
Abstract
This meta-analysis aimed to evaluate single-case studies that used high-tech speech-generating devices (SGDs) for children with autism spectrum disorders (ASD) ages 0–8. The focus of this review was to measure the effect size of high-tech SGD intervention on verbal behavior. The review included 20 studies with 54 participants with ASD. The results suggest that high-tech SGDs are strongly effective to teach manding, intraverbal, and multistep tacting to children with ASD. Another aim was to evaluate the quality of the studies based on Horner et al.’s (2005) quality indicators. The results suggest a moderate level of evidence for high-tech SGD intervention in children with ASD. Directions for future research and implications for practice are discussed.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Children with autism spectrum disorders (ASD) often have profound deficits in the language and communication developmental domain (Baron-Cohen 2004; Matson et al. 2012). Recent research has indicated 30% of children diagnosed with ASD may never develop functional spoken language (Wodka et al. 2013). As a result of such deficits, children with ASD may be at a greater risk of engaging in challenging behaviors as means of communicating wants and needs (Chung et al. 1996). Studies of Chiang (2008) Kaiser et al. (2002), and Park et al. (2012) continue to show a strong relation between the lack of communication skills and the presence of challenging behaviors such as aggression or self-injurious behavior. Lack of communication skills can also negatively impact social skills (Park et al. 2012) and academic achievement (Walker and Snell 2013). Hence, early intervention to enhance the communication skills of children with ASD is necessary to prevent those effects (Chiang 2008; Walker and Snell 2013).
One way to support the communication skills of children with ASD is through the use of augmentative and alternative communication (AAC) systems. AAC refers to any communicative system that is used to either compensate or supplement existing speech (Schlosser and Wendt 2008). AAC can be an unaided system such as manual signs (MS; e.g., Wendt 2009) or an aided system such as picture exchange (PE; e.g., Frea et al. 2001), picture exchange communication system (PECS; Frost and Bondy 2002), and speech-generating devices (SGDs; e.g., Waddington et al. 2014). SGDs, also known as voice output communication aid (VOCA), are computer electronic devices that can be activated by the communicator to generate digitized or synthesized speech outputs (Rispoli et al. 2010). These devices are typically combined with visual cues such as graphics or line drawings (Mirenda 2003; Ogletree and Oren 2006).
SGDs may be a viable option for children with ASD who lack communication skills. Unlike manual signs, SGDs do not require complex fine motor skills. In addition, speech outputs produced by SGDs are easier to interpret by the communicative partner compared to MS (Lorah et al. 2015). In comparison to picture-communication systems (e.g., PE, PECS), SGDs, tablets with AAC apps to be specific, have more capacity to store more speech outputs/pictures, are easier to carry, and more socially acceptable (Lorah et al. 2013, 2015). Further, SGDs can be used to serve various communication needs such as requesting, labeling, as well as commenting and answering questions (Schlosser 2003). Skinner (1957) refers to these communicative behaviors (i.e., verbal operants) as mands, tacts, and intraverbals, respectively.
Several reviews and meta-analyses have been conducted to evaluate the effects of high-tech SGDs for individuals with ASD. For instance, Lorah et al. (2015) conducted a literature review to summarize and evaluate the quality of existing research on high-tech SGDs. A total of 17 studies that targeted communication skills were included. These studies included a total of 57 participants with ASD and/or developmental disabilities ages 3 to 23 years. The results showed 93% of the participants acquired the skill of communicating via an SGD (i.e., iPad or iPod). Additionally, out of 19 participants taking a preference assessment, 16 showed a clear preference for using an SGD over other types of AAC systems (e.g., PECS). Lorah and colleagues also indicated the reviewed studies reflected a high level of quality based on Horner et al.'s (2005) quality indicators for single-case research. Nonetheless, the authors did not determine the level of evidence for using high-tech SGDs.
Ganz et al. (2012) meta-analyzed 24 single-case studies that had involved a PE, PECS, or SGD-based intervention. The participants included 58 individuals with ASD and other developmental disabilities ages 3 to 40 years. The included studies targeted communication, social, academic skills, and/or challenging behaviors. Overall, Ganz et al. indicated strong impact of aided AAC (i.e., PE, PECS, SGDs) on the targeted skills for this population. However, out of the 24 reviewed studies, only 8 had involved an SGD-based intervention. In addition, the participants included a wide range of ages, and the interventions targeted various skills. Thus, conclusions about the effects of high-tech SGD as an AAC communication intervention for children with ASD specifically remain unclear.
More focused on SGDs, Alzrayer et al. (2014) conducted a meta-analysis to evaluate the effects of high-tech SGDs on the communication skills of individuals with ASD and other developmental disabilities ages 3 to 23 years. The SGDs, in this review, were limited to devices that operate on an iOS system (i.e., iPad and iPod Touch). Alzrayer and colleagues included 15 single-case studies that solely targeted the communication skills of 52 participants. The results showed that iPads and iPod Touch were highly to moderately effective in enhancing the communication skills of individuals with ASD and developmental disabilities. However, in addition to including a wide age range, the effect size was calculated using percentage of non-overlapping data points metric (PND; Scruggs et al. 1987). PND is the percentage of phase B (i.e., intervention) data points that exceed the highest data point in phase A (i.e., baseline) (Parker et al. 2011). Although this metric is widely used in meta-analyses (Scruggs and Mastropieri 2001), it is insensitive to sampling distribution (Parker et al. 2011). In addition, as it only uses the highest data point in phase A and ignores the rest, it can limit the results in studies that have one unusual spike in phase A.
Similarly, Schlosser and Koul (2015) meta-analyzed 47 single-case studies and one group experimental study to evaluate the effects of SGDs on the communication skills and challenging behaviors of individuals with ASD ages 3 to 21 years. The review included a total of 187 participants who had received high-tech SGD as a component of a treatment package, as a comparison to another type of AAC method (e.g., PE), or as a comparison to an SGD condition without a speech output. Overall, the results showed SGDs are effective in teaching individuals with ASD requesting skills. Nonetheless, the researchers directed future meta-analyses to use an effect size metric other than PND—which they used to calculate the effects on communication skills—due to its limitations.
As communication skills are often a high priority in early intervention programs, and as early communication interventions can have a substantial impact on children with ASD (American Academy of Pediatrics 2007; Chiang 2008; Tager-Flusberg and Kasari 2013; Walker and Snell 2013), evaluating the effects of high-tech SGDs for children with ASD is necessary. Previous meta-analyses included a wide age range (3 to age 23, Alzrayer et al. 2014; 3 to age 40, Ganz et al. 2012; 3 to age 21, Schlosser and Koul 2015) which makes the results for a smaller age range inconclusive. In addition, out of the three analyses, only Ganz et al. (2012) applied improvement rate difference (IRD) to calculate the effect size. However, the effect size was not solely calculated for SGDs on communication skills; but rather SGDs on communication, social, academic skills, and challenging behaviors combined. Finally, as federal laws require the implementation of evidence-based practices (Individuals with Disabilities Education Improvement Act [IDEIA] 2004; No Child Left Behind [NCLB] 2001), it becomes crucial to determine whether using high-tech SGD as a communication intervention is evidence-based for children with ASD.
Therefore, the purpose of this review was to meta-analyze single-case studies that used high-tech SGDs to develop communication skills in children with ASD from birth to age 8 using IRD metric. The birth to 8 age range was chosen based on the definition of early childhood by CEC’s Division for Early Childhood (DEC n.d.). Another purpose of this review was to evaluate the quality of the studies based on Horner et al.’s (2005) quality indicators and determine the level of evidence as strong, moderate, or potential (National Technical Assistance Center on Transition [NTACT]; Test et al. 2009), for using high-tech SGD as a communication intervention for children with ASD from birth to 8.
Method
Search Strategy
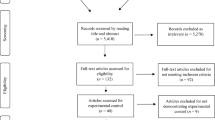
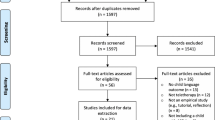
Google Scholar, PsycINFO, MEDLINE, and ERIC were searched to locate studies that focused on the use of high-tech SGDs for children with ASD. The systematic search was conducted using a combination of the following keywords: autism, ASD, SGDs, tablets, communication skills, iPad/iPod Touch, and high-tech AAC/SGD. The search was limited to English-language and peer-reviewed journal articles, but no other geographical or temporal constrains were applied. Additional search strategy was conducted by reviewing the reference lists of the included studies to further find other relevant studies. The initial search that was completed in July of 2017 resulted in a total of 1972 pieces of literature. The majority of the literature (e.g., dissertations/theses, descriptive case studies, books, book chapters) was eliminated based on reviewing the title or the abstract. The full text of 25 potential studies were reviewed and 5 were excluded because they did not meet one or more of the inclusion criteria. A total of 20 studies were included in the meta-analysis. The inter-rater agreement for the selection process was calculated by dividing the number of agreements by the number of agreement sand disagreements multiplied by 100. The agreement for the study selection was 90%. The disagreement between the two authors was resolved by discussing the rationales behind including or excluding the potential studies.
Inclusion and Exclusion Criteria
The studies had to meet the following criteria to be included in the review: (a) applied single-case research design that demonstrated an experimental control (e.g., reversal, multiple baseline/probe, alternating treatment); (b) included participants between the ages of 0 and 8 years who were diagnosed with ASD (i.e., autism prototype disorder, childhood disintegrative disorder —CDD, pervasive developmental disabilities—not otherwise specified—PDD—NOS); (c) evaluated the effects of high-tech SGDs (i.e., tablet-based SGDs, Dynavox); and (d) targeted functional and/or social-communication skills (i.e., mand, tact, intraverbal) as the primary measure. Studies that were excluded from the review met at least one of the following criteria: (a) did not include empirical data that demonstrated an experimental control (e.g., review articles, narrative case reports, descriptive observations, case studies); (b) targeted skills other than communication (e.g., social, vocational, entertainment, discrimination training, listener response); (c) utilized low-tech SGDs (e.g., GoTalk, Tech/Talk); (d) did not include at least one participant with ASD; or (e) included participants older than 8 years old.
Data Extraction
The included studies were summarized in terms of (a) authors; (b) brief participant descriptions (i.e., number, gender, age range, diagnosis, previous exposure to high-tech SGDs); (c) setting/teaching format (i.e., discrete trial teaching —DTT, natural environment teaching —NET); (d) single-case design; (e) dependent measure (i.e., single and/or multistep augmentative verbal operants); (f) device/application; and (g) effectiveness (i.e., IRD, 95% confidence interval —CI). The second author checked the data extraction that was performed by the first author across all included studies to ensure accuracy. There were no disagreements on the extracted data.
The quality indicators suggested by Horner et al. (2005) were used to determine the quality of the included studies. These quality indicators related to (a) participants and settings, (b) dependent variable, (c) independent variable, (d) baseline, (e) experimental control/internal validity, (f) external validity, and (g) social validity. For a study to be considered as high quality, the following indicators had to be met: (a) an in-depth description of the participants and setting(s), (b) a reliable and repeated measurement of the primary measure, (c) valid systematic manipulations under the control of the experimenter and a thorough description of the intervention, (d) a sufficient description of baseline phase that allows replication, (e) a demonstration of a functional control, (f) a demonstration of external validity, and (g) a social validity measurement. The agreement between the two authors was 91% based on random selection and review of 32% of the included studies. The disagreement between the two authors was discussed.
Quality Appraisal
The two-step procedure developed by the NTACT (Test et al. 2009) was used to determine the level of evidence for using tablets as SGDs with children with ASD. The first step consisted of evaluating the quality of each study (i.e., high, acceptable) using the quality indictors suggested by Horner et al. (2005). For a study to be considered as high quality, the study had to meet all the quality indicators. For acceptable quality, the study had to meet all indicators—except for indicator 2 and/or 11—and at least one of indicators 17–21.
The second step entailed determining the level of evidence for using tablet-based SGDs based on the following: (a) the number of high or acceptable quality studies, (b) the number of research teams, (c) a demonstration of a functional relation, and (d) the nonexistence of contradictory empirical results from a study with strong evidence. For a practice to be established as having a strong level of evidence, the practice must have five high-quality studies that demonstrated a functional relation and were conducted by three independent research teams. In addition, the practice must have no contradictory data from a study with strong evidence. For a moderate level of evidence, the practice must have three high or acceptable quality studies that demonstrated a functional relation and were implemented by one or two independent research team. For a potential level of evidence, a practice must have two studies with high or acceptable quality that demonstrated a functional relation and were conducted by one or two independent research teams (Test et al. 2009).
Calculations of Effects Sizes
The magnitude of change in the dependent variable(s) was analyzed in each study. An IRD (Parker et al. 2009) was utilized to determine the difference between the data in baseline and intervention phases. There are numerous advantages to applying IRD to calculate the effect size of an intervention in comparison to other non-overlap methods (Parker et al. 2009). Some of these advantages include the simplicity of calculations, the easiness to include CIs, and the ability to complement visual analysis with quantitative value to measure the effectiveness of an intervention. Further, IRD does not need prerequisite distribution assumptions. IRD values range from 1.00 (the intervention has very strong or large effects on the dependent variable) to 0 (the intervention has no effect on the depended variable). Based on the interpretations of IRD values by Parker et al. (2009), IRD scores of .50 or lower indicate small effects, IRD scores of .50 and .70 indicate moderate effects, and IRD scores of .70 or .75 and higher indicate strong effects. In addition to IRD, 95% CI was calculated to determine the level of precision in the IRD values. Narrow CIs indicate more trustworthy and reliable calculated IRD values compared to wide range CIs (Harper 1999). For example, if the estimated IRD value is .93 with 95% CI (.78, 1.00), it means that the estimated IRD value is between .78 and 1.00 (narrow intervals). If, however, the estimated IRD value is .28 with 95% CI (0, .56), it means that the estimated value is between 0 and .56 (wider intervals).
The first author calculated the IRD with 95% CI for each included participant in the studies. There were two studies in which the IRD was not calculated due to cumulative data (Sigafoos et al. 2013) or the absence of baseline data (Gevarter et al. 2014). For the studies that compared between multiple AAC modalities, the IRD with 95% CI was only calculated on the high-tech SGD data to determine the effectiveness of the intervention. The second author recalculated the IRD with 95% CI on 32% of randomly selected studies to determine the inter-rater agreement for reliability purposes. The agreement between the two authors was 99%.
Results
Based on the inclusion criteria, a total of 20 studies were reviewed. The studies are summarized in Table 1 in terms of participants, settings, single-case designs, dependent measures, types of speech-generating device and application, and IRD.
Participants
Fifty-four participants (10 females, and 44 males) were included in the 20 reviewed studies. The age range of the participants was from 3 to 8 years (M = 5 years). The majority of the participants had a diagnosis of ASD (n = 42) only, or combined with a developmental disability (n = 12), such as childhood disintegrative disorder, Down syndrome, and intellectual disability.
The majority of the participants (n = 38) had not had any prior experience with high-tech SGDs. In four studies, the participants (n = 16) had a history of using high-tech SGDs, such as iPad or iPod Touch with AAC apps (Couper et al. 2014; Gevarter et al. 2016; Lorah and Parnell 2017; Waddington et al. 2014).
Participants in three studies engaged in challenging behaviors such as crying, self-injurious behaviors, and tantrums as means of communication (Achmadi et al. 2014; Agius and Vance 2016; Sigafoos et al. 2013). However, only Sigafoos et al.’s study included a measure to determine the effects of an SGD on children’s challenging behaviors.
Settings
Studies were conducted in several types of settings such as school, clinic, home, or a combination of two or more settings. Elven studies (55%) were conducted in a school (Dundon et al. 2013; Flores et al. 2012; King et al. 2014; Lorah et al. 2013; Lorah 2016; Lorah and Parnell 2017; McLay et al. 2015; Schlosser et al. 2007; Strasberger and Ferreri 2014 van der Meer et al. 2012b) or a childcare setting (van der Meer et al. 2012a). Out of these 11 studies, 6 (55%) were carried out in an isolated room (van der Meer et al. 2012a, b), or an isolated area in the participants’ classroom (Dundon et al. 2013; Lorah et al. 2013; McLay et al. 2015; Schlosser et al. 2007). In addition, four studies (20%) were conducted in a clinical room (Agius and Vance 2016; Lorah et al. 2014; Sigafoos et al. 2013; Waddington et al. 2014), and three (15%) were carried out in the homes of the participants (Gevarter et al. 2014, 2016; van der Meer et al. 2012c). Two studies (10%) were implemented in a combination of three settings; home, school, and clinic (Achmadi et al. 2014; Couper et al. 2014).
Training Formats
Intervention sessions in a total of 17 studies (85%) were conducted in a one-on-one DTT format (Achmadi et al. 2014; Agius and Vance 2016; Couper et al. 2014; Dundon et al. 2013; Gevarter et al. 2014, 2016; King et al. 2014; Lorah et al. 2013, 2014; McLay et al. 2015; Schlosser et al. 2007; Sigafoos et al. 2013; Strasberger and Ferreri 2014; van der Meer et al. 2012a, b, c; Waddington et al. 2014). In this format, the interventionist sat next to or across from the child and conducted training sessions in isolation from the regular home or classroom routine.
On the other hand, only three studies (15%) employed NET strategies. Training sessions were embedded in regular classroom routines such as snack time (Flores et al. 2012), play time, (Lorah 2016), and circle time (Lorah and Parnell 2017).
Types of SGDs and Applications
Most studies used devices such as an iPad, iPod, or mini iPad that operate on an iOS system. An iPad was used in a total of 12 studies (60%) whether alone (Agius and Vance 2016; Dundon et al. 2013; Flores et al. 2012; Gevarter et al. 2014, 2016; King et al. 2014; Lorah et al. 2013, 2014; Sigafoos et al. 2013; Waddington et al. 2014) or combined with other devices (Couper et al. 2014; van der Meer et al. 2012c). iPods or iPod Touch were used in six studies (30%) (Achmadi et al. 2014; Couper et al. 2014; Strasberger and Ferreri 2014; van der Meer et al. 2012a, b, c), and iPad mini was used in only three studies (15%) (Lorah 2016; Lorah and Parnell 2017; McLay et al. 2015). Another less common device was Vantage (Schlosser et al. 2007).
In terms of the applications used in the reviewed studies, Proloquo2Go was the most frequently used application which was examined in 14 studies (70%) (Achmadi et al. 2014; Couper et al. 2014; King et al. 2014; Lorah et al. 2013, 2014; Lorah 2016; Lorah and Parnell 2017; McLay et al. 2015; Sigafoos et al. 2013; Strasberger and Ferreri 2014; van der Meer et al. 2012a, b, c; Waddington et al. 2014), followed by GoTalk which was experimented in only three studies (15%) (Dundon et al. 2013; Gevarter et al. 2014, 2016). Other less commonly utilized applications were SoundingBoard (Agius and Vance 2016), My Choice Board (Dundon et al. 2013), Lexigrams (Schlosser et al. 2007), Pick-A-Word (Flores et al. 2012), and Scene and Heard (Gevarter et al. 2014).
Targeted Verbal Operants
The verbal operants targeted in the reviewed studies included manding, tacting, and intraverbal. Eighteen studies (90%) targeted manding in which the child had to request an item (e.g., toy) using vocalizations (e.g., Gevarter et al. 2016) or through touching a button on the SGD that generated a corresponding speech output for the desired item (e.g., Achmadi et al. 2014). Manding was taught based on Skinner’s analysis (1957) of verbal behavior: (a) the participant was presented with a preferred stimulus, (b) the preferred stimulus was taken away (i.e., establishing operation), (c) the participant responded by touching the corresponding button on the SGD (i.e., manding), and (d) the participant was given the preferred stimulus (e.g., contingent reinforcement).
Manding was measured in the reviewed studies either as a single step (e.g., Achmadi et al. 2014; Couper et al. 2014), or multistep (e.g., Flores et al. 2012; Waddington et al. 2014). In single-step manding, the child had to touch only one button that evoked a corresponding speech output (e.g., “car”) to get access to the requested item. In multistep manding, the child was required to request a preferred item in two or three steps using an SGD to get access to the requested item. The child would touch a button that evoked a corresponding speech output to a certain category (e.g., toys), and then touch another button to request a specific item (e.g., car) in that category (Flores et al. 2012). In one study, the child was also required to activate a button corresponding with “thank you” upon receiving the requested item (Waddington et al. 2014).
Only two studies targeted tacting in which the child labeled an object after being presented with one (e.g., train), and asked a question (e.g., “what do you see?”). Similar to manding, tacting occurred in the reviewed studies in a single step (Lorah and Parnell 2017) or multistep (Lorah et al. 2014). In single-step tacting, the child was presented with a stimulus, asked a question, and required to touch one button that generated a corresponding speech output to the stimulus (e.g., train) (Lorah and Parnell 2017). In multistep tacting, the child had to label the stimulus in two steps, for instance, (a) touching a button that evoked a corresponding speech output to “I see,” and then (b) touching a button that generated a corresponding speech output to “train” (Lorah et al. 2014).
In addition, only one study targeted intraverbals in addition to manding (Strasberger and Ferreri 2014). Children were taught to answer a question “what is your name?” using PECS Phase VI procedures.
Effects of High-Tech SGDs
The effect size of the intervention was calculated across 18 studies (see Table 2). The IRD scores for 13 studies (72%) out of 18 indicated that high-tech SGDs showed a strong effect on teaching verbal behaviors (Achmadi et al. 2014; Agius and Vance 2016; Couper et al. 2014; Dundon et al. 2013; Flores et al. 2012; King et al. 2014; Lorah et al. 2013, 2014, 2016; McLay et al. 2015; Strasberger and Ferreri 2014; van der Meer et al. 2012a, b). Further, IRD scores for four studies (22%) revealed that high-tech SGDs were moderately effective (Lorah and Parnell 2017; Schlosser et al. 2007; van der Meer et al. 2012c; Waddington et al. 2014). The average IRD value in one study (6%) was under .50 which indicated that high-tech SGDs had weak effects on vocalizations (Gevarter et al. 2016).
Quality Indicators and Level of Evidence
Out of the 20 studies, two (10%) met all the 21 quality indicators (see Table 3) of single-case design research described by Horner et al. (2005) (Flores et al. 2012; Strasberger and Ferreri 2014). A total of 13 studies (65%) met all the quality indicators from 1 to 17 and at least one of the quality indicators pertaining to social validity (Couper et al. 2014; Gevarter et al. 2016; King et al. 2014; Lorah et al. 2013, 2014; Lorah 2016; Lorah and Parnell 2017; McLay et al. 2015; Schlosser et al. 2007; Sigafoos et al. 2013; van der Meer et al. 2012a, b, c). Four studies (20%) failed to meet at least one quality indicator from 1 to 17 such as describing the physical setting (Agius and Vance 2016; Waddington et al. 2014) or the participants and the selection process with sufficient details that would allow replication (Dundon et al. 2013), collecting a minimum of three data points in the baseline phase or describing the baseline procedures with thorough details (Achmadi et al. 2014; Gevarter et al. 2014), failing to provide a demonstration of an experimental control (Dundon et al. 2013; Waddington et al. 2014) or demonstrating external validity (Dundon et al. 2013).
Based on the application of Horner et al.’s (2005) quality indicators, only two studies (10%) demonstrated a high level of quality (Flores et al. 2012; Strasberger and Ferreri 2014). These studies were considered high-quality because they met all the quality indicators. Sixteen studies (80%) were appraised as acceptable quality as they met all indicators—except for indicator 2 and/or 11 and at least one of indicators 17–21 (Achmadi et al. 2014; Couper et al. 2014; Gevarter et al. 2014, 2016; King et al. 2014; Lorah et al. 2013, 2014; Lorah 2016; Lorah and Parnell 2017; McLay et al. 2015; Schlosser et al. 2007; Sigafoos et al. 2013; van der Meer et al. 2012a, b, c). As described by Test et al. (2009), a moderate level of evidence is established by three studies with a high or acceptable level of quality that demonstrated a functional relation and were implemented by one or two independent research team. Per the evaluation of level of quality across all the reviewed studies, the use of high-tech SGDs to enhance the communication skills of children with ASD has been established as an evidence-based practice with a moderate level of evidence.
Discussion
The purpose of this systematic review was to meta-analyze single-case studies that utilized high-tech SGDs with children with ASD between the ages of 0 to 8 years. Based on IRD scores, high-tech SGDs are strongly effective to teach single-step manding, multistep manding, multistep tacting, and multistep intraverbal to children with ASD. The findings also show that high-tech SGDs as a communication intervention has moderate effects on single-step tacting and weak effects on vocal production in children with ASD.
Another purpose of this review was to evaluate the included studies based on Horner et al.'s (2005) quality indicators for single-case research and to determine the level of evidence for using high-tech SGDs with children with ASD. Only two studies reflected high quality (Flores et al. 2012; Strasberger and Ferreri 2014), whereas 16 studies reflected acceptable quality (Achmadi et al. 2014; Couper et al. 2014; Gevarter et al. 2014, 2016; King et al. 2014; Lorah et al. 2013, 2014; Lorah 2016; Lorah and Parnell 2017; McLay et al. 2015; Schlosser et al. 2007; Sigafoos et al. 2013; Strasberger and Ferreri 2014; van der Meer et al. 2012a, b, c). Based on the decision rules developed by Test et al. (2009), a moderate level of evidence was established for using high-tech SGDs as a communication intervention for children with ASD.
The findings of this review revealed the need for more high-tech SGD studies to be conducted within the natural routines of children with ASD. Only three studies were embedded in natural contexts (Flores et al. 2012; Lorah 2016; Lorah and Parnell 2017). Embedding high-tech SGD in a naturalistic context may facilitate the acquisition of the targeted communication skills and make these skills more meaningful to the child. Additionally, the current findings are consistent with Walker and Snell’s (2013) in that SGD interventions were mostly implemented by researchers. There remains a critical need to have teachers and caregivers serve as interventionists in high-tech SGD studies. This may help close the existing gap between research and practice.
Generalizing communication skills across settings or communicative partners was lacking in the reviewed studies. Only one study assessed generalization across settings (Strasberger and Ferreri 2014), and none assessed generalization across communicative partners (e.g., parents, teachers). This is consistent with the findings of Franco et al. (2009) in which they indicated the need for assessing generalization across communicative partners when examining SGDs as a communication tool.
Additionally, only three studies collected social validity data from stakeholders (Agius and Vance 2016; Flores et al. 2012; Strasberger and Ferreri 2014). Future research on high-tech SGD intervention should collect social validity data on the importance of the targeted skills, effectiveness and acceptability of intervention, and willingness to continue using the intervention after the termination of the study. To make data collection of social validly more feasible, stakeholders such as teachers and caregivers need to be involved in the intervention process so that they can rate their satisfaction with the intervention. It may be impossible for a parent, for instance, to rate an intervention if it was conducted in a clinical setting without his/her presence. This, again, magnifies the need for stakeholders as interventionists and/or communicative partners for generalization purposes.
Consistent with the findings of Lorah et al. (2014), most high-tech SGD studies were conducted to teach manding. The need still remains for future research to examine the effects of high-tech SGDs on other types of verbal behavior such as tact and intraverbal.
Teaching children with ASD to navigate the device, access the application, and then perform the targeted verbal behavior (e.g., tact) needs to be addressed in future research. Teaching children with ASD to perform a more complex sequence may enhance their independence skills as they would not need to rely on an adult to navigate the device/application.
As previous research indicated that the use of AAC, in general, is not likely to impede vocal production (Millar et al. 2006), there still is a clear need to examine whether the use of SGDs can, on the other hand, enhance the vocalizations in children with ASD. Out of 20 studies, only Gevarter et al.’s (2016) measured vocal production. Replications of Gevarter et al.’s study may provide additional data to support the use of high-tech SGDs to target vocal production in children with ASD.
Implications for Practice
High-tech SGDs may be a viable option for children with ASD with limited or no functional speech. These devices, tablets to be exact, are socially acceptable and portable. Additionally, Peluso (2012) indicated that tablets are commonly available in classrooms. In addition to these advantages, educators were highly satisfied with tablets as dedicated SGDs and were willing to continue to use it (Strasberger and Ferreri 2014). Thus, the use of high-tech SGDs may be feasible and practical to educators.
For successful results, educators may need to consider multiple variables related to the child. These may include the current level of fine motor skills, communication skills, and prior history with SGDs. For instance, children with more severe communication delays (Rispoli et al. 2010) or children who have no history with SGDs may need to start with a basic single-step functional communication (e.g., Gevarter et al. 2014) such as presenting only one picture of an item on the SGD screen to mand or tact an item.
This meta-analysis included and evaluated 20 studies. The findings of this review should be taken with caution as descriptions of the independent variables were not included. Additionally, the analysis did not take into consideration the differences in the intervention components used in the reviewed studies such as differential reinforcement, least-to-most promoting, or time delay. Thus, future meta-analyses should evaluate the use of high-tech SGDs with children with ASD based on intervention components.
References
Achmadi, D., Sigafoos, J., van der Meer, L., Sutherland, D., Lancioni, G. E., O’Reilly, M. F., … Marschik, P. B. (2014). Acquisition, preference, and follow-up data on the use of three AAC options by four boys with developmental disability/delay. Journal of Developmental and Physical Disabilities, 26(5), 565–583. https://doi.org/10.1007/s10882-014-9379-z.
Agius, M., & Vance, M. (2016). A comparison of PECS and iPad to teach requesting to preschoolers with autistic spectrum disorders. Augmentative and Alternative Communication, 32(1), 58–68. https://doi.org/10.3109/07434618.2015.1108363.
Alzrayer, N., Banda, D., & Koul, R. (2014). Use of iPad/iPods with individuals with autism and other developmental disabilities: A meta-analysis of communication interventions. Review Journal of Autism and Developmental Disorders, 1(3), 179–191. https://doi.org/10.1007/s40489-014-0018-5.
American Academy of Pediatrics. (2007). Management of children with autism spectrum disorder. Pediatrics, 120(5), 1162–1182. https://doi.org/10.1542/peds.2007-2362.
Baron-Cohen, S. (2004). Autism: Research into causes and intervention. Pediatric Rehabilitation, 7(2), 73–78.
Chiang, H. M. (2008). Expressive communication of children with autism: The use of challenging behaviour. Journal of Intellectual Disability Research, 52(11), 966–972. https://doi.org/10.1111/j.1365-2788.2008.01042.x.
Chung, M. C., Jenner, L., & Chamberlain, L. (1996). Communication skill and behaviour disorder. Perceptual and Motor Skills, 83(3), 1183–1186. https://doi.org/10.2466/pms.1996.83.3f.1183.
Couper, L., van der Meer, L., Schäfer, M. C. M., McKenzie, E., McLay, L., O'Reilly, M. F., … Sutherland, D. (2014). Comparing acquisition of and preference for manual signs, picture exchange, and speech-generating devices in nine children with autism spectrum disorder. Developmental Neurorehabilitation, 17(2), 99–109. https://doi.org/10.3109/17518423.2013.870244.
Division for Early Childhood. (n.d.) http://www.dec-sped.org/. Accessed 2 July 2017.
Dundon, M., McLaughlin, T., Neyman, J., & Clark, A. (2013). The effects of a model, lead, and test procedure to teach correct requesting using two apps on an iPad with a 5-year-old student with autism spectrum disorder. Educational Research International, 1(3), 1–10.
Flores, M., Musgrove, K., Renner, S., Hinton, V., Strozier, S., Franklin, S., & Hil, D. (2012). A comparison of communication using the Apple iPad and a picture-based system. Augmentative and Alternative Communication, 28(2), 74–84. https://doi.org/10.3109/07434618.2011.644579.
Franco, J. H., Lang, R. L., O’Reilly, M. F., Chang, J. M., Sigafoos, J., & Rispoli, M. (2009). Functional and treatment of inappropriate vocalizations using a speech-generating device for a child with autism. Focus on Autism and Other Developmental Disabilities, 24(3), 146–155.
Frea, W. D., Arnold, C. L., & Vittimberga, G. L. (2001). A demonstration of the effects of augmentative communication on the extreme aggressive behavior of a child with autism within an integrated preschool setting. Journal of Positive Behavior Interventions, 3(4), 194–198. https://doi.org/10.1177/109830070100300401.
Frost, L., & Bondy, A. (2002). Picture exchange communication system training manual (2nd ed.). Newark: Pyramid Education Products.
Ganz, J. B., Earles-Vollrath, T. L., Heath, A. K., Parker, R. I., Rispoli, M. J., & Duran, J. B. (2012). A meta-analysis of single case research studies on aided augmentative and alternative communication systems with individuals with autism spectrum disorders. Journal of Autism and Developmental Disorders, 42(1), 60–74. https://doi.org/10.1007/s10803-011-1212-2.
Gevarter, C., O’Reilly, M. F., Rojeski, L., Sammarco, N., Sigafoos, J., Lancioni, G. E., & Lang, R. (2014). Comparing acquisition of AAC-based mands in three young children with autism spectrum disorder using iPad applications with different display and design elements. Journal of Autism and Developmental Disorders, 44(10), 2464–2474. https://doi.org/10.1007/s10803-014-2115-9.
Gevarter, C., O’Reilly, M. F., Kuhn, M., Mills, K., Ferguson, R., Watkins, L., … Lancioni, G. E. (2016). Increasing the vocalizations of individuals with autism during intervention with a speech-generating device. Journal of Applied Behavior Analysis, 49(1), 17–33. https://doi.org/10.1002/jaba.270.
Harper, R. (1999). Reporting of precision of estimates for diagnostic accuracy: A review. British Medical Journal, 318(7194), 1322–1323.
Horner, R. H., Carr, E. G., Halle, J., McGee, G., Odom, S., & Wolery, M. (2005). The use of single-subject research to identify evidence-based practice in special education. Exceptional Children, 71(2), 165–179. https://doi.org/10.1177/001440290507100203.
Individuals with Disabilities Education Improvement Act Regulations, 34 C.F.R. § 300.35 et seq. (2004).
Kaiser, A. P., Cai, X., Hancock, T. B., & Foster, E. M. (2002). Teacher reported behavior problems and language delays in boy and girls enrolled in head start. Behavioral Disorders, 28(1), 23–39.
King, M. L., Takeguchi, K., Barry, S. E., Rehfeldt, R. A., Boyer, V. E., & Mathews, T. L. (2014). Evaluation of the iPad in the acquisition of requesting skills for children with autism spectrum disorder. Research in Autism Spectrum Disorders, 8(9), 1107–1120. https://doi.org/10.1016/j.rasd.2014.05.011.
Lorah, E. R. (2016). Evaluating the iPad mini as a speech-generating device in the acquisition of a discriminative mand repertoire for young children with autism. Focus on Autism and Other Developmental Disabilities. https://doi.org/10.1177/1088357616673624.
Lorah, E., & Parnell, A. (2017). Acquisition of tacting using a speech-generating device in group learning environments for preschoolers with autism. Journal of Developmental and Physical Disabilities, 29(4), 597–609. https://doi.org/10.1007/s10882-017-9543-3.
Lorah, E., Tincani, M., Dodge, J., Gilroy, S., Hickey, A., & Hantula, D. (2013). Evaluating picture exchange and the iPad™ as a speech generating device to teach communication to young children with autism. Journal of Developmental and Physical Disabilities, 25(6), 637–649. https://doi.org/10.1007/s10882-013-9337-1.
Lorah, E. R., Parnell, A., & Speight, D. R. (2014). Acquisition of sentence frame discrimination using the iPad as a speech-generating device in young children with developmental disabilities. Research in Autism Spectrum Disorders, 8(12), 1734–1740. https://doi.org/10.1016/j.rasd.2014.09.004.
Lorah, E. R., Parnell, A., Whitby, P. S., & Hantula, D. (2015). A systematic review of tablet computers and portable media players as speech generating devices for individuals with autism spectrum disorder. Journal of Autism and Developmental Disorders, 45(12), 3792–3804. https://doi.org/10.1007/s10803-014-2314-4.
Matson, J. L., Kozlowski, A. M., & Matson, M. M. (2012). Speech deficits in persons with autism: Etiology and symptom presentation. Research in Autism Spectrum Disorders, 6(2), 573–577.
McLay, L., Meer, L., Schäfer, M., Couper, L., McKenzie, E., O’Reilly, M., & … Sutherland, D. (2015). Comparing acquisition, generalization, maintenance, and preference across three AAC options in four children with autism spectrum disorder. Journal of Developmental and Physical Disabilities, 27(3), 323–339. https://doi.org/10.1007/s10882-014-9417-x.
Millar, D., Light, J. C., & Schlosser, R. W. (2006). The impact of augmentative and alternative communication intervention on the speech production of individuals with developmental disabilities: A research review. Journal of Speech, Language, and Hearing Research, 49(2), 248–264. https://doi.org/10.1044/1092-4388(2006/021).
Mirenda, P. (2003). Toward functional augmentative and alternative communication for students with autism manual signs, graphic symbols, and voice output communication aids. Language, Speech, and Hearing Services in Schools, 34(3), 203–216. https://doi.org/10.1044/0161-1461(2003/017).
No Child Left Behind Act. (NCLB). (2001). Pub. L. No. 107–110, 115 Stat. 1425. Retrieved July 29, 2017, from http://www.ed.gov/legislation/ESEA02.
Ogletree, B. T., & Oren, T. (2006). How to use augmentative and alternative communication. Austin: Pro-Ed.
Park, C. J., Yelland, G. W., Taffe, J. R., & Gray, K. M. (2012). Brief report: The relationship between language skills, adaptive behavior, and emotional and behavior problems in preschoolers with autism. Journal of Autism and Developmental Disorders, 42(12), 2761–2766. https://doi.org/10.1007/s10803-012-1534-8.
Parker, R. I., Vannest, K. J., & Brown, L. (2009). The improvement rate difference for single case research. Exceptional Children, 75(2), 135–150. https://doi.org/10.1177/001440290907500201.
Parker, R. I., Vannest, K. J., & Davis, J. L. (2011). Effect size in single-case research: A review of nine nonoverlap techniques. Behavior Modification, 35(4), 303–322. https://doi.org/10.1177/0145445511399147.
Peluso, D. (2012). The fast-paced iPad revolution: Can educators stay up to date and relevant about these ubiquitous devices? British Journal of Educational Technology, 43(4), 125–127. https://doi.org/10.1111/j.1467-8535.2012.01310.x.
Rispoli, M. J., Franco, J. H., van der Meer, L., Lang, R., & Camargo, S. P. H. (2010). The use of speech generating devices in communication interventions for individuals with developmental disabilities: A review of the literature. Developmental Neurorehabilitation, 13(4), 276–293. https://doi.org/10.3109/17518421003636794.
Schlosser, R. (2003). Roles of speech output in augmentative and alternative communication: Narrative review. Augmentative and Alternative Communication, 19(1), 5–27. https://doi.org/10.1080/0743461032000056450.
Schlosser, R. W., & Koul, R. K. (2015). Speech output technologies in interventions for individuals with autism spectrum disorders: A scoping review. Augmentative and Alternative Communication, 31(4), 285–309. https://doi.org/10.3109/07434618.2015.1063689.
Schlosser, R. W., & Wendt, O. (2008). Effects of augmentative and alternative communication intervention on speech production in children with autism: A systematic review. American Journal of Speech-Language Pathology, 17(3), 212–230. https://doi.org/10.1044/1058-0360(2008/021).
Schlosser, R. W., Sigafoos, J., Luiselli, J. K., Angermeier, K., Harasymowyz, U., Schooley, K., & Belfiore, P. J. (2007). Effects of synthetic speech output on requesting and natural speech production in children with autism: A preliminary study. Research in Autism Spectrum Disorders, 1(2), 139–163. https://doi.org/10.1016/j.rasd.2006.10.001.
Scruggs, T. E., & Mastropieri, M. A. (2001). How to summarize single-participant research: Ideas and applications. Exceptionality, 9(4), 227–244.
Scruggs, T. E., Mastropieri, M. A., & Casto, G. (1987). The quantitative synthesis of single subject research: Methodology and validation. Remedial and Special Education, 8(2), 24–33. https://doi.org/10.1177/074193258700800206.
Sigafoos, J., Lancioni, G. E., O’Reilly, M. F., Achmadi, D., Stevens, M., Roche, L., … Green, V. A. (2013). Teaching two boys with autism spectrum disorders to request the continuation of toy play using an iPad®-based speech-generating device. Research in Autism Spectrum Disorders, 7(8), 923–930. https://doi.org/10.1016/j.rasd.2013.04.002.
Skinner, B. F. (1957). Verbal behavior. Englewood Cliffs: Prentice Hall.
Strasberger, S. K., & Ferreri, S. J. (2014). The effects of peer assisted communication application training on the communicative and social behaviors of children with autism. Journal of Developmental and Physical Disabilities, 26(5), 513–526. https://doi.org/10.1007/s10882-013-9358-9.
Tager-Flusberg, H., & Kasari, C. (2013). Minimally verbal school-aged children with autism spectrum disorder: The neglected end of the spectrum. Autism Research, 6(6), 468–478. https://doi.org/10.1002/aur.1329.
Test, D. W., Fowler, C. H., Richter, S. M., White, J., Mazzotti, V, Walker, A. R., … & Kortering, L. (2009). Evidence based practices in secondary transition. Career Development for Exceptional Individuals, 32(2), 115–128. https://doi.org/10.1177/0885728809336859.
van der Meer, L., Didden, R., Sutherland, D., O'Reilly, M., Lancioni, G., & Sigafoos, J. (2012a). Comparing three augmentative and alternative communication modes for children with developmental disabilities. Journal of Developmental & Physical Disabilities, 24(5), 451–468. https://doi.org/10.1007/s10882-012-9283-3.
van der Meer, L., Kagohara, D., Achmadi, D., O'Reilly, M. F., Lancioni, G. E., Sutherland, D., & Sigafoos, J. (2012b). Speech-generating devices versus manual signing for children with developmental disabilities. Research in Developmental Disabilities, 33(5), 1658–1669. https://doi.org/10.1016/j.ridd.2012.04.004.
van der Meer, L., Sutherland, D., O’Reilly, M. F., Lancioni, G. E., & Sigafoos, J. (2012c). A further comparison of manual signing, picture exchange, and speech-generating devices as communication modes for children with autism spectrum disorders. Research in Autism Spectrum Disorders, 6(4), 1247–1257. https://doi.org/10.1016/j.rasd.2012.04.005.
Waddington, H., Sigafoos, J., Lancioni, G. E., O’Reilly, M. F., Van der Meer, L., Carnett, A., … Green, V. A. (2014). Three children with autism spectrum disorder learn to perform a three-step communication sequence using an iPad®-based speech-generating device. International Journal of Developmental Neuroscience, 39, 59–67. https://doi.org/10.1016/j.ijdevneu.2014.05.001.
Walker, V. L., & Snell, M. E. (2013). Effects of augmentative and alternative communication on challenging behavior: A meta-analysis. Augmentative and Alternative Communication, 29(2), 117–131. https://doi.org/10.3109/07434618.2013.785020.
Wendt, O. (2009). Research on the use of manual signs and graphic symbols in autism spectrum disorders: A systematic review. In P. Mirenda & T. Iacono (Eds.), Autism spectrum disorders and AAC (pp. 83–140). Baltimore: Paul H. Brookes Publishing Co..
Wodka, E. L., Mathy, P., & Kalb, L. (2013). Predictors of phrase and fluent speech in children with autism and severe language delay. Pediatrics, 131(4), e1128–e1134. https://doi.org/10.1542/peds.2012-2221.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Muharib, R., Alzrayer, N.M. The Use of High-Tech Speech-Generating Devices as an Evidence-Based Practice for Children with Autism Spectrum Disorders: A Meta-analysis. Rev J Autism Dev Disord 5, 43–57 (2018). https://doi.org/10.1007/s40489-017-0122-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40489-017-0122-4