
Abstract
The purpose of this review was to assess the effectiveness of tablet-based speech-generating devices (SGDs) in improving communication skills for individuals with autism spectrum disorder (ASD). A total of 31 single-case design intervention studies involving 84 individuals with ASD were reviewed and included in the analysis. We calculated Tau-U to evaluate the impact of interventions involving tablet-based SGDs on four different communication responses: specifically, mands, intraverbals, tacts, and vocalizations. To explore potential moderating variables for mand outcomes, we used the Kruskal–Wallis one-way test. The analysis revealed that interventions utilizing tablet-based SGDs led to improvements in communication responses. Specifically, large to very large changes were observed in mand and intraverbal responses, whereas moderate changes were noted in tact responses and vocalizations. The findings of this review underscore the potential of tablet-based SGDs in enhancing communication among individuals with ASD. We discuss the findings and provide implications for future research and practice.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental condition characterized by persistent limitations in social communication and interaction, as well as restricted and repetitive patterns of behavior, interests, or activities (American Psychiatric Association, 2013). Communication support needs are among the core characteristics of ASD and can have a profound impact on individuals' daily functioning and quality of life (Estes et al., 2011; Liptak et al., 2011; McNaughton et al., 2012). It has been estimated that about 30% of individuals with ASD may not have intelligible functional speech (Wodka et al., 2013) and, therefore, augmentative and alternative communication (AAC) may be necessary to promote communication. AAC is a set of tools used to supplement or replace speech for individuals with complex communication needs (Schlosser & Wendt, 2008). There are several types of AAC, including unaided AAC and aided AAC (Mirenda, 2003). Unaided AAC includes options that do not require equipment such as gestures and sign language, whereas aided AAC includes options that require equipment and can be classified as low-tech (e.g., picture exchange) and high-tech (e.g., speech-generating devices [SGDs]). SGDs are electronic devices that generate synthesized or digitized speech. Schlosser (2003) noted that SGDs can address different communication needs, such as making requests, naming items, and expressing opinions or answering questions. Skinner (1957) categorized these types of communicative actions as verbal operants, specifically mands, tacts, and intraverbals, respectively.
Recently, electronic tablets (e.g., Samsung, Apple iPads) have been used with communication applications (apps) as SGDs, allowing for a more portable and user-friendly option for individuals with ASD to access AAC (Lorah et al., 2022b). These devices have the added benefit of being highly customizable, providing users with the ability to personalize their communication systems and adapt to changing needs over time. Additionally, tablets are often less stigmatizing than traditional AAC devices, making them a more socially acceptable option for individuals with ASD to use in various settings (Lorah et al., 2022b). As such, the use of tablets and communication apps as SGDs has become increasingly popular in recent years and warrants further investigation through meta-analytic techniques.
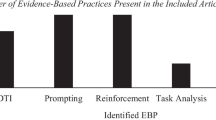
Recent meta-analyses and systematic literature reviews have shed light on the effectiveness of SGDs in supporting communication and language development for individuals with ASD. Tincani et al. (2020) conducted a systematic review of verbal operants in SGD research, focusing on research that utilized Skinner's (1957) analysis of verbal behavior. The authors analyzed 56 studies and found that SGDs were effective in increasing a variety of verbal operants, including mand, tact, and intraverbal responses, among individuals with ASD and other developmental disabilities. Another recent systematic review focused on the use of SGDs to support communication and language development for individuals with ASD (Lorah et al., 2022b). The authors reviewed 38 studies and found that SGDs were effective in improving communication outcomes of individuals with ASD. The authors also identified several evidence-based instructional practices that were incorporated into SGD-based interventions including prompts, discrete trial training, naturalistic teaching, peer-mediated instruction, and reinforcement. Although both systematic reviews provided valuable support for SGDs to promote the communication skills of individuals with ASD, neither review analyzed potential moderators that might influence the effectiveness of SGDs for individuals with ASD.
Similarly, Morin et al. (2018) conducted a systematic quality review of high-tech AAC interventions as an evidence-based practice across 23 studies. Although their review examined a range of SGDs for individuals with ASD and intellectual disability, the present meta-analysis aims to build on their work by focusing on up-to-date tablet-based SGDs for individuals with ASD specifically. Additionally, although Morin et al. focused on the quality of studies, the present meta-analysis also examines the outcomes of tablet-based SGDs across specific verbal operants of individuals with ASD, as well as potential moderators of these outcomes. By specifically examining the effectiveness of interventions utilizing tablet-based SGDs, this meta-analysis provides a more targeted and focused approach to evaluating the use of tablet-based SGDs in the context of supporting the communication needs of individuals with ASD.
Muharib and Alzrayer (2018) conducted a meta-analysis specifically focused on the use of high-tech SGDs as an evidence-based practice for children with ASD ages 0 to 8 years. Although their review examined the overall effectiveness of high-tech SGDs on communication outcomes, the present meta-analysis aims to expand on their work by examining the specific effects of interventions involving up-to-date tablet-based SGD on different verbal operants (i.e., mands, tacts, intraverbals) as well as vocalizations and potential moderators of the effects of tablet-based SGD interventions for individuals with ASD without age restrictions.
Recent systematic literature reviews and meta-analyses have provided valuable insights into the effectiveness of SGDs in supporting communication and language development for individuals with ASD. However, there is still a need for a comprehensive meta-analysis that focuses specifically on the use of tablet-based SGDs to increase verbal operants for individuals with ASD. Previous literature reviews (Lorah et al., 2022b; Morin et al., 2018; Muharib & Alzrayer, 2018; Tincani et al., 2020) provided valuable contributions to the literature, but their focus on broader areas of AAC technology (including outdated technology) or diagnosis (ASD, intellectual disability, developmental delay), and the lack of analyses of potential moderators suggest that a more focused examination of tablet-based SGDs is needed.
Thus, this meta-analysis aims to fill this gap by systematically reviewing the literature on the use of tablet-based SGDs to increase the communication skills of individuals with ASD. In the meta-analysis, we examined the characteristics of studies using up-to-date tablet-based SGDs to increase communication, the quality of these studies, and the overall estimated effects of these interventions on communication outcomes of individuals with ASD. Additionally, the meta-analysis explored potential moderators of these estimated effects, such as age, diagnosis, communication levels, prior experience with SGDs, setting, interventionist, and context. By synthesizing the available literature on SGD interventions for individuals with ASD, this meta-analysis contributes to a better understanding of the potential benefits of tablet-based SGDs in supporting communication and language development for individuals with ASD. Specific research questions included:
-
(a)
What are the characteristics of studies using tablet-based SGDs to increase mand, tact, and intraverbal responses and vocalizations of individuals with ASD?
-
(b)
What is the quality of studies involving the use of tablet-based SGDs for individuals with ASD based on the CEC (2014) standards?
-
(c)
What are the overall estimated effects of tablet-based SGDs on mand, tact, and intraverbal responses and vocalizations of individuals with ASD?
-
(d)
Do age, diagnosis, communication levels, prior experience with SGD, setting, interventionist, and context moderate the effects of tablet-based SGDs on mand, tact, and intraverbal responses and vocalizations of individuals with ASD?
Method
Search Procedure
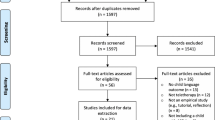
We searched EBSCO, PsycInfo, ERIC, MedLine, and ProQuest Dissertations and Theses Global to locate studies that incorporated the use of an SGD using the following three categories of search terms: (a) SGD (keywords: speech-generating device, SGD, AAC, augmentative and alternative communication, iPad, tablet, high-tech), (b) autism (keywords: autis* OR ASD), and (c) verbal behavior (keywords: mand*, fill-in, tact*, intraverbal, verbal behavior, verbal operant, request, label, comment, answer question). The searches were restricted to studies published since 2010 in English. We restricted the publication date because iPads were released in 2010 for the first time (Tincani et al., 2020) and to focus only on devices that are up to date. It is important to note that we did not limit the searches to iPads; however, because iPads were the first tablets introduced in the market, we restricted the search to 2010 up to the present date. We searched published and unpublished studies (e.g., dissertations) to reduce the threat of publication bias. We completed additional searches by (a) reviewing the reference lists of six recently published literature reviews on SGDs (i.e., Logan et al., 2022; Lorah et al., 2022a, 2022b, 2022c; Morin et al., 2018; Tincani et al., 2020) and (b) reviewing the reference lists of all included studies identified via the online database search. Searches concluded in February of 2023 and resulted in a total of 5410 articles (5405 from online database searches and five from ancillary searches) after removing duplicates. See Fig. 1 for a flowchart.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) summary of article extraction process
Inclusion and Exclusion Criteria
We evaluated each study against the following inclusion criteria: (a) included at least one participant with ASD; (b) was an experimental study (single-case research designs or experimental group designs); (c) involved teaching individuals with ASD to use a tablet-based SGD to mand, tact, or engage in an intraverbal response; (d) involved an SGD that was a touchscreen tablet (e.g., iPad, Samsung) and was not outdated (i.e., not available on the market as a new product such as iPods); and (e) involved behavioral interventions that were intended to promote communication via SGD.
We excluded studies from the review when they met at least one of the following exclusion criteria: (a) none of the participants had a diagnosis of ASD, (b) was not an experimental study, (c) an SGD was outdated (e.g., iPod) or not indicated, (d) the dependent variable combined multiple communication skills in one dependent variable (e.g., communicative acts that included mands, comments, head nods, gestures) because this would not allow for categorizing the dependent variable under one specific verbal operant (however, if a study included more than one verbal operant but each was its own dependent variable [e.g,. requesting preferred items, tacting, answering personal questions], then the study was included), and (e) when the study involved a tablet-based SGD but the intervention was programmed to decrease SGD use and increase vocalizations only (e.g., Muharib et al., 2021a). Although this is may be the ultimate goal for some individuals with ASD (i.e., transitioning from SGD use to vocal communication), we excluded these studies because our primary aim was to determine the effects of SGDs and behavioral strategies that were intended to increase SGD-based communication. We reviewed the abstracts of the 5410 studies to identify those that were not intervention-based (e.g., literature reviews) or not relevant to the current study (e.g., studies on different topics). This led to the exclusion of 5278 studies. We then accessed the full text of the remaining 132 studies to evaluate against our inclusion criteria. This resulted in 40 potentially relevant studies.
Next, we evaluated the experimental control of each of the 40 studies. Because common published quality evaluation tools (e.g., Council for Exceptional Children [CEC], 2014; Horner et al., 2005; Kratochwill et al., 2013) emphasize the importance of establishing experimental control, we only included studies that attempted to demonstrate experimental control in our analyses. Because all 40 studies used a single-case design, a study had to show at least three attempts to show an intervention effect. Thus, we excluded studies that used a multiple baseline design (or variations thereof) with fewer than three tiers (e.g., a multiple baseline across two participants). If a study used an alternating treatment design, then the study had to show some separation in the data paths to show experimental control. After evaluating the 40 studies, we excluded nine studies for not demonstrating experimental control (see Fig. 1 for a flow chart).
Data Extraction and Coding
We extracted descriptive information across each of the 84 participants represented in the 31 included studies in terms of (a) participant characteristics (i.e., age, sex, race/ethnicity, diagnosis, reported severity of ASD, communication level, prior experience with SGD); (b) settings (i.e., clinic, home, school); (c) interventionists (i.e., researcher, practitioner, parent); (d) components of the behavioral intervention (e.g., reinforcement, prompts) and context (i.e., discrete trial training [DTT] or naturalistic); (e) primary verbal operant addressed through SGD-based intervention (i.e., mand, tact, interverbal) and vocalizations if applicable; (f) the communication app in the device (e.g., Proloqu2Go, GoTalk Now); and (g) whether social validity, generalization, or maintenance were collected for each participant. We coded data using “1” to indicate the variable was relevant to the participant or “0” to indicate the variable was not relevant to the participant. When a study did not clearly provide specific information regarding those variables (e.g., communication level, severity of ASD), we coded the variable as “cannot determine.” In addition to coding those aforementioned variables, we descriptively extracted information from each article about the research design used (e.g., multiple baseline across behaviors, multiple probe across participants) and types of preference assessments completed if applicable (e.g., reports, multiple stimulus without replacement, paired choice).
Participant characteristics For the age group variable, we coded each participant as early childhood (younger than 5 years old), middle childhood (5–12 years old), adolescence (13–17 years old), and adulthood (18 years old and older). For the sex variable, we coded each participant as a male or female based on what was reported in the original study. For the race/ethnicity variable, we coded each participant as White, Black, Latino, Mixed race, Asian, Pacific, Native American, or not reported. For the diagnosis variable, we coded each participant as diagnosed with ASD only (e.g., autism, autistic disorder, pervasive developmental disorder not otherwise specified) or ASD + . This reflects participants that had a diagnosis of ASD and another diagnosis such as intellectual disability, speech impairment, or hearing impairment. For the severity of ASD, we coded each participant as mild, moderate, or severe based on what was reported in the original study. For the communication level variable, we coded each participant as communicating using prelinguistic behaviors (e.g., pointing, leading an adult), one-word utterances (vocally or using the SGD), or full sentences (vocally or using SGD; Muharib et al., 2021b). For the prior experience with SGD, we coded each participant as (a) a user if they were current users of an SGD or had an experience with an SGD prior to being a participant in the original study or (b) new to SGD if they never had an experience with any SGD.
Settings We coded three variables related to settings. For settings, we coded whether a participant received the intervention in a clinic, school, or home setting.
Interventionists For interventionists, we coded whether the intervention was delivered by a researcher, parent, or practitioner. A practitioner was considered someone already working with the participant and who was not part of the research team (e.g., behavioral therapist, speech-language pathologist, teacher, paraprofessional).
Components of the intervention and context We coded five variables related to the components of the intervention. These were the use of prompts, prompt delay, reinforcement, behavior chain interruption strategy, and backward chaining. Under each variable, we coded whether it was part of the behavioral intervention for each participant. For the intervention context, we coded whether the intervention was delivered in a DTT format or was embedded in naturally occurring activities for each participant.
Primary verbal operant We coded each participant’s primary verbal operant addressed through the SGD-based intervention (i.e., mand, tact, intraverbal). For the majority of participants, verbal operants were multiply controlled. For example, when a participant responds “I want an apple” after a practitioner asks “what do you want?” and the apple is present, the verbal operant is controlled by an establishing operation (assuming the participant was deprived of food), a non-verbal stimulus (the apple), and a verbal stimulus (what do you want?). However, the primary verbal operant in this case is a mand. In addition to primary SGD-based verbal operants, we also coded whether data on vocalizations were collected. This was to determine whether the use of SGD could increase or decrease vocalizations of individuals with ASD.
Communication app in the device We coded the communication app that was used by each participant. Examples included Proloqu2Go, GoTalk Now, and LAMP.
Social validity, generalization, and maintenance We coded whether social validity data were gathered. Additionally, we coded whether generalization or maintenance were collected and graphed.
CEC Standards
Because all included studies used a single-case design, we only applied the CEC (2014) quality indicators applicable to single-case design studies. Thus, we evaluated each study against 22 quality indicators under eight categories (i.e., context and setting, participants, intervention agent, description of practice, implementation fidelity, internal validity, dependent variable, visual analysis).
Interrater Reliability
The third author served as a secondary coder for interrater reliability (IRR) purposes. Training the third author entailed oral and written explicit operational definitions of the inclusion criteria, coding variables, CEC quality indicators as well as examples and non-examples for each of the aforementioned items. We calculated IRR item-by-item and divided the number of agreements by the number of agreements plus disagreement and multiplied by 100 to obtain a percentage of agreement.
Inclusion of the studies The first author assigned 40 randomly selected studies of the 132 full texts (30.3%) to the third author. The IRR result for the inclusion of the studies was 100%.
Data Extraction and coding The first author assigned 31 randomly selected participants (36.9%) for data coding to the third author. The IRR result for data coding was 100%.
CEC quality indicators The first author assigned 10 randomly selected articles (32.2%) for CEC quality indicators to the third author. The IRR result for data coding was 100%.
Intervention Effect Estimation and Moderator Analyses
We examined the effect of interventions involving tablet-based SGDs on communication outcomes of individuals with ASD and whether certain variables moderated these outcomes. To estimate intervention effect, we calculated Tau-U (Parker et al., 2011) for each participant across communication measures (i.e., SGD-based mands, tacts, and intraverbals, vocalizations). Tau-U is a nonoverlap index that takes into account undesirable trends in baseline and has outperformed other nonoverlap indices for estimating intervention effect in single-case research contexts (Parker et al., 2011). Tau-U can be interpreted in the following way: < 0.20: small change, 0.20–0.60: moderate change, 0.60–0.80: large change, and > 0.80: large to very large change (Vannest et al., 2016). To calculate Tau-U, we initially extracted numerical values from graphic displays of participant data using WebPlotDigitizer (Rohatgii, 2018). Once numerical data values were obtained, we calculated Tau-U using a free online Tau-U calculator (Vannest et al., 2016). During this process, we corrected for baseline when monotonic trends were present, contrasted baseline and intervention data (n = 99 for mands, n = 25 for tacts, n = 46 for intraverbals, n = 11 for vocalizations), selected weighted Tau-U outcomes to account for complex research designs (Parker et al., 2011), and combined these weighted Tau-U outcomes to provide aggregated Tau-U data for each participant and communication measure.
To explore whether certain variables moderated intervention outcomes, we conducted nonparametric moderator analyses across variables with eight or more cases (Walker & Snell, 2013). As such, we only were able to conduct moderator analyses for mand outcome measures across the following variables: age (early childhood and middle childhood), diagnosis (ASD and ASD +), communication levels (prelinguistic and one word), prior experience with SGD (current user and new user), setting (clinic and school), interventionist (researcher and practitioner), and context (DTT format and embedded). Using SPSS 28.0 for Mac, we applied the Kruskal–Wallis one-way analysis of variance test to determine whether significant differences existed for eligible variables based on Tau-U.
Results
Descriptive Findings
Descriptive findings of study characteristics are presented in Tables 1 and 2. In this analysis, 84 participants were included in the 31 studies. Of the 84 participants, 84.5% had an ASD diagnosis only whereas 15.5% had a secondary diagnosis in addition to ASD. Race and severity of ASD symptoms were not reported for the majority of participants (67.8% and 71.4%, respectively). A total of 72.6% were male and 27.4% were female. Participants mostly fell in the early childhood (40.4%) or middle childhood (52.3%) categories. Participants primarily communicated using prelinguistic means of communication (e.g., leading an adult, pointing; 35.7%) or used one-word communication (using an SGD or vocally; 47.6%). More participants were new to using the SGD (63%) compared to participants who had some experience using an SGD (37%). In terms of settings, the intervention was mainly implemented in school environments (69%) or a clinic (27%). The intervention was primarily implemented by a researcher (71%). In terms of the primary verbal operant targeted, manding was taught for the majority of participants (84.5%). Vocalizations were only measured and secondarily targeted for 12% of participants. All participants received reinforcement (specific reinforcement for manding, and generalized reinforcement for tacting and intraverbal) as part of the behavioral intervention. In addition, for most participants, the intervention also included prompts (95%) and prompt delay (90%). Behavior chain interruption strategy was used for teaching 19% of participants to mand for missing items. Backward chaining was used to increase the complexity of a verbal response for 9.5% of participants. A total of 70% of participants received the intervention in a DTT context whereas 30% of participants received the intervention in a naturalistic context. Most participants (79.7%) used Proloqu2Go as the communication app on their devices. Finally, social validity, generalization, and maintenance were collected for only some participants (20%, 44%, 12%, respectively).
CEC Standards
Overall, all studies met most or all quality indicators under the following six categories: setting, description of practice, implementation fidelity, internal validity, dependent variable, and visual analysis. However, 17 studies did not report how a diagnosis was determined, 11 studies did not report background information about the intervention agent, and 21 studies did not report information about the nature of training (or amount of training) received by the intervention agent (see the supplemental table).
Tau-U and Moderator Analyses
Overall, intervention effect estimates across communication measures reflected moderate to very large changes in participant outcomes according to the interpretation guidelines described by Vannest et al. (2016). Table 3 provides a summary of Tau-U results. Specifically, mand outcomes (Tau-U = 0.92, p < 001, 95% CI [0.85, 0.98], SD = 0.13, range 0.39–1.00) and intraverbal outcomes (Tau-U = 0.81, p < 001, 95% CI [0.71, 0.90], SD = 0.35, range – 0.13 to 1.0) reflected overall large to very large changes, whereas tact outcomes (Tau-U = 0.60, p < 001, 95% CI [0.49, 0.72], SD = 0.29, range 0.07–1.00) and vocalizations outcomes (Tau-U = 0.77, p < 001, 95% CI = [0.63, 0.94], SD = 0.28, range 0.15–1.00) reflected overall moderate changes. Results of the moderate analyses indicated that none of eligible variables moderated intervention effectiveness in relation to mand outcomes.
Discussion
In this review, we summarized and meta-analyzed data for 84 participants with ASD across 31 studies that included tablet-based SGDs to increase the communication of individuals with ASD. Overall, our findings are consistent with previous reviews that found SGDs to be effective at increasing the communication of individuals with ASD (e.g., Morin et al., 2018; Muharib & Alzrayer, 2018; Tincani et al., 2020).
Specifically, findings from the current meta-analysis reveal a pattern of outcomes that highlights the nuanced effectiveness of tablet-based SGDs. One key finding is that interventions involving tablet-based SGDs resulted in large to very large changes in mand and intraverbal responses and moderate changes in tact responses and vocalizations. A noteworthy observation from our review pertains to the prominence of mands as the most targeted verbal operant among participants with ASD (n = 71), which is consistent with previous reviews (e.g., Muharib & Alzrayer, 2018; Tincani et al., 2020). One reason for the pronounced outcomes for mands is that mands are the only verbal operant that results in attainment of a specific reinforcer (e.g., a child asks for candy, the child receives candy). Thus, a child may be more motivated to engage in a mand to acquire a specific reinforcer than to tact an object or a picture. Intriguingly, our study found interventions involving tablet-based SGDs resulted in greater change in intraverbal responses compared to tact responses, despite participants often lacking prior experience with SGDs for either operant; notably, although both tacts and intraverbals yield social or arbitrary reinforcement (e.g., praise) and intraverbals represent a higher-level verbal operant, the outcomes for intraverbals were more pronounced.
In addition, we conducted analyses to determine whether certain variables moderated the estimated effectiveness of interventions involving tablet-based SGDs. Our results show that there are no statistically significant differences in any of these variables for mand outcomes, which suggests that tablet-based SGDs can be effective in promoting mand responses for individuals with ASD regardless of these participant and study characteristics. Furthermore, our descriptive analysis sheds light on the uneven distribution of studies across various demographic and methodological dimensions. Notably, the majority of participants were male, diagnosed solely with ASD, and situated within the childhood age range. In contrast, a mere 27.4% represented females, while only 15.5% exhibited an additional diagnosis alongside ASD, and 7% were beyond the childhood phase. Similarly, our findings highlight a prevalent trend wherein interventions were predominantly implemented by researchers, constituting 71% of the cases, and often following a DTT format (70%). This underscores the need for more studies conducted by practitioners and parents and within the natural routine of the individuals with ASD (Ganz et al., 2019).
Finally, we assessed the extent to which the included studies adhered to the CEC (2014) quality indicators. Notably, although the majority of indicators were met, a recurrent shortfall pertained to the lack of detailing pertaining to training procedures and required training duration for successful intervention implementation. This trend potentially arises from the substantial involvement of researchers as intervention implementers for most participants (71.4%).
Limitations and Directions for Future Research
There are a few limitations that should be considered when interpreting findings from this review. First, as noted previously, we were unable to conduct moderator analyses for tact, interverbal, and vocalization outcomes due to an insufficient number of cases across all categories. Likewise, moderator analyses were not possible for specific categories under mand outcomes (e.g., adolescent and adult variables, home setting variable). To inform best practices in supporting the communication needs of individuals with ASD through tablet-based SGDs, it will be important to examine for whom and under which conditions these communication supports are effective. The limited number of cases representing certain communication measures and participant and study characteristics underscores the urgent need for additional research to build the literature base, thus permitting future examination of potential moderators. Second and related to the first limitation, although our findings suggest that interventions involving tablet-based SGDs produce moderate to very large changes in outcomes for individuals with ASD, is it possible that participant and study characteristics beyond those reported in this review may have moderated intervention outcomes. For example, due to insufficient information in the included studies, we did not code for participants’ motor abilities, unique features or settings used to navigate apps, or interventionists’ prior experience and training. These additional characteristics should be considered in future systematic literature reviews.
Our findings also revealed significant gaps in the literature base that should be addressed in future research. Of particular note were the limited number of cases involving individuals falling under the adolescent and adult categories, practitioner- and parent-implemented interventions, and implementation in natural contexts. We also found that a majority of cases focused on mand outcomes and few studies included measures of social validity, generalization and maintenance. To advance research and practice to support the communication needs of individuals with ASD, researchers will need to explore how tablet-based SGDs can be used in natural environments (e.g., inclusive school settings, community settings, home) by natural implementers (e.g., peers, teachers, family members) across all age groups as well as effective strategies for promoting skill generalization and maintenance with intentional assessment of social validity from the perspective of those supporting individuals with ASD and those who receive such support (Horner et al., 2005; Reichow et al., 2011).
In addition, our findings show a lack of race and ethnicity reporting in research related to tablet-based SGDs. Without data on the racial and ethnic backgrounds of participants in SGD studies, it becomes challenging to ensure that the benefits and outcomes of SGD interventions are universally applicable. Cultural sensitivity is vital in providing effective communication support for individuals with diverse backgrounds, including those from different racial and ethnic groups (Battaglia, 2017). For example, a parent of a child with ASD may prefer her child to communicate using their home language over English or in both languages using an SGD. Researchers should report and incorporate participants' racial and ethnic backgrounds in SGD interventions to meet the specific needs and cultural contexts of individuals with ASD.
Implications for Practice
Our findings suggest that interventions involving tablet-based SGDs are effective in enhancing the communication skills of individuals with ASD. Therefore, we encourage practitioners and caregivers to consider the use of these devices, particularly given the evidence presented in this review and the potential advantages, such as cost-effectiveness, portability, and social acceptability (Lorah, Holyfield, Griffen, et al., 2022). However, as with any decision related to planned support, it is imperative to conduct a thorough assessment, including the social validity from the perspective of the AAC user, to determine whether a tablet-based SGD option is suitable. Assessments might include considerations related to motor skills (e.g., ability to point, grasp, type, swipe), discrimination skills (e.g., ability to identify real objects and pictures), hearing and vision needs, and the durability of the device. It is also important to consider the individual’s communication preference and availability of adult training and support (Alzrayer & Banda, 2017; Beukelman & Light, 2019). Ultimately, the specific communication needs and abilities of the individual should serve as the guiding principles in the decision-making process. By thoroughly assessing these factors, practitioners and caregivers can make informed choices regarding the suitability of a tablet-based SGD as a communication support option.
Although there were limited cases across certain variables, evidence from this review suggests that SGDs can be effective across different settings, implementers, and contexts. It is essential to stress the importance of fostering communication in natural contexts, as this may facilitate skill generalization (Ganz et al., 2019). To ensure that individuals with ASD have ample opportunities to use SGDs across various settings and people, it is imperative to establish collaborative teaming among teachers, related services providers (e.g., speech-language pathologists, occupational therapists), and caregivers. Collaborative teaming plays a vital role in embedding communication opportunities within the natural routines and activities of individuals with ASD throughout the day. Moreover, it may assist in determining the most effective approaches for providing training to the adults involved in the individual's life. For example, teams can collaboratively decide whether and how training will occur (e.g., live coaching, telehealth support) and by whom to ensure those involved in supporting the communication and language development for individuals with ASD have the resources and knowledge necessary to do so. Adult training may include aspects such as how to program the SGD app to include a certain number of icons (based on the individual’s preferences and their ability to discriminate between icons), how to select specific communication goals, and how to use prompts and prompt fading strategies (e.g., least to most, most to least). Although the studies lacked information on the racial and ethnic backgrounds of participants, it is essential to tailor SGD interventions to the specific needs of individuals with ASD, ensuring that the interventions align with the cultural values and contexts of these individuals (Battaglia, 2017).
In conclusion, findings from this study suggest the efficacy of tablet-based SGDs in advancing the communication skills of individuals with ASD and highlights their estimated effects across distinct verbal operants and vocalizations. Furthermore, our findings underscore the need for more studies in certain underexplored areas.
References
Alzrayer, N. M., & Banda, D. R. (2017). Implementing tablet-based devices to improve communication skills of students with autism. Intervention in School and Clinic, 53(1), 50–57.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (DSM-5®). American Psychiatric Publications.
Battaglia, D. (2017). Functional communication training in children with autism spectrum disorder. Young Exceptional Children, 20, 30–40.
Beukelman, D. R., & Light, J. C. (2019). Augmentative and alternative communication: Supporting children and adults with complex communication needs (5th ed.). Brookes Publishing.
Council for Exceptional Children. (2014). Council for exceptional children standards for evidence-based practices in special education. Retrieved from https://www.cec.sped.org/~/media/Files/Standards/Evidence%20based%20Practices%20and%20Practice/EBP%20FINAL.pdf
Estes, A., Rivera, V., Bryan, M., Cali, P., & Dawson, G. (2011). Discrepancies between academic achievement and intellectual ability in higher-functioning school-aged children with autism spectrum disorder. Journal of Autism and Developmental Disorders, 41, 1044–1052. https://doi.org/10.1007/s10803-010-1127-3
Ganz, J. B., Hong, E. R., Leuthold, E., & Yllades, V. (2019). Naturalistic augmentative and alternative communication instruction for practitioners and individuals with autism. Intervention in School and Clinic, 55(1), 58–64. https://doi.org/10.1177/1053451219833012
Horner, R. H., Carr, E. G., Halle, J., McGee, G., Odom, S., & Wolery, M. (2005). The use of single-subject research to identify evidence-based practice in special education. Exceptional Children, 71(2), 165–179. https://doi.org/10.1177/001440290507100203
Kratochwill, T. R., Hitchcock, J. H., Horner, R. H., Levin, J. R., Odom, S. L., Rindskopf, D. M., et al. (2013). Single-case intervention research design standards. Remedial and Special Education, 34, 26–38.
Liptak, G. S., Kennedy, J. A., & Dosa, N. P. (2011). Social participation in a nationally representative sample of older youth and young adults with autism. Journal of Developmental and Behavioral Pediatrics, 32, 277–283. https://doi.org/10.1097/DBP.0b013e31820b49fc
Logan, K., Iacono, T., & Trembath, D. (2022). A systematic search and appraisal of intervention characteristics used to develop varied communication functions in children with autism who use aided AAC. Research in Autism Spectrum Disorders, 90, 101896. https://doi.org/10.1016/j.rasd.2021.101896
Lorah, E. R., Chatham, C., & Taylor, K. N. (2022a). A systematic review of evidence-based instruction for individuals with autism using mobile augmentative and alternative communication technology. Augmentative and Alternative Communication, 38(1), 22–33. https://doi.org/10.1080/07434618.2021.1955858
Lorah, E. R., Holyfield, C., Griffen, B., & Caldwell, N. (2022b). A systematic review of evidence-based instruction for individuals with autism using mobile augmentative and alternative communication technology. Review Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s40489-022-00334-6
Lorah, E. R., Holyfield, C., Miller, J., Griffen, B., & Lindbloom, C. (2022c). A systematic review of research comparing mobile technology speech-generating devices to other AAC modes with individuals with autism spectrum disorder. Journal of Developmental and Physical Disabilities, 4, 187–210. https://doi.org/10.1007/s10882-021-09803-y
McNaughton, D., Bryen, D., Blackstone, S., Williams, M., & Kennedy, P. (2012). Young adults with complex communication needs: Research and development in AAC for a “diverse” population. Assistive Technology, 24, 45–53. https://doi.org/10.1080/10400435.2011.648715
Mirenda, P. (2003). Toward functional augmentative and alternative communication for students with autism manual signs, graphic symbols, and voice output communication aids. Language, Speech, and Hearing Services in Schools, 34(3), 203–216. https://doi.org/10.1044/0161-1461(2003/017)
Morin, K. L., Ganz, J. B., Gregori, E. V., Foster, M. J., Gerow, S. L., Genc-Tosune, D., & Hong, E. R. (2018). A systematic quality review of high-tech AAC interventions as an evidence-based practice. Augmentative and Alternative Communication, 34(2), 104–117. https://doi.org/10.1080/07434618.2018.1458900
Muharib, R., & Alzrayer, N. M. (2018). The use of high-tech speech-generating devices as an evidence-based practice for children with autism spectrum disorders: A meta-analysis. Review Journal of Autism & Developmental Disorders, 5, 43–57.
Muharib, R., Lang, R., Walker, V. L., Phinney, A., & Rodriguez, M. (2021a). An evaluation of reinforcer magnitude and echoic prompts on vocal requesting of individuals with autism spectrum disorder. Journal of Developmental and Physical Disabilities, 33(6), 947–961.
Muharib, R., Walker, V. L., Alresheed, F., & Gerow, S. (2021b). Effects of multiple schedules of reinforcement on appropriate communication and challenging behaviors: A meta-analysis. Journal of Autism and Developmental Disorders, 51(3), 613–631. https://doi.org/10.1007/s10803-020-04569-2
Parker, R. I., Vannest, K. J., & Davis, J. L. (2011). Effect size in single-case research: A review of nine overlap techniques. Behavior Modification, 35, 303–322.
Reichow, B., et al. (2011). Development, procedures, and application of the evaluative method for determining evidence-based practices in autism. In B. Reichow (Ed.), Evidence-based practices and treatments for children with autism (pp. 25–39). Springer.
Schlosser, R. (2003). Roles of speech output in augmentative and alternative communication: Narrative review. Augmentative and Alternative Communication, 19(1), 5–27. https://doi.org/10.1080/0743461032000056450
Schlosser, R. W., & Wendt, O. (2008). Effects of augmentative and alternative communication intervention on speech production in children with autism: A systematic review. American Journal of Speech Language Pathology, 17(3), 212–230. https://doi.org/10.1044/1058-0360(2008/021)
Skinner, B. F. (1957). Verbal behavior. Prentice Hall.
Tincani, M., Cassella, M. A., & Tierney, K. (2020). Systematic review of verbal operants in speech-generating device research from Skinner’s analysis of verbal behavior. Augmentative and Alternative Communication, 36(4), 229–240. https://doi.org/10.1080/07434618.2020.1781584
Vannest, K. J., Parker, R. I., Gonen, O., & Adiguzel, T. (2016). Single Case Research: web based calculators for SCR analysis. (Version 2.0) [Web-based application]. Texas A&M University.
Walker, V. L., & Snell, M. E. (2013). Effects of augmentative and alternative communication on challenging behavior: A meta-analysis. Augmentative and Alternative Communication, 29(2), 117–131. https://doi.org/10.3109/07434618.2013.785020
Wodka, E. L., Mathy, P., & Kalb, L. (2013). Predictors of phrase and fluent speech in children with autism and severe language delay. Pediatrics, 131(4), e1128–e1134. https://doi.org/10.1542/peds.2012-2221
*Refers to the included studies in this review
*Alzrayer, N. M. (2020). Transitioning from a low- to high-tech Augmentative and Alternative Communication (AAC) system: Effects on augmented and vocal requesting. AAC: Augmentative & Alternative Communication, 36(3), 155–165.
*Alzrayer, N. M., Banda, D. R., & Koul, R. (2017). Teaching children with autism spectrum disorder and other developmental disabilities to perform multistep requesting using an iPad. AAC: Augmentative & Alternative Communication, 33(2), 65–76.
*Alzrayer, N. M., Banda, D. R., & Koul, R. K. (2019). The effects of systematic instruction in teaching multistep social-communication skills to children with autism spectrum disorder using an iPad. Developmental Neurorehabilitation, 22(6), 415–429.
*Alzrayer, N. M., Muharib, R., & Wood, C. (2020). Effects of a behavior intervention package on augmented and vocal mands by children with developmental disabilities. Journal of Developmental & Physical Disabilities, 32(1), 57–74.
*Carnett, A., Bravo, A., & Waddington, H. (2019). Teaching mands for actions to children with autism spectrum disorder using systematic instruction, behavior chain interruption, and a speech-generating device. International Journal of Developmental Disabilities, 65(2), 98–107.
*Carnett, A., Hansen, S., Tullis, C., & Machalicek, W. (2021). Using behavioural skills training via telehealth to increase teachers use of communication interventions and increase student use of speech-generating devices in a high school functional skills classroom. Journal of Intellectual Disability Research, 65(2), 133–148.
*Carnett, A., Ingvarsson, E. T., Bravo, A., & Sigafoos, J. (2020). Teaching children with autism spectrum disorder to ask “where” questions using a speech-generating device. Journal of Applied Behavior Analysis, 53(3), 1383–1403.
*Carnett, A., Waddington, H., & Bravo, A. (2018). Teaching intraverbal fill-ins to a child with autism spectrum disorder using a speech-generating device and systematic instruction. Advances in Neurodevelopmental Disorders, 2(1), 62–68.
*Genc-Tosun, D., Kurt, O., Cevher, Z., & Gregori, E. V. (2022). Teaching children with autism spectrum disorder to answer questions using an iPad-based speech-generating device. Journal of Autism and Developmental Disorders. https://doi.org/10.1007/s10803-022-05683-z
*Gevarter, C., Groll, M., Stone, E., & Medina Najar, A. (2021). A parent-implemented embedded AAC intervention for teaching navigational requests and other communicative functions to children with autism spectrum disorder. AAC: Augmentative & Alternative Communication, 37(3), 180–193.
*Holyfield, C. (2021). Comparative effects of picture symbol with paired text and text-only augmentative and alternative communication representations on communication from children with autism spectrum disorder. American Journal of Speech-Language Pathology, 30, 584–597.
*King, M. L., Takeguchi, K., Barry, S. E., Rehfeldt, R. A., Boyer, V. E., & Mathews, T. L. (2014). Evaluation of the iPad in the acquisition of requesting skills for children with autism spectrum disorder. Research in Autism Spectrum Disorders, 8(9), 1107–1120.
*Krcek, T. E. (2015). Effectiveness of Proloquo2Go in enhancing communication in children with autism during ABA therapy. (Unpublished doctoral dissertation). [The University of Tennessee].
*Lorah, E. R. (2018). Evaluating the iPad Mini as a speech-generating device in the acquisition of a discriminative mand repertoire for young children with autism. Focus on Autism and Other Developmental Disabilities, 33(1), 47–54.
*Lorah, E. R., Crouser, J., Gilroy, S. P., Tincani, M., & Hantula, D. (2014a). Within stimulus prompting to teach symbol discrimination using an iPad speech generating device. Journal of Developmental and Physical Disabilities, 26(3), 335–346.
*Lorah, E. R., & Griffen, B. (2023a). Teaching children with autism traveling skills for using a speech-generating device for manding. Journal of Developmental and Physical Disabilities, 35, 509–522.
*Lorah, E. R., & Griffen, B. (2023b). Establishing a mand repertoire using an interrupted chain procedure with SGD in children with autism spectrum disorder. Journal of Developmental & Physical Disabilities, 35(1), 97–110.
*Lorah, E. R., Karnes, A., Miller, J., & Welch-Beardsley, J. (2019). Establishing peer manding in young children with autism using a speech-generating device. Journal of Developmental and Physical Disabilities, 31(6), 791–801.
*Lorah, E. R., Karnes, A., & Speight, D. R. (2015). The acquisition of intraverbal responding using a speech generating device in school-aged children with autism. Journal of Developmental and Physical Disabilities, 27(4), 557–568.
*Lorah, E. R., Miller, J., & Griffen, B. (2021). The acquisition of peer manding using a speech-generating device in naturalistic classroom routines. Journal of Developmental and Physical Disabilities, 33, 619–631.
*Lorah, E. R., & Parnell, A. (2017). Acquisition of tacting using a speech-generating device in group learning environments for preschoolers with autism. Journal of Developmental and Physical Disabilities, 29(4), 597–609.
*Lorah, E. R., Parnell, A., & Speight, D. R. (2014b). Acquisition of sentence frame discrimination using the iPad as a speech generating device in young children with developmental disabilities. Research in Autism Spectrum Disorders, 8(12), 1734.
*Lorah, E. R., Tincani, M., Dodge, J., Gilroy, S., Hickey, A., & Hantula, D. (2013). Evaluating picture exchange and the iPad as a speech generating device to teach communication to young children with autism. Journal of Developmental and Physical Disabilities, 25(6), 637–649.
*McLay, L., van der Meer, L., Schäfer, M. C. M., Couper, L., McKenzie, E., O’Reilly, M. F., Lancioni, G. E., Marschik, P. B., Green, V. A., Sigafoos, J., & Sutherland, D. (2015). Comparing acquisition, generalization, maintenance, and preference across three AAC options in four children with autism spectrum disorder. Journal of Developmental and Physical Disabilities, 27(3), 323–339. https://doi.org/10.1007/s10882-014-9417-x
*Muharib, R., Alzrayer, N. M., Wood, C. L., & Voggt, A. P. (2019). Backward chaining and speech-output technologies to enhance functional communication skills of children with autism spectrum disorder and developmental disabilities. AAC: Augmentative & Alternative Communication, 35(4), 251–262.
*Rinaldi, B. (2019). Effects of naturalistic time delay on promoting functional requests using AAC in preschoolers with autism spectrum disorders. (Unpublished doctoral dissertation). [University of Kentucky].
*Sawchak, A., Waddington, H., & Sigafoos, J. (2023). Teaching multi-step requesting and social communication to five autistic children using speech-generating devices and systematic instruction. Advances in Neurodevelopmental Disorders. https://doi.org/10.1007/s41252-023-00320-x
*Tullis, C. A., Marya, V., & Alice Shillingsburg, M. (2019). Enhancing instruction via instructive feedback for a child with autism using a speech-generating device. The Analysis of Verbal Behavior, 35(1), 103–112.
*Waddington, H., van der Meer, L., Carnett, A., & Sigafoos, J. (2017). Teaching a child with ASD to approach communication partners and use a speech-generating device across settings: Clinic, school, and home. Canadian Journal of School Psychology, 32, 228–243.
*Wendt, O., Hsu, N., Simon, K., Dienhart, A., & Cain, L. (2019). Effects of an iPad-based speech-generating device infused into instruction with the picture exchange communication system for adolescents and young adults with severe autism spectrum disorder. Behavior Modification, 43(6), 898–932.
*Yong, Y. H. L., Dutt, A. S., Chen, M., & Yeong, A. M. (2021). Evaluating acquisition, preference and discrimination in requesting skills between picture exchange and iPad®-based speech generating device across preschoolers. Child Language Teaching and Therapy, 37(2), 123–136.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Muharib, R., Walker, V. & Dunn, W. Effects of Interventions Involving Tablet-Based Speech-Generating Devices for Individuals with ASD: A Meta-analysis. J Autism Dev Disord (2023). https://doi.org/10.1007/s10803-023-06173-6
Accepted:
Published:
DOI: https://doi.org/10.1007/s10803-023-06173-6