
Abstract
Background
The sit-to-stand movement requires balance control and coordination between the trunk and lower limbs. For these reasons, it is commonly used in clinics for evaluating lower limb muscle function in the elderly. The aim of the present study was to point out re levant biomechanical and neurophysiological sit-to-stand parameters allowing comparison between elderly fallers and non-fallers.
Methods
Ten elderly fallers and thirty non-fallers performed sit-to-stand movements. Sit-to-stand mechanical (maximal and mean force, impulse) and temporal parameters were measured in the vertical and anteroposterior axes using force platforms. Activity of rectus femoris, vastus lateralis, and gastrocnemius lateralis muscles was bilaterally recorded by surface electromyography.
Results
Time to realize sit-to-stand movements was significantly longer in elderly fallers compared to non-fallers (p < 0.05). In the same way, maximal vertical force and mean posterior force applied on force platform were significantly lower (p < 0.05) in fallers than in non-fallers individual. At muscular activity level, results showed a main statistical difference in gastrocnemius lateralis muscle activity patterns between faller and non-faller groups.
Conclusion
Vertical and anteroposterior data from force platform, and gastrocnemius lateralis muscle activity determined during sit-to-stand movement are the most relevant parameters to differentiate fallers and non-fallers. Moreover, these factors highlight different strategies to rise from a chair between faller and non-faller group, suggesting that fallers would constantly adjust their control balance during the sit-to-stand movement.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Aging causes changes in the neuromuscular system such as strength loss and alteration of muscle activation (i.e., dynapenia) [1] which creates a deficit in the production of an optimal motor response and impairs motion control during activities of daily living. Then, decline of neuromuscular factor, combined with the sensorimotor system decrease with aging has important functional consequences such as difficulty to rise from a chair [2] and increased risk of falling [3]. Moreover, the occurrence of falls is related to various factors as a disturbed sense of balance [6], lower body instability [7], and functional limitations [8].
Despite the importance of fall occurrence in public health, no reliable processes evaluating the risk of fall are available, while several methods are mobilized to monitor the elderly, such as postural tests and physical scales. All these evaluations are widely used because they are easy to apply and provide a good index of postural aging. However, they often suffer of a lack of standardization [9] and of reproducibility [10]. Thus, they are considered to give poor predictive values for falling risk in the elderly [4, 5]. Among classical tests used, the sit-to-stand movement requires coordination between the trunk and lower limbs balance and stability [11–14]. So, it deals with skills and autonomy of elderly people. Because of the reduced physical burden on the subjects and the low risk of inducing disorders [15], STS remains a common test for clinical assessments of the lower limb muscle function in the elderly [16]. Nevertheless, when it is coupled with force platform, it can allow better discriminating motor behavior in a specific population such as elderly people [12, 17]. Previous studies focused on comparing young adults and elderly through STS movement force platform data [15, 18, 19]. For example, it was shown that the horizontal component of ground reaction forces was greater in younger subjects, reflecting the difficulties in ensuring postural control in elderly people [19]. Likewise, postural adaptation was highlighted by the earlier activation of soleus and gastrocnemius muscles in the elderly to prepare the transfer of body weight before seat-off [19]. Such differences were attributed to the development of compensatory strategies for balance control during STS [20]. All these results also suggest that the different potentials in lower limb muscle force and/or muscle activation strategies, objectified by dynamic and electromyographic (EMG) measurements, could be used to discriminate faller to non-faller profiles.
All these characteristics, associated with lower muscular strength in lower limb in the elderly with fall experience (i.e., faller group vs. non-fallers) [21–23], can cause a different strategies employed by these two population to stand up.
The aim of the present study was to point out the most relevant mechanical (force platform measurements) and muscular (EMG activity) parameters that could allow differentiating a group of elderly fallers (FG) from a group of non-fallers people (NFG), during STS movement.
Materials and methods
Population
Forty women aged from 64 to 79 years volunteered to participate in the present study. Subjects were split into two groups: (1) a non-faller group (NFG, n = 30) without history of fall and (2) a faller group (FG, n = 10) with subjects who had a previous history of at least one or more falls in the year preceding the test. A fall was defined as an event in which an individual unintentionally drops onto the ground or at a lower level [24], excluding environmental causes (e.g., rushes and snow). Subjects’ anthropometric data are presented in Table 1. All participants were living in community dwelling and were devoid of any pathology.
Protocol
Each participant performed a set of five repeated STS movements as quickly as possible [25]. Subjects had to keep their starting (sitting) and final (standing) position during 5 s before performing the following STS movement.
To reduce the required work for full knee extension and stand up [26], chair-seat height was adjusted according to Perennou [27], i.e., each subject’s lower leg length with a 90° knee angle when seated. STS movements were performed with participants’ arms crossed on their chest, in order to standardize the position and to suppress the influence of arm swaying [17] on STS strategy and force platform parameters as described elsewhere [25].
Ground reaction force recording and processing
During all STS movements, ground reaction forces (GRF) were recorded using two force platforms (type 9286BA, Kistler Group, Winterthur, Switzerland) placed under each foot. Each platform recorded the ground reaction force of each lower limb. To determine a global dynamic force in the vertical and anteroposterior axes, it must sum the values of the two platforms. Data were recorded at 100 Hz. Offset was made without any load on the platform (i.e., before the subject stood on the plate).
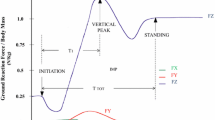
GRF data were processed offline with Bioware® software (V5.1.0.0, Kistler Group, Winterthur, Switzerland), and with custom-built Matlab scripts (R2008b, The Mathworks, Natick, Massachussetts, USA). According to Etnyre and Thomas [17], STS movement began with a relief phase and ended when the vertical component of the GRF normalized relative to the body weight was equal to one, which meant that the subject was standing. From the force–time curves, several parameters were determined during STS movement (Fig. 1a): peak GRF (F Peak, in N kg−1), average GRF produced during the complete STS (F mean, in N kg−1), time to reach F Peak (T 1, in s), STS total time (T tot, in s); STS Impulse (Imp, in N kg−1 s) which corresponded to the area under the force–time curve during total STS movement. Each parameter was analyzed according to the vertical (z) and anteroposterior (y) axes. For all parameters, data were expressed as the mean ± standard deviation (SD) of the five trials. Anterior (y ANT) and posterior (y POST) directions were differentiated in the analysis of results.

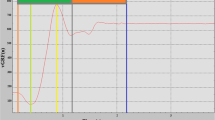
Synchronization between EMG and STS parameters. a Typical example of a sit-to-stand (STS) vertical and anteroposterior force–time curve recorded from a force platform (modified from Etnyre et al. 2007); Fz vertical force curve, Fy anteroposterior force curve, F Peak peak GRF, F mean average GRF produced during the complete STS, T 1 time to reach peak GRF, T tot STS total time, Imp corresponds to the area under the force–time curve during the total STS. b Synchronization between EMG (i.e., vastus lateralis left) and platform data. T ISO time between initiation of STS and seat-off, T DYN1 time between seat-off and F Peak, T DYN2 time between F Peak and the relief peak, T DYN3 time between relief peak and stand up position
Surface electromyographic recording and processing
During the STS movement, surface electromyographic signals (EMG) of rectus femoris (RF), vastus lateralis (VL), and gastrocnemius lateralis (GL) muscles were bilaterally recorded and analyzed to evaluate any potential functional asymmetry between both lower limbs. For each muscle, dry surface electrode (Delsys DE 2.1, Delsys Inc, Boston, USA; 1-cm interelectrode distance) was attached on the skin. Before electrode application, the skin was shaved and cleaned with alcohol to minimize impedance. Electrodes were placed on the muscle bellies, longitudinally with respect to the underlying muscle fibers arrangement and were located according to the recommendations of SENIAM (surface EMG or non-invasive assessment of muscles) [28]. The wires connected to the electrodes were well secured with adhesive tape. EMG signals were amplified (1000×) and digitized (6–450 Hz bandwidth) at a sampling rate of 2 kHz (Delsys Myomonitor IV, Delsys Inc., Boston, USA), and stored on a computer.
Surface EMG signals were processed offline with custom-built Matlab scripts (R2008b, The Mathworks, Natick, Massachussetts, USA). First, EMG signals were band-pass filtered (10–450 Hz, 4th order Butterworth filter) to ensure that the signals were free of any potential artifacts induced by muscle vibrations contained in low frequencies [29]. Then, the linear envelop of the rectified EMG signals was calculated by using a zero lag low-pass filter (10 Hz, 4th order Butterworth filter). EMG profiles were normalized by their respective maximum value obtained during the STS movement, thereby obtaining values of relative activation between 0 and 1. EMG results were presented by mean muscle activation into each STS phase.
Sit-to-stand phases
An electronic goniometer was placed on the knee joint (Delsys Inc, Boston, USA, full range of ±180°, precision of ±0.5°) to verify initial condition respect. Goniometer was synchronized with the EMG measurements and allowed determining the seat-off phase and the end of the movement. STS movement has been splitted into two phases: 1/the first one is an isometric lower limb phase (T ISO) (i.e., lower limbs did not move) corresponding to the time interval between the initiation of STS (i.e., relief phase) and the seat-off; 2/the second phase is a dynamic phase (T DYN), during which lower limbs are actually in movement, that begins from the seat-off until the end of movement (i.e., stand up position). The dynamic phase can be divided in three consecutive time periods (Fig. 1b), defined relatively to the GRF signal. The period 1 corresponded to the time between the beginning of dynamic phase and F Peak (T DYN1). Then, the period 2 ran from F Peak to the relief peak (T DYN2). Finally, the period 3 corresponded to the time between relief peak and stand up position (T DYN3).
These phases of STS finally correspond to (1) trunk flexion (T ISO), (2) verticalization (T DYN1 and T DYN2), and (3) stabilization (T DYN3) of the STS movement, typically referred in the literature [30, 31].
Statistical analysis
Data are presented as their mean ± SD. Skewness and Kurtosis analysis was used to verify the normality of distribution and homogeneity of variance in the datasets. Since all data followed a normal distribution, a one-way ANOVA with repeated measures was applied to determine the significant differences between the two groups (NFG vs. FG) for platform data. A one-way ANOVA was applied for EMG data. Tukey and Kramer post hoc comparisons were carried out to identify pairwise differences in muscle activation between all phases. Power analysis was estimated by using the method of averages of two independent groups [32]. Power was considered as excellent when its value ranges between 0.8 and 1, good between 0.6 and <0.8, and low for values <0.6. For all statistical procedures, significance threshold was set at p < 0.05.
Results
Force platform parameters
Whatever the considered group and force platform parameters, no significant differences were observed between data recorded on both right and left sides, meaning that there was no asymmetry considering all the subjects during STS. Consequently, parameters related to the force platforms corresponded to the combined recordings from the two force platforms (i.e., as if only one force plate was used), to determine a global dynamic force in the vertical and anteroposterior axes.
Mean platform parameters determined during STS for each group (NFG and FG) are presented in Table 2. During STS, T TOT (1.57 vs. 1.43 s) was significantly longer in FG than NFG (p < 0.05). Also, F ZPeak and F YMEAN POST were significantly (p > 0.05) greater in NFG than in FG (+7 and +38 %, respectively). Inversely, ImpZ (7.2 vs. 12.3 N kg−1 s, respectively) and ImpY POST (379.4 vs. 436.1 N kg−1 s, respectively) were found to be significantly smaller in NFG.
EMG analysis
EMG of rectus femoris (RF), vastus lateralis (VL), and gastrocnemius lateralis (GL) muscles were bilaterally recorded and analyzed, but no significant differences were observed between data recorded on both right and left sides. Thus, only results from the dominant leg (i.e., right) were presented. Mean muscle activations in both populations are presented in Fig. 2, and the power analysis was equal to 1 for all EMG results.

Sequence of muscular activation movements in old subjects during sit-to-stand movement. RFR rectus femoris right side, VLR vastus lateralis right side, GLR gastrocnemius lateralis right side
EMG measurements revealed a phase effect for each group and each muscle. For instance, the mean activation of RF and VL muscles was the highest (RF: 62.6 vs. 61.4 % and VL: 52.6 vs. 58.4 %, respectively for FG vs. NFG) at the beginning of the dynamic phase (T DYN1), and decreased after reaching the maximum vertical force (T DYN2 and T DYN3) in both populations. However, the GL muscles activities exhibited some intergroup discrepancies. Indeed, there was a gradual and progressive increase in the mean activation of the GL muscles during STS for NFG (T ISO = 22.4 %, T DYN1 = 35.6 %, T DYN2 = 58.4 %, and T DYN3 = 72.9 %), while the mean activation of the GL muscles displayed an almost constant period with no significant differences (between T ISO = 37.6 %, T DYN1 = 44.9 % and T DYN2 = 50.4 %) for FG. The mean activation for these three phases (T ISO, T DYN1, and T DYN2) was significantly different to T DYN3 (75.8 %) for FG.
Discussion
The aim of the present study was to determine mechanical and muscular STS parameters that could be relevant for comparing a group of elderly fallers (FG) to a group of non-fallers (NFG) from force platform and muscle activation parameters when executing fast STS movements. Results showed significant discrepancies in force platform parameters and mean activation of the GL between FG and NFG assuming different motion strategies to rise from a chair in the two groups.
Force platform parameters
Among the various factors involved in fall occurrence, the “lower body instability” plays an essential role [7]. Whatever the considered group, results of the present study presented no statistical difference between the two lower limbs concerning the force platform parameters. This shows that our FG is not affected by lower limb asymmetry. Nevertheless, results indicated that several parameters can be proposed to discriminate fallers and non-fallers behavior. One can assume that difference between the two groups is mainly due to the fact that fallers are more careful during movements of daily living. This is supported by the longer time observed during STS. Kim and Shin [33] showed that the elderly with fall experience performed movements with relatively less stability, implying to take more time to complete a movement. Concerning the kinetic parameters, when the STS movement was performed as fast as possible, results revealed significant difference in the force production between the two groups. Indeed, the maximal vertical force (F ZPeak) produced by NFG was significantly higher (p < 0.05) than the one produced by FG (1.27 vs. 1.20 N kg−1, respectively). As previously reported, this may reflect a lack of strength in lower limbs of fallers [22, 23], and confirm that loss of muscle strength is a main risk factor for falls [34]. Moreover, the stronger and faster performance levels on STS release in NFG than in FG may be assigned to the phenomenon of sarcopenia. Indeed, sarcopenia is characterized by a loss of the number and size in type 2 muscle (fast-twitch) fibers with age, which causes a lower level of force production [35] and affects the speed of movements.
Comparison of dynamic parameters between the two groups also revealed a significant higher F YMEAN POST in fallers. Yoshida et al. [36] demonstrated that the forward lean was greater in healthy elderly subjects than in young healthy subject. From the Yoshida et al. [36] results, one can assume that fallers need to lean forward more than non-fallers, inducing a backward imbalance during the backward return of the trunk. By definition, the STS movement is a transitional movement where the center of mass moves from a stable position to a less stable position over extended lower extremities [37]. It was previously suggested that the time to perform the lower limb extension was related to the center of mass position in order to ensure both a change in direction (from horizontal to vertical) and the preservation of equilibrium [38]. To preserve their equilibrium, elderly people should perform an important trunk flexion before extending the leg. This anteroposterior trunk flexion may be more accentuated in fallers, assuming that aging induces the development of compensatory strategies on balance control during STS movement, which could probably be objectified by kinematic measurements.
Generally, two functional strategies can be described when performing STS movement. The first one consists in producing a small trunk flexion to transfer forwards and then to begin the seat-off [39]; the second way consists in increasing trunk flexion before initializing the movement [20]. The first strategy involves more strength to stand up and is preferentially performed by our non-fallers’ subjects; the second one involves a more pronounced anteroposterior swing as observed in fallers. Consequently, preferentially performing a strategy rather than the other one could explain the differences in the force platform parameters (F ZPeaK, F YMEAN POST) between FG and NFG. Further investigations including video analysis should be done to verify this hypothesis.
Electromyography
In the present study, muscle activation analysis only focused on lower limbs muscles which mainly contribute to ensure greater autonomy in all daily activities. Indeed, Wretenberg and Arborelius [40] showed that the knee extensors represent 72 % of the total concentric work produced when rising from a chair and are often considered as the main actor in the STS [41]. Results of the present study demonstrated that muscles were activated before the seat-off (T ISO), whatever the considered group suggesting a pre-activation of lower limb muscles before their extension to rise, as already shown by Groos et al. [19]. Results also indicated that RF and VL were activated in the same way during STS, with no statistical difference between the two subjects’ groups, but revealed that the main difference between FG and NFG results in the sequence of GL muscle activity during STS. In fact, it can be observed that muscle activity of GL increased significantly during each phase only in non-faller group, whereas it remains quite identical during T ISO, T DYN1, and T DYN2 for FG. However, it can be noted that, whatever the considered group, the maximal activity of the GL muscle was observed in T DYN3 phase. According to this observation, several studies [42, 43] observed that the triceps surae muscles contributed to postural adjustments during STS movement and were activated at the end of STS, having an important postural role for standing stability [44]. Our results suggest that GL muscles are also involved in preparatory and accompanying postural movement, and allow for controlling balance during STS. So, fallers would adjust their control balance constantly during the STS movement as objectified by the GL activity.
One can think that elderly fallers and non-fallers use a different strategy to perform STS movement, explain by significant difference of anteroposterior data and a different muscular activity distribution. Indeed, it is commonly accepted that the GL allows to control equilibrium [19, 30, 31, 37]. Because VL and RF are activated when the center of gravity is adequately positioned, this suggests that subjects comply a motor program consisting in triggering the muscles that are used to perform sit-to-stand movement (quadriceps) when they are placed in a stable position. Such an observation is in accordance with previous finding from Goulard and Valls-Solé [44] who suggested that “the pattern of lumbar paraspinal, quadriceps, and hamstrings, is likely a centrally programmed sequence of activation, and this motor program is probably executed only when the preparatory postural muscles have ensured that the center of gravity is appropriately placed.” This hypothesis can explain the difference in the pattern of GL muscle activity and the similarity in the VL and RF muscles activity pattern between fallers and non-fallers, in connection with different strategies to rise of chair mentioned. The motor program is the same but the adequate stability condition to begin the stand phase of STS movement is different.
Practical applications
To the authors’ knowledge, differentiation between fallers and non-fallers in elderly has never been done by associating mechanical and neuromuscular parameters like horizontal and vertical ground reaction forces and gastrocnemius muscular activity, etc., during a sit-to-stand movement at high speed. When exist, such measurements mainly concern comparison between elderly and young people [19]. Comparing population of similar age presents higher interest for clinicians, and also for elderly subjects, allowing to, propose some keys in their rehabilitation and/or reinforcement (i.e., squat exercise and proprioception exercise to work equilibrium). Moreover, the sit-to-stand movement, which is a repetitive daily activity can allow detecting information on the muscular deficit, especially at the hip [19] and knee levels. Indeed, despite a strategy which requires higher energy/strength level, elderly fallers favor balance control, even during fast movement [45], and mainly during the knee extension phase. Indeed, elderly fallers reduce their body moment of inertia by flexing their trunk, bringing their upper body nearest the body center of mass. This allows them to control their balance, but requires a greater force production during the knee extension, since the movement is not carried out in one step. This seems paradoxal in comparison with previous studies showing that elderly fallers present a less muscular strength in lower limb that non-faller ones [22, 23]. This continuous preservation of the balance is supported by electromyographic results.
Findings of the present study point out that elderly fallers and non-fallers use different strategies to achieve the sit-to-stand movement. The first strategy, called “moment-transfer” [46], induces an important speed on the anteroposterior component of the subject’s center of mass, due to a kinetic energy transfer during flexion of the trunk to stand up. The trunk flexion causes a great strength production in the lower limbs before the seat-off moment. This strategy requires a high level of equilibrium control and is the most common way among non-disabled people [39], corresponding to non-faller people in the present study. The second strategy, called “stabilization strategy” [46], consists on bringing the center of mass above the support polygon, before the seat-off, upon important trunk flexion. Subsequently, the subject performs a knee extension phase to stand up. This strategy focuses on postural stability and is usually used by people with muscle weakness in the lower limbs [20], corresponding to the faller subjects of the present study. This finding was supported by the kinematic results obtained in the present study (i.e., trunk flexion, trunk angular velocity, etc.) which offer the perspective of analyzing easily and quickly the sit-to-stand movement thanks to a simple 2D video capture. This represents a promising opportunity to characterize the different sit-to-stand strategies. Indeed, in clinical practice, a video camera (2D analysis) would be a more available tool and easy to use than a 3D force platform coupled with surface electromyography. The improving technology for the development of smartphones (e.g., video resolution and recording rate) and the growing range of applications gives us the reasons to think that determining sit-to-stand strategies in elderly would be greatly facilitated in the near future.
Conclusion
This study determined mechanical and muscular STS parameters that are relevant for distinguishing a group of elderly fallers vs. a group of non-fallers. Our main results also demonstrated differences in anteroposterior and vertical dynamometric parameters, and a different pattern of GL muscle activity. The differences reported between fallers and non-fallers could be explained by a different motion strategy to rise from a chair. A video analysis should be useful to verify this hypothesis. Finally, one can also ask if there are one or more threshold values from force platform parameters that discriminate fallers and non-fallers
Abbreviations
- ANOVA:
-
Analysis of variance
- EMG:
-
Electromyography
- FG:
-
Faller group
- GL:
-
Gastrocnemius lateralis
- GRF:
-
Ground reaction force
- NFG:
-
Non-faller group
- RF:
-
Rectus femoris
- STS:
-
Sit to stand
- TUG:
-
Timed up and go test
- VL:
-
Vastus lateralis
References
Clark BC, Manini TM (2008) Sarcopenia ≠ dynapenia. J Gerontol A Biol Sci Med Sci 63:829–834
Kuh D, Hardy R, Butterworth S et al (2006) Developmental origins of midlife physical performance: evidence from a British birth cohort. Am J Epidemiol 164:110–121
Orr R, de Vos NJ, Singh NA et al (2006) Power training improves balance in healthy older adults. J Gerontol A Biol Sci Med Sci 61:78–85
Bloem BR, Boers I, Cramer M et al (2001) Falls in the elderly. I. Identification of risk factors. Wien Klin Wochenschr 113:352–362
Gerdhem P, Ringsberg KA, Akesson K et al (2005) Clinical history and biologic age predicted falls better than objective functional tests. J Clin Epidemiol 58:226–232
Jung YM, Lee SE, Chung KS (2006) Prevalence and associated factors of falls according to health status in elderly living in the community. J Korean Gerontol Soc 26:291e303
Tinetti ME, Speechley M, Ginter SF (1988) Risk factors for falls among persons living in the community. N Engl J Med 319:1701–1707
Pluijm SM, Smit JH, Tromp EA et al (2006) A risk profile for identifying community-dwelling elderly with a high risk of recurrent falling: results of a 3-year prospective study. Osteopor Int 17:417e425
Siggeirsdottir K, Jonsson BY, Jonsson H Jr et al (2002) The timed ‘Up & Go’ is dependent on chair type. Clin Rehabil 16:609–616
Rockwood K, Awalt E, Carver D et al (2000) Feasibility and measurement properties of the functional reach and the timed up and go tests in the Canadian study of health and aging. J Gerontol A Biol Sci Med Sci 55:M70–M73
Galli M, Cimolin V, Crivellini M et al (2008) Quantitative analysis of sit to stand movement: experimental set-up definition and application to healthy and hemiplegic adults. Gait Posture 28:80–85
Fotoohabadi R, Tully EA, Galea P (2012) Kinematics of rising from a chair: image- based analysis of the sagittal hip-spine movement pattern in elderly people who are healthy. Phys Ther 90:561–571
Wall JC, Bell C, Campbell S et al (2000) The timed get-up-and-go test revisited: measurement of the component tasks. J Rehabil Res Dev 37:109–113
Burnett DR, Campbell-Kyureghyan NH, Cerrito PB et al (2011) Symmetry of ground reaction forces and muscle activity in asymptomatic subjects during walking, sit-to-stand, and stand-to-sit tasks. J Electromyogr Kinesiol 21:610–615
Yamada T, Demura S (2009) Relationships between ground reaction force parameters during a sit-to-stand movement and physical activity and falling risk of the elderly and a comparison of the movement characteristics between the young and the elderly. Arch Gerontol Geriatr 48:73–77
Jones CJ, Rikli RE, Beam WC (1999) A 30-s chair-stand test as a measure of lower body strength in community-residing older adults. Res Q Exerc Sport 70:113–119
Etnyre B, Thomas DQ (2007) Event standardization of sit-to-stand movements. Phys Ther 87:1651–1666
Papa E, Cappozzo A (2000) Sit-to-stand motor strategies investigated in able-bodied young and elderly subjects. J Biomech 33:1113–1122
Gross MM, Stevenson PJ, Charette SL et al (1998) Effect of muscle strength and movement speed on the biomechanics of rising from a chair in healthy elderly and young women. Gait Posture 8:175–185
Cuesta-Vargas AI, Gonzalez-Sanchez M (2013) Differences in muscle activation patterns during sit to stand task among subjects with and without intellectual disability. Biomed Res Int:173–178
Shin KR, Kang Y, Jung D et al (2012) A comparative study on physical function test between faller group and nonfaller group among community-dwelling elderly. Asian Nurs Res 6:42e48
Chung JW, Choi HJ (2009) Functional fitness and asymmetry on lower body muscle strength of elderly women with fall experience. Kinesiology 11:65–72
Sung SC, Kang CG, Lee MG (2007) Effects of falling experience on physical fitness, isokinetic leg strength, and balance in the elderly women. Korean J Phys Educ 46:503–515
Hauer K, Becker C, Lindemann U et al (2006) Effectiveness of physical training on motor performance and fall prevention in cognitively impaired older persons: a systematic review. Am J Phys Med Rehabil 85:847–857
Chorin F, Rahmani A, Beaune B et al (2015) Determination of reliable force platform parameters and number of trial to evaluate sit-to-stand movement. Aging Clin Exp Res 27:473–482
Chen S-H, Lee Y-H, Chiou W-K et al (2010) A pilot study examining seat heights and subjective ratings during rising and sitting. Inter J Ind Ergon 40:41–46
Perennou D, Decavel P, Manckoundia P et al (2005) Evaluation of balance in neurologic and geriatric disorders. Ann Readapt Med Phys 48:317–335
Hermens HJ, Freriks B, Disselhorst-Klug C et al (2000) Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol 10:361–374
Conforto S, D’Alessio T, Pignatelli S (1999) Optimal rejection of movement artefacts from myoelectric signals by means of a wavelet filtering procedure. J Electromyogr Kinesiol 9:47–57
Schenkman M, Berger RA, Riley PO et al (1990) Whole-body movements during rising to standing from sitting. Phys Ther 70:L638–L648 (discussion 648–651)
Kralj A, Jaeger RJ, Munih M (1990) Analysis of standing up and sitting down in humans: definitions and normative data presentation. J Biomech 23:1123–1138
Jones SR, Carley S, Harrison M (2003) An introduction to power and sample size estimation. Emerg Med J 20:453–458
Kim CB, Shin JY (2005) Analysis of gait movement following the fall experience and non-experience in the elderly. Korea Sport Res 16:85–92
Bento PC, Pereira G, Ugrinowitsch C et al (2010) Peak torque and rate of torque development in elderly with and without fall history. Clin Biomech 25:450–454
Aoyagi Y, Shephard RJ (1992) Aging and muscle function. Sports Med 14:376–396
Yoshida K, Iwakura H, Inoue F (1983) Motion analysis in the movements of standing up from and sitting down on a chair. A comparison of normal and hemiparetic subjects and the differences of sex and age among the normals. Scand J Rehabil Med 15:133–140
Vander Linden DW, Brunt D, McCulloch MU (1994) Variant and invariant characteristics of the sit-to-stand task in healthy elderly adults. Arch Phys Med Rehabil 75:653–660
Carr JH (1992) Balancing the centre of mass during standing up. Physiother Theory Pract 8:159–164
Hale L, Bray A, Littmann A (2007) Assessing the balance capabilities of people with profound intellectual disabilities who have experienced a fall. J Intellect Disabil Res 51:260–268
Wretenberg P, Arborelius UP (1994) Power and work produced in different leg muscle groups when rising from a chair. Eur J Appl Physiol Occup Physiol 68:413–417
Dehail P, Bestaven E, Muller F et al (2007) Kinematic and electromyographic analysis of rising from a chair during a “sit-to-walk” task in elderly subjects: role of strength. Clin Biomech 22:1096–1103
Khemlani MM, Carr JH, Crosbie WJ (1999) Muscle synergies and joint linkages in sit-to-stand under two initial foot positions. Clin Biomech 14:236–246
Magnan A, McFadyen BJ, St. Vincent G (1996) Modification of the sit-to-stand task with the addition of gait initiation. Gait Posture 4:232–241
Goulart FR, Valls-Sole J (1999) Patterned electromyographic activity in the sit-to-stand movement. Clin Neurophysiol 110:1634–1640
Schultz AB (1992) Mobility impairment in the elderly: challenges for biomechanics research. J Biomech 25:519–528
Hughes MA, Weiner DK, Schenkman ML et al (1994) Chair rise strategies in the elderly. Clin Biomech (Bristol, Avon) 9:187–192
Acknowledgments
The authors are grateful to the participants for their involvement in this study. This study was supported by grants from the Region des Pays de la Loire (France), for the project “RP3AP.” The authors would like to thank Sébastien Boyas for his useful comments that helped improving the quality of this manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors have participated in (a) conception and design, or analysis and interpretation of the data; (b) drafting the article or revising it critically for important intellectual content; and (c) approval of the final version. The authors have no affiliation with any organization with a direct or indirect financial interest in the subject matter discussed in the manuscript.
Statement of human and animal rights
The experimental design of the study was performed in accordance with the Declaration of Helsinki (last modified in 2004).
Informed consent
They were informed of the possible risk and discomfort associated with the experimental procedures before they gave written consent.
Rights and permissions
About this article

Cite this article
Chorin, F., Cornu, C., Beaune, B. et al. Sit to stand in elderly fallers vs non-fallers: new insights from force platform and electromyography data. Aging Clin Exp Res 28, 871–879 (2016). https://doi.org/10.1007/s40520-015-0486-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-015-0486-1