and NT groups are significantly different in ABC (F(2, 46) = 14.94, P ≤ 0.001, η2 ≥ 0.39) and QOL (F(2, 46) = 50.22, P ≤ 0.001, η2 ≥ 0.68). Table 6 represents the post hoc pairwise comparisons related to Table 5. It shows that compared to NT group, PT group showed more progress in ABC and all domains of QOL, except mental health (P < 0.05). Progress of PT group was better than that of BT group in ABC and vitality as well (P < 0.05). Compared to NT group, BT group also showed more progress in ABC and all domains of QOL scores, except social and mental health (P < 0.05).
Discussion
Postural preparation
The purpose of this study was to do a comparison between perturbation training and balance training on ML, BC, and QOL of elderly who have a falling record.
The results showed that PT and BT both are effective for improved ML and PT is even more effective than BT. The CNS uses two anticipatory and compensatory mechanisms to maintain and restore the balance when confronting perturbation. The balance control depends on the effectiveness of using these two mechanisms. Impairment of anticipatory mechanisms is one of the main reasons for the reduction of balance and, consequently, the reduction of motor function in the elderly. The anticipatory mechanism is significantly delayed in healthy elderly as compared to young people; thus, muscles activate or inhibit activation too late in elderly [22]. This delay in the muscle onset increases both the COP displacement and the instability rate after perturbation [8].
CNS controls the APA by feed forward in an open-looped manner (with no proprioceptive sensory feedback) [7]. APA center is anatomically a portion of reticular formation located in pontomedullary junction (the boundary of the pons and the medulla oblongata) [23]. Biomechanical and morphological studies have shown that “changes associated with age” occur in these neuronal structures. These centers are reported to be partially or totally diminished in elderly with balance disorder and those with impaired APA [24]. Thus, negative changes in muscular responses of elderly can be considered as a reflection of diminishing changes in CNS structures that are responsible for posture control. So, it can be argued how perturbation training probably affects these CNS structures, and thereby improve the performance of APA and the muscular latency. It is suggested that the APA-focused training accelerates the onset of CNS activation in APAs muscles, leading to reduction of displacement of the COP, and it probably decreases the need for CPA activation [9, 10]. Our findings support such claims, as they showed that, compared to BT and NT groups, PT group showed more improvement in postural preparation and stability. However, the mechanism of such functional improvements is not yet fully understood and explained. It can be viewed from the perspective of motor changes or changes in neuroanatomical plasticity, or an interaction of both [25].
Balance confidence
We used the ABC scale to track the changes of BC. Our findings showed that PT and BT both are effective for improved ABC scores and PT is even more effective than BT. Previous studies have reported that ABC scale is one of the strongest predictors of falling in the elderly, and there is a correlation between the score of ABC scale and the probability of falling, and older adults whose score is below 67 have more fear of falling and are more likely to fall [26]. For PT group, the mean scores of ABC scale improved from 65 to 80 and showed a progression rate of 25%. The progression rate was 22% for BT group (a change from 62 to 76). It supports this claim that balance and perturbation training are both effective exercises to improve the ADL performance and BC. More balance confidence probably results in both reducing fear of falling and reducing the probability of falling, which would finally prevent the consequences of falls. It is reported that a Tai Chi training program increased BC of the elderly up to 11% [27]. Researchers have shown that a 12-week Pilates training program scheduled as two sessions per week increased the BC of the elderly by 17% [28]. Also, researchers have found that after 4 weeks of PT, the BC improved up to 4.6% though this improvement was not significant [10]. The rate of progression was the highest in our study, and it could be due to a higher number of participants exercising together, more organized exercise program which enabled us to have a longer duration of training by using a variety of different exercises which helped us to make a enjoyable and happy atmosphere and avoid tedium. However, the progression rate was even higher in PT group than BT group. Playing with a ball is more fun and the ability to manipulate the ball probably increased the skill self-efficacy of participants. Moreover, many participants in PT group stated that they revived memories of childhood and adolescence when catching and throwing balls. They were very enthusiastic about the exercises. Better motivation could justify more fun, longer duration, and more practice. These could be a bonus to a better exercise regimen which holds more challenging activities.
Considering the relationship between ABC score and functional balance [29], it can be concluded that PT implicitly improves elderly’s functional balance more than BT and thereby reduced the chance of falling more effectively. It has been shown that APA is impaired in elderly compared to younger people and such an impairment is more likely to occur in elderly who have experienced falling [8]. It is suggested that ball catching exercises activate predictive muscles by influencing the APA and by decreasing the delay in the onset of muscle contraction. As a result, they reduce the need for a larger contraction of the CPA muscles. Therefore, the restoration of the balance is faster and reduce the risk of falling [9]. This finding was in line with the results of our study. PT influence elderly’s balance and BC in ADL because of the anticipatory muscular activity and ML contraction improvements. That is why the mean score of the ABC was improved in the PT group more than other groups.
Quality of life
The findings obtained from SF-36 questionnaire showed that compared to NT group, PT group illustrated more progress in all domains of QOL, except mental health (P < 0.05). Progress of PT group was not better than that of BT group, except in vitality (P < 0.05). Compared to NT group, BT group also showed more progress in all domains of QOL scores, except social and mental health (P < 0.05). Putting together, we can conclude both PT and BT positively affect the QOL, but PT has more impact on vitality, social health, and mental health.
As age increases, functional activity impairment develops and leaves a more negative impact on maintaining independence by increasing the need for help [30], which might reduce the QOL. Hence, exercises that reduce functional activity impairment would improve the QOL of the elderly by increasing their self-efficacy and independence in ADL, and by reducing the fear of falling. In line with findings of our study, many researchers have reported improvement in the elderly’s QOL followed by a training program [31,32,33]. Also, researchers have reported that the elderly who do not perform physical activities have a lower QOL than those who do [34]. On the other hand, because the fear of falling and participation in training is highly associated with QOL, improving the ABC scale score in training groups especially in PT group reduces the fear of falling and can justify the reasons why QOL improved in the elderly in PT group more than other groups.
Conclusions
The results of this study showed that the PT improves the muscle onset and postural preparation more than the BT and thus, it is more useful in improving the BC and QOL in the elderly with the record of a fall. Thereby, in PT group, the fear of falling, the likelihood of falling and the consequences of falling decreased more than BT group.
References
van Uffelen JG, Khan A, Burton NW (2017) Gender differences in physical activity motivators and context preferences: a population-based study in people in their sixties. BMC Public Health 17:624
Snijders T, Verdijk LB, van Loon LJ (2009) The impact of sarcopenia and exercise training on skeletal muscle satellite cells. Ageing Res Rev 8:328–338
Evitt CP, Quigley PA (2004) Fear of falling in older adults: a guide to its prevalence, risk factors, and consequences. Rehabil Nurs 29:207
Tinetti ME, Richman D, Powell L (1990) Falls efficacy as a measure of fear of falling. J Gerontol 45:239–243
Parry SW, Steen N, Galloway SR et al (2001) Falls and confidence related quality of life outcome measures in an older British cohort. Postgrad Med J 77:103–108
Santos MJ, Kanekar N, Aruin AS (2010) The role of anticipatory postural adjustments in compensatory control of posture: 1. Electromyographic analysis. J Electromyogr Kinesiol 20:388–397
Alexandrov AV, Frolov AA, Horak FB et al (2005) Feedback equilibrium control during human standing. Biol Cybern 93:309–322
Kanekar N, Aruin AS (2014) Aging and balance control in response to external perturbations: role of anticipatory and compensatory postural mechanisms. Age 36:9621
Aruin AS, Kanekar N, Lee YJ et al (2015) Enhancement of anticipatory postural adjustments in older adults as a result of a single session of ball throwing exercise. Exp Brain Res 233:649–655
Jagdhane S, Kanekar N, Aruin AS (2016) The effect of a four-week balance training program on anticipatory postural adjustments in older adults: a pilot feasibility study. Curr Aging Sci 9:295–300
Santos MJ, Kanekar N, Aruin AS (2010) The role of anticipatory postural adjustments in compensatory control of posture: 2. Biomechanical analysis. J Electromyogr Kinesiol 20:398–405
Krishnan V, Kanekar N, Aruin AS (2012) Feedforward postural control in individuals with multiple sclerosis during load release. Gait Posture 36:225–230
Powell LE, Myers AM (1995) The activities-specific balance confidence (ABC) scale. J Gerontol A Biol Sci Med Sci 50:28–34
Hatch J, Gill-Body KM, Portney LG (2003) Determinants of balance confidence in community-dwelling elderly people. Phys Ther 83:1072–1079
Podsiadlo D, Richardson S (1991) The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 39:142–148
Khajavi D (2017) Psychometric properties of persian translated version of activities-specific balance confidence scale (ABC) in community-dwelling older adults. Arak Med Univ J 20:39–48
Ware JE Jr (2000) SF-36 health survey update. Spine 25:3130–3139
Montazeri A, Goshtasebi A, Vahdaninia M et al (2005) The Short Form Health Survey (SF-36): translation and validation study of the Iranian version. Qual Life Res 14:875–882
Montazeri A, Goshtasbi A, Vahdaninia M (2004) Translation, reliability and validity of Persia type of SF-36 Standard instrument. Payesh 5:49–56
Li X, Zhou P, Aruin AS (2007) Teager-Kaiser energy operation of surface EMG improves muscle activity onset detection. Ann Biomed Eng 1:1532–1538
Solnik S, DeVita P, Rider P et al (2008) Teager–Kaiser operator improves the accuracy of EMG onset detection independent of signal-to-noise ratio. Acta Bioeng Biomech 10:65
Inglin B, Woollacott M (1988) Age-related changes in anticipatory postural adjustments associated with arm movements. J Gerontol 43:105–113
Asaka T, Wang Y (2011) Feedforward postural muscle modes and multi-mode coordination in mild cerebellar ataxia. Exp Brain Res 210:153–163
Massion J (1992) Movement, posture and equilibrium: interaction and coordination. Prog Neurobiol 38:35–56
Hylin MJ, Kerr AL, Holden R (2017) Understanding the mechanisms of recovery and/or compensation following injury. Neural Plast
Lajoie Y, Gallagher SP (2004) Predicting falls within the elderly community: comparison of postural sway, reaction time, the Berg balance scale and the Activities-specific Balance Confidence (ABC) scale for comparing fallers and non-fallers. Arch Gerontol Geriatr 38:11–26
Sattin RW, Easley KA, Wolf SL et al (2005) Reduction in fear of falling through intense tai chi exercise training in older, transitionally frail adults. J Am Geriatr Soc 53:1168–1178
Josephs S, Pratt ML, Meadows EC et al (2016) The effectiveness of Pilates on balance and falls in community dwelling older adults. J Bodyw Mov Ther 20:815–823
Bennie S, Bruner K, Dizon A et al (2003) Measurements of balance: comparison of the timed “Up and Go” test and Functional Reach test with the Berg Balance Scale. J Phys Ther Sci 15:93–97
van Iersel MB, Munneke M, Esselink RA et al (2008) Gait velocity and the Timed-Up-and-Go test were sensitive to changes in mobility in frail elderly patients. J Clin Epidemiol 61:186–191
Khajavi D, Farrokhi A, Jaberi-Moghaddam A et al (2016) Effect of strength and balance training program on maintaining balance and quality of life in older male adults with fear of fall. Iran J Ageing 11:270–279
dos Santos M, Komeroski IG, Monteiro EP et al (2018) Effects of dance practice on functional mobility, motor symptoms and quality of life in people with Parkinson’s disease: a systematic review with meta-analysis. Aging Clin Exp Res 30:727–735
Silva MR, Alberton CL, Portella EG et al (2018) Water-based aerobic and combined training in elderly women: effects on functional capacity and quality of life. Exp Gerontol 106:54–60
Taraldsen K, Chastin SF, Riphagen II et al (2012) Physical activity monitoring by use of accelerometer-based body-worn sensors in older adults: a systematic literature review of current knowledge and applications. Maturitas 71:13–19
Funding
This research did not receive any specific grant from funding agencies, public, commercial, or non-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report that there is no conflict of interest.
Statement of human and animal rights
This study was approved by the Research Ethics Board of University of Isfahan.
Informed consent
At the beginning of the study, we explained the study to all potential participants and answered their questions. We just used those participants who signed the written informed consent form.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Arghavani, H., Zolaktaf, V. & Lenjannejadian, S. Comparing the effects of anticipatory postural adjustments focused training and balance training on postural preparation, balance confidence and quality of life in elderly with history of a fall. Aging Clin Exp Res 32, 1757–1765 (2020). https://doi.org/10.1007/s40520-019-01358-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-019-01358-5