
Abstract
Cancer is a major disease worldwide and different approaches are needed to reduce its risk. Previous laboratory studies suggested that cancer can be prevented by many naturally occurring and synthetic chemicals. In human cancer prevention studies, however, most of the successful examples are the repurposing of existing drugs, such as tamoxifen and aspirin. Epidemiological studies have established associations between certain dietary patterns or nutrient insufficiencies with elevated cancer risk. Laboratory research has also shown impressive results on the cancer preventive activities of constituents from food and beverages. However, such cancer preventive activities have not been demonstrated in many human intervention trials. This article reviews the advances in this field and discusses the reasons for the discrepancies between laboratory studies and human trials. Lessons learned for cancer prevention research in the past decades will be illustrated using studies with β-carotene, vitamin E, green tea polyphenols, tamoxifen, and aspirin as examples. In future studies, more interdisciplinary collaboration in the integration of laboratory and human studies are needed to advance the field of cancer chemoprevention.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The association between certain dietary patterns and cancer risks first gained recognition in the 1960s, and Dr. Lee Wattenberg proposed the concept of chemoprophylaxis of carcinogenesis by dietary chemicals and the possible mechanisms involved [124, 125]. Dr. Michael Sporn later coined the term “chemoprevention” to advocate cancer prevention by using chemicals, including those of dietary origin [109]. Since then, this term has been widely used. Subsequently, numerous laboratory studies on the cancer prevention activities of synthetic and naturally occurring compounds have been conducted [8, 33, 100, 125, 129]. In spite of the interesting results from many laboratory studies, very few agents have been shown to be effective cancer preventive agents in human trials. In this article, studies on nutrients such as vitamin E, β-carotene, and selenium; non-nutritive dietary compounds such as tea polyphenols; and chemopreventive drugs such as tamoxifen and aspirin, are used to illustrate some of the progresses and challenges in this area of research. Reasons for the discrepancies among results from epidemiological observations, laboratory studies, and human trials, as well as possible ways to improve future cancer chemoprevention research, are discussed.
Early Cancer Prevention Studies on Antioxidant Nutrients
Early epidemiology studies established an association between certain micronutrient insufficiencies and risks for many types of epithelial cancer. Esophageal cancer, for example, was prevalent in populations with a monotonous diet, such as those in certain areas of northern China, central Asia, and northern Iran. In these populations, people survived on a diet with staples such as corn, wheat, or millet with a low intake of vegetables, fruits, and animal products, leading to insufficiency in micronutrients, such as vitamins A, B2, and C, selenium, zinc, magnesium, and calcium [127]. Similarly, laboratory studies have demonstrated that diets with insufficiency in micronutrients enhance N-nitrosomethylbenzylamine-induced esophageal carcinogenesis in rats, which may be attenuated by supplementation with zinc, molybdenum, vitamin A, and riboflavin (reviewed in [129]).
Linxian Nutrition Intervention Trial
The hypothesis that supplementation with micronutrients can prevent esophageal cancer was tested in a large-scale US-China Cooperative Linxian Nutritional Intervention Trial (LNIT) started in the early 1980s. The rural population in Linxian (now named Linzhou City) had low intake of micronutrients, and insufficiencies in some nutrients that were indicated in blood nutrient analyses [128, 131]. Because many micronutrients had been suggested to be associated with esophageal cancer, a design with nutrient combination was adopted, in which nutrients were divided into four groups: (A) retinol, zinc; (B) riboflavin, niacin; (C) ascorbate, molybdenum; and (D) α-tocopherol, β-carotene, selenium. The nutrient groups were combined in a factorial design with eight groups: placebo, AB, AC, BC, AD, BD, CD, and ABCD. Each nutrient was given at 1–3 times the levels of the US Recommended Daily Allowance (RDA). The study involved 29,584 adults (aged 40 to 69), who were randomized into eight groups and given supplementations as daily pills for 63 months (1985 to 1991). There were 2127 deaths during the trial period; 32% were due to esophageal and gastric cancer. The so-called esophageal cancer in Linxian actually consisted of 60% esophageal squamous cell carcinoma (ESCC) and 40% gastric cardia adenoma (GCA). The latter was therefore classified as gastric cancer in this trial. The study showed that supplementation with a combination of α-tocopheryl acetate (50 mg), β-carotene (15 mg), and selenium (50 μg) to the general population (aged 40 to 69) for 63 months decreased mortality due to gastric cancer (mainly GCA) by 20% and total cancer mortality by 13% [7], suggesting the involvement of these nutrients in this cancer. Nested case-control studies also showed that the blood levels of α-tocopherol and selenium were inversely associated with gastroesophageal cancer risk [78, 115]. Other nutrient combinations, however, did not show any effect on the endpoints measured [7]. Results from a 10-year follow-up found that the protective effect of α-tocopherol/β-carotene/selenium on GCA was sustained. In addition, this nutrient combination also protected against ESCC in subjects enrolled in the trial at age 55 years or younger (but not in those older than 55 years) [92].
It is possible that the intervention was ineffective in older subjects because they already had more advanced precancerous lesions than the younger subjects. This is consistent with the result of a parallel trial in Linxian on subjects with esophageal dysplasia, which showed a lack of beneficial effect by supplementation with multiple micronutrients [66]. These results are supported by studies in a rat model demonstrating that insufficiencies in vitamin E and selenium enhanced N-methylbenzylnitrosamine-induced esophageal carcinogenesis, and that the preventive effect was more pronounced when these nutrients were administered at the early stage of carcinogenesis [134]. The concept that chemoprevention is more effective in patients with less severe precancerous lesions was also demonstrated in a randomized placebo-controlled trial (RCT) in Linxian in the 2000s, which showed that supplementation with selenomethionine for 10 months improved squamous histology in 115 patients with mild esophageal dysplasia, but not in the 125 patients with severe dysplasia [70]. Celecoxib was also used in this trial, but had no effect on the squamous histology.
Trials with β-Carotene
In the 1980s, β-carotene was lauded as a very promising chemopreventive antioxidant [89]. This viewpoint was mainly based on epidemiological studies showing that decreased cancer risk was associated with vegetable and fruit consumption. The hypothesis that β-carotene can prevent lung cancer was tested in male Finnish smokers in the α-Tocopherol and β-Carotene (ATBC) study started in 1985 [34]. This was a randomized, double-blind, placebo-controlled primary-prevention trial with a total of 29,133 male smokers, 50 to 69 years of age, from southwestern Finland using α-tocopheryl acetate (50 mg per day) and β-carotene (20 mg per day) in a 2 × 2 factorial design for an average of 4.5 years, with follow-up continued for 5 to 8 years. Unexpectedly, among the 876 new cases of lung cancer diagnosed during the trial, increased lung cancer incidence (by 18%) was observed in the β-carotene group. No effect in incidence was observed among the men who received α-tocopherol. However, supplementation with α-tocopherol was found to reduce the incidence of prostate cancer (by 45%) and other cancers in a secondary endpoint analysis [38].
In another large study involving β-carotene, the β-Carotene and Retinol Efficacy Trial (CARET), a primary-prevention trial involving a total of 18,314 smokers, former smokers, and workers exposed to asbestos in the USA, the relative risk of lung cancer was increased (~ 28%) in the group treated daily with a combination of 30 mg of β-carotene and 25,000 IU of vitamin A [84]. The CARET also indicated that the combination of β-carotene and vitamin A may increase the risk of deaths from lung cancer, cardiovascular disease, and other causes in smokers and workers exposed to asbestos.
These studies essentially ended further research on β-carotene as a preventive agent. The reasons for the β-carotene-enhanced lung cancer rate are not fully understood. It is possible that in an environment of excessive oxidative stress in the lung of individuals exposed to cigarette or asbestos, the redox active compound β-carotene may further enhance oxidative stress and promote lung tumorigenesis.
Trials with Selenium
Selenium is another “antioxidant” that has been studied extensively as a chemopreventive agent [18, 45, 57, 93]. A multicenter, double-blind, randomized, placebo-controlled cancer prevention trial, known as the Nutritional Prevention of Cancer Study (NPC), was conducted in the Eastern United States from 1983 through 1991 [16]. A total of 1312 patients with a history of basal cell or squamous cell carcinomas of the skin were randomized to take 200 μg of selenium per day as selenium-enriched yeast or non-enriched yeast as placebo orally for a mean of 4.5 years, and had a total follow-up of 6.4 years. After a total follow-up of 8271 person-years, selenium treatment did not significantly affect the incidence of basal cell or squamous cell skin cancer. However, secondary endpoint analysis yielded very interesting results showing that, compared to controls, patients treated with selenium had significant reduction in total cancer mortality, total cancer incidence, and incidences of prostate, lung and colorectal cancers. However, the Vitamins And Lifestyle (VITAL) prospective cohort study, which contained detailed questionnaires about vitamin E and selenium supplement intake from 35,242 men recruited between 2000 and 2002 in western Washington State, showed that a 10-year average intake of selenium at > 50 μg/day was not associated with a reduced prostate cancer risk. Nevertheless, risk of advanced prostate cancer (regionally invasive or distant metastatic) was significantly decreased with greater intake of supplemental vitamin E [88].
Recent Studies on Cancer Prevention by Tocopherols
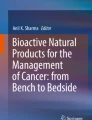
Tocopherols, the major forms of vitamin E, contain a chromanol ring system and a phytyl chain of 16 carbons (Fig. 1). Depending on the number and position of methyl groups on the ring, they exist as α-, β-, γ-, or δ-tocopherol (α-, β-, γ-, and δ-T) [117]. The possible cancer preventive activities by tocopherols have been studied extensively (reviewed in [46, 51, 130]). Of interest is the result of a nested case-control study (CLUE II), showing that the prostate cancer risk was inversely associated with serum levels of γ-T (but not α-T) [43]. A recent report by Weinstein et al. on the Prostate, Lung, Colorectal, and Ovarian Cancer (PLCO) Screening Trial and some previous reports indicated that higher serum levels of α-T were associated with decreased risk of prostate cancer, particularly among smokers ([126] and references cited).

The structures of tocopherols
Disappointing Results from Recent Intervention Studies with α-Tocopherol
Because α-T is the most abundant form of tocopherols in blood and tissues, and has the highest activity in the classical fertility-restoration assay, α-tocopheryl acetate is the vitamin E used in many studies. The results from several large-scale intervention studies with α-T, however, have been disappointing [32, 56, 64, 71]. For example, in the Women’s Health Study, supplementation with α-tocopheryl acetate (600 mg every other day) for 10 years failed to protect against cancer or cardiovascular diseases (CVDs) [64]. Similarly, in the Physicians’ Health Study II RCT, supplementation with α-tocopheryl acetate (400 mg every other day) alone or in combination with vitamin C for 10 years did not prevent prostate or total cancer [32].
The Selenium and Vitamin E Cancer Prevention Trial (SELECT) was designed with great optimism based on the encouraging results from the ATBC and VITAL studies, as well as the NPC Nutritional trial. However, daily supplementation with 400 mg of α-tocopheryl acetate and 200 μg selenium (from L-selenomethionine) in a 2 × 2 design, for an average of 5.5 years, did not prevent prostate or other cancers [71]. In the 7–12 year follow-up of this study, subjects receiving α-T had a hazard ratio of 1.17 for developing prostate cancer [56]. It was noted that, in the SELECT, α-T supplementation caused a 50% decrease in median plasma γ-T levels [71]. The mean baseline median plasma level of α-T in subjects of the SELECT was at an adequate level of 12.5 μg/mL [71]. A possible interpretation for the lack of a cancer preventive effect of α-T is that the supplementation of a nutrient to a population that is already adequate in this nutrient may not produce any beneficial effect. Since γ-T has been suggested to have strong anti-inflammatory and cancer preventive activities [10, 39, 47, 51], the decrease in blood and tissue levels of γ-T, caused by high doses of α-T, may have decreased the prostate cancer prevention potential [56, 71]. Another possibility is that some of these subjects already had preneoplastic lesions when entering the trial, and the supplementation with high doses of α-T promoted prostate cancer development. The exact reasons for these negative results from the SELECT and other trials are still not known. Nevertheless, the disappointing outcome of these large-scale trials reflects our inadequate understanding of the biological activities of tocopherols and points to the need for systematic studies of the disease preventive activities of the different forms of tocopherols.
New Insights from Recent Laboratory Studies of Specific Forms of Tocopherols
Previous cancer prevention studies in different animal models, mainly with α-T, have obtained inconsistent results [51]. However, the cancer preventive activity of γ-T has recently received much attention [10, 39, 47, 51, 86, 130]. Recent studies from our research team at Rutgers University have demonstrated the inhibition of cancer formation and growth in the lung, colon, mammary gland, and prostate by γ-T, δ-T, and a tocopherol mixture that is rich in γ-T (named γ-TmT) [14, 15, 23, 49, 62, 63, 74, 130]. γ-TmT, a product derived from vegetable oil usually containing (per g) 130 mg α-T, 15 mg β-T, 568 mg γ-T, and 243 mg δ-T, was shown to significantly inhibit the formation of colon adenoma in a mouse carcinogenesis model induced by azoxymethane and dextran sodium sulfate. We also demonstrated that δ-T was more active than (or had similar activity as) γ-T in inhibiting cancer cell growth in culture, human lung cancer H1299 cell tumorigenesis in a xenograft model, colon carcinogenesis induced by azoxymethane in rats, colon carcinogenesis by 2-amino-1-methyl-6-phenylimidazo(4,5-b)pyridine (PhIP) in CYP1A-humanized mice, and prostate carcinogenesis induced by PhIP, whereas α-T was not effective in these models [15, 35, 65]. Takahashi et al. also demonstrated that γ-T (0.005 or 0.01% in the diet), but not α-T, decreased the number of adenocarcinomas in the ventral lobe in the “Transgenic rat for adenocarcinoma of prostate” model [113]. In these studies, the possible mechanisms of inhibitory actions of δ-T and γ-T are the quenching of reactive oxygen and nitrogen species, the lowering of prostaglandin E2 and leukotriene B4 levels, inhibition of PI3K/AKT pathway, activation of PPARγ, and the enhancement of cancer cell apoptosis [14, 15, 23, 35, 65, 108, 123].
Based on the above epidemiological and laboratory studies, we propose that under conditions of vitamin E insufficiency, all forms of vitamin E contribute to cancer prevention. In vitamin E sufficient individuals, however, supra-nutritional levels of γ-T, δ-T, and γ-TmT prevent cancer, whereas α-T is not effective. The preventive activities of δ-T, γ-T, and γ-TmT warrant further investigation in preclinical and clinical studies.
Studies on Cancer Prevention by Non-nutritive Dietary Constituents
Numerous dietary phytochemicals have been studied for their cancer preventive activities. These include a variety of polyphenols, such as tea catechins, resveratrol, curcumin, genistein, chlorogenic acid, epigenin, delphinidin, luteolin, and silibinin; terpenoids such as carnosol and limonene; and organosulfur compounds such as sulforaphane, phenethylisothiocyanate, indole-3-carbinol, and diallyl sulfide. A great deal of interesting results from laboratory studies have accumulated [8, 33, 100]. However, convincing evidence on cancer preventive activities from human studies are lacking. We will use studies on green tea as examples to illustrate the challenges in extrapolating results from in vitro studies to animals, and from studies in animal models to human situations.
Studies on Tea in Animal Models
Green tea, made from the leaves of the plant Camellia sinensis, is a popular beverage worldwide. The abundance of data from investigations on green tea provides a unique opportunity for us to compare results obtained from laboratory and human studies. The characteristic tea polyphenols can be used as exposure biomarkers in epidemiological studies. The structures of the major green tea polyphenols known as catechins: (−)-epigallocatechin-3-gallate (EGCG), (−)-epigallocatechin (EGC), (−)-epicatechin-3-gallate (ECG), and (−)-epicatechin (EC) are shown in Fig. 2. Among the tea polyphenols, EGCG is the most abundant, most active, and most studied. The cancer preventive activities of green tea extracts, tea polyphenols, and EGCG have been demonstrated in many animal models (reviewed in [132, 133]). These include chemically induced and genetic models for lung, oral, esophageal, stomach, small intestinal, colorectal, and prostate cancers. The inhibitory activity against carcinogenesis in the lung and other organs has been observed when tea preparations are administered to mice during the initiation, promotion, or progression stages. These results demonstrate the broad cancer preventive activities of tea catechins in animal models.

The structures of tea catechins
Studies on Tea In Vitro and Mechanistic Considerations
The biological activities of tea catechins, especially EGCG, have been studied extensively in vitro and in vivo (reviewed in [132, 133]). EGCG is known for its antioxidant action, but it can also produce reactive oxygen species (ROS), especially in vitro. The phenolic groups of EGCG are donors for hydrogen bonding, and EGCG binds strongly to many different proteins via multiple hydrogen bonds. Some of these proteins have been proposed as targets of EGCG for inhibitory actions against cancer cells [132, 133]. For example, EGCG has been proposed to bind to different molecular targets, inhibit the activities of many key enzymes, and inhibit several receptor-dependent signaling pathways [133]. Binding of EGCG to the 67-kDa laminin receptor with a dissociation constant (K d) value of 0.04 μM was observed using a surface plasmon resonance assay, and this was proposed to be a mechanism for the anti-cancer actions of EGCG [59, 112]. Dong et al. identified vimentin, IGF-1R, GYN, GRP78, 2AP70, G3BP1, and Pin1 as high affinity EGCG binding or EGCG target proteins [28, 29, 37, 67, 104, 105, 121, 133]. In several studies, the binding of EGCG to proteins showed rather low (sub μM) K d or K i values; however, the concentrations required for inhibiting cell growth or inducing apoptosis are in the range of 10–30 μM EGCG [133]. This is most likely due to the non-specific binding of EGCG to other proteins and cellular materials.
Many of these proposed mechanisms are quite interesting; however, it is uncertain whether many of these proposed mechanisms are relevant to cancer prevention in animals. EGCG can be autoxidized under the conditions of many cell culture studies. For example, at 50 μM, most EGCG is generally autoxidized within 2 h (mediated by superoxide in a chain reaction) to dimers, which are unstable and converted to unidentified products [41]. The dimers of EGCG may have even higher affinities for protein binding. It is unclear whether many of the in vitro binding studies are affected by the formation of dimers or other derivatives and whether some of the reported cell-killing effects of EGCG are mediated by its autoxidation products, superoxide and hydrogen peroxide, generated outside of the cells.
Mechanisms derived from cancer prevention studies in animal models are likely to be more relevant than those from studies in vitro. These include the induction of apoptosis in different animal models, inhibition of phosphorylation of c-JUN and ERK1/2 in lung tumorigenesis models, suppression of nuclear β-catenin and phospho-AKT levels in colon cancer models, inhibition of the IGF/IGF-1R axis in colon and prostate cancer models, and suppression of VEGF-dependent angiogenesis in lung and prostate cancer models [1, 12, 50, 73, 106, 133]. It is still unclear whether these molecules are direct targets for EGCG or from downstream events of the primary action. In theory, the high affinity binding proteins mentioned above could serve as initial targets, but this point remains to be substantiated in vivo. From the limited human studies available, the action of tea constituents in reducing oxidative stress and enhancing the elimination of carcinogens could also be important mechanisms for the cancer preventive activity of tea [36, 99, 114].
Possible Cancer Prevention by Tea in Humans
In spite of the strong evidence for the cancer preventive activity of tea constituents in animal models, results on such activities in humans from epidemiological studies have not been consistent (reviewed in [132, 133, 137]). A large cohort study in Japan suggested that tea consumption decreased deaths due to CVDs, but not cancer [60]. In the Chinese Prospective Smoking Study of 165,000 adult men in China, tea consumption was associated with a significant reduction of deaths from cancer, as well as CVDs, in men who never smoked. In smokers, protective effects against risk of cancer death was only observed in those who consumed high quantities of tea (> 10 g/day) [72]. However, another large cohort study in Shanghai did not show an association between tea consumption and deaths from cancer, even though a decreased risk for CVDs was observed [138].
A comprehensive review by Yuan et al. [137] concluded that the consumption of green tea was frequently associated with a reduced risk of upper-gastrointestinal tract cancer, after adjusting for confounding factors, and limited data supported its protective effect of lung and hepatocellular carcinogenesis. However, intake of black tea was not associated with a lower risk of cancer [137]. Some recent studies are consistent with this conclusion. For example, a meta-analysis of perspective cohort studies in Asian populations (nine studies involving 465,274 participants and 3694 cases of liver cancer) found that protective effects of green tea for liver cancer was only observed in women (RR, 0.78), but not in men [44]. A population-based cohort study in Japan also suggested that green tea consumption lowered the risk of biliary tract cancer [75]. In a recent systematic review and meta-analysis for endometrial cancer, a protective effect was found with green tea, but not black tea consumption [139].
Smoking and probably alcohol drinking are strong interfering factors. In a case-control study on esophageal cancer in Shanghai by Gao et al. [31], a protective effect of tea consumption was only observed in non-smokers and non-drinkers, who were mostly women. Similarly, a systematic review of cohort studies in Japan showed an inverse association between green tea consumption and gastric cancer only in non-smoking, non-drinking women [97]. The relationship between tea consumption and cancer risk may become clearer if the interfering factors are corrected for. Nevertheless, the above results suggested the cancer preventive effect of tea in humans is only mild.
The results of human intervention studies with green tea polyphenols, mostly small randomized clinical trials (RCT), have been inconsistent. It is disappointing that some of the exciting results from earlier studies have not been fully reproduced in recent studies. For example, an earlier RCT on oral cancer prevention in China, with a mixed tea product (3 g/day administered orally or topically) in patients with oral mucosa leukoplakia for 6 months, showed significant decrease in the number and total volume of proliferation index and silver-stained nucleoli organizer regions [68]. However, a later phase II RCT in the USA with green tea extract (500, 750, or 1000 mg/m2 2 times daily) for 12 weeks, to patients with oral pre-malignant lesions, showed possible beneficial effects in the suppression of oral pre-malignant lesions, but it was not statistically significant [118]. In an impressive prostate cancer prevention study in Italy, 30 men with high-grade prostate intraepithelial neoplasia (PIN) were given 600 mg of green tea catechins daily for 12 months [5]. Only one patient developed prostate cancer, whereas 9 of the 30 patients with high-grade PIN in the placebo group developed prostate cancer. The difference was highly significant. However, a recent trial in Florida with a similar design using Polyphenon E (proprietary mixture of green tea catechins containing 400 mg of EGCG) in 97 men with high-grade PIN and/or atypical small acinar proliferation showed no differences in the number of observed prostate cancer cases between the treatment group (n = 49) and the placebo group (n = 48) [58]. Yet, some beneficial effects and a decrease in serum prostate-specific antigen were observed in the supplemented group. Some recent intervention studies on breast cancer and esophageal adenocarcinoma were only able to obtain results on bioavailability and some biomarkers [48, 96]. At present, the earlier optimistic expectation of cancer preventive activity by tea polyphenols has not materialized in RCTs.
Successful Examples of Chemopreventive Agents for High-Risk Populations
The scientific basis for chemoprevention is that the development of most epithelial cancers involves a series of genetic and epigenetic alterations over a rather long period of time, from 10 to 40 years [120]. If effective and safe drugs can be used to arrest or reverse these carcinogenic effects, cancer can be prevented.
Selective Estrogen Receptor Modulators (SERMs)
Among the most well-studied drugs are the SERMs, such as tamoxifen and raloxifene, for the prevention of breast cancer in high-risk populations [21, 22, 24, 76]. These compounds, which are effective for the prevention of estrogen receptor (ER)-positive breast cancer, have been approved in the USA for breast cancer prevention. The efficacy of tamoxifen in the treatment and prevention of ER-positive breast cancer has long been known. In 1986, the Royal Marsden Tamoxifen Breast Cancer Prevention Trial began, involving treatment with either tamoxifen or placebo for a period of 8 years. In 2006, the study was unblinded. The hazard ratio (HR) of the treatment was 0.77. After a follow-up for 5 and 10 years, the HR decreased to 0.48, suggesting a greater preventive effect post treatment [24]. These findings are promising in that this may lead to reduced side effects if administration time is shortened because of a long post-treatment activity. In addition, this study further confirmed that the incidence of only ER-positive, not ER-negative, breast cancer is reduced [24]. According to a recent review, tamoxifen reduces breast cancer by almost 50% in high-risk populations and by 62% in patients with BRCA mutations [76].
Raloxifene, another SERM, has shown similar effectiveness to tamoxifen, but it has fewer side effects including less uterine cancer, cataract development, pulmonary embolisms, deep-vein thromboses, and vasomotor symptoms [21, 76]. The most common side effects with raloxifene are thromboembolism and vasomotor symptoms [20, 76]. In addition to its SERM effects, raloxifene has anti-inflammatory activities involving upregulation of transcription factors: Nrf-2 and heat shock factor-1 [103]. Decreased intracellular levels of ATP and the activated AMPK/ULK1 pathway by raloxifene have been proposed to enhance autophagy-dependent cell death and contribute to the chemopreventive activity [54]. An added advantage of raloxifene is its reduction of bone fracture incidence and prevention of osteoporosis in postmenopausal women [80]. A recent study showed that raloxifene increased bone-mineral density in the femoral neck and lumbar spine by 1.4% after 1 year of therapy and by 2.1% after 2 years of therapy [135].
To reduce the side effects, clinical trials have been conducted to use lower doses, less frequent dosing, hydroalcoholic gel for topical application, and low-dose tamoxifen in combination with fenretinide. An approach to co-target ER and NF-κB pathways has been proposed, and the concept has been demonstrated by a hybrid drug raloxifene-fumarate [52]. In a human trial, the addition of diindolylmethane, a metabolite of indole-3-carbinol—a constituent in cruciferous vegetables, to tamoxifen therapy increased serum sex-hormone binding globulin and reduced tamoxifen metabolites compared to tamoxifen treatment alone, but did not change in breast density [116]. A recent study in rats showed that combination with n-3 fatty acids enabled the use of a lower dose of raloxifene and increased the chemopreventive effect against ER-negative breast cancer [77]. More research is needed to find better combinations of SERMs with drugs or dietary chemicals to enhance chemoprevention at doses that minimize adverse side effects.
The use of SERMs, even by women at high risk for breast cancer, has been limited by their side effects, including cardiovascular events and infertility, as well as by risk perception [69, 83, 94]. Women may be reluctant to initiate tamoxifen because studies have not shown an increase in overall survival rate or quality of life. In a 2016 survey of 622 women, it was shown that women see cancer prevention and maintenance of fertility as the two top concerns and they do not feel that current drugs meet their needs [69]. Risk perception is one of the main reasons for low uptake of tamoxifen as well as other chemopreventive drugs. Despite research that correlates early menopause to lowered breast cancer risk, women who have an early onset of menopause have a higher worry over breast cancer and a lower likelihood to initiate tamoxifen therapy [94]. Emotional counseling in high-risk women may lead to an increase in initiation and maintenance of therapy, but this needs to be verified.
Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
Inflammation is known to promote cancer development, especially colorectal cancer (CRC) [26]. CRC prevention by NSAIDs has been extensively studied [4, 11, 119]. The major mechanism by which NSAIDs prevent CRC is the inhibition of cyclooxygenase enzymes and suppression of the NF-kB pathway, which decreases inflammation and increases apoptosis [119]. Aspirin is an inhibitor of both cyclooxygenase (COX)-1 and -2. The strong evidence of colon cancer prevention by aspirin, as well as its side effects in causing gastrointestinal bleeding in some individuals, have been studied extensively [2, 13, 19, 30, 42, 95]. Early epidemiological studies have suggested that aspirin intake is associated with a lower incidence of CRC. In five RCTs in more than 3000 subjects with a prior history of adenoma or CRC, intake of aspirin (doses ranged of 81–325 mg daily) showed significantly reduced risk for the recurrence of colon adenoma. In two large cohort studies: the Nurses’ Health Study and the Health Professional Follow-Up Study, starting in 1980 and 1986, respectively, information on diet aspirin use, tobacco use, BMI, and other information were taken. In these studies, regular aspirin use for more than 10 years was found to reduce the risk of CRC by more than 30%. Further studies also indicated that aspirin use in this cohort also significantly reduced CRC-specific mortality. However, aspirin use was found to have a dose-dependent increase in gastrointestinal bleeding, showing a relative risk of 1.59 in groups using 6–14 standard tablets of aspirin per week [42]. Because of this concern, the US Preventive Service Task Force recommended against routine use of aspirin or NSAIDs to prevent CRC in average risk individuals in 2007. However, the Task Force recently reversed its position and recommended the use of aspirin for the prevention of CRC, because recent studies revealed more beneficial effects of aspirin use [6]. For example, a study suggests that aspirin intake not only reduces the risk of CRC but also other cancers [2, 95]. In the two large cohort studies mentioned above, aspirin was found to be more effective in individuals with low expression of 15-hydroxyprostaglandin dehydrogenase [30]. Regular aspirin use was found to reduce the risk and mortality in patients with tumors overexpressing COX-2 and reduced CRC-induced mortality within patients with tumors expressing mutant PIK3CA. The use of aspirin for the treatment of cancer has also been explored. After a systematic review and meta-analyses of the published studies, the authors highlighted the need for randomized trials of aspiring treatment in a variety of cancers [27].
To avoid the side effects due to inhibition of COX-1, many selective COX-2-inhibitors have been developed for the treatment of pain-associated arthritis. Such drugs have also been studied for CRC prevention. For example, celecoxib (400 mg/day) was studied in individuals who have a history of adenomas in two trials, with treatment and follow-up for 3 years [3, 4]. Celecoxib treatment was shown to significantly reduce the relative risk of adenoma recurrence and advanced adenocarcinoma incidence. However, these two trials had to be terminated early because of cardiovascular events. Other related “-coxib” COX-2 inhibitors have also been shown to have similar cardiovascular toxicity to celecoxib, with a higher risk in patients with pre-existing cardiovascular risk factors. Because of this concern, two COX-2 inhibitors, rofecoxib and valdecoxib, were withdrawn from the market. A risk and benefit analysis indicated that the risk of celecoxib for inducing cardiovascular events outweighs its beneficial effect for the prevention of CRC [91]. Some researchers believe that drugs, such as celecoxib, can still be used to prevent colon cancer by individuals who are at high risk for this cancer but at low risk for CVDs. A microbead formulation being studied has the potential to decrease the cardiovascular side effects [122]. Another approach is to use these NSAIDs at low doses in combination with another class of drugs. A successful example is the use of sulindac in combination with a low dose of difluoromethylornithine in a trial for preventing the progression of adenomas [82].
In the development of chemopreventive drugs, repurposing existing drugs appears to be an effective approach, because the safety profile of the drug is already known. The successful stories are tamoxifen and aspirin. Since tamoxifen is already a therapeutic drug for breast cancer, its application illustrates the concept of “early treatment.” In the study of “-coxib” drugs for CRC prevention, after much effort and earlier excitement, the risk for cardiovascular events destroyed a good story.
Lessons Learned
Leads from epidemiological studies have generated interesting hypotheses on cancer prevention by dietary constituents, but few human trials have yielded convincing data to support the hypotheses tested [79]. A great number of laboratory studies suggested the potential cancer preventive activities of many naturally occurring and synthetic compounds, but results of these agents in human studies have been disappointing. In this section, we will discuss why many of the human trials failed to generate the expected results. The lessons learned in cancer chemoprevention research are discussed below.
Importance of Nutritional Status of the Population
As discussed above, epidemiological studies have shown associations between lower intake of certain micronutrients and increased cancer risk. In most situations, supplementation of a nutrient is only effective in preventing cancer in subjects with insufficiency in that nutrient. This concept is consistent with the result from the LNIT in studying a population with general micronutrient insufficiency. The NPC trial also showed that a beneficial effect of selenium supplementation was observed only in individuals with low baseline serum levels of selenium [16, 25]. Thus, trials would probably not work in subjects with sufficient levels of the intervening nutrients. This may be the case with the SELECT [71]. The mean baseline median plasma level of α-T and serum level of selenium was 12.5 μg/mL and 135 ng/mL, respectively, indicating the sufficiency of these nutrients. Many efforts have been made to develop metabolites or derivatives of nutrients as chemopreventive agents. For example, retinoic acid derivatives [110] have shown promise in the prevention of head and neck cancers in early studies [40], but later studies demonstrated lower beneficial to risk ratio [53, 85]. There are yet good examples to show that nutrients or their derivatives can be used as pharmaceutical agents for cancer prevention.
Problems in Interpreting Results from Laboratory Studies
At high enough concentrations, most phytochemicals are likely to inhibit growth or induce death of cancer cells in culture, and a large number of associated molecular changes can be observed. Based on these results, numerous mechanisms for the action of these agents have been proposed. Because of the large differences between situations in vitro and in vivo, it is possible that most of these proposed mechanisms are just the effects observed under the experimental conditions, but may not be related to cancer prevention. Even when an agent can be demonstrated to prevent cancer in rodent models, such activity in humans cannot be predicted because of the biological differences between rodents and humans. The dose-response relationship is also an important issue.
Bioavailabilities of Chemopreventive Agents and Dose-Response Relationship
Bioavailability is a major issue in correlating results from studies in cell lines, animals, and humans. An agent is only effective if sufficient concentrations can reach the target organs. Without considering the poor bioavailability of certain compounds (such as EGCG and curcumin), cell line studies could be misleading. A human trial may yield negative results because the dose of an agent may be too low or too high. For most agents, the doses required to demonstrate a cancer preventive effect in laboratory animals are usually higher than the levels of human consumption. However, a recent study of Apc Min mice on a high-fat diet showed a nonlinear dose-response of resveratrol: the lowest dose of resveratrol (0.00007% in the diet) suppressed intestinal adenoma development better than a higher dose (0.0143% in diet) did [9]. The dose of 0.00007% in the diet (corresponding to 0.35 mg for a person taking 500 g of food in dry weight per day) is extremely low. The results are intriguing. This demonstrates more studies on dose-response relationships are needed.
Side Effects and Toxicity
With pharmacological agents, there are often side effects. The cardiovascular risk of some “-coxib” NSAIDS outweighs the benefits in CRC prevention, and their use in cancer prevention is not recommended. On the other hand, the CRC preventive activity of aspirin outweighs the gastrointestinal bleeding issues (in some individuals) and the US Prevention Task Force recently endorsed the use of aspirin for the prevention of CRC [6]. For developing new drugs, toxicity is always a concern. The concept that natural products have very low or no toxicity may not be correct. For example, liver toxicity, due to intake of green tea extract-based supplement in large bolus doses for weight reduction, is well documented [61, 98]. The concept that naturally occurring compounds are nontoxic is based on observations from the intake of moderate doses or from agents with low bioavailabilities. When the bioavailability is significantly increased, for example, by the use of nanoparticles, toxicity should be an important concern.
Limitations of Current Chemoprevention Trials
Some dietary constituents may exert their protective effects early in life or many years before the onset of pre-malignant lesions. Clinical intervention studies are not able to study the population at such an early stage or for a long period of time. Some intervention studies might have started too late, such as when individuals already had precancerous lesions, or ended too early. Therefore, post-intervention follow-up is very important. It has been reported that in rats, supplementation with folic acid at an early stage of carcinogenesis decreased colon carcinogenesis, whereas supplementation at the late stage enhanced colon carcinogenesis [55]. The latter phenomenon is also consistent with the results of a human trial on colon cancer [17]. Therefore, a negative result in a human trial does not imply a lack of cancer preventive effect of this agent in early life or under other settings. Research on cancer chemoprevention is a rather complicated field. It is possible that many of the inconsistent observations in human studies were due to the lack of power to detect a protective effect in some intervention trials or due to chances for false negative or false positive results when multiple endpoints were analyzed.
Concluding Remarks
Important advances have been made in the field of cancer chemoprevention in the past 30 years [101, 111]; however, there are also many inconsistent and disappointing results. There is even the notion that “Chemoprevention of cancer is an almost universal failure” [90]. We do not agree with this statement. Many trials yielded disappointing results because of problems in the hypothesis, agent and the dosage used, the trial population, and/or the short trial period as described above. Therefore, more basic and clinical studies are needed. After we understand why some of the previous human trials failed, we can design better studies in the future.
Development of new approaches and new agents is urgently needed for cancer chemoprevention. The importance of immune defense is well-recognized and rapid advancement in immunotherapy has been made (reviewed in [81, 102, 107]). Phytochemical approaches for developing cancer immunotherapy has also been discussed [136]. The development of agents that enhance immune functions, such as natural killer cells mobilization and redistribution—recently demonstrated in mice subjected to running wheel exercise [87]—may be a promising approach for cancer prevention.
Among the lessons that we have learned, we would like to emphasize the importance of the integration of laboratory and human studies. For laboratory researchers, it is important to have human relevance in mind when pursuing studies. It is also important for epidemiologists and human trial investigators to appreciate the value of laboratory studies and recognize the limitation in the power of their studies in testing a hypothesis. Cancer prevention is an important field of research aimed to reduce human suffering. More interactions between laboratory researchers and scientists in human studies will lead to fruitful collaborations to advance the field of cancer chemoprevention.
Abbreviations
- α-, γ- or δ-T:
-
α-, γ- or δ-tocopherol
- ATBC:
-
α-Tocopherol and β-Carotene study
- CARET:
-
Carotene and Retinol Efficacy Trial
- CVDs:
-
cardiovascular diseases
- EGCG:
-
(−)-epigallocatechin-3-gallate
- ESCC:
-
esophageal squamous cell carcinoma
- GCA:
-
gastric cardia adenoma
- LNIT:
-
Linxian Nutritional Intervention Trial
- NPC:
-
Nutritional Prevention of Cancer study
- PIN:
-
prostate intraepithelial neoplasia
- RCT:
-
randomized controlled trial
- ROS:
-
reactive oxygen species
- SELECT:
-
Selenium and Vitamin E Cancer Prevention Trial
References
Adhami VM, Siddiqui IA, Ahmad N, Gupta S, Mukhtar H. Oral consumption of green tea polyphenols inhibits insulin-like growth factor-I-induced signaling in an autochthonous mouse model of prostate cancer. Cancer Res. 2004;64(23):8715–22. https://doi.org/10.1158/0008-5472.CAN-04-2840.
Algra AM, Rothwell PM. Effects of regular aspirin on long-term cancer incidence and metastasis: a systematic comparison of evidence from observational studies versus randomised trials. Lancet Oncol. 2012;13(5):518–27. https://doi.org/10.1016/S1470-2045(12)70112-2.
Arber N, Eagle CJ, Spicak J, Racz I, Dite P, Hajer J, et al. Celecoxib for the prevention of colorectal adenomatous polyps. N Engl J Med. 2006;355(9):885–95. https://doi.org/10.1056/NEJMoa061652.
Bertagnolli MM, Eagle CJ, Zauber AG, Redston M, Solomon SD, Kim K, et al. Celecoxib for the prevention of sporadic colorectal adenomas. N Engl J Med. 2006;355(9):873–84. https://doi.org/10.1056/NEJMoa061355.
Bettuzzi S, Brausi M, Rizzi F, Castagnetti G, Peracchia G, Corti A. Chemoprevention of human prostate cancer by oral administration of green tea catechins in volunteers with high-grade prostate intraepithelial neoplasia: a preliminary report from a one-year proof-of-principle study. Cancer Res. 2006;66(2):1234–40. https://doi.org/10.1158/0008-5472.can-05-1145.
Bibbins-Domingo K. Force USPST. Aspirin use for the primary prevention of cardiovascular disease and colorectal cancer: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2016;164(12):836–45. https://doi.org/10.7326/M16-0577.
Blot WJ, Li J-Y, Taylor PR, Guo W, Dawsey S, Wang G-Q, et al. Nutrition intervention trials in Linxian, China: supplementation with specific vitamin/mineral combinations, cancer incidence, and disease-specific mortality in the general population. J Natl Cancer Inst. 1993;85:483–1491.
Bode AM, Dong Z. Cancer prevention research—then and now. Nat Rev Cancer. 2009;9(7):508–16. https://doi.org/10.1038/nrc2646.
Cai H, Scott E, Kholghi A, Andreadi C, Rufini A, Karmokar A, et al. Cancer chemoprevention: evidence of a nonlinear dose response for the protective effects of resveratrol in humans and mice. Sci Transl Med. 2015;7(298):298ra117. https://doi.org/10.1126/scitranslmed.aaa7619.
Campbell S, Stone W, Whaley S, Krishnan K. Development of gamma-tocopherol as a colorectal cancer chemopreventive agent. Crit Rev Oncol Hematol. 2003;47(3):249–59.
Cao Y, Nishihara R, Wu K, Wang M, Ogino S, Willett WC, et al. Population-wide impact of long-term use of aspirin and the risk for cancer. JAMA Oncology. 2016;2(6):762–9. https://doi.org/10.1001/jamaoncol.2015.6396.
Caporali A, Davalli P, Astancolle S, D’Arca D, Brausi M, Bettuzzi S, et al. The chemopreventive action of catechins in the TRAMP mouse model of prostate carcinogenesis is accompanied by clusterin over-expression. Carcinogenesis. 2004;25(11):2217–24. https://doi.org/10.1093/carcin/bgh235.
Chan AT, Arber N, Burn J, Chia WK, Elwood P, Hull MA, et al. Aspirin in the chemoprevention of colorectal neoplasia: an overview. Cancer Prev Res (Phila). 2012;5(2):164–78. https://doi.org/10.1158/1940-6207.capr-11-0391.
Chen JX, Li G, Wang H, Liu A, Lee MJ, Reuhl K, et al. Dietary tocopherols inhibit PhIP-induced prostate carcinogenesis in CYP1A-humanized mice. Cancer Lett. 2016;371(1):71–8. https://doi.org/10.1016/j.canlet.2015.11.010.
Chen JX, Liu A, Lee MJ, Wang H, Yu S, Chi E, et al. Delta- and gamma-tocopherols inhibit phIP/DSS-induced colon carcinogenesis by protection against early cellular and DNA damages. Mol Carcinog. 2017;56(1):172–83. https://doi.org/10.1002/mc.22481.
Clark LC, Combs GF Jr, Turnbull BW, Slate EH, Chalker DK, Chow J, et al. Effects of selenium supplementation for cancer prevention in patients with carcinoma of the skin. A randomized controlled trial. Nutritional Prevention of Cancer Study Group. JAMA. 1996;276(24):1957–63.
Cole BF, Baron JA, Sandler RS, Haile RW, Ahnen DJ, Bresalier RS, et al. Folic acid for the prevention of colorectal adenomas: a randomized clinical trial. J Am Medical Asso. 2007;297(21):2351–9. https://doi.org/10.1001/jama.297.21.2351.
Combs GF Jr, Clark LC, Turnbull BW. An analysis of cancer prevention by selenium. Biofactors. 2001;14(1–4):153–9.
Cook NR, Lee IM, Zhang SM, Moorthy MV, Buring JE. Alternate-day, low-dose aspirin and cancer risk: long-term observational follow-up of a randomized trial. Ann Intern Med. 2013;159(2):77–85. https://doi.org/10.7326/0003-4819-159-2-201307160-00002.
Costa M, Saldanha P. Risk reduction strategies in breast cancer prevention. Eur J Breast Health. 2017;13(3):103–12. https://doi.org/10.5152/ejbh.2017.3583.
Crew KD, Albain KS, Hershman DL, Unger JM, Lo SS. How do we increase uptake of tamoxifen and other anti-estrogens for breast cancer prevention? npj Breast Cancer. 2017;3(1):20. https://doi.org/10.1038/s41523-017-0021-y.
Cuzick J, Sestak I, Bonanni B, Costantino JP, Cummings S, DeCensi A, et al. Selective oestrogen receptor modulators in prevention of breast cancer: an updated meta-analysis of individual participant data. Lancet. 2013;381(9880):1827–34. https://doi.org/10.1016/s0140-6736(13)60140-3.
Das Gupta S, Sae-Tan S, Wahler J, So JY, Bak MJ, Cheng LC, et al. Dietary gamma-tocopherol-rich mixture inhibits estrogen-induced mammary tumorigenesis by modulating estrogen metabolism, antioxidant response, and PPARgamma. Cancer Prev Res (Phila). 2015;8(9):807–16. https://doi.org/10.1158/1940-6207.capr-15-0154.
Detre SI, Ashley S, Mohammed K, Smith IE, Powles TJ, Dowsett M. Immunohistochemical phenotype of breast cancer during 25-year follow-up of the Royal Marsden Tamoxifen Prevention Trial. Cancer Prev Res. 2017;10(3):171–6. https://doi.org/10.1158/1940-6207.CAPR-16-0247-T.
Duffield-Lillico AJ, Dalkin BL, Reid ME, Turnbull BW, Slate EH, Jacobs ET, et al. Selenium supplementation, baseline plasma selenium status and incidence of prostate cancer: an analysis of the complete treatment period of the Nutritional Prevention of Cancer Trial. BJU Int. 2003;91(7):608–12.
Elinav E, Nowarski R, Thaiss CA, Hu B, Jin C, Flavell RA. Inflammation-induced cancer: crosstalk between tumours, immune cells and microorganisms. Nat Rev Cancer. 2013;13(11):759–71. https://doi.org/10.1038/nrc3611.
Elwood PC, Morgan G, Pickering JE, Galante J, Weightman AL, Morris D, et al. Aspirin in the treatment of cancer: reductions in metastatic spread and in mortality: a systematic review and meta-analyses of published studies. PLoS One. 2016;11(4):e0152402. https://doi.org/10.1371/journal.pone.0152402.
Ermakova S, Choi BY, Choi HS, Kang BS, Bode AM, Dong Z. The intermediate filament protein vimentin is a new target for epigallocatechin gallate. J Biol Chem. 2005;280(17):16882–90. https://doi.org/10.1074/jbc.M414185200.
Ermakova SP, Kang BS, Choi BY, Choi HS, Schuster TF, Ma WY, et al. (-)-Epigallocatechin gallate overcomes resistance to etoposide-induced cell death by targeting the molecular chaperone glucose-regulated protein 78. Cancer Res. 2006;66(18):9260–9. https://doi.org/10.1158/0008-5472.CAN-06-1586.
Fink SP, Yamauchi M, Nishihara R, Jung S, Kuchiba A, Wu K, et al. Aspirin and the risk of colorectal cancer in relation to the expression of 15-hydroxyprostaglandin dehydrogenase (HPGD). Sci Transl Med. 2014;6(233):233re2. https://doi.org/10.1126/scitranslmed.3008481.
Gao YT, McLaughlin JK, Blot WJ, Ji BT, Dai Q, Fraumeni JF Jr. Reduced risk of esophageal cancer associated with green tea consumption. J Natl Cancer Inst. 1994;86(11):855–8.
Gaziano JM, Glynn RJ, Christen WG, Kurth T, Belanger C, MacFadyen J, et al. Vitamins E and C in the prevention of prostate and total cancer in men: the Physicians’ Health Study II randomized controlled trial. J Am Medical Asso. 2009;301(1):52–62. https://doi.org/10.1001/jama.2008.862.
Gonzalez-Vallinas M, Gonzalez-Castejon M, Rodriguez-Casado A, Ramirez de Molina A. Dietary phytochemicals in cancer prevention and therapy: a complementary approach with promising perspectives. Nutr Rev. 2013;71(9):585–99. https://doi.org/10.1111/nure.12051.
Group TA-TBCCPS. The effect of Vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. N Engl J Med. 1994;330(15):1029–35. https://doi.org/10.1056/nejm199404143301501.
Guan F, Li GX, Liu AB, Lee M-J, Yang Z, Chen Y-K, et al. Delta- and gramma-tocopherols, but no alpha-tocopherols, inhibit colon carcinogenesis in azoxymethane-treated F344 rats. Cancer Prev Res. 2012;5:644–54.
Hakim IA, Harris RB, Brown S, Chow HH, Wiseman S, Agarwal S, et al. Effect of increased tea consumption on oxidative DNA damage among smokers: a randomized controlled study. J Nutr. 2003;133(10):3303S–9S.
He Z, Tang F, Ermakova S, Li M, Zhao Q, Cho YY, et al. Fyn is a novel target of (-)-epigallocatechin gallate in the inhibition of JB6 Cl41 cell transformation. Mol Carcinog. 2008;47(3):172–83. https://doi.org/10.1002/mc.20299.
Heinonen OP, Albanes D, Virtamo J, Taylor PR, Huttunen JK, Hartman AM, et al. Prostate cancer and supplementation with alpha-tocopherol and beta-carotene: incidence and mortality in a controlled trial. J Natl Cancer Inst. 1998;90(6):440–6.
Hensley K, Benaksas EJ, Bolli R, Comp P, Grammas P, Hamdheydari L, et al. New perspectives on vitamin E: gamma-tocopherol and carboxyelthylhydroxychroman metabolites in biology and medicine. Free Radic Biol Med. 2004;36(1):1–15.
Hong WK, Lippman SM, Itri LM, Karp DD, Lee JS, Byers RM, et al. Prevention of second primary tumors with isotretinoin in squamous-cell carcinoma of the head and neck. N Engl J Med. 1990;323(12):795–801. https://doi.org/10.1056/NEJM199009203231205.
Hou Z, Sang S, You H, Lee MJ, Hong J, Chin KV, et al. Mechanism of action of (-)-epigallocatechin-3-gallate: auto-oxidation-dependent inactivation of epidermal growth factor receptor and direct effects on growth inhibition in human esophageal cancer KYSE 150 cells. Cancer Res. 2005;65(17):8049–56. https://doi.org/10.1158/0008-5472.CAN-05-0480.
Huang ES, Strate LL, Ho WW, Lee SS, Chan AT. Long-term use of aspirin and the risk of gastrointestinal bleeding. Am J Med. 2011;124(5):426–33. https://doi.org/10.1016/j.amjmed.2010.12.022.
Huang HY, Alberg AJ, Norkus EP, Hoffman SC, Comstock GW, Helzlsouer KJ. Prospective study of antioxidant micronutrients in the blood and the risk of developing prostate cancer. Am J Epidemiol. 2003;157(4):335–44.
Huang YQ, Lu X, Min H, Wu QQ, Shi XT, Bian KQ, et al. Green tea and liver cancer risk: A meta-analysis of prospective cohort studies in Asian populations. Nutrition. 2016;32(1):3–8. https://doi.org/10.1016/j.nut.2015.05.021.
Ip C. Lessons from basic research in selenium and cancer prevention. J Nutr. 1998;128(11):1845–54.
Jiang Q. Natural forms of vitamin E: metabolism, antioxidant, and anti-inflammatory activities and their role in disease prevention and therapy. Free Radic Biol Med. 2014;72:76–90. https://doi.org/10.1016/j.freeradbiomed.2014.03.035.
Jiang Q, Christen S, Shigenaga MK, Ames BN. gamma-tocopherol, the major form of vitamin E in the US diet, deserves more attention. Am J Clin Nutr. 2001;74(6):714–22.
Joe AK, Schnoll-Sussman F, Bresalier RS, Abrams JA, Hibshoosh H, Cheung K, et al. Phase Ib randomized, double-blinded, placebo-controlled, dose escalation study of Polyphenon E in patients with Barrett’s esophagus. Cancer Prev Res. 2015;8(12):1131–7. https://doi.org/10.1158/1940-6207.CAPR-14-0274-T.
Ju J, Hao X, Lee MJ, Lambert JD, Lu G, Xiao H, et al. A gamma-tocopherol-rich mixture of tocopherols inhibits colon inflammation and carcinogenesis in azoxymethane and dextran sulfate sodium-treated mice. Cancer Prev Res. 2009;2(2):143–52. https://doi.org/10.1158/1940-6207.CAPR-08-0099.
Ju J, Hong J, Zhou JN, Pan Z, Bose M, Liao J, et al. Inhibition of intestinal tumorigenesis in Apcmin/+ mice by (-)-epigallocatechin-3-gallate, the major catechin in green tea. Cancer Res. 2005;65(22):10623–31. https://doi.org/10.1158/0008-5472.CAN-05-1949.
Ju J, Picinich SC, Yang Z, Zhao Y, Suh N, Kong AN, et al. Cancer-preventive activities of tocopherols and tocotrienols. Carcinogenesis. 2010;31(4):533–42. https://doi.org/10.1093/carcin/bgp205.
Kastrati I, Siklos MI, Brovkovych SD, Thatcher GRJ, Frasor J. A novel strategy to co-target estrogen receptor and nuclear factor kappaB pathways with hybrid drugs for breast cancer therapy. Hormones Cancer. 2017;8(3):135–42. https://doi.org/10.1007/s12672-017-0294-5.
Khuri FR, Lee JJ, Lippman SM, Kim ES, Cooper JS, Benner SE, et al. Randomized phase III trial of low-dose isotretinoin for prevention of second primary tumors in stage I and II head and neck cancer patients. J Natl Cancer Inst. 2006;98(7):441–50. https://doi.org/10.1093/jnci/djj091.
Kim DE, Kim Y, Cho DH, Jeong SY, Kim SB, Suh N, et al. Raloxifene induces autophagy-dependent cell death in breast cancer cells via the activation of AMP-activated protein kinase. Mol Cells. 2015;38(2):138–44. 10.14348/molcells.2015.2193.
Kim YI. Folate, colorectal carcinogenesis, and DNA methylation: lessons from animal studies. Environ Mol Mutagen. 2004;44(1):10–25. https://doi.org/10.1002/em.20025.
Klein EA, Thompson IM Jr, Tangen CM, Crowley JJ, Lucia MS, Goodman PJ, et al. Vitamin E and the risk of prostate cancer: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). J Am Medical Asso. 2011;306(14):1549–56. https://doi.org/10.1001/jama.2011.1437.
Kristal AR, Darke AK, Morris JS, Tangen CM, Goodman PJ, Thompson IM, et al. Baseline selenium status and effects of selenium and vitamin e supplementation on prostate cancer risk. J Natl Cancer Inst. 2014;106(3):djt456. https://doi.org/10.1093/jnci/djt456.
Kumar NB, Pow-Sang J, Egan KM, Spiess PE, Dickinson S, Salup R, et al. Randomized, placebo-controlled trial of green tea catechins for prostate cancer prevention. Cancer Prev Res (Phila). 2015; https://doi.org/10.1158/1940-6207.capr-14-0324.
Kumazoe M, Sugihara K, Tsukamoto S, Huang Y, Tsurudome Y, Suzuki T, et al. 67-kDa laminin receptor increases cGMP to induce cancer-selective apoptosis. J Clin Invest. 2013;123(2):787–99. https://doi.org/10.1172/JCI64768.
Kuriyama S, Shimazu T, Ohmori K, Kikuchi N, Nakaya N, Nishino Y, et al. Green tea consumption and mortality due to cardiovasular disease, cancer, and all causes in Japan: the Ohsaki study. JAMA. 2006;296(10):1255–65.
Lambert JD, Kennett MJ, Sang S, Reuhl KR, Ju J, Yang CS. Hepatotoxicity of high oral dose (-)-epigallocatechin-3-gallate in mice. Food Chem Toxicol. 2010;48(1):409–16. https://doi.org/10.1016/j.fct.2009.10.030.
Lambert JD, Lu G, Lee MJ, Hu J, Ju J, Yang CS. Inhibition of lung cancer growth in mice by dietary mixed tocopherols. Mol Nutr Food Res. 2009;53(8):1030–5. https://doi.org/10.1002/mnfr.200800438.
Lee HJ, Ju J, Paul S, So JY, DeCastro A, Smolarek A, et al. Mixed tocopherols prevent mammary tumorigenesis by inhibiting estrogen action and activating PPAR-gamma. Clin Cancer Res. 2009;15(12):4242–9. https://doi.org/10.1158/1078-0432.CCR-08-3028.
Lee IM, Cook NR, Gaziano JM, Gordon D, Ridker PM, Manson JE, et al. Vitamin E in the primary prevention of cardiovascular disease and cancer: the Women’s Health Study: a randomized controlled trial. J Am Medical Asso. 2005;294(1):56–65.
Li GX, Lee MJ, Liu AB, Yang Z, Lin Y, Shih WJ, et al. Delta-tocopherol is more active than alpha- or gamma-tocopherol in inhibiting lung tumorigenesis in vivo. Cancer Prev Res. 2011;4(3):404–13. https://doi.org/10.1158/1940-6207.CAPR-10-0130.
Li JY, Taylor PR, Li B, Dawsey S, Wang GQ, Ershow AG, et al. Nutrition intervention trials in Linxian, China: multiple vitamin/mineral supplementation, cancer incidence, and disease-specific mortality among adults with esophageal dysplasia. J Natl Cancer Inst. 1993;85(18):1492–8.
Li M, He Z, Ermakova S, Zheng D, Tang F, Cho YY, et al. Direct inhibition of insulin-like growth factor-I receptor kinase activity by (-)-epigallocatechin-3-gallate regulates cell transformation. Cancer Epidemiol Biomark Prev. 2007;16(3):598–605. https://doi.org/10.1158/1055-9965.EPI-06-0892.
Li N, Sun Z, Han C, Chen J. The chemopreventive effects of tea on human oral precancerous mucosa lesions. Proc Soc Exp Biol Med Soc Exp Biol Med. 1999;220(4):218–24.
Liede A, Mansfield CA, Metcalfe KA, Price MA, Kathleen Cuningham Foundation Consortium for Research into Familial Breast C, Snyder C, et al. Preferences for breast cancer risk reduction among BRCA1/BRCA2 mutation carriers: a discrete-choice experiment. Breast Cancer Res Treat. 2017; https://doi.org/10.1007/s10549-017-4332-3.
Limburg PJ, Wei W, Ahnen DJ, Qiao Y, Hawk ET, Wang G, et al. Randomized, placebo-controlled, esophageal squamous cell cancer chemoprevention trial of selenomethionine and celecoxib. Gastroenterology. 2005;129(3):863–73. https://doi.org/10.1053/j.gastro.2005.06.024.
Lippman SM, Klein EA, Goodman PJ, Lucia MS, Thompson IM, Ford LG, et al. Effect of selenium and vitamin E on risk of prostate cancer and other cancers: the Selenium and Vitamin E Cancer Prevention Trial (SELECT). J Am Medical Asso. 2009;301(1):39–51. https://doi.org/10.1001/jama.2008.864.
Liu J, Liu S, Zhou H, Hanson T, Yang L, Chen Z, et al. Association of green tea consumption with mortality from all-cause, cardiovascular disease and cancer in a Chinese cohort of 165,000 adult men. Eur J Epidemiol. 2016;31(9):853–65.
Lu G, Liao J, Yang G, Reuhl KR, Hao X, Yang CS. Inhibition of adenoma progression to adenocarcinoma in a 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone-induced lung tumorigenesis model in A/J mice by tea polyphenols and caffeine. Cancer Res. 2006;66(23):11494–501. https://doi.org/10.1158/0008-5472.CAN-06-1497.
Lu G, Xiao H, Li GX, Picinich SC, Chen YK, Liu A, et al. A gamma-tocopherol-rich mixture of tocopherols inhibits chemically induced lung tumorigenesis in A/J mice and xenograft tumor growth. Carcinogenesis. 2010;31(4):687–94. https://doi.org/10.1093/carcin/bgp332.
Makiuchi T, Sobue T, Kitamura T, Ishihara J, Sawada N, Iwasaki M, et al. Association between green tea/coffee consumption and biliary tract cancer: a population-based cohort study in Japan. Cancer Sci. 2016;107(1):76–83. https://doi.org/10.1111/cas.12843.
Mallick S, Benson R, Julka PK. Breast cancer prevention with anti-estrogens: review of the current evidence and future directions. Breast Cancer. 2016;23(2):170–7. https://doi.org/10.1007/s12282-015-0647-2.
Manni A, El-Bayoumy K, Skibinski CG, Thompson HJ, Santucci-Pereira J, Bidinotto LT, et al. Combination of antiestrogens and omega-3 fatty acids for breast cancer prevention. Biomed Res Int. 2015;2015:638645. https://doi.org/10.1155/2015/638645.
Mark SD, Qiao YL, Dawsey SM, Wu YP, Katki H, Gunter EW, et al. Prospective study of serum selenium levels and incident esophageal and gastric cancers. J Natl Cancer Inst. 2000;92(21):1753–63.
Martinez ME, Jacobs ET, Baron JA, Marshall JR, Byers T. Dietary supplements and cancer prevention: balancing potential benefits against proven harms. J Natl Cancer Inst. 2012;104(10):732–9. https://doi.org/10.1093/jnci/djs195.
Maximov PY, Jordan VC. Is there a role for raloxifene and tamoxifen for the prevention of breast cancer? In: Russo J, editor. Trends in breast cancer prevention. Cham: Springer International Publishing; 2016. p. 83–101.
McNutt M. Cancer immunotherapy. Science. 2013;342(6165):1417. https://doi.org/10.1126/science.1249481.
Meyskens FL Jr, McLaren CE, Pelot D, Fujikawa-Brooks S, Carpenter PM, Hawk E, et al. Difluoromethylornithine plus sulindac for the prevention of sporadic colorectal adenomas: a randomized placebo-controlled, double-blind trial. Cancer Prev Res. 2008;1(1):32–8. https://doi.org/10.1158/1940-6207.CAPR-08-0042.
Nichols HB, Stürmer T, Lee VS, Anderson C, Lee JS, Roh JM, et al. Breast cancer chemoprevention in an integrated health care setting. JCO Clin Cancer Inform. 2017;1:1–12. https://doi.org/10.1200/cci.16.00059.
Omenn GS, Goodman GE, Thornquist MD, Balmes J, Cullen MR, Glass A, et al. Effects of a combination of beta carotene and vitamin A on lung cancer and cardiovascular disease. N Engl J Med. 1996;334(18):1150–5. https://doi.org/10.1056/NEJM199605023341802.
Papadimitrakopoulou VA, Lee JJ, William WN Jr, Martin JW, Thomas M, Kim ES, et al. Randomized trial of 13-cis retinoic acid compared with retinyl palmitate with or without beta-carotene in oral premalignancy. J Clin Oncol. 2009;27(4):599–604. https://doi.org/10.1200/JCO.2008.17.1850.
Patel A, Liebner F, Netscher T, Mereiter K, Rosenau T. Vitamin E chemistry. Nitration of non-alpha-tocopherols: products and mechanistic considerations. J Organic Chem. 2007;72(17):6504–12. https://doi.org/10.1021/jo0706832.
Pedersen L, Idorn M, Olofsson GH, Lauenborg B, Nookaew I, Hansen RH, et al. Voluntary running suppresses tumor growth through epinephrine- and IL-6-dependent NK cell mobilization and redistribution. Cell Metab. 2016;23(3):554–62. https://doi.org/10.1016/j.cmet.2016.01.011.
Peters U, Littman AJ, Kristal AR, Patterson RE, Potter JD, White E. Vitamin E and selenium supplementation and risk of prostate cancer in the Vitamins and lifestyle (VITAL) study cohort. Cancer Causes Control. 2008;19(1):75–87. https://doi.org/10.1007/s10552-007-9072-y.
Peto R, Doll R, Buckley JD, Sporn MB. Can dietary beta-carotene materially reduce human cancer rates? Nature. 1981;290(5803):201–8.
Potter JD. The failure of cancer chemoprevention. Carcinogenesis. 2014;35(5):974–82. https://doi.org/10.1093/carcin/bgu063.
Psaty BM, Potter JD. Risks and benefits of celecoxib to prevent recurrent adenomas. N Engl J Med. 2006;355(9):950–2. https://doi.org/10.1056/NEJMe068158.
Qiao YL, Dawsey SM, Kamangar F, Fan JH, Abnet CC, Sun XD, et al. Total and cancer mortality after supplementation with vitamins and minerals: follow-up of the Linxian General Population Nutrition Intervention Trial. J Natl Cancer Inst. 2009;101(7):507–18. https://doi.org/10.1093/jnci/djp037.
Rayman MP. Selenium in cancer prevention: a review of the evidence and mechanism of action. Proc Nutr Soc. 2005;64(4):527–42.
Rondanina G, Puntoni M, Guerrieri-Gonzaga A, Marra D, Bonanni B, DeCensi A. Worry and risk perception of breast cancer in a prevention trial of low dose tamoxifen in midlife postmenopausal hormone users. Breast. 2017;34:108–14. https://doi.org/10.1016/j.breast.2017.05.008.
Rothwell PM, Price JF, Fowkes FG, Zanchetti A, Roncaglioni MC, Tognoni G, et al. Short-term effects of daily aspirin on cancer incidence, mortality, and non-vascular death: analysis of the time course of risks and benefits in 51 randomised controlled trials. Lancet. 2012;379(9826):1602–12. https://doi.org/10.1016/S0140-6736(11)61720-0.
Samavat H, Dostal AM, Wang R, Bedell S, Emory TH, Ursin G, et al. The Minnesota Green Tea Trial (MGTT), a randomized controlled trial of the efficacy of green tea extract on biomarkers of breast cancer risk: study rationale, design, methods, and participant characteristics. Cancer Causes Control. 2015;26(10):1405–19. https://doi.org/10.1007/s10552-015-0632-2.
Sasazuki S, Tamakoshi A, Matsuo K, Ito H, Wakai K, Nagata C, et al. Green tea consumption and gastric cancer risk: an evaluation based on a systematic review of epidemiologic evidence among the Japanese population. Jpn J Clin Oncol. 2012;42(4):335–46. https://doi.org/10.1093/jjco/hys009.
Schonthal AH. Adverse effects of concentrated green tea extracts. Mol Nutr Food Res. 2011;55(6):874–85. https://doi.org/10.1002/mnfr.201000644.
Schwartz JL, Baker V, Larios E, Chung FL. Molecular and cellular effects of green tea on oral cells of smokers: a pilot study. Mol Nutr Food Res. 2005;49(1):43–51. https://doi.org/10.1002/mnfr.200400031.
Scott EN, Gescher AJ, Steward WP, Brown K. Development of dietary phytochemical chemopreventive agents: biomarkers and choice of dose for early clinical trials. Cancer Prev Res (Phila). 2009;2(6):525–30. https://doi.org/10.1158/1940-6207.CAPR-08-0223.
Serrano D, Lazzeroni M, Bonanni B. Cancer chemoprevention: much has been done, but there is still much to do. State of the art and possible new approaches. Mol Oncol. 2015;9(5):1008–17. https://doi.org/10.1016/j.molonc.2014.12.006.
Sharma P, Allison JP. Immune checkpoint targeting in cancer therapy: toward combination strategies with curative potential. Cell. 2015;161(2):205–14. https://doi.org/10.1016/j.cell.2015.03.030.
Shen HH, Huang SY, Cheng PY, Chu YJ, Chen SY, Lam KK, et al. Involvement of HSP70 and HO-1 in the protective effects of raloxifene on multiple organ dysfunction syndrome by endotoxemia in ovariectomized rats. Menopause. 2017; https://doi.org/10.1097/GME.0000000000000864.
Shim JH, Choi HS, Pugliese A, Lee SY, Chae JI, Choi BY, et al. (-)-Epigallocatechin gallate regulates CD3-mediated T cell receptor signaling in leukemia through the inhibition of ZAP-70 kinase. J Biol Chem. 2008;283(42):28370–9. https://doi.org/10.1074/jbc.M802200200.
Shim JH, Su ZY, Chae JI, Kim DJ, Zhu F, Ma WY, et al. Epigallocatechin gallate suppresses lung cancer cell growth through Ras-GTPase-activating protein SH3 domain-binding protein 1. Cancer Prev Res. 2010;3:670–9.
Shimizu M, Shirakami Y, Sakai H, Adachi S, Hata K, Hirose Y, et al. (-)-Epigallocatechin gallate suppresses azoxymethane-induced colonic premalignant lesions in male C57BL/KsJ-db/db mice. Cancer Prev Res. 2008;1(4):298–304. https://doi.org/10.1158/1940-6207.CAPR-08-0045.
Showalter A, Limaye A, Oyer JL, Igarashi R, Kittipatarin C, Copik AJ, et al. Cytokines in immunogenic cell death: applications for cancer immunotherapy. Cytokine. 2017;97:123–32. https://doi.org/10.1016/j.cyto.2017.05.024.
Smolarek AK, So JY, Thomas PE, Lee HJ, Paul S, Dombrowski A, et al. Dietary tocopherols inhibit cell proliferation, regulate expression of ERalpha, PPARgamma, and Nrf2, and decrease serum inflammatory markers during the development of mammary hyperplasia. Mol Carcinog. 2013;52(7):514–25. https://doi.org/10.1002/mc.21886.
Sporn MB. Approaches to prevention of epithelial cancer during the preneoplastic period. Cancer Res. 1976;36(7 PT 2):2699–702.
Sporn MB, Dunlop NM, Newton DL, Smith JM. Prevention of chemical carcinogenesis by vitamin A and its synthetic analogs (retinoids). Fed Proc. 1976;35(6):1332–8.
Steward WP, Brown K. Cancer chemoprevention: a rapidly evolving field. Br J Cancer. 2013;109(1):1–7. https://doi.org/10.1038/bjc.2013.280.
Tachibana H, Koga K, Fujimura Y, Yamada K. A receptor for green tea polyphenol EGCG. Nat Struct Mol Biol. 2004;11(4):380–1. https://doi.org/10.1038/nsmb743.
Takahashi S, Takeshita K, Seeni A, Sugiura S, Tang M, Sato SY, et al. Suppression of prostate cancer in a transgenic rat model via gamma-tocopherol activation of caspase signaling. Display Settings. 2009;69:644–51.
Tang L, Tang M, Xu L, Luo H, Huang T, Yu J, et al. Modulation of aflatoxin biomarkers in human blood and urine by green tea polyphenols intervention. Carcinogenesis. 2008;29(2):411–7. https://doi.org/10.1093/carcin/bgn008.
Taylor PR, Qiao YL, Abnet CC, Dawsey SM, Yang CS, Gunter EW, et al. Prospective study of serum vitamin E levels and esophageal and gastric cancers. J Natl Cancer Inst. 2003;95(18):1414–6.
Thomson CA, Chow HHS, Wertheim BC, Roe DJ, Stopeck A, Maskarinec G, et al. A randomized, placebo-controlled trial of diindolylmethane for breast cancer biomarker modulation in patients taking tamoxifen. Breast Cancer Res Treat. 2017;165(1):97–107. https://doi.org/10.1007/s10549-017-4292-7.
Traber MG. Vitamin E. In: Bowman BA, Russell RM, editors. Present knowledge in nutrition. 9th ed. Washington DC: ILSI Press; 2006. p. 211–9.
Tsao AS, Liu D, Martin J, Tang XM, Lee JJ, El-Naggar AK, et al. Phase II randomized, placebo-controlled trial of green tea extract in patients with high-risk oral premalignant lesions. Cancer Prev Res (Phila). 2009;2(11):931–41. https://doi.org/10.1158/1940-6207.CAPR-09-0121.
Tsioulias GJ, Go MF, Rigas B. NSAIDs and colorectal cancer control: promise and challenges. Curr Pharmacol Rep. 2015;1(5):295–301. https://doi.org/10.1007/s40495-015-0042-x.
Umar A, Dunn BK, Greenwald P. Future directions in cancer prevention. Nat Rev Cancer. 2012;12(12):835–48. https://doi.org/10.1038/nrc3397.
Urusova DV, Shim JH, Kim DJ, Jung SK, Zykova TA, Carper A, et al. Epigallocatechin-gallate suppresses tumorigenesis by directly targeting Pin1. Cancer Prev Res. 2011;4(9):1366–77. https://doi.org/10.1158/1940-6207.CAPR-11-0301.
Venè R, Tosetti F, Minghelli S, Poggi A, Ferrari N, Benelli R. Celecoxib increases EGF signaling in colon tumor associated fibroblasts, modulating EGFR expression and degradation. Oncotarget. 2015;6(14):12310–25.
Wang H, Hong J, Yang CS. Delta-tocopherol inhibits receptor tyrosine kinase-induced AKT activation in prostate cancer cells. Mol Carcinog. 2016;55(11):1728–38. https://doi.org/10.1002/mc.22422.
Wattenberg LW. Chemoprophylaxis of carcinogenesis: a review. Cancer Res. 1966;26(7):1520–6.
Wattenberg LW. An overview of chemoprevention: current status and future prospects. Proc Soc Exp Biol Med Soc Exp Biol Med. 1997;216(2):133–41.
Weinstein SJ, Peters U, Ahn J, Friesen MD, Riboli E, Hayes RB, et al. Serum alpha-tocopherol and gamma-tocopherol concentrations and prostate cancer risk in the PLCO Screening Trial: a nested case-control study. PLoS One. 2012;7(7):e40204. https://doi.org/10.1371/journal.pone.0040204.
Yang CS. Research on esophageal cancer in China: a review. Cancer Res. 1980;40(8 Pt 1):2633–44.
Yang CS, Miao J, Yang W, Huang M, Wang T, Xue H, et al. Diet and vitamin nutrition of the high esophageal cancer risk population in Linxian, China. Nutrition Cancer. 1982;4(2):154–64. https://doi.org/10.1080/01635588209513751.
Yang CS, Newmark H. The roles of micronutrient deficiency in carcinogenesis. In: David S, editor. CRC critical reviews in oncology/hematology. Boca Raton, FL: CRC Press; 1987. p. 267–87.
Yang CS, Suh N, Kong AN. Does vitamin E prevent or promote cancer? Cancer Prev Res. 2012;5(5):701–5. https://doi.org/10.1158/1940-6207.CAPR-12-0045.
Yang CS, Sun Y, Yang QU, Miller KW, Li GY, Zheng SF, et al. Vitamin A and other deficiencies in Linxian, a high esophageal cancer incidence area in northern China. J Natl Cancer Inst. 1984;73(6):1449–53.
Yang CS, Wang H. Cancer preventive activities of tea catechins. Molecules. 2016;21(12) https://doi.org/10.3390/molecules21121679.
Yang CS, Wang X, Lu G, Picinich SC. Cancer prevention by tea: animal studies, molecular mechanisms and human relevance. Nat Rev Cancer. 2009;9(6):429–39. https://doi.org/10.1038/nrc2641.
Yang H, Fang J, Jia X, Han C, Chen X, Yang CS, et al. Chemopreventive effects of early-stage and late-stage supplementation of vitamin E and selenium on esophageal carcinogenesis in rats maintained on a low vitamin E/selenium diet. Carcinogenesis. 2011;32(3):381–8. https://doi.org/10.1093/carcin/bgq279.
Yang HS, Kim MW. The effects of five-year hormone therapy, alendronate, tibolone, and raloxifene on bone mineral density in postmenopausal women (second study). Maturitas. 2017;100:151. https://doi.org/10.1016/j.maturitas.2017.03.124.
Yin SY, Yang NS, Lin TJ. Phytochemicals approach for developing cancer immunotherapeutics. Front Pharmacol. 2017;8:386. https://doi.org/10.3389/fphar.2017.00386.
Yuan JM, Sun C, Butler LM. Tea and cancer prevention: epidemiological studies. Pharmacol Res. 2011;64(2):123–35. https://doi.org/10.1016/j.phrs.2011.03.002.
Zhao LG, Li HL, Sun JW, Yang Y, Ma X, Shu XO, et al. Green tea consumption and cause-specific mortality: results from two prospective cohort studies in China. J Epidemiol. 2017;27(1):36–41. https://doi.org/10.1016/j.je.2016.08.004.
Zhou Q, Li H, Zhou JG, Ma Y, Wu T, Ma H. Green tea, black tea consumption and risk of endometrial cancer: a systematic review and meta-analysis. Arch Gynecol Obstet. 2016;293(1):143–55. https://doi.org/10.1007/s00404-015-3811-1.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Cancer Chemoprevention
Rights and permissions
About this article

Cite this article
Yang, C.S., Wang, H., Dan, V. et al. Cancer Chemoprevention: What Have we Learned?. Curr Pharmacol Rep 3, 409–422 (2017). https://doi.org/10.1007/s40495-017-0108-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40495-017-0108-z