
Abstract
Background
Sit-to-stand (STS) movement is useful for evaluating lower limb muscle function, especially from force platforms. Nevertheless, due to a lack of standardization of the STS movement (e.g., position, subject’s instructions, etc.), it is difficult to compare results obtained in previous studies.
Aims
The aim of the present study was to determine the most relevant condition, parameters, and number of trial to perform STS movements.
Methods
In this study, STS mechanical (maximal and mean force, impulse) and temporal parameters were measured in the vertical, medio-lateral and antero-posterior axes using a force platform. Five STS conditions (i.e., with or without armrests, variation of the height of the chair and the movement speed) were analyzed to evaluate repeatability of different standardized procedures.
Results
Most of the mechanical and temporal parameters were influenced by the STS condition (p < 0.05). Regarding vertical axis, results showed a strong to perfect repeatability for all parameters (0.72 < ICC < 0.9) for only one condition: STS performed as rapidly as possible with a 90° knee angle when seated, without using armrests. Regardless conditions of performance, our results also showed that the most repeatable parameters were mean and peak force in medio-lateral axis, and the impulse measured in the three directions. Three trials should be performed to reach high repeatability.
Conclusion
Our results suggest that the fast condition, with a 90° knee joint angle, with arms crossed over the chest, is the most reliable condition to evaluate performance during STS movement.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Standing up from a chair, so-called sit-to-stand (STS) movement, is one of the fundamental daily living activities performed by an individual that calls upon coordination and accurate balance control [1]. STS requires coordinated interaction of body segments to move the body’s center of mass of an individual in a horizontal and vertical direction by balancing above a small support [2]. It is considered as a functional prerequisite for many daily tasks and consequently independent life [3, 4]. Indeed, STS is consequently often used during clinical assessments as it has been reported to be a relevant tool for the evaluation of leg muscle function [5], and individual motor ability [6]. This test is associated with limited physical burden placed on participants and low risks of induced disorders [7, 8]. Clinically, STS is often used to evaluate the imbalance especially in the elderly [4], hemiparetic [9] and amputee [10, 11] populations. This kind of evaluation is also conventionally used as an indicator of postural control [12], and as a mean to assess the risk of falling associated with muscle strength in the lower limbs [13]. Moreover, STS evaluation allows assessing strength of knee flexors and extensors and/or hip concentric and eccentric mode without the use of specific scientific equipment. It provides information on the physical profile of subjects and functional limitations of the lower limbs. In the elderly, it is an objective measure of physical ability to identify people at high risk of falling [14], related with the level of autonomy of the elderly.
Parameters associated with the performance of a STS movement (e.g. force, velocity, impulse, etc.) can easily be determined using a force platform [15]. However, no consensus has been established yet to standardize the initial position and subjects’ instructions during STS. Indeed, previous studies [16, 17], have demonstrated that vertical, antero-posterior and medio-lateral ground reaction forces (GRF) are not influenced by the position of the arms (crossed over the chest, setting free, or hands on knee), unlike height of chair set and/or use of arm rest clearly and foot position, during STS performance. Due to this lack of standardization in the STS procedures [16], some discrepancies are observed when comparing results from previous studies. In general, each study tried to find its own parameters, with available laboratory equipment and varied purposes [15]. Moreover, inter-individual differences exist in performing STS movement [18], reflecting the use of different strategies [19, 20] which influence force and moment components [21]. Generally differentiated by the degree of trunk flexion before the separation of the seat (i.e. seat off) [22], measuring the horizontal linear momentum required moving from a stable position (e.g. before seat-off) to unstable position (e.g. after seat-off) takes all sense. This observation shows the importance of studying the data in the three axes (i.e., antero-posterior, medio-lateral and vertical) during STS movement, and be able to refer to relevant way. To our knowledge, no parameters were shown to be relevant to discriminate individual specific behavior during STS movement.
The purpose of the present study was twofold: (1) to determine the most relevant and reliable parameters to assess the STS movement from a force platform and (2) to evaluate the repeatability of different standardized procedures to identify the necessary number of trials to get a reliable assessment.
Materials and methods
Subjects
Twenty-one male subjects (i.e., student, member of laboratory, and staff university), aged from 21 to 60 years volunteered to participate in this study. The mean ± standard deviation age, height and body mass were 33.9 ± 12.3 years, 1.79 ± 0.07 m, 79.1 ± 12.3 kg, respectively. All subjects answered to a call of volunteer to participate in the study, and they accepted to realize the experimental protocol after being informed on it. Subjects reported no lower limbs injury and/or feel pain. They were not wearing prosthesis and declared to have neither neurological problem (i.e., AVC) nor drug treatment. Anyone recognizing injuries were excluded from the study. All the subjects were devoided of any lower limbs and/or lumbar pathologies. All the volunteers were informed about the experimental procedure that conformed to the Declaration of Helsinki (last modified in 2004).
Material
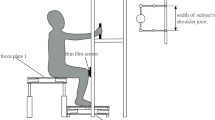
Ground Reaction Force measurements were performed using a force platform (9286BA, Kistler Group, Winterthur, Switzerland) placed under the feet of the subjects. Analog signals issued from the force plate were amplified by charge amplifiers (Kistler type 5691A1). Force signals were linear (<±0.2 %) over a range of 0–10 kN in the vertical axis, and of −2.5 to 2.5 kN in the antero-posterior and medio-lateral axis. Data were collected using BIOWARE V5.1.0.0 software, and recording was performed at 100 Hz. Data processing was performed using MATLAB scripts (R2008b, The Mathworks, Natick, Massachusetts, USA) to extract each parameter of interest. Signals were filtered digitally with a 10-Hz low-pass Butterworth filter (4th order) with zero phase lag.
Protocol
Subjects were asked to perform STS movements in five conditions: (1) as rapidly as possible with a 90° knee angle when seated (STS1); (2) at comfort speed with a 90° knee angle when seated (STS2); (3) at comfort speed from a standard chair (H = 48 cm) using armrests (STS3); (4) at comfort speed, from a 40 cm-heighted chair without armrests (STS4) and (5) at comfort speed from a 59 cm-heighted chair without armrests (STS5). Except during STS3, arms were crossed over the chest to standardize the lift chair position. Before the movement began, the chair height was adjusted for every subject to reach a standardized seated position with a 90° knee angle. The knee angle was evaluated and controlled by a medical goniometer (accuracy 1°) composed of two arms (stationary and moveable arms). The center of the goniometer was aligned with the knee joint center. A hash marks on the center of the goniometer allowed measuring precisely the joint range of motion. Range of motion was controlled by placing the stationary arm on the thigh (aligned with a virtual line traced between the knee and the great trochanter), whereas the moveable arm was placed on the shank (aligned with a virtual line traced between the knee and the ankle) to reach a knee angle of 90°. Measurements were all realized in the same way and by the same operator. Three trials, spaced by 5 s rest, were performed for all conditions. Whatever the condition, a 1-s break was asked to the subjects when they reached the standing position, to clearly identify the end of the movement. The different testing conditions were spaced by 2 min of rest and were randomized to prevent any fatigue process or experimental influences.
Data analysis
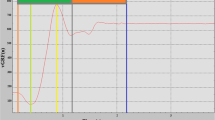
According to Etnyre and Thomas [15], the STS movement (Fig. 1) begins with a relief phase and ends when GRF normalized relatively to the body weight is equal to 1, which means that the subject is standing. For each condition, as classically done, the following parameters were determined from the force–time evolution: peak GRF (F peak, in N kg−1), average GRF produced during the complete STS (F mean, in N kg−1), time to reach F peak (T 1, in s), STS total time (T TOT, in s); STS Impulse (Imp, in N kg−1 s) which correspond to the area under the force–time curve during the total STS movement. Each parameter was analyzed according to the vertical (Z), medio-lateral (X), antero-posterior (Y) axes.

Typical example of a sit-to-stand (STS) vertical force–time curve recorded from a force platform (modified from Etnyre and Thomas 2007, and Yamada 2010)
Statistical analysis
Data are presented as means ± standards deviations. Skewness and Kurtosis analysis were used to verify the normality of distribution and homogeneity of variance in the data sets. A one-way factorial ANOVA was applied to determine the effect of the STS conditions on the force platform parameters (Table 1). A one-way ANOVA with repeated measures was used to analyze trials repeatability, and to determine the number of trials necessary to obtain reliable results. Scheffe post hoc comparisons were carried out to identify any significantly different trials and conditions. Intraclass correlation coefficient (ICC) was used to represent agreements between trials. ICC was calculated across all trials to examine the reliability of force platform parameters. ICC was interpreted as follows: ICC less than 0.5 indicates poor to fair agreement; 0.5–0.6 moderate agreement; 0.7–0.8 strong agreement; and >0.8 almost perfect agreement [23]. Because of ICC dependence on inter-subjects homogeneity, standard error of the mean (SEM), which corresponds to an absolute reliability index unaffected by inter-subject variability was taken into account [24]. SEM was expressed as a percentage of the average value for comparison between tasks. Coefficient of variation (CV %) was also computed to give information on the data stability between individuals rather than between trials [25]. The acceptability threshold is usually set at 10 % [26]. For all statistical procedures, significance threshold was set at p < 0.05.
Results
Whatever force platform parameters, no significant differences were observed between right and left sides, meaning that there was no asymmetry during STS. Consequently, parameters related to the force platform corresponded to the combined recordings from the two force plates (i.e., as if only one force plate was used).
STS parameters
Values of measured parameters during all STS conditions are presented in Table 1. Most of the mechanical and temporal parameters appeared to be significantly different for each condition (p < 0.05). More precisely, speed of movement (STS1 vs. STS2), chair-height variation (STS2 vs. STS4 vs. STS5), and using or not armrest (STS2 vs. STS3) induced significant differences in the collected parameters. For example, vertical force (F ZPeak) was greater for the highest speed of movement (1.85 N kg−1 during STS1 vs. 1.27 N kg−1 during STS2) and for the lowest height of the chair (1.37 N kg−1 during STS4 vs. 1.22 N kg−1 during STS5). On the other hand, the use of armrest decreases F ZPeak (1.27 N kg−1 during STS2 vs. 1.02 N kg−1 during STS3). Moreover, temporal data showed a decrease in execution time (T TOT) with the increase of the height of chair (1.71 s during STS4 vs. 1.54 s during STS5) and speed of movement (1.06 s during STS1 vs. 1.73 s during STS2).
Repeatability
ICC values for all parameters and all STS conditions are presented in Table 2.
Strong to perfect repeatability was observed for the impulse in all axes under each condition (0.79 < ICC < 0.97). Regarding the vertical axis, ICC showed a strong to perfect repeatability for all parameters (0.72 < ICC < 0.9) during STS1 (fast movement condition). Regarding medio-lateral axis, all parameters presented strong repeatability (0.82 < ICC < 0.98) whatever the STS condition is. In the antero-posterior axis, strong repeatability (0.71 < ICC < 0.81) was found for all force platform parameters during STS2 and STS4 (0.78 < ICC < 0.88). Only F YPeak parameter, for STS1 and STS3, has a moderate (ICC = 0.60) and a poor repeatability (ICC = 0.36), respectively.
Considering the influence of the height of the chair, our results showed the same repeatability levels during STS2, STS4 and STS5 for all parameters except F ZPeak.
Regarding the use of armrest, the repeatability is strong for all parameters during STS2 and STS3 in the medio-lateral axis. In the antero-posterior axis, F YPeak presented a poor agreement when armrests were used (STS3, ICC = 0.36). In the vertical axis, the repeatability was similar for F ZMEAN and Imp Z whereas the use of armrests was associated with a poor agreement for F ZPeak (STS3, ICC = 0.35).
The comparison between STS1 vs. STS2 showed that the STS performed as fast as possible (STS1) is more repeatable that when performed at the comfort speed (STS2). Indeed, vertical and temporal data are all repeatable for the fast condition (STS1, 0.72 < ICC < 0.90) contrary to the comfort condition when one datum is repeatable.
Temporal parameters (T TOT and T 1) were highly repeatable (0.76 < ICC < 0.84) under STS1 and STS3 conditions but less repeatable during STS2, STS4 and STS5 (0.45 < ICC < 0.65).
Coefficient of variation (CV %) and standard error of the mean (SEM %) are presented in Table 3. Considering SEM % values, all parameters measured in three axes and during all STS conditions, exhibited low dispersion calculation (SEM <16 %) except the impulse in medio-lateral and antero-posterior axes. All CV % values were upper 10 % except F ZPeak parameters.
Number of trials to get repeatable measurements
Results of the ANOVA regarding the number of trials needed to show no significant differences are presented in Fig. 2.

Number of trials needed to show no significant difference between trials
For all the other parameters, the STS condition allowing more homogenous data is STS5. Furthermore, during STS5, all parameters required only one trial to achieve relevant measurements except T 1 that required three trials. When antero-posterior axis only is considered, results highlight the fact that using a single trial is relevant for all parameters and all STS conditions except for the impulse during STS1.
Discussion
STS parameters
The first purpose of the present study was to determine the most relevant and reliable parameters to assess the STS movement using a force platform while taking the STS condition into account. Results showed that instructions and STS procedures greatly influence the mechanical parameters obtained from a force platform. Indeed, F ZPeak, was significantly greater under STS1 than under STS2. Similar results were obtained when the armrests were used as suggested by Etnyre and Thomas [15]. Analyzing F ZPeak, these authors showed significant differences between arms crossed over the chest and hands-on-armrests conditions. Our results also highlighted a decrease in the GRF, reinforcing the need to standardize a seated position to be able to compare results from different studies.
When considering the impact of the height of chair on STS parameters, STS2 can be excluded because the height of chair is people-dependant. One can observe that at comfort speed, the temporal parameters (T 1 and T TOT) and, mean and peak forces in the three axes, except F ZMEAN and F YPeak, values are influenced by the height of chair. A 19 cm difference on the height of chair causes an increase of 12 % of the time to rise of the chair. This result confirms that lowering the height of the seat makes the STS movement difficult or even unsuccessful [19, 22, 27] because angulations of the knee becomes smaller than 90°. Overall, the lower the chair seat was, the smaller the knee angle and the longer the distance to stand up were, resulting in a longer execution time. Moreover, this movement forms a low position required a greater F ZPeak and F XPeak. Thus, “the height of a chair seat affects the burden on the lower limbs during STS” [7] and in view of factorial ANOVA results, reference position to evaluate lower limbs force must not be established from a fixed height of the chair seat but rather from an identical reference position for all subjects (i.e., to begin the STS movement from a knee angle fixed at 90° when seated). This result is in agreement with the hypothesis formulated by Pérennou et al. [28] on the fact that a normalization of the reference position relatively to the size of the subjects would be desirable. Moreover, variation in the height of the chair seat can result in an altered strategy to rise on chair [16, 22]. Indeed, when the initial seated position is modified, one can observe a decrease in the hip angular velocity, and an increase in trunk knee and ankle angular displacement [27, 29, 30]. Indeed, when the initial seated position is lowest, this leads to an increase of the angular displacement. Consequently, a seated position with a 90° knee joint angle can be recommended for all population.
Considering the impact of the STS speed, our results are in agreement with those of Kerr et al. [31] for comfort speeds. Our results showed a variation of 60 % duration of movement between comfort and fast speed demonstrating compliance with the instructions. Consequently, determination of the speed of the STS movement is important to consider. Moreover, influence of the STS movement velocity modified the hip flexion, knee extension and ankle dorsiflexion joint moment [32]. A faster STS gave a shorter flexion and momentum-transfer phase [33, 34]. Time to perform the STS movement is a parameter fluently used in clinical evaluation to assess patient ability and the efficiency of prevention or rehabilitation programs. More, both conditions could be useful, one for training (comfort) and the other for evaluation (fast). Indeed, comfort speed seems to give more subjective data than maximum speed which can be explained considering that subjects can adjust their speed in comfort condition of a STS to another, while they can not do so under condition of maximum speed. Even if people with disorders (e.g., elderly subject) were less able to increase the speed of their STS movement [35, 36], the maximum speed instruction seems clearer than comfort speed condition.
Overall, the aforementioned results are in accordance with the literature [7, 15, 28, 31]. Our study also revealed a speed effect (STS1 vs STS2) for all parameters except to F YMEAN, an influence of the use of armrests (STS2 vs STS3) for all parameters, and an effect of the height of the chair (STS4 vs STS5) except for F ZMEAN and F YPeak parameters for vertical and antero-posterior axes.
Repeatability
The second purpose of the present study was to evaluate the repeatability of different standardized procedures to identify the number of trials that are necessary to get relevant and reliable data. It is recommended not to use the ICC as the unique indicator of reliability [26]. Indeed, if subject’s parameters differ little from each other, ICC will be low even if the inter-assay variability is low. High ICC, with low SEM is considered an adequate way to determine the most pertinent parameters and conditions to realize an efficient assessment.
Regardless conditions of performance, our results showed that the most repeatable parameters are mean and peak forces in the medio-lateral axis, and the impulse in the three axes.
Nevertheless, STS movement is principally defined by an upward body transfer which could explain that only few changes are observed in the medio-lateral axis. For this reason, the vertical component of the parameters extracted from the force platform is usually considered as the most interesting parameters to evaluate the lower limb. Our results showed that mechanical parameters measured in this axis exhibited high ICC values and were most repeatable during the fast speed condition (STS1). This is in accordance with the GRF reliability observed by Yamada and Demura [5].
Few studies were interested in antero-posterior data [1, 15, 37]. The original contribution of the present study is to consider also data obtained on this other axe. Repeatability is good for antero-posterior data except peak force when armrests were used (STS3) and during the fast condition (STS1). This suggests that antero-posterior data could be interesting additional measures, to quantify imbalance during the STS movement mostly in frail people.
Interestingly, under STS3 condition, repeatability is strong for all parameters, except for force parameters in the vertical axis. This result may be explained by the strength of arms applied on the armrests, which varies with the considered trials.
When aiming at getting the most repeatable data, it appears that the fast condition is the most appropriate in view of the vertical parameters and temporal parameters. Fast (STS1) and armrests (STS3) conditions are those that allowed the greatest reliability for T 1 and T TOT. These results are in agreement with several studies which showed that the best reproducibility is reached when the movement speed is imposed, allowing a better comparison between studies [38, 39].
The high CV values for all parameters and during all conditions except F ZPeak, show the heterogeneity of the population of this study, including subjects aged from 21 to 60 years old. Results of the present study are then independent of subjects’ age. Indeed, heterogeneity associated with the good measurements repeatability confirmed that the selected condition is not applicable only to a specific population, but allows for further investigation and extrapolation for any type of population.
Number of trials to get repeatable measurements
Independently of all parameters, it was observed that the number of trials required for the data to be repeatable is higher when the height of the chair decreased (STS4 vs. STS5). The same result was found when considering the speed of the STS movement (STS1 vs. STS2). To limit the intra- and inter-subject variability in STS performance, it is suitable to reduce many constraints (e.g., initial position, speed condition…) [16]. These results are in agreement with those obtained by Hopkins [40] and suggest that three STS trials should be performed to reach high repeatability.
Practical application
Even if the selected population enclosed a large part of the adult period [21–60 year old], and is not an intuitively representative sample of individuals typically evaluated with the sit-to-stand test (STS), its statistical distribution was normal, indicating that the tested population can serve as a baseline data. Our purpose was to get this baseline data that could be of interest during pathological or aging population’s assessment.
Considering subjects who are able to perform all the proposed tests, our results suggest that the fast condition, with a 90° knee joint angle, with arms crossed over the chest (STS1) was the most relevant procedure to reach reliable data to evaluate performance during STS movements. Indeed, the vertical axis is the most important axis to consider for STS movement analysis in view of the fact that this test is defined by a body transfer mainly in this axis [31] and STS1 was the only condition which is repeatable for all parameters in the vertical axis.
However, if subjects present some motor functional limitations due to pathology or aging for instance, STS3 can be performed with particular interest to all platform parameters except F ZPeak, F ZMEAN and F YPeak. Nevertheless, as it was reported in the present study, the vertical data were the most interesting data considering the STS movement used for a lower limb evaluation. The use of armrest would make necessary, in parallels with postural data, the measurement of the strength applied by the arm on the armrests to use force parameters in the vertical axis. For this purpose, using armrest cannot be recommended to minimize the impact of upper limb use on data measurements. This recommendation is in agreement with recent studies in which authors asked subjects to cross his arms over his chest systematically [17, 37].
Some authors [17, 37, 41] also proposed interesting solutions (1) to analyze the STS sequencing and (2) to compare pathological populations, in different conditions from those obtained in our study, especially considering the height of the chair. On one hand, Galli et al. [17] showed differences between healthy and hemiplegic populations while the seat height was adjusted for each subject to be equal to 110 % of the distance between the head of the fibula and the lateral malleolus (i.e. knee angle 67° ± 5°). On the other hand Papa and Cappozzo [41] adjusted the seat height at 80 % of the subjects’ leg size. These results are in agreement with ours, supporting that normalization of the reference position relative to the subject’s height is a crucial methodological point during STS movement [28], even if the normalization process remained to be standardized.
Limitations of the research
Depending on daily activity, it has been shown that mean number of STS released by every subject ranged from 42.8 to 49.3 per day [42]. However, standing up from a chair is almost part of a goal-oriented behavior [16] and aims at introducing a novel motor task. For this reason, it would be interesting to verify whether our results are consistent with a sit-to-walk movement [1].
Our results showed no significant differences between the two lower limbs, because the participant of this study was devoided of any pathology. Measures of symmetry during movement could provide useful informations concerning functional activities among patients with disorders [43] and could potentially be used to alert clinicians to early detect pathology stages which would presumably affect subjects asymmetrically.
Finally, STS movement is often associated with electromyography and kinematic data for a complete analysis of this movement. Complementary studies are needed to complete the present analysis.
Conclusion
To conclude, this study put forward the importance of the standardized position, the characteristics, and the instruction given to the subjects when performing STS test. Our results also allowed determining the more relevant/reliable parameters that should be extracted from such tests for the follow-up of specific population.
Abbreviations
- ANOVA:
-
Analysis of variance
- CV:
-
Coefficient of variation
- GRF:
-
Ground reaction force
- ICC:
-
Intraclass correlation coefficient
- IMP:
-
Impulsion
- SEM:
-
Standard error of the mean
- STS:
-
Sit to stand
- TTOT :
-
Total time
References
Dehail P, Bestaven E, Muller F, Mallet A, Robert B, Bourdel-Marchasson I, Petit J (2007) Kinematic and electromyographic analysis of rising from a chair during a ‘‘Sit-to-Walk’’ task in elderly subjects: Role of strength. Clin Biomech 22:1096–1103
Tully EA, Fotoohabadi MR, Galea MP (2005) Sagittal spine and lower limb movement during sit-to-stand in healthy young subjects. Gait Posture 22(4):338–345
Burnett D, Campbell-Kyureghyan C, Cerrito P, Quesada M (2011) Symmetry of ground reaction forces and muscle activity in asymptomatic subjects during walking, sit-to-stand, and stand-to-sit tasks. J Electromyogr Kinesiol 21(4):610–615
Fotoohabadi R, Tully EA, Galea P (2012) Kinematics of rising from a chair: image-based analysis of the sagittal hip-spine movement pattern in elderly people who are healthy. Phys Ther 90(4):561–571
Yamada T, Demura S (2009) Relationships between ground reaction force parameters during a sit-to-stand movement and physical activity and falling risk of the elderly and a comparison of the movement characteristics between the young and the elderly. Arch Gerontol Geriatr 48:73–77
Yamada T, Demura S (2010) The relationship of force output characteristics during a sit-to-stand movement with lower limb muscle mass and knee joint extension in the elderly. Arch Gerontol Geriatr 50:46–50
Demura S, Yamada T (2007) Height of chair seat and movement characteristics in sit-to-stand by young and elderly adults. Percept Mot Skills 104:21–31
Schofield JS, Parent EC, Lewicke J, Carey JP, El-Rich M, Adeeb S (2013) Characterizing asymmetry across the whole sit to stand movement in healthy participants. J Biomech 46(15):2730–2735
Roy G, Nadeau S, Gravel D, Piotte F, Malouin F, McFadyen B (2007) Side difference in the hip and knee joint moments during sit-to-stand and stand-to-sit tasks in individuals with hemiparesis. Clin Biomech 22(7):795–804
Agrawal V, Gailey R, Gaunaurd I, Gailey R, O’Toole C (2011) Weight distribution symmetry during the sit-to-stand movement of unilateral transtibial amputees. Ergonomics 54(7):656–664
Gao F, Zhang F, Huang H (2011) Investigation of sit-to-stand and stand-to-sit in an above knee amputee. In: Proceedings of the 33rd annual international conference IEEE EMBS, Boston, 20 August 2011
Whitney SL, Wrisley DM, Marchetti GF, Gee MA, Redfern MS, Furman JM (2005) Clinical measurement of sit-to-stand performance in people with balance disorders: validity of data for the Five-Times-Sit-to-Stand Test. Phys Ther 85(10):1034–1045
Butler-Browne G, Bigard A-X (2006) Caractéristiques du vieillissement musculaire et effets préventifs de l’exercice régulier. Sci Sports 21(4):184–193
Cooper R, Kuh D, Hardy R (2010) Objectively measured physical capability levels and mortality: systematic review and meta-analysis. BMJ Clin Res Ed 341:c4467
Etnyre B, Thomas DQ (2007) Event standardization of sit-to-stand movements. Phys Ther 87:1651–1666
Janssen WG, Bussmann HB, Stam HJ (2002) Determinants of the sit-to-stand movement: a review. Phys Ther 82:866–879
Galli M, Cimolin V, Crivellini M, Campanini I (2008) Quantitative analysis of sit to stand movement: experimental set-up definition and application to healthy and hemiplegic adults. Gait Posture 28:80–85
Borzelli G, Cappozzo A, Papa E (1999) Inter- and intra-individual variability of ground reaction forces during sit-to-stand with principal component analysis. Med Eng Phys 21(4):235–240
Schenkman ML, Berger RA, Riley PO, Mann PW, Hodge WA (1990) Whole body movements during rising from sitting to standing. Phys Ther 70:638–651
Roberts PD, McCollum G (1996) Dynamics of the sit-to-stand movement. Biol Cyber 74:147–157
Nadeau S, Desjardins P, Briere A, Roy G, Gravel D (2008) A chair with a platform setup to measure the forces under each thigh when sitting, rising from a chair and sitting down. Med Biol Eng Comput 46(3):299–306. doi:10.1007/s11517-007-0301-z
Hughes MA, Schenkman ML (1996) Chair rise strategy in the functionally impaired elderly. J Rehabil Res Dev 33:409–412
Portney LG, Watkins MP (2000) Foundations of clinical research applications to practice. Prentice Hall Inc. New Jersey ISBN 0-8385-2695-0: 560–567
Weir JP (2005) Quantifying test–retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond Res 19:231–240
Knutson LM, Soderberg GL, Ballantyne BT, Clarke WR (1994) A study of various normalization procedures for within day electromyographic data. J Electromyogr Kinesiol 4:47–59
Atkinson G, Nevill AM (1998) Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med 26:217–238
Munro BJ, Steele JR, Bashford GM (1998) A kinematic and kinetic analysis of the sit-to-stand transfer using an ejector chair: implications for elderly rheumatoid arthritic patients. J Biomech 31:263–271
Pérennou D, Decavel P, Manckoundia P, Penven Y, Mourey F, Launay F, Pfitzenmeyer P, Casillas JM (2005) Evaluation of balance in neurologic and geriatric disorders. Ann Readapt Med Phys 48:317–335
Rodosky MW, Andriacchi TP, Andersson GB (1989) The influence of chair height on lower limb mechanics during rising. J Orthop Res 7:266–271
Su FC, Lai KA, Hong WH (1998) Rising from chair after total knee arthroplasty. Clin Biomech 13:176–181
Kerr KM (1997) Analysis of the sit-stand-sit movement cycle in normal subjects. Clin Biomech 12:236–245
Pai YC, Rogers MW (1991) Speed variation and resultant joint torques during sit-to-stand. Arch Phys Med Rehabil 72:881–885
Vander Linden DW, Brunt D, McCulloch MU (1994) Variant and invariant characteristics of the sit-to-stand task in healthy elderly adults. Arch Phys Med Rehabil 75:653–660
Hanke TA, Pai YC, Rogers MW (1995) Reliability of measurements of body center-of-mass momentum during sit-to-stand in healthy adults. Phys Ther 75(2):105–113; discussion 113–108
Gross MM, Stevenson PJ, Charette SL (1998) Effect of muscle strength and movement speed on the biomechanics of rising from a chair in healthy elderly and young women. Gait Posture 8:175–185
Mourey F, Grishin A, d’Athis P (2000) Standing up from a chair as a dynamic equilibrium task: a comparison between young and elderly subjects. J Gerontol A Biol Sci Med Sci 55:B425–B431
Mazza C, Mounir Zok M, Ugo Della (2005) Croce Sequencing sit-to-stand and upright posture for mobility limitation assessment: determination of the timing of the task phases from force platform data. Gait Posture 21:425–431
Schenkman ML, Riley PO, Pieper C (1996) Sit to stand from progressively lower seat heights: alterations in angular velocity. Clin Biomech 11:153–158
Roebroeck ME, Doorenbosch CA, Harlaar J (1994) Biomechanics and muscular activity during sit-to-stand transfer. Clin Biomech 9:235–244
Hopkins Will G (2000) Measures of reliability in sports medicine and science. Sports Med 30:1–15
Papa E, Cappozzo A (2000) Sit-to-stand motor strategies investigated in able-bodied young and elderly subjects. J Biomech 33(9):1113–1122
Bohannon RW, Barreca SR, Shove ME, Lambert C, Masters LM, Sigouin CS (2008) Documentation of daily sit-to-stands performed by community-dwelling adults. Physiother Theory Pract 24(6):437–442
Burnett D, Campbell-Kyureghyan N, Topp R, Quesada P (2009) Asymmetry in vertical ground reaction force and hip range of motion in asymptomatic subjects and total knee arthroplasty patients either with or without back pain. Gait Posture 30:S142–S143
Acknowledgments
The authors are grateful to the participants for their involvement in this study. This study was supported by grants from the Region des Pays de la Loire (France), for the project “RP3AP”. The authors would like to thank Sébastien Boyas for his useful comments that helped improve the quality of this manuscript.
Conflict of interest
The authors declare that they have no conflict of interest.
Statement of Human Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This article does not contain any studies with animals performed by any of the author.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Chorin, F., Rahmani, A., Beaune, B. et al. Determination of reliable force platform parameters and number of trial to evaluate sit-to-stand movement. Aging Clin Exp Res 27, 473–482 (2015). https://doi.org/10.1007/s40520-014-0294-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40520-014-0294-z